
The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective

 ,
,  ,
,  ,
,  ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Major Depressive Disorder in Women
2.1. General Pathophysiology
2.1.1. Can MDD Be Located in the Brain?
2.1.2. Cellular and Molecular Changes Associated with MDD
2.1.3. Systemic Alterations Associated with MDD
2.2. Pathophysiology Specific to MDD in Women
2.2.1. Biological Mechanisms
2.2.2. Psychological and Sociocultural Factors
2.3. MDD Clinic
2.3.1. General MDD Manifestations and Approaches
2.3.2. Women’s MDD Clinic
3. The Importance of Malnutrition in MDD from a Sex-Gender Perspective
3.1. Macronutrients
3.2. Micronutrient Deficiencies Related to Reproductive Age, Postpartum and Later Life
3.3. Specific Micronutrient Deficiencies Related to Menstruation, PMS and PMDD
3.4. Specific Micronutrient Deficiencies Related to Perinatal and Postpartum Depression
3.5. Specific Micronutrient Deficiencies Related to Peri- and Postmenopausal Depression
4. Nutritional Intervention in Women with MDD
4.1. Fatty Acids
4.2. Vitamins
4.2.1. Vitamin D
4.2.2. Vitamin B
4.2.3. Minerals
4.2.4. S-Adenosyl Methionine
4.2.5. Creatine and Amino Acids
4.2.6. Bioactive Compounds
Phytoestrogens
Caffeine
Anthocyanins
Resveratrol
Cannabidiol
4.2.7. Probiotics and Prebiotics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Otte, C.; Gold, S.M.; Penninx, B.W.; Pariante, C.M.; Etkin, A.; Fava, M.; Mohr, D.C.; Schatzberg, A.F. Major Depressive Disorder. Nat. Rev. Dis. Primers 2016, 2, 16065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD. Results Tool|GHDx. Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 23 November 2021).
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Lépine, J.P.; Briley, M. The Increasing Burden of Depression. Neuropsychiatr. Dis. Treat. 2011, 7, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruffaerts, R.; Vilagut, G.; Demyttenaere, K.; Alonso, J.; AlHamzawi, A.; Andrade, L.H.; Benjet, C.; Bromet, E.; Bunting, B.; de Girolamo, G.; et al. Role of Common Mental and Physical Disorders in Partial Disability around the World. Br. J. Psychiatry J. Ment. Sci. 2012, 200, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 5356. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Preventing Depression in the WHO European Region (2016). Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/publications/2016/preventing-depression-in-the-who-european-region-2016 (accessed on 5 February 2022).
- Rai, D.; Zitko, P.; Jones, K.; Lynch, J.; Araya, R. Country- and Individual-Level Socioeconomic Determinants of Depression: Multilevel Cross-National Comparison. Br. J. Psychiatry J. Ment. Sci. 2013, 202, 195–203. [Google Scholar] [CrossRef]
- Flint, J.; Kendler, K.S. The Genetics of Major Depression. Neuron 2014, 81, 484–503. [Google Scholar] [CrossRef] [Green Version]
- Kendler, K.S.; Gatz, M.; Gardner, C.O.; Pedersen, N.L. A Swedish National Twin Study of Lifetime Major Depression. Am. J. Psychiatry 2006, 163, 109–114. [Google Scholar] [CrossRef]
- Kuehner, C. Why Is Depression More Common among Women than among Men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Hankin, B.L.; Young, J.F.; Abela, J.R.Z.; Smolen, A.; Jenness, J.L.; Gulley, L.D.; Technow, J.R.; Gottlieb, A.B.; Cohen, J.R.; Oppenheimer, C.W. Depression from Childhood into Late Adolescence: Influence of Gender, Development, Genetic Susceptibility, and Peer Stress. J. Abnorm. Psychol. 2015, 124, 803–816. [Google Scholar] [CrossRef]
- Albert, P.R. Why Is Depression More Prevalent in Women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Weyand, A.C.; Fitzgerald, K.D.; McGrath, M.; Gupta, V.; Braun, T.M.; Quint, E.H.; Choi, S.W. Depression in Female Adolescents with Heavy Menstrual Bleeding. J. Pediatr. 2022, 240, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.; AACAP Work Group on Quality Issues. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Depressive Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1503–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windfuhr, K.; While, D.; Hunt, I.; Turnbull, P.; Lowe, R.; Burns, J.; Swinson, N.; Shaw, J.; Appleby, L.; Kapur, N.; et al. Suicide in Juveniles and Adolescents in the United Kingdom. J. Child Psychol. Psychiatry 2008, 49, 1155–1165. [Google Scholar] [CrossRef] [PubMed]
- Owens, S.A.; Eisenlohr-Moul, T.A.; Prinstein, M.J. Understanding When and Why Some Adolescent Girls Attempt Suicide: An Emerging Framework Integrating Menstrual Cycle Fluctuations in Risk. Child Dev. Perspect. 2020, 14, 116–123. [Google Scholar] [CrossRef]
- Mckeever, A.; Agius, M.; Mohr, P. A Review of the Epidemiology of Major Depressive Disorder and of Its Consequences for Society and the Individual. Psychiatr. Danub. 2017, 29, 222–231. [Google Scholar]
- Platt, J.; Prins, S.; Bates, L.; Keyes, K. Unequal Depression for Equal Work? How the Wage Gap Explains Gendered Disparities in Mood Disorders. Soc. Sci. Med. 2016, 149, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Heise, L.L.; Kotsadam, A. Cross-National and Multilevel Correlates of Partner Violence: An Analysis of Data from Population-Based Surveys. Lancet Glob. Health 2015, 3, e332–e340. [Google Scholar] [CrossRef] [Green Version]
