
Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty

 ,
,  ,
, 
Abstract
1. Introduction: A Basic Model for Geroscience
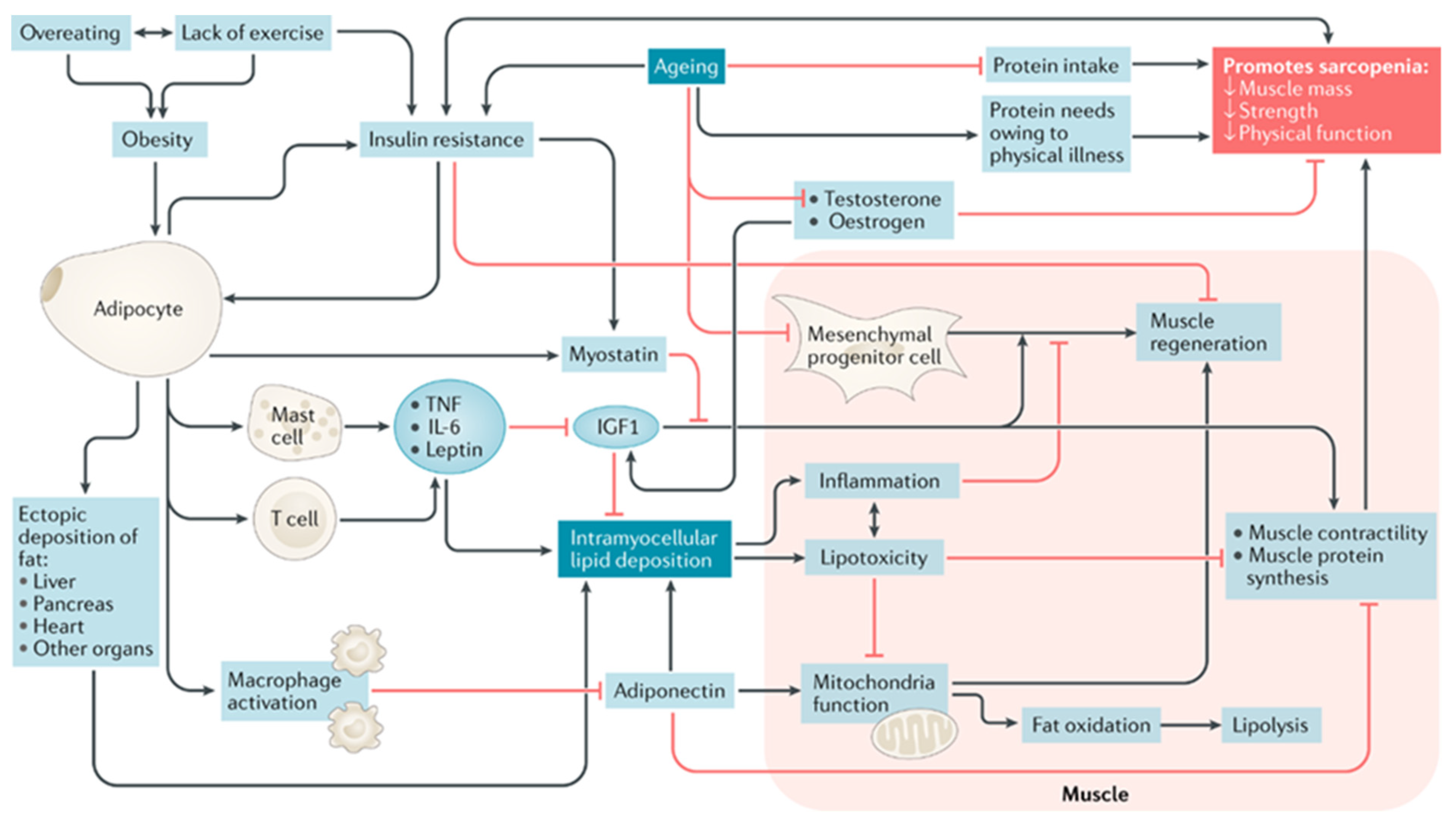
2. Biological Changes Contributing to the Development of Sarcopenic Obesity
2.1. Sarcopenic Obesity
2.2. Body Composition
2.3. Sex-Specific Hormones
2.4. Inflammatory Pathways
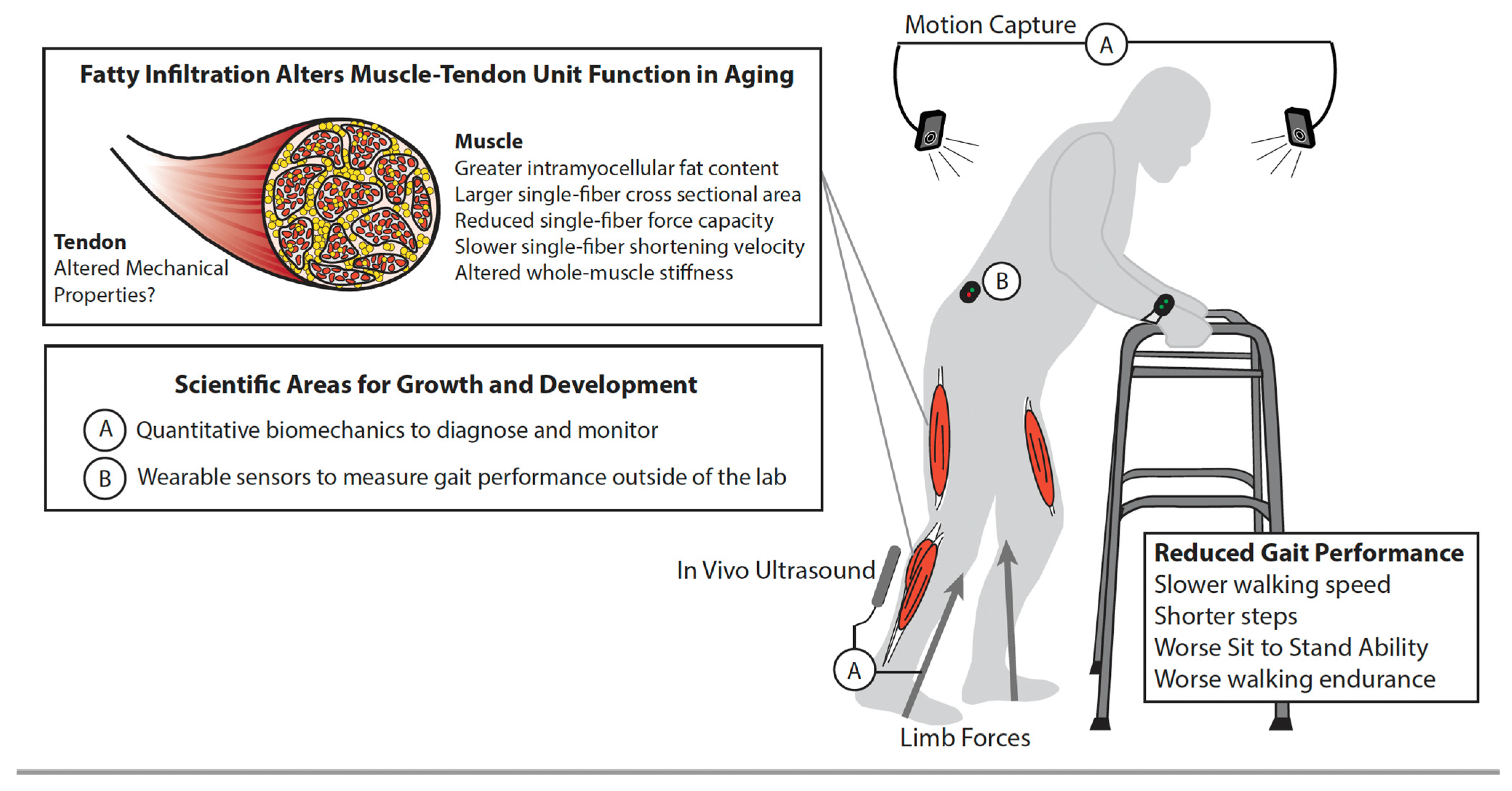
2.5. Myocellular Pathways and Intramuscular Fat Deposition
3. Biomechanics and Gait Performance
4. Imaging Modalities to Identify Intramuscular Fat
4.1. Magnetic Resonance Imaging
4.2. Computed Tomography (CT)
4.3. Ultrasonography
5. Integrating Biological Measures to Identify and Target Mechanistic Pathways

{kind=link}
{kind=link}
{kind=link}
| Study | Model | Category | Syndrome | Summary of Study Findings Regarding Biomarkers, Metabolic Pathways, and Gene Associated with Aging |
|---|---|---|---|---|
| Lin et al. [76] | Human | Genomics | Sarcopenia | The A allele of the CAV1G14713A Caveolin protein 1 (CAV1) may be a predictor for higher likelihood of developing sarcopenia and severe sarcopenia in a Taiwanese older adult population. |
| Dos Santos et al. [74] | Human | Proteomics | Sarcopenia | The functional decline in 17 carboxylate proteins involved in cellular transport, energy metabolism and muscle contraction may be associated with a sarcopenic phenotype. |
| Tsai et al. [72] | Human | Metabolomics | Sarcopenia | Plasma traumatic acid has been identified as potential biomarker for sarcopenia. |
| Opazo et al. [78] | Human | Metabolomics | Sarcopenia | Pathways of biosynthesis of amino acids and alkaloids derived from ornithine, arginine and proline metabolism, linoleic acid metabolism, and the biosynthesis of unsaturated fatty acids are associated with a “sarcopenic phenotype.” |
| Pujols et al. [79] | Human | Metabolomics | Pre-frailty | Four potential markers for each sex that discriminate between sub-phenotypes of pre-frailty.