- Bebbington, P.; Dunn, G.; Jenkins, R.; Lewis, G.; Brugha, T.; Farrell, M.; Meltzer, H. The Influence of Age and Sex on the Prevalence of Depressive Conditions: Report from the National Survey of Psychiatric Morbidity. Int. Rev. Psychiatry 2003, 15, 74–83. [Google Scholar] [CrossRef]
- Ljungberg, T.; Bondza, E.; Lethin, C. Evidence of the Importance of Dietary Habits Regarding Depressive Symptoms and Depression. Int. J. Environ. Res. Public Health 2020, 17, 1616. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Mon, M.A.; Ortega, M.A.; García-Montero, C.; Fraile-Martinez, O.; Monserrat, J.; Lahera, G.; Mora, F.; Rodriguez-Quiroga, A.; Fernandez-Rojo, S.; Quintero, J.; et al. Exploring the Role of Nutraceuticals in Major Depressive Disorder (MDD): Rationale, State of the Art and Future Prospects. Pharmaceuticals 2021, 14, 821. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; Murphy, J.; Mischoulon, D.; Papakostas, G.I.; Fava, M.; Berk, M.; Ng, C.H. Adjunctive Nutraceuticals for Depression: A Systematic Review and Meta-Analyses. Am. J. Psychiatry 2016, 173, 575–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.F.; Peng, W.; Sweeney, J.A.; Jia, Z.Y.; Gong, Q.Y. Brain structure alterations in depression: Psychoradiological evidence. CNS Neurosci. Ther. 2018, 24, 994–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Eijndhoven, P.; van Wingen, G.; Katzenbauer, M.; Groen, W.; Tepest, R.; Fernández, G.; Buitelaar, J.; Tendolkar, I. Paralimbic Cortical Thickness in First-Episode Depression: Evidence for Trait-Related Differences in Mood Regulation. Am. J. Psychiatry 2013, 170, 1477–1486. [Google Scholar] [CrossRef]
- Yao, Z.; Zou, Y.; Zheng, W.; Zhang, Z.; Li, Y.; Yu, Y.; Zhang, Z.; Fu, Y.; Shi, J.; Zhang, W.; et al. Structural Alterations of the Brain Preceded Functional Alterations in Major Depressive Disorder Patients: Evidence from Multimodal Connectivity. J. Affect. Disord. 2019, 253, 107–117. [Google Scholar] [CrossRef]
- Peng, W.; Chen, Z.; Yin, L.; Jia, Z.; Gong, Q. Essential Brain Structural Alterations in Major Depressive Disorder: A Voxel-Wise Meta-Analysis on First Episode, Medication-Naive Patients. J. Affect. Disord. 2016, 199, 114–123. [Google Scholar] [CrossRef]
- Phillips, J.L.; Batten, L.A.; Tremblay, P.; Aldosary, F.; Blier, P. A Prospective, Longitudinal Study of the Effect of Remission on Cortical Thickness and Hippocampal Volume in Patients with Treatment-Resistant Depression. Int. J. Neuropsychopharmacol. 2015, 18, pyv037. [Google Scholar] [CrossRef]
- Hurley, R.A.; Hayman, L.A.; Taber, K.H.; Wen, C.; Khan, A. The Limbic Thalamus. J. Neuropsychiatry Clin. Neurosci. 2004, 16, 127–132. [Google Scholar] [CrossRef]
- Gent, T.C.; la Bassetti, C.; Adamantidis, A.R. Sleep-Wake Control and the Thalamus. Curr. Opin. Neurobiol. 2018, 52, 188–197. [Google Scholar] [CrossRef]
- Zhang, H.; Li, L.; Wu, M.; Chen, Z.; Hu, X.; Chen, Y.; Zhu, H.; Jia, Z.; Gong, Q. Brain Gray Matter Alterations in First Episodes of Depression: A Meta-Analysis of Whole-Brain Studies. Neurosci. Biobehav. Rev. 2016, 60, 43–50. [Google Scholar] [CrossRef]
- Lu, Y.; Liang, H.; Han, D.; Mo, Y.; Li, Z.; Cheng, Y.; Xu, X.; Shen, Z.; Tan, C.; Zhao, W.; et al. The Volumetric and Shape Changes of the Putamen and Thalamus in First Episode, Untreated Major Depressive Disorder. NeuroImage Clin. 2016, 11, 658–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmaal, L.; Veltman, D.J.; van Erp, T.G.M.; Smann, P.G.; Frodl, T.; Jahanshad, N.; Loehrer, E.; Tiemeier, H.; Hofman, A.; Niessen, W.J.; et al. Subcortical Brain Alterations in Major Depressive Disorder: Findings from the ENIGMA Major Depressive Disorder Working Group. Mol. Psychiatry 2015, 21, 806–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frodl, T.; O’Keane, V. How Does the Brain Deal with Cumulative Stress? A Review with Focus on Developmental Stress, HPA Axis Function and Hippocampal Structure in Humans. Neurobiol. Dis. 2013, 52, 24–37. [Google Scholar] [CrossRef]
- Zhang, B.; Qi, S.; Liu, S.; Liu, X.; Wei, X.; Ming, D. Altered Spontaneous Neural Activity in the Precuneus, Middle and Superior Frontal Gyri, and Hippocampus in College Students with Subclinical Depression. BMC Psychiatry 2021, 21, 280. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Monteggia, L.M. A Neurotrophic Model for Stress-Related Mood Disorders. Biol. Psychiatry 2006, 59, 1116–1127. [Google Scholar] [CrossRef]
- Huang, E.J.; Reichardt, L.F. Neurotrophins: Roles in Neuronal Development and Function. Annu. Rev. Neurosci. 2001, 24, 677–736. [Google Scholar] [CrossRef] [Green Version]
- Lu, B.; Nagappan, G.; Lu, Y. BDNF and Synaptic Plasticity, Cognitive Function, and Dysfunction. Handb. Exp. Pharmacol. 2014, 220, 223–250. [Google Scholar] [CrossRef]
- Jaggar, M.; Fanibunda, S.E.; Ghosh, S.; Duman, R.S.; Vaidya, V.A. The Neurotrophic Hypothesis of Depression Revisited: New Insights and Therapeutic Implications. Neurobiol. Depress. Road Nov. Ther. 2019, 43–62. [Google Scholar] [CrossRef]
- Duman, C.H.; Duman, R.S. Spine Synapse Remodeling in the Pathophysiology and Treatment of Depression. Neurosci. Lett. 2015, 601, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, N.A.L.; del Ángel, D.S.; Olguín, H.J.; Silva, M.L. Neuroprogression: The Hidden Mechanism of Depression. Neuropsychiatr. Dis. Treat. 2018, 14, 2837–2845. [Google Scholar] [CrossRef] [Green Version]
- Hirschfeld, R.M.A. History and Evolution of the Monoamine Hypothesis of Depression. J. Clin. Psychiatry 2000, 61, 4–6. [Google Scholar] [PubMed]
- Fakhoury, M. Revisiting the Serotonin Hypothesis: Implications for Major Depressive Disorders. Mol. Neurobiol. 2016, 53, 2778–2786. [Google Scholar] [CrossRef] [PubMed]
- Maletic, V.; Eramo, A.; Gwin, K.; Offord, S.J.; Duffy, R.A. The Role of Norepinephrine and Its α-Adrenergic Receptors in the Pathophysiology and Treatment of Major Depressive Disorder and Schizophrenia: A Systematic Review. Front. Psychiatry 2017, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Belujon, P.; Grace, A.A. Dopamine System Dysregulation in Major Depressive Disorders. Int. J. Neuropsychopharmacol. 2017, 20, 1036–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pytka, K.; Dziubina, A.; Młyniec, K.; Dziedziczak, A.; Zmudzka, E.; Furgała, A.; Olczyk, A.; Sapa, J.; Filipek, B. The Role of Glutamatergic, GABA-Ergic, and Cholinergic Receptors in Depression and Antidepressant-like Effect. Pharmacol. Rep. 2016, 68, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Neumann, I.D.; Neumann, I.D. Brain Oxytocin: A Key Regulator of Emotional and Social Behaviours in Both Females and Males. J. Neuroendocrinol. 2008, 20, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Landgraf, R.; Neumann, I.D. Vasopressin and Oxytocin Release within the Brain: A Dynamic Concept of Multiple and Variable Modes of Neuropeptide Communication. Front. Neuroendocrinol. 2004, 25, 150–176. [Google Scholar] [CrossRef]
- Neumann, I.D.; Landgraf, R. Balance of Brain Oxytocin and Vasopressin: Implications for Anxiety, Depression, and Social Behaviors. Trends Neurosci. 2012, 35, 649–659. [Google Scholar] [CrossRef]
- Postal, M.; Appenzeller, S. The Importance of Cytokines and Autoantibodies in Depression. Autoimmun. Rev. 2015, 14, 30–35. [Google Scholar] [CrossRef]
- Wohleb, E.S.; Franklin, T.; Iwata, M.; Duman, R.S. Integrating Neuroimmune Systems in the Neurobiology of Depression. Nat. Rev. Neurosci. 2016, 17, 497–511. [Google Scholar] [CrossRef]
- Schirmer, M.; Smeekens, S.P.; Vlamakis, H.; Jaeger, M.; Oosting, M.; Franzosa, E.A.; Jansen, T.; Jacobs, L.; Bonder, M.J.; Kurilshikov, A.; et al. Linking the Human Gut Microbiome to Inflammatory Cytokine Production Capacity. Cell 2016, 167, 1125–1136.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peirce, J.M.; Alviña, K. The Role of Inflammation and the Gut Microbiome in Depression and Anxiety. J. Neurosci. Res. 2019, 97, 1223–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvarez-Mon, M.A.; Gomez-Lahoz, A.M.; Orozco, A.; Lahera, G.; Sosa-Reina, M.D.; Diaz, D.; Albillos, A.; Quintero, J.; Molero, P.; Monserrat, J.; et al. Blunted Expansion of Regulatory T Lymphocytes Is Associated With Increased Bacterial Translocation in Patients With Major Depressive Disorder. Front. Psychiatry 2021, 11, 591962. [Google Scholar] [CrossRef]
- Steiger, A.; Pawlowski, M. Depression and Sleep. Int. J. Mol. Sci. 2019, 20, 607. [Google Scholar] [CrossRef] [Green Version]
- Riemann, D.; Krone, L.B.; Wulff, K.; Nissen, C. Sleep, Insomnia, and Depression. Neuropsychopharmacology 2019, 45, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Dhabhar, F.S.; James, S.J.; Hough, C.M.; Jain, F.A.; Bersani, F.S.; Reus, V.I.; Verhoeven, J.E.; Epel, E.S.; Mahan, L.; et al. Oxidative Stress, Inflammation and Treatment Response in Major Depression. Psychoneuroendocrinology 2017, 76, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mellon, S.H.; Wolkowitz, O.M.; Schonemann, M.D.; Epel, E.S.; Rosser, R.; Burke, H.B.; Mahan, L.; Reus, V.I.; Stamatiou, D.; Liew, C.C.; et al. Alterations in Leukocyte Transcriptional Control Pathway Activity Associated with Major Depressive Disorder and Antidepressant Treatment. Transl. Psychiatry 2016, 6, e821. [Google Scholar] [CrossRef] [Green Version]
- Seney, M.L.; Huo, Z.; Cahill, K.; French, L.; Puralewski, R.; Zhang, J.; Logan, R.W.; Tseng, G.; Lewis, D.A.; Sibille, E. Opposite Molecular Signatures of Depression in Men and Women. Biol. Psychiatry 2018, 84, 18–27. [Google Scholar] [CrossRef]
- Majd, M.; Graham-Engeland, J.E.; Smyth, J.M.; Sliwinski, M.J.; Lipton, R.B.; Katz, M.J.; Engeland, C.G. Distinct Inflammatory Response Patterns Are Evident among Men and Women with Higher Depressive Symptoms. Physiol. Behav. 2018, 184, 108–115. [Google Scholar] [CrossRef]
- Cyranowski, J.M.; Marsland, A.L.; Bromberger, J.T.; Whiteside, T.L.; Chang, Y.; Matthews, K.A. Depressive Symptoms and Production of Proinflammatory Cytokines by Peripheral Blood Mononuclear Cells Stimulated in Vitro. Brain Behav. Immun. 2007, 21, 229–237. [Google Scholar] [CrossRef]