|
| Burd et al. [70] | Mice | Proteomics | Frailty | Mice models suggest that molecular markers associated with aging, such as p16IN and IL6, are potential targets for pharmacological interventions using Janus kinase inhibitors. |
6. Nutritional Interventions
7. Gaps in the Science
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for Clinical Practice and Public Health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Walston, J.; Buta, B.; Xue, Q.-L. Frailty Screening and Interventions: Considerations for Clinical Practice. Clin. Geriatr. Med. 2018, 34, 25. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between Frailty and Quality of Life among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Cohen, A.A.; Xue, Q.-L.; Walston, J.; Bandeen-Roche, K.; Varadhan, R. The Physical Frailty Syndrome as a Transition from Homeostatic Symphony to Cacophony. Nat. Aging 2021, 1, 36–46. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R.; Zhou, J.; Fried, L.P. Initial Manifestations of Frailty Criteria and the Development of Frailty Phenotype in the Women’s Health and Aging Study II. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 984–990. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic Obesity in Older Adults: Aetiology, Epidemiology and Treatment Strategies. Nat. Rev. Endocrinol. 2018, 14, 513. [Google Scholar] [CrossRef]
- Batsis, J.A.; Barre, L.K.; Mackenzie, T.A.; Pratt, S.I.; Lopez-Jimenez, F.; Bartels, S.J. Variation in the Prevalence of Sarcopenia and Sarcopenic Obesity in Older Adults Associated with Different Research Definitions: Dual-Energy X-ray Absorptiometry Data from the National Health and Nutrition Examination Survey 1999–2004. J. Am. Geriatr. Soc. 2013, 61, 974–980. [Google Scholar] [CrossRef] [PubMed]
- el Ghoch, M.; Calugi, S.; Grave, R.D. Sarcopenic Obesity: Definition, Health Consequences and Clinical Management. Open Nutr. J. 2018, 12, 70–73. [Google Scholar] [CrossRef]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Kuchel, G.A. Heterogeneity of Aging: Individual Risk Factors, Mechanisms, Patient Priorities, and Outcomes. J. Am. Geriatr. Soc. 2021, 69, 610–612. [Google Scholar] [CrossRef]
- Sierra, F.; Caspi, A.; Fortinsky, R.H.; Haynes, L.; Lithgow, G.J.; Moffitt, T.E.; Olshansky, S.J.; Perry, D.; Verdin, E.; Kuchel, G.A. Moving Geroscience from the Bench to Clinical Care and Health Policy. J. Am. Geriatr. Soc. 2021, 69, 2455–2463. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Zagaria, A.B. Addressing Obesity in Aging Patients. Med. Clin. N. Am. 2018, 102, 65–85. [Google Scholar] [CrossRef]
- Perkisas, S.; Baudry, S.; Bauer, J.; Beckwée, D.; de Cock, A.-M.; Hobbelen, H.; Jager-Wittenaar, H.; Kasiukiewicz, A.; Landi, F.; Marco, E.; et al. Application of Ultrasound for Muscle Assessment in Sarcopenia: Towards Standardized Measurements. Eur. Geriatr. Med. 2018, 9, 739–757. [Google Scholar] [CrossRef]
- Addison, O.; Marcus, R.L.; LaStayo, P.C.; Ryan, A.S. Intermuscular Fat: A Review of the Consequences and Causes. Int. J. Endocrinol. 2014, 2014, 309570. [Google Scholar] [CrossRef]
- Sowers, M.F.; Zheng, H.; Tomey, K.; Karvonen-Gutierrez, C.; Jannausch, M.; Li, X.; Yosef, M.; Symons, J. Changes in Body Composition in Women over Six Years at Midlife: Ovarian and Chronological Aging. J. Clin. Endocrinol. Metab. 2007, 92, 895–901. [Google Scholar] [CrossRef]
- Kozakowski, J.; Gietka-Czernel, M.; Leszczynska, D.; Majos, A. Obesity in Menopause—Our Negligence or an Unfortunate Inevitability? Prz. Menopauzalny Menopause Rev. 2017, 16, 61–65. [Google Scholar] [CrossRef]
- D’Eon, T.M.; Souza, S.C.; Aronovitz, M.; Obin, M.S.; Fried, S.K.; Greenberg, A.S. Estrogen Regulation of Adiposity and Fuel Partitioning: Evidence of Genomic and Non-Genomic Regulation of Lipogenic and Oxidative Pathways. J. Biol. Chem. 2005, 280, 35983–35991. [Google Scholar] [CrossRef] [PubMed]