- Chen, J.J.; Zheng, P.; Liu, Y.Y.; Zhong, X.G.; Wang, H.Y.; Guo, Y.J.; Xie, P. Sex Differences in Gut Microbiota in Patients with Major Depressive Disorder. Neuropsychiatr. Dis. Treat. 2018, 14, 647–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores, R.; Shi, J.; Fuhrman, B.; Xu, X.; Veenstra, T.D.; Gail, M.H.; Gajer, P.; Ravel, J.; Goedert, J.J. Fecal Microbial Determinants of Fecal and Systemic Estrogens and Estrogen Metabolites: A Cross-Sectional Study. J. Transl. Med. 2012, 10, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plottel, C.S.; Blaser, M.J. Microbiome and Malignancy. Cell Host Microbe 2011, 10, 324–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahokas, A.; Kaukoranta, J.; Aito, M. Estrogen Deficiency in Severe Postpartum Depression: Successful Treatment with Sublingual Physiologic 17β-Estradiol: A Preliminary Study. J. Clin. Psychiatry 2001, 62, 332–336. [Google Scholar] [CrossRef]
- Parker, G.B.; Brotchie, H.L. From Diathesis to Dimorphism: The Biology of Gender Differences in Depression. J. Nerv. Ment. Dis. 2004, 192, 210–216. [Google Scholar] [CrossRef]
- Solomon, M.B.; Herman, J.P. Sex Differences in Psychopathology: Of Gonads, Adrenals and Mental Illness. Physiol. Behav. 2009, 97, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Newhouse, P.; Albert, K. Estrogen, Stress, and Depression: A Neurocognitive Model. JAMA Psychiatry 2015, 72, 727–729. [Google Scholar] [CrossRef]
- Santos-Marcos, J.A.; Rangel-Zuñiga, O.A.; Jimenez-Lucena, R.; Quintana-Navarro, G.M.; Garcia-Carpintero, S.; Malagon, M.M.; Landa, B.B.; Tena-Sempere, M.; Perez-Martinez, P.; Lopez-Miranda, J.; et al. Influence of Gender and Menopausal Status on Gut Microbiota. Maturitas 2018, 116, 43–53. [Google Scholar] [CrossRef]
- Audet, M.C. Stress-Induced Disturbances along the Gut Microbiota-Immune-Brain Axis and Implications for Mental Health: Does Sex Matter? Front. Neuroendocrinol. 2019, 54, 100772. [Google Scholar] [CrossRef]
- Sovijit, W.N.; Sovijit, W.E.; Pu, S.; Usuda, K.; Inoue, R.; Watanabe, G.; Yamaguchi, H.; Nagaoka, K. Ovarian Progesterone Suppresses Depression and Anxiety-like Behaviors by Increasing the Lactobacillus Population of Gut Microbiota in Ovariectomized Mice. Neurosci. Res. 2021, 168, 76–82. [Google Scholar] [CrossRef]
- Rapkin, A.J.; Akopians, A.L. Pathophysiology of Premenstrual Syndrome and Premenstrual Dysphoric Disorder. Menopause Int. 2012, 18, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Geng, X.; Li, Z.; Xu, K.; Hu, M.; Wu, H.; Shi, W.; Qiao, M. A Forced Swim-Based Rat Model of Premenstrual Depression: Effects of Hormonal Changes and Drug Intervention. Aging 2020, 12, 24357–24370. [Google Scholar] [CrossRef] [PubMed]
- Schüle, C.; Nothdurfter, C.; Rupprecht, R. The Role of Allopregnanolone in Depression and Anxiety. Prog. Neurobiol. 2014, 113, 79–87. [Google Scholar] [CrossRef]
- Willi, J.; Süss, H.; Grub, J.; Ehlert, U. Biopsychosocial Predictors of Depressive Symptoms in the Perimenopause-Findings from the Swiss Perimenopause Study. Menopause 2021, 28, 247–254. [Google Scholar] [CrossRef] [PubMed]
- de Wit, A.E.; Giltay, E.J.; de Boer, M.K.; Nathan, M.; Wiley, A.; Crawford, S.; Joffe, H. Predictors of Irritability Symptoms in Mildly Depressed Perimenopausal Women. Psychoneuroendocrinology 2021, 126, 105128. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.E.; Pollak, S.D. Early life stress and development: Potential mechanisms for adverse outcomes. J. Neurodev. Disord. 2020, 12, 34. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhao, Y.; Wang, Y.; Liu, L.; Zhang, X.; Li, B.; Cui, R. The Effects of Psychological Stress on Depression. Curr. Neuropharmacol. 2015, 13, 494–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syed, S.A.; Nemeroff, C.B. Early Life Stress, Mood, and Anxiety Disorders. Chronic Stress 2017, 1, 2470547017694461. [Google Scholar] [CrossRef]
- Goodwill, H.L.; Manzano-Nieves, G.; Gallo, M.; Lee, H.I.; Oyerinde, E.; Serre, T.; Bath, K.G. Early life stress leads to sex differences in development of depressive-like outcomes in a mouse model. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2019, 44, 711–720. [Google Scholar] [CrossRef]
- Spyrka, J.; Gugula, A.; Rak, A.; Tylko, G.; Hess, G.; Blasiak, A. Early life stress-induced alterations in the activity and morphology of ventral tegmental area neurons in female rats. Neurobiol. Stress 2020, 13, 100250. [Google Scholar] [CrossRef]
- Loi, M.; Mossink, J.C.; Meerhoff, G.F.; Den Blaauwen, J.L.; Lucassen, P.J.; Joëls, M. Effects of early-life stress on cognitive function and hippocampal structure in female rodents. Neuroscience 2017, 342, 101–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammen, C.; Kim, E.Y.; Eberhart, N.K.; Brennan, P.A. Chronic and acute stress and the prediction of major depression in women. Depress. Anxiety 2009, 26, 718–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammen, C. Interpersonal stress and depression in women. J. Affect. Disord. 2003, 74, 49–57. [Google Scholar] [CrossRef]
- Hammen, C. Social stress and women’s risk for recurrent depression. Arch. Women’s Ment. Health 2003, 6, 9–13. [Google Scholar] [CrossRef]