- Kadi, F. Cellular and Molecular Mechanisms Responsible for the Action of Testosterone on Human Skeletal Muscle. A Basis for Illegal Performance Enhancement. Br. J. Pharmacol. 2008, 154, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Schrager, M.A.; Metter, E.J.; Simonsick, E.; Ble, A.; Bandinelli, S.; Lauretani, F.; Ferrucci, L. Sarcopenic Obesity and Inflammation in the InCHIANTI Study. J. Appl. Physiol. 2007, 102, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Park, J.Y.; Yu, R. Relationship of Obesity and Visceral Adiposity with Serum Concentrations of CRP, TNF-Alpha and IL-6. Diabetes Res. Clin. Pract. 2005, 69, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Shulman, G.I. Ectopic Fat in Insulin Resistance, Dyslipidemia, and Cardiometabolic Disease. N. Engl. J. Med. 2014, 371, 1131–1141. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The Loss of Skeletal Muscle Strength, Mass, and Quality in Older Adults: The Health, Aging and Body Composition Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Stenholm, S.; Harris, T.B.; Rantanen, T.; Visser, M.; Kritchevsky, S.B.; Ferrucci, L. Sarcopenic Obesity: Definition, Cause and Consequences. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 693–700. [Google Scholar] [CrossRef]
- Marcus, R.L.; Addison, O.; Dibble, L.E.; Foreman, K.B.; Morrell, G.; LaStayo, P. Intramuscular Adipose Tissue, Sarcopenia, and Mobility Function in Older Individuals. J. Aging Res. 2012, 2012, 629637. [Google Scholar] [CrossRef]
- Moore, A.Z.; Caturegli, G.; Metter, E.J.; Makrogiannis, S.; Resnick, S.M.; Harris, T.B.; Ferrucci, L. Difference in Muscle Quality over the Adult Life Span and Biological Correlates in the Baltimore Longitudinal Study of Aging. J. Am. Geriatr. Soc. 2014, 62, 230–236. [Google Scholar] [CrossRef]
- Choi, S.J.; Files, D.C.; Zhang, T.; Wang, Z.-M.; Messi, M.L.; Gregory, H.; Stone, J.; Lyles, M.F.; Dhar, S.; Marsh, A.P.; et al. Intramyocellular Lipid and Impaired Myofiber Contraction in Normal Weight and Obese Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 71, 557–564. [Google Scholar] [CrossRef]
- Straight, C.R.; Voigt, T.B.; Jala, A.V.; Chase, J.D.; Ringham, O.R.; Ades, P.A.; Toth, M.J.; Miller, M.S. Quadriceps Lipid Content Has Sex-Specific Associations with Whole-Muscle, Cellular, and Molecular Contractile Function in Older Adults. J. Gerontol. Ser. A 2018, 74, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Pinel, S.; Kelp, N.Y.; Bugeja, J.M.; Bolsterlee, B.; Hug, F.; Dick, T.J.M. Quantity versus Quality: Age-Related Differences in Muscle Volume, Intramuscular Fat, and Mechanical Properties in the Triceps Surae. Exp. Gerontol. 2021, 156, 111594. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, D.J.; Erskine, R.M.; Morse, C.I.; Pappachan, J.M.; Sanderson-Gillard, E.; Onambélé-Pearson, G.L. The Combined Effects of Obesity and Ageing on Skeletal Muscle Function and Tendon Properties in Vivo in Men. Endocrine 2021, 72, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Salini, V.; Andia, I. How Obesity Affects Tendons? In Metabolic Influences on Risk for Tendon Disorders; Springer International Publishing: Cham, Switzerland, 2016; pp. 167–177. [Google Scholar]
- Fessel, G.; Li, Y.; Diederich, V.; Guizar-Sicairos, M.; Schneider, P.; Sell, D.R.; Monnier, V.M.; Snedeker, J.G. Advanced Glycation End-Products Reduce Collagen Molecular Sliding to Affect Collagen Fibril Damage Mechanisms but Not Stiffness. PLoS ONE 2014, 9, e110948. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.-C.; Hsu, C.-C.; Lee, W.-J.; Liang, C.-K.; Chou, M.-Y.; Lin, M.-H.; Hsiao, F.-Y.; Peng, L.-N.; Chen, L.-K. Muscle-to-Fat Ratio Identifies Functional Impairments and Cardiometabolic Risk and Predicts Outcomes: Biomarkers of Sarcopenic Obesity. J. Cachexia Sarcopenia Muscle 2021, 13, 368–376. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J. Sarcopenic Obesity Revisited: Insights from the Mr and Ms Os Cohort. J. Am. Med. Dir. Assoc. 2018, 19, 679–684.e2. [Google Scholar] [CrossRef]