- Holden, K.B.; Hall, S.P.; Robinson, M.; Triplett, S.; Babalola, D.; Plummer, V.; Treadwell, H.; Bradford, L.D. Psychosocial and sociocultural correlates of depressive symptoms among diverse African American women. J. Natl. Med. Assoc. 2012, 104, 493–504. [Google Scholar] [CrossRef] [Green Version]
- Falicov, C.J. Culture, society and gender in depression. J. Fam. Ther. 2003, 25, 371–387. [Google Scholar] [CrossRef]
- Jambunathan, J. Sociocultural factors in depression in Asian Indian women. Health Care Women Int. 1992, 13, 261–270. [Google Scholar] [CrossRef]
- Farid, D.; Li, P.; Da Costa, D.; Afif, W.; Szabo, J.; Dasgupta, K.; Rahme, E. Undiagnosed depression, persistent depressive symptoms and seeking mental health care: Analysis of immigrant and non-immigrant participants of the Canadian Longitudinal Study of Aging. Epidemiol. Psychiatr. Sci. 2020, 29, e158. [Google Scholar] [CrossRef]
- Yussuf, F. Immigrant Women: Risk and Protective Factors Associated with Depression and Anxiety Disorders. Master’s Thesis, Wright State University, Dayton, OH, USA, 2015. [Google Scholar]
- Kim, J.; Richardson, V.; Park, M. A Multilevel Perspective on Gender Differences in the Relationship Between Poverty Status and Depression Among Older Adults in the United States. J. Women Aging 2013, 25, 207–226. [Google Scholar] [CrossRef]
- Humeniuk, E.; Bojar, I.; Owoc, A.; Wojtyła, A.; Fronczak, A. Psychosocial conditioning of depressive disorders in post-menopausal women. Ann. Agric. Environ. Med. 2011, 18, 441–445. [Google Scholar]
- O’Campo, P.; Eaton, W.; Muntaner, C. Labor market experience, work organization, gender inequalities and health status: Results from a prospective analysis of US employed women. Soc. Sci. Med. 2004, 58, 585–594. [Google Scholar] [CrossRef]
- Silva, M.; Loureiro, A.; Cardoso, G. Social determinants of mental health: A review of the evidence. Eur. J. Psychiatry 2016, 30, 259–292. [Google Scholar]
- Cutrona, C.E.; Russell, D.W.; Brown, P.A.; Clark, L.A.; Hessling, R.M.; Gardner, K.A. Neighborhood context, personality, and stressful life events as predictors of depression among African American women. J. Abnorm. Psychol. 2005, 114, 3–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keita, G.P. Psychosocial and cultural contributions to depression in women: Considerations for women midlife and beyond. J. Manag. Care Pharm. 2007, 13 (Suppl. SA), S12–S15. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, J.C.; Schmidt, S.L. DSM-5 Criteria and Depression Severity: Implications for Clinical Practice. Front. Psychiatry 2018, 9, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, M.; Martinez, J.H.; Young, D.; Chelminski, I.; Dalrymple, K. Severity Classification on the Hamilton Depression Rating Scale. J. Affect. Disord. 2013, 150, 384–388. [Google Scholar] [CrossRef]
- Davidson, J.R.T. Major Depressive Disorder Treatment Guidelines in America and Europe. J. Clin. Psychiatry 2010, 71, 27767. [Google Scholar] [CrossRef]
- Cuijpers, P.; Quero, S.; Dowrick, C.; Arroll, B. Psychological Treatment of Depression in Primary Care: Recent Developments. Curr. Psychiatry Rep. 2019, 21, 129. [Google Scholar] [CrossRef] [Green Version]
- Voineskos, D.; Daskalakis, Z.J.; Blumberger, D.M. Management of Treatment-Resistant Depression: Challenges and Strategies. Neuropsychiatr. Dis. Treat. 2020, 16, 221–234. [Google Scholar] [CrossRef] [Green Version]
- Dwyer, J.B.; Aftab, A.; Widge, A.; Rodriguez, C.I.; Carpenter, L.L.; Nemeroff, C.B.; McDonald, W.M.; Kalin, N.H. Hormonal Treatments for Major Depressive Disorder: State of the Art. Am. J. Psychiatry 2020, 177, 686–705. [Google Scholar] [CrossRef] [PubMed]
- Rotermann, M.; Sanmartin, C.; Hennessy, D.; Arthur, M. Prescription Medication Use by Canadians Aged 6 to 79. Health Rep. 2014, 6, 3–9. [Google Scholar]
- Perugi, G.; Musetti, L.; Simonini, E.; Piagentini, F.; Cassano, G.B.; Akiskal, H.S. Gender-Mediated Clinical Features of Depressive Illness the Importance of Temperamental Differences. Br. J. Psychiatry 1990, 157, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McGonagle, K.A.; Nelson, C.B.; Hughes, M.; Swartz, M.; Blazer, D.G. Sex and Depression in the National Comorbidity Survey. II: Cohort Effects. J. Affect. Disord. 1994, 30, 15–26. [Google Scholar] [CrossRef] [Green Version]
- Marcus, S.M.; Young, E.A.; Kerber, K.B.; Kornstein, S.; Farabaugh, A.H.; Mitchell, J.; Wisniewski, S.R.; Balasubramani, G.K.; Trivedi, M.H.; Rush, A.J. Gender Differences in Depression: Findings from the STAR*D Study. J. Affect. Disord. 2005, 87, 141–150. [Google Scholar] [CrossRef]
- Marcus, S.M.; Kerber, K.B.; Rush, A.J.; Wisniewski, S.R.; Nierenberg, A.; Balasubramani, G.K.; Ritz, L.; Kornstein, S.; Young, E.A.; Trivedi, M.H. Sex Differences in Depression Symptoms in Treatment-Seeking Adults: Confirmatory Analyses from the Sequenced Treatment Alternatives to Relieve Depression Study. Compr. Psychiatry 2008, 49, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Sramek, J.J.; Murphy, M.F.; Cutler, N.R. Sex Differences in the Psychopharmacological Treatment of Depression. Dialogues Clin. Neurosci. 2016, 18, 447–457. [Google Scholar] [CrossRef]