- Yamashita, M.; Kamiya, K.; Matsunaga, A.; Kitamura, T.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Tanaka, S.; Nakamura, T.; Maekawa, E.; et al. Prognostic Value of Sarcopenic Obesity Estimated by Computed Tomography in Patients with Cardiovascular Disease and Undergoing Surgery. J. Cardiol. 2019, 74, 273–278. [Google Scholar] [CrossRef]
- de Campos, G.C.; Lourenço, R.A.; Lopes, C.S. Prevalence of Sarcopenic Obesity and Its Association with Functionality, Lifestyle, Biomarkers and Morbidities in Older Adults: The FIBRA-RJ Study of Frailty in Older Brazilian Adults. Clinics 2020, 75, e1814. [Google Scholar] [CrossRef]
- Purcell, S.A.; Mackenzie, M.; Barbosa-Silva, T.G.; Dionne, I.J.; Ghosh, S.; Siervo, M.; Ye, M.; Prado, C.M. Prevalence of Sarcopenic Obesity Using Different Definitions and the Relationship with Strength and Physical Performance in the Canadian Longitudinal Study of Aging. Front. Physiol. 2021, 11, 583825. [Google Scholar] [CrossRef]
- Therakomen, V.; Petchlorlian, A.; Lakananurak, N. Prevalence and Risk Factors of Primary Sarcopenia in Community-Dwelling Outpatient Elderly: A Cross-Sectional Study. Sci. Rep. 2020, 10, 19551. [Google Scholar] [CrossRef]
- Waters, D.L.; Hale, L.; Grant, A.M.; Herbison, P.; Goulding, A. Osteoporosis and Gait and Balance Disturbances in Older Sarcopenic Obese New Zealanders. Osteoporos. Int. 2009, 21, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Rahemi, H.; Nigam, N.; Wakeling, J.M. The Effect of Intramuscular Fat on Skeletal Muscle Mechanics: Implications for the Elderly and Obese. J. R. Soc. Interface 2015, 12, 20150365. [Google Scholar] [CrossRef] [PubMed]
- Stock, M.S.; Thompson, B.J. Echo Intensity as an Indicator of Skeletal Muscle Quality: Applications, Methodology, and Future Directions. Eur. J. Appl. Physiol. 2020, 121, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.; Rosander, J.; Romu, T.; Tallberg, J.; Grönqvist, A.; Borga, M.; Leinhard, O.D. Automatic and Quantitative Assessment of Regional Muscle Volume by Multi-Atlas Segmentation Using Whole-Body Water-Fat MRI. J. Magn. Reson. Imaging 2014, 41, 1558–1569. [Google Scholar] [CrossRef] [PubMed]
- Orgiu, S.; Lafortuna, C.L.; Rastelli, F.; Cadioli, M.; Falini, A.; Rizzo, G. Automatic Muscle and Fat Segmentation in the Thigh FromT1-Weighted MRI. J. Magn. Reson. Imaging 2015, 43, 601–610. [Google Scholar] [CrossRef]
- Bray, T.J.P.; Chouhan, M.D.; Punwani, S.; Bridge, A.; Hall-Craggs, M.A. Fat Fraction Mapping Using Magnetic Resonance Imaging: Insight into Pathophysiology. Br. J. Radiol. 2018, 91, 20170344. [Google Scholar] [CrossRef]
- Hu, H.H.; Yokoo, T.; Bashir, M.R.; Sirlin, C.B.; Hernando, D.; Malyarenko, D.; Chenevert, T.L.; Smith, M.A.; Serai, S.D.; Middleton, M.S.; et al. Linearity and Bias of Proton Density Fat Fraction as a Quantitative Imaging Biomarker: A Multicenter, Multiplatform, Multivendor Phantom Study. Radiology 2021, 298, 640–651. [Google Scholar] [CrossRef]
- Amini, B.; Boyle, S.P.; Boutin, R.D.; Lenchik, L. Approaches to Assessment of Muscle Mass and Myosteatosis on Computed Tomography: A Systematic Review. J. Gerontol. Ser. A 2019, 74, 1671–1678. [Google Scholar] [CrossRef]
- Albano, D.; Messina, C.; Vitale, J.; Sconfienza, L.M. Imaging of Sarcopenia: Old Evidence and New Insights. Eur. Radiol. 2019, 30, 2199–2208. [Google Scholar] [CrossRef]
- Giraudo, C.; Cavaliere, A.; Lupi, A.; Guglielmi, G.; Quaia, E. Established Paths and New Avenues: A Review of the Main Radiological Techniques for Investigating Sarcopenia. Quant. Imaging Med. Surg. 2020, 10, 1602–1613. [Google Scholar] [CrossRef]
- Schedel, H.; Reimers, C.D.; Nägele, M.; Witt, T.N.; Pongratz, D.E.; Vogl, T. Imaging Techniques in Myotonic Dystrophy. A Comparative Study of Ultrasound, Computed Tomography and Magnetic Resonance Imaging of Skeletal Muscles. Eur. J. Radiol. 1992, 15, 230–238. [Google Scholar] [CrossRef]
- Hyun, S.-J.; Bae, C.-W.; Lee, S.-H.; Rhim, S.-C. Fatty Degeneration of the Paraspinal Muscle in Patients with Degenerative Lumbar Kyphosis. Clin. Spine Surg. A Spine Publ. 2016, 29, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; et al. Pitfalls in the Measurement of Muscle Mass: A Need for a Reference Standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Franco-Sadud, R.; Schnobrich, D.; Mathews, B.K.; Candotti, C.; Abdel-Ghani, S.; Perez, M.G.; Rodgers, S.C.; Mader, M.J.; Haro, E.K.; Dancel, R.; et al. Recommendations on the Use of Ultrasound Guidance for Central and Peripheral Vascular Access in Adults: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, E1–E22. [Google Scholar] [CrossRef] [PubMed]
- Soni, N.J.; Franco-Sadud, R.; Kobaidze, K.; Schnobrich, D.; Salame, G.; Lenchus, J.; Kalidindi, V.; Mader, M.J.; Haro, E.K.; Dancel, R.; et al. Recommendations on the Use of Ultrasound Guidance for Adult Lumbar Puncture: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, 591–601. [Google Scholar] [CrossRef]
- Dancel, R.; Schnobrich, D.; Puri, N.; Franco-Sadud, R.; Cho, J.; Grikis, L.; Lucas, B.P.; El-Barbary, M.; Abdel-Ghani, S.; Arntfield, R.; et al. Recommendations on the Use of Ultrasound Guidance for Adult Thoracentesis: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2018, 13, 126–135. [Google Scholar] [CrossRef]
- Cho, J.; Jensen, T.P.; Reierson, K.; Mathews, B.K.; Bhagra, A.; Franco-Sadud, R.; Grikis, L.; Mader, M.; Dancel, R.; Lucas, B.P.; et al. Recommendations on the Use of Ultrasound Guidance for Adult Abdominal Paracentesis: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, E7. [Google Scholar] [CrossRef]
- Qaseem, A.; Etxeandia-Ikobaltzeta, I.; Mustafa, R.A.; Kansagara, D.; Fitterman, N.; Wilt, T.J. Appropriate Use of Point-of-Care Ultrasonography in Patients with Acute Dyspnea in Emergency Department or Inpatient Settings: A Clinical Guideline from the American College of Physicians. Ann. Intern. Med. 2021, 174, 985–993. [Google Scholar] [CrossRef]
- Breunig, M.; Burkhamer, K.J.; Kashiwagi, D. Using Point-of-Care Ultrasound: Skin and Soft Tissue Infections. JAAPA Off. J. Am. Acad. Physician Assist. 2019, 32, 46–50. [Google Scholar] [CrossRef]
- Soni, N.J.; Schnobrich, D.; Mathews, B.K.; Tierney, D.M.; Jensen, T.P.; Dancel, R.; Cho, J.; Dversdal, R.K.; Mints, G.; Bhagra, A.; et al. Point-of-Care Ultrasound for Hospitalists: A Position Statement of the Society of Hospital Medicine. J. Hosp. Med. 2019, 14, E1. [Google Scholar] [CrossRef]
- Stringer, H.J.; Wilson, D. The Role of Ultrasound as a Diagnostic Tool for Sarcopenia. J. Frailty Aging 2018, 7, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Dankel, S.J.; Abe, T.; Bell, Z.W.; Jessee, M.B.; Buckner, S.L.; Mattocks, K.T.; Mouser, J.G.; Loenneke, J.P. The Impact of Ultrasound Probe Tilt on Muscle Thickness and Echo-Intensity: A Cross-Sectional Study. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2020, 23, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Justice, J.; Miller, J.D.; Newman, J.C.; Hashmi, S.K.; Halter, J.; Austad, S.N.; Barzilai, N.; Kirkland, J.L. Frameworks for Proof-of-Concept Clinical Trials of Interventions That Target Fundamental Aging Processes. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1415–1423. [Google Scholar] [CrossRef] [PubMed]
- Kane, A.E.; Hilmer, S.N.; Boyer, D.; Gavin, K.; Nines, D.; Howlett, S.E.; de Cabo, R.; Mitchell, S.J. Impact of Longevity Interventions on a Validated Mouse Clinical Frailty Index. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 333. [Google Scholar] [CrossRef]