- Gordon, J.I.; Dewey, K.G.; Mills, D.A.; Medzhitov, R.M. The Human Gut Microbiota and Undernutrition. Sci. Transl. Med. 2012, 4, 137ps12. [Google Scholar] [CrossRef] [Green Version]
- Correia, J.; Ravasco, P. Weight Changes in Portuguese Patients with Depression: Which Factors Are Involved? Nutr. J. 2014, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, Obesity, and Depression: A Systematic Review and Meta-Analysis of Longitudinal Studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Gezahegn, E.; Edris, M.; Dachew, B.A. Prevalence and Factors Associated with Undernutrition among Adults with Major Depressive Disorder in Northwest Ethiopia. Psychiatry J. 2016, 2016, 7034582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, S.C.; Mikhail, M.E.; Keel, P.K.; Burt, S.A.; Neale, M.C.; Boker, S.; Klump, K.L. Increased Rates of Eating Disorders and Their Symptoms in Women with Major Depressive Disorder and Anxiety Disorders. Int. J. Eat. Disord. 2020, 53, 1844–1854. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Michels, N.; Sioen, I.; Ruige, J.; de Henauw, S. Children’s Psychosocial Stress and Emotional Eating: A Role for Leptin? Int. J. Eat. Disord. 2017, 50, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Ma, R.; Mikhail, M.E.; Culbert, K.M.; Johnson, A.W.; Sisk, C.L.; Klump, K.L. Ovarian Hormones and Reward Processes in Palatable Food Intake and Binge Eating. Physiology 2020, 35, 69–78. [Google Scholar] [CrossRef]
- Fassino, S.; Pierò, A.; Gramaglia, C.; Abbate-Daga, G. Clinical, Psychopathological and Personality Correlates of Interoceptive Awareness in Anorexia Nervosa, Bulimia Nervosa and Obesity. Psychopathology 2004, 37, 168–174. [Google Scholar] [CrossRef]
- Rao, T.S.S.; Asha, M.R.; Ramesh, B.N.; Rao, K.S.J. Understanding Nutrition, Depression and Mental Illnesses. Indian J. Psychiatry 2008, 50, 77–82. [Google Scholar] [CrossRef]
- Potter, G.G.; McQuoid, D.R.; Steffens, D.C. Appetite Loss and Neurocognitive Deficits in Late-Life Depression. Int. J. Geriatr. Psychiatry 2015, 30, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Loo, R.S.X.; Yap, F.; Ku, C.W.; Cheung, Y.B.; Tan, K.H.; Chan, J.K.Y.; Loy, S.L. Maternal Meal Irregularities during Pregnancy and Lifestyle Correlates. Appetite 2022, 168, 105747. [Google Scholar] [CrossRef]
- Simmons, W.K.; Burrows, K.; Avery, J.A.; Kerr, K.L.; Bodurka, J.; Savage, C.R.; Drevets, W.C. Depression-Related Increases and Decreases in Appetite: Dissociable Patterns of Aberrant Activity in Reward and Interoceptive Neurocircuitry. Am. J. Psychiatry 2016, 173, 418–428. [Google Scholar] [CrossRef]
- Muth, A.K.; Park, S.Q. The Impact of Dietary Macronutrient Intake on Cognitive Function and the Brain. Clin. Nutr. 2021, 40, 3999–4010. [Google Scholar] [CrossRef]
- Gorczyca, A.M.; Sjaarda, L.A.; Mitchell, E.M.; Perkins, N.J.; Schliep, K.C.; Wactawski-Wende, J.; Mumford, S.L. Changes in Macronutrient, Micronutrient, and Food Group Intakes throughout the Menstrual Cycle in Healthy, Premenopausal Women. Eur. J. Nutr. 2016, 55, 1181–1188. [Google Scholar] [CrossRef]
- Dalvit-McPhillips, S.P. The Effect of the Human Menstrual Cycle on Nutrient Intake. Physiol. Behav. 1983, 31, 209–212. [Google Scholar] [CrossRef]
- Butera, P.C. Estradiol and the Control of Food Intake. Physiol. Behav. 2010, 99, 175–180. [Google Scholar] [CrossRef] [Green Version]
- Markus, C.R. Effects of Carbohydrates on Brain Tryptophan Availability and Stress Performance. Biol. Psychol. 2007, 76, 83–90. [Google Scholar] [CrossRef]
- Peng, Y.F.; Zhong, S.M.; Qin, Y.H. The Relationship between Major Depressive Disorder and Glucose Parameters: A Cross-Sectional Study in a Chinese Population. Adv. Clin. Exp. Med. Off. Organ Wroc. Med. Univ. 2017, 26, 665–669. [Google Scholar] [CrossRef] [Green Version]
- Koponen, H.; Kautiainen, H.; Leppänen, E.; Mäntyselkä, P.; Vanhala, M. Association between Suicidal Behaviour and Impaired Glucose Metabolism in Depressive Disorders. BMC Psychiatry 2015, 15, 163. [Google Scholar] [CrossRef] [Green Version]
- Su, H.; Zuo, C.; Zhang, H.; Jiao, F.; Zhang, B.; Tang, W.; Geng, D.; Guan, Y.; Shi, S. Regional Cerebral Metabolism Alterations Affect Resting-State Functional Connectivity in Major Depressive Disorder. Quant. Imaging Med. Surg. 2018, 8, 910–924. [Google Scholar] [CrossRef]
- Mantantzis, K.; Schlaghecken, F.; Sünram-Lea, S.I.; Maylor, E.A. Sugar Rush or Sugar Crash? A Meta-Analysis of Carbohydrate Effects on Mood. Neurosci. Biobehav. Rev. 2019, 101, 45–67. [Google Scholar] [CrossRef] [Green Version]
- Winwood-Smith, H.S.; Franklin, C.E.; White, C.R. Low-Carbohydrate Diet Induces Metabolic Depression: A Possible Mechanism to Conserve Glycogen. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 313, R347–R356. [Google Scholar] [CrossRef] [Green Version]
- Houghton, S.C.; Manson, J.E.; Whitcomb, B.W.; Hankinson, S.E.; Troy, L.M.; Bigelow, C.; Bertone-Johnson, E.R. Carbohydrate and Fiber Intake and the Risk of Premenstrual Syndrome. Eur. J. Clin. Nutr. 2018, 72, 861–870. [Google Scholar] [CrossRef]