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto, R.I.; Pessin, J.E.; et al. Geroscience: Linking Aging to Chronic Disease. Cell 2014, 159, 709–713. [Google Scholar] [CrossRef]
- Hshieh, T.T.; Yue, J.; Oh, E.; Puelle, M.; Dowal, S.; Travison, T.; Inouye, S.K. Effectiveness of Multicomponent Nonpharmacological Delirium Interventions: A Meta-Analysis. JAMA Intern. Med. 2015, 175, 512–520. [Google Scholar] [CrossRef]
- Huffman, D.M.; Justice, J.N.; Stout, M.B.; Kirkland, J.L.; Barzilai, N.; Austad, S.N. Evaluating Health Span in Preclinical Models of Aging and Disease: Guidelines, Challenges, and Opportunities for Geroscience. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1395–1406. [Google Scholar] [CrossRef]
- Bartoli, F.; Debant, M.; Chuntharpursat-Bon, E.; Evans, E.L.; Musialowski, K.E.; Parsonage, G.; Morley, L.C.; Futers, T.S.; Sukumar, P.; Bowen, T.S.; et al. Endothelial Piezo1 Sustains Muscle Capillary Density and Contributes to Physical Activity. J. Clin. Investig. 2022, 132, e141775. [Google Scholar] [CrossRef]
- Burd, C.E.; Gill, M.S.; Niedernhofer, L.J.; Robbins, P.D.; Austad, S.N.; Barzilai, N.; Kirkland, J.L. Barriers to the Preclinical Development of Therapeutics That Target Aging Mechanisms. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1388. [Google Scholar] [CrossRef]
- Melouane, A.; Ghanemi, A.; Yoshioka, M.; St-Amand, J. Functional Genomics Applications and Therapeutic Implications in Sarcopenia. Mutat. Res. Rev. Mutat. Res. 2019, 781, 175–185. [Google Scholar] [CrossRef]
- Tsai, J.S.; Wang, S.Y.; Chang, C.H.; Chen, C.Y.; Wen, C.J.; Chen, G.Y.; Kuo, C.H.; Tseng, Y.J.; Chen, C.Y. Identification of Traumatic Acid as a Potential Plasma Biomarker for Sarcopenia Using a Metabolomics-Based Approach. J. Cachexia Sarcopenia Muscle 2022, 13, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-C.; Dong, S.-S.; Shen, H.; Yang, D.-Y.; Chen, B.-B.; Ma, X.-Y.; Peng, Y.-R.; Xiao, H.-M.; Deng, H.-W. Multi-Omics Research in Sarcopenia: Current Progress and Future Prospects. Ageing Res. Rev. 2022, 76, 101576. [Google Scholar] [CrossRef] [PubMed]
- Lourenço dos Santos, S.; Baraibar, M.A.; Lundberg, S.; Eeg-Olofsson, O.; Larsson, L.; Friguet, B. Oxidative Proteome Alterations during Skeletal Muscle Ageing. Redox Biol. 2015, 5, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Mougeolle, A.; Poussard, S.; Decossas, M.; Lamaze, C.; Lambert, O.; Dargelos, E. Oxidative Stress Induces Caveolin 1 Degradation and Impairs Caveolae Functions in Skeletal Muscle Cells. PLoS ONE 2015, 10, e0122654. [Google Scholar] [CrossRef]
- Lin, C.H.; Lin, C.C.; Tsai, C.W.; Chang, W.S.; Yang, M.D.; Bau, D.T. A Novel Caveolin-1 Biomarker for Clinical Outcome of Sarcopenia. In Vivo 2014, 28, 383–389. [Google Scholar]
- Picca, A.; Coelho-Junior, H.J.; Cesari, M.; Marini, F.; Miccheli, A.; Gervasoni, J.; Bossola, M.; Landi, F.; Bernabei, R.; Marzetti, E.; et al. The Metabolomics Side of Frailty: Toward Personalized Medicine for the Aged. Exp. Gerontol. 2019, 126, 110692. [Google Scholar] [CrossRef]
- Opazo, R.; Angel, B.; Márquez, C.; Lera, L.; Cardoso Dos Santos, G.R.; Monnerat, G.; Albala, C. Sarcopenic Metabolomic Profile Reflected a Sarcopenic Phenotype Associated with Amino Acid and Essential Fatty Acid Changes. Metab. Off. J. Metab. Soc. 2021, 17, 83. [Google Scholar] [CrossRef]
- Pujos-Guillot, E.; Pétéra, M.; Jacquemin, J.; Centeno, D.; Lyan, B.; Montoliu, I.; Madej, D.; Pietruszka, B.; Fabbri, C.; Santoro, A.; et al. Identification of Pre-Frailty Sub-Phenotypes in Elderly Using Metabolomics. Front. Physiol. 2019, 9, 1903. [Google Scholar] [CrossRef]