- Murakami, K.; Sasaki, S.; Takahashi, Y.; Uenishi, K.; Watanabe, T.; Kohri, T.; Yamasaki, M.; Watanabe, R.; Baba, K.; Shibata, K.; et al. Dietary Glycemic Index Is Associated with Decreased Premenstrual Symptoms in Young Japanese Women. Nutrition 2008, 24, 554–561. [Google Scholar] [CrossRef]
- Minobe, N.; Murakami, K.; Kobayashi, S.; Suga, H.; Sasaki, S. Higher Dietary Glycemic Index, but Not Glycemic Load, Is Associated with a Lower Prevalence of Depressive Symptoms in a Cross-Sectional Study of Young and Middle-Aged Japanese Women. Eur. J. Nutr. 2018, 57, 2261–2273. [Google Scholar] [CrossRef]
- Rahimlou, M.; Morshedzadeh, N.; Karimi, S.; Jafarirad, S. Association between Dietary Glycemic Index and Glycemic Load with Depression: A Systematic Review. Eur. J. Nutr. 2018, 57, 2333–2340. [Google Scholar] [CrossRef]
- Salari-Moghaddam, A.; Larijani, B.; Esmaillzadeh, A. Review of Earlier Evidence on Dietary Glycemic Index and Load and Depression Needs Further Attention. Eur. J. Nutr. 2018, 57, 2341–2342. [Google Scholar] [CrossRef]
- Sparling, T.M.; Henschke, N.; Nesbitt, R.C.; Gabrysch, S. The Role of Diet and Nutritional Supplementation in Perinatal Depression: A Systematic Review. Matern. Child Nutr. 2017, 13, e12235. [Google Scholar] [CrossRef]
- Khan, R.; Waqas, A.; Bilal, A.; Mustehsan, Z.H.; Omar, J.; Rahman, A. Association of Maternal Depression with Diet: A Systematic Review. Asian J. Psychiatry 2020, 52, 102098. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Hale, L.; Garcia, L.; Malaspina, D.; Opler, M.G.; Payne, M.E.; Rossom, R.C.; Lane, D. High Glycemic Index Diet as a Risk Factor for Depression: Analyses from the Women’s Health Initiative. Am. J. Clin. Nutr. 2015, 102, 454–463. [Google Scholar] [CrossRef] [Green Version]
- Colangelo, L.A.; Craft, L.L.; Ouyang, P.; Liu, K.; Schreiner, P.J.; Michos, E.D.; Gapstur, S.M. Association of Sex Hormones and Sex Hormone-Binding Globulin with Depressive Symptoms in Postmenopausal Women: The Multiethnic Study of Atherosclerosis. Menopause 2012, 19, 877–885. [Google Scholar] [CrossRef] [Green Version]
- Wu, G. Dietary Protein Intake and Human Health. Food Funct. 2016, 7, 1251–1265. [Google Scholar] [CrossRef] [Green Version]
- Belluscio, L.M.; Berardino, B.G.; Ferroni, N.M.; Ceruti, J.M.; Cánepa, E.T. Early Protein Malnutrition Negatively Impacts Physical Growth and Neurological Reflexes and Evokes Anxiety and Depressive-like Behaviors. Physiol. Behav. 2014, 129, 237–254. [Google Scholar] [CrossRef]
- Belluscio, L.M.; Alberca, C.D.; Pregi, N.; Cánepa, E.T. Altered Gene Expression in Hippocampus and Depressive-like Behavior in Young Adult Female Mice by Early Protein Malnutrition. Genes Brain Behav. 2016, 15, 741–749. [Google Scholar] [CrossRef]
- Wolfe, A.R.; Arroyo, C.; Tedders, S.H.; Li, Y.; Dai, Q.; Zhang, J. Dietary Protein and Protein-Rich Food in Relation to Severely Depressed Mood: A 10 Year Follow-up of a National Cohort. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 232–238. [Google Scholar] [CrossRef]
- Houghton, S.C.; Manson, J.A.E.; Whitcomb, B.W.; Hankinson, S.E.; Troy, L.M.; Bigelow, C.; Bertone-Johnson, E.R. Protein Intake and the Risk of Premenstrual Syndrome. Public Health Nutr. 2019, 22, 1762–1769. [Google Scholar] [CrossRef]
- Bennett, E.; Peters, S.A.E.; Woodward, M. Sex Differences in Macronutrient Intake and Adherence to Dietary Recommendations: Findings from the UK Biobank. BMJ Open 2018, 8, e020017. [Google Scholar] [CrossRef]
- Ge, Y.; Liu, W.; Tao, H.; Zhang, Y.; Liu, L.; Liu, Z.; Qiu, B.; Xu, T. Effect of Industrial Trans-Fatty Acids-Enriched Diet on Gut Microbiota of C57BL/6 Mice. Eur. J. Nutr. 2019, 58, 2625–2638. [Google Scholar] [CrossRef]
- Li, D.; Tong, Y.; Li, Y. Associations of Dietary Trans Fatty Acid Intake with Depressive Symptoms in Midlife Women. J. Affect. Disord. 2020, 260, 194–199. [Google Scholar] [CrossRef]
- Calder, P.C.; Albers, R.; Antoine, J.M.; Blum, S.; Bourdet-Sicard, R.; Ferns, G.A.; Folkerts, G.; Friedmann, P.S.; Frost, G.S.; Guarner, F.; et al. Inflammatory Disease Processes and Interactions with Nutrition. Br. J. Nutr. 2009, 101, 1–45. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, F.T.; Dias, V.T.; Roversi, K.; Vey, L.T.; de Freitas, D.L.; Pase, C.S.; Roversi, K.; Veit, J.C.; Emanuelli, T.; Bürger, M.E. Cross-Generational Trans Fat Consumption Favors Self-Administration of Amphetamine and Changes Molecular Expressions of BDNF, DAT, and D1/D2 Receptors in the Cortex and Hippocampus of Rats. Neurotox. Res. 2015, 28, 319–331. [Google Scholar] [CrossRef]
- Deacon, G.; Kettle, C.; Hayes, D.; Dennis, C.; Tucci, J. Omega 3 Polyunsaturated Fatty Acids and the Treatment of Depression. Crit. Rev. Food Sci. Nutr. 2017, 57, 212–223. [Google Scholar] [CrossRef]
- Park, S.J.; Lee, D.K.; Kim, B.; Na, K.S.; Lee, C.H.; Son, Y.D.; Lee, H.J. The Association between Omega-3 Fatty Acid Intake and Human Brain Connectivity in Middle-Aged Depressed Women. Nutrients 2020, 12, 2191. [Google Scholar] [CrossRef]
- Zhang, M.M.; Zou, Y.; Li, S.M.; Wang, L.; Sun, Y.H.; Shi, L.; Lu, L.; Bao, Y.P.; Li, S.X. The Efficacy and Safety of Omega-3 Fatty Acids on Depressive Symptoms in Perinatal Women: A Meta-Analysis of Randomized Placebo-Controlled Trials. Transl. Psychiatry 2020, 10, 193. [Google Scholar] [CrossRef]