- Batsis, J.A.; Petersen, C.L.; Clark, M.M.; Cook, S.B.; Kotz, D.; Gooding, T.L.; Roderka, M.N.; Al-Nimr, R.I.; Pidgeon, D.; Haedrich, A.; et al. Feasibility and Acceptability of a Technology-Based, Rural Weight Management Intervention in Older Adults with Obesity. BMC Geriatr. 2021, 21, 44. [Google Scholar] [CrossRef]
- Villareal, D.T.; Aguirre, L.; Gurney, A.B.; Waters, D.L.; Sinacore, D.R.; Colombo, E.; Armamento-Villareal, R.; Qualls, C. Aerobic or Resistance Exercise, or Both, in Dieting Obese Older Adults. N. Engl. J. Med. 2017, 376, 1943–1955. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Hashemi, R.; Heshmat, R.; Motlagh, A.D.; Esmaillzadeh, A. Association of Dietary Approaches to Stop Hypertension Eating Style and Risk of Sarcopenia. Sci. Rep. 2020, 10, 19339. [Google Scholar] [CrossRef] [PubMed]
- Stanton, A.; Buckley, J.; Villani, A. Adherence to a Mediterranean Diet Is Not Associated with Risk of Sarcopenic Symptomology: A Cross-Sectional Analysis of Overweight and Obese Older Adults in Australia. J. Frailty Aging 2019, 8, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.A.; van Guilder, G.P.; Kauffman, A.; Hossain, M. A Calorie-Restricted DASH Diet Reduces Body Fat and Maintains Muscle Strength in Obese Older Adults. Nutrients 2019, 12, 102. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.C.; McDaniel, J.L.; Mora, K.; Villareal, D.T.; Fontana, L.; Weiss, E.P. Preferential Reductions in Intermuscular and Visceral Adipose Tissue with Exercise-Induced Weight Loss Compared with Calorie Restriction. J. Appl. Physiol. 2012, 112, 79. [Google Scholar] [CrossRef]
- Greiwe, J.; Nyenhuis, S.M. Wearable Technology and How This Can Be Implemented into Clinical Practice. Curr. Allergy Asthma Rep. 2020, 20, 36. [Google Scholar] [CrossRef]
- Regterschot, G.R.H.; Ribbers, G.M.; Bussmann, J.B.J. Wearable Movement Sensors for Rehabilitation: From Technology to Clinical Practice. Sensors 2021, 21, 4744. [Google Scholar] [CrossRef]



| Modality | Method | Pros | Cons |
|---|---|---|---|
| MR | Threshold Intensity: sets intensity threshold on T1-weighted images to assign pixels to muscle or fat categories |
|
|
| Chemical Shift Methods: Based on the difference between different molecular resonance frequencies (i.e., fat and water) |
|
| |
| Dixon: generates images based on the constructive and destructive interference between water and fat |
|
| |
| MR Spectroscopy: calculated based on the area under the lipid peak produced, for a single voxel |
|
| |
| CT | 2D maps of pixels of different X-ray attenuation (HU). FF = inversely proportional to muscle attenuation in region of interest (darker muscle = more fat). |
|
|
| US | Based on muscle echointensity (higher echointensity = increased fat/decreased quality) |
|
|
| DEXA | Cannot determine fat fraction or muscle quality—only percent of lean muscle mass | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lynch, D.H.; Spangler, H.B.; Franz, J.R.; Krupenevich, R.L.; Kim, H.; Nissman, D.; Zhang, J.; Li, Y.-Y.; Sumner, S.; Batsis, J.A. Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty. Nutrients 2022, 14, 1384. https://doi.org/10.3390/nu14071384
Lynch DH, Spangler HB, Franz JR, Krupenevich RL, Kim H, Nissman D, Zhang J, Li Y-Y, Sumner S, Batsis JA. Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty. Nutrients. 2022; 14(7):1384. https://doi.org/10.3390/nu14071384
Chicago/Turabian StyleLynch, David H., Hillary B. Spangler, Jason R. Franz, Rebecca L. Krupenevich, Hoon Kim, Daniel Nissman, Janet Zhang, Yuan-Yuan Li, Susan Sumner, and John A. Batsis. 2022. "Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty" Nutrients 14, no. 7: 1384. https://doi.org/10.3390/nu14071384
APA StyleLynch, D. H., Spangler, H. B., Franz, J. R., Krupenevich, R. L., Kim, H., Nissman, D., Zhang, J., Li, Y.-Y., Sumner, S., & Batsis, J. A. (2022). Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty. Nutrients, 14(7), 1384. https://doi.org/10.3390/nu14071384