- Sohrabi, N.; Kashanian, M.; Ghafoori, S.S.; Malakouti, S.K. Evaluation of the Effect of Omega-3 Fatty Acids in the Treatment of Premenstrual Syndrome: “A Pilot Trial”. Complement. Ther. Med. 2013, 21, 141–146. [Google Scholar] [CrossRef]
- Freeman, M.P.; Hibbeln, J.R.; Silver, M.; Hirschberg, A.M.; Wang, B.; Yule, A.M.; Petrillo, L.F.; Pascuillo, E.; Economou, N.I.; Joffe, H.; et al. Omega-3 Fatty Acids for Major Depressive Disorder Associated with the Menopausal Transition: A Preliminary Open Trial. Menopause 2011, 18, 279–284. [Google Scholar] [CrossRef] [Green Version]
- Simopoulos, A.P.; Simopoulos, A.P. Evolutionary Aspects of the Dietary Omega-6/Omega-3 Fatty Acid Ratio: Medical Implications. In Evolutionary Thinking in Medicine; Springer: Cham, Switzerland, 2016; pp. 119–134. [Google Scholar] [CrossRef]
- de Sousa, T.M.; dos Santos, L.C. Dietary Fatty Acids, Omega-6/Omega-3 Ratio and Cholesterol Intake Associated with Depressive Symptoms in Low-Risk Pregnancy. Nutr. Neurosci. 2020, 25, 642–647. [Google Scholar] [CrossRef]
- De Vriese, S.R.; Christophe, A.B.; Maes, M. Lowered serum n-3 polyunsaturated fatty acid (PUFA) levels predict the occurrence of postpartum depression: Further evidence that lowered n-PUFAs are related to major depression. Life Sci. 2003, 73, 3181–3187. [Google Scholar] [CrossRef]
- Lotrich, F.E.; Sears, B.; McNamara, R.K. Elevated Ratio of Arachidonic Acid to Long-Chain Omega-3 Fatty Acids Predicts Depression Development Following Interferon-Alpha Treatment: Relationship with Interleukin-6. Brain Behav. Immun. 2013, 31, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Anjum, I.; Jaffery, S.S.; Fayyaz, M.; Samoo, Z.; Anjum, S. The Role of Vitamin D in Brain Health: A Mini Literature Review. Cureus 2018, 10, e2960. [Google Scholar] [CrossRef] [Green Version]
- Lardner, A.L. Vitamin D and Hippocampal Development-the Story so Far. Front. Mol. Neurosci. 2015, 8, 58. [Google Scholar] [CrossRef] [Green Version]
- Berridge, M.J. Vitamin D and Depression: Cellular and Regulatory Mechanisms. Pharmacol. Rev. 2017, 69, 80–92. [Google Scholar] [CrossRef] [Green Version]
- Libuda, L.; Laabs, B.H.; Ludwig, C.; Bühlmeier, J.; Antel, J.; Hinney, A.; Naaresh, R.; Föcker, M.; Hebebrand, J.; König, I.R.; et al. Vitamin D and the Risk of Depression: A Causal Relationship? Findings from a Mendelian Randomization Study. Nutrients 2019, 11, 1085. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.S.; Jacques, P.F.; Rosenberg, I.H.; Selhub, J. Folate and Vitamin B-12 Status in Relation to Anemia, Macrocytosis, and Cognitive Impairment in Older Americans in the Age of Folic Acid Fortification. Am. J. Clin. Nutr. 2007, 85, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Sangle, P.; Sandhu, O.; Aftab, Z.; Anthony, A.T.; Khan, S. Vitamin B12 Supplementation: Preventing Onset and Improving Prognosis of Depression. Cureus 2020, 12, e11169. [Google Scholar] [CrossRef] [PubMed]
- Esnafoglu, E.; Ozturan, D.D. The Relationship of Severity of Depression with Homocysteine, Folate, Vitamin B12, and Vitamin D Levels in Children and Adolescents. Child Adolesc. Ment. Health 2020, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Bottiglieri, T. Homocysteine and Folate Metabolism in Depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 1103–1112. [Google Scholar] [CrossRef]
- Bhatia, P.; Singh, N. Homocysteine Excess: Delineating the Possible Mechanism of Neurotoxicity and Depression. Fundam. Clin. Pharmacol. 2015, 29, 522–528. [Google Scholar] [CrossRef]
- Szewczyk, B.; Szopa, A.; Serefko, A.; Poleszak, E.; Nowak, G. The Role of Magnesium and Zinc in Depression: Similarities and Differences. Magnes. Res. 2018, 31, 78–89. [Google Scholar] [CrossRef]
- Młyniec, K. Zinc in the Glutamatergic Theory of Depression. Curr. Neuropharmacol. 2015, 13, 505–513. [Google Scholar] [CrossRef] [Green Version]
- Doboszewska, U.; Wlaź, P.; Nowak, G.; Radziwoń-Zaleska, M.; Cui, R.; Młyniec, K. Zinc in the Monoaminergic Theory of Depression: Its Relationship to Neural Plasticity. Neural Plast. 2017, 2017, 3682752. [Google Scholar] [CrossRef]
- Brigelius-Flohé, R.; Flohé, L. Selenium and Redox Signaling. Arch. Biochem. Biophys. 2017, 617, 48–59. [Google Scholar] [CrossRef]
- Casaril, A.M.; Ignasiak, M.T.; Chuang, C.Y.; Vieira, B.; Padilha, N.B.; Carroll, L.; Lenardão, E.J.; Savegnago, L.; Davies, M.J. Selenium-Containing Indolyl Compounds: Kinetics of Reaction with Inflammation-Associated Oxidants and Protective Effect against Oxidation of Extracellular Matrix Proteins. Free Radic. Biol. Med. 2017, 113, 395–405. [Google Scholar] [CrossRef]
- Casaril, A.M.; Domingues, M.; Bampi, S.R.; de Andrade Lourenço, D.; Padilha, N.B.; Lenardão, E.J.; Sonego, M.; Seixas, F.K.; Collares, T.; Nogueira, C.W.; et al. The Selenium-Containing Compound 3-((4-Chlorophenyl)Selanyl)-1-Methyl-1H-Indole Reverses Depressive-like Behavior Induced by Acute Restraint Stress in Mice: Modulation of Oxido-Nitrosative Stress and Inflammatory Pathway. Psychopharmacology 2019, 236, 2867–2880. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, W.; Xin, X.; Song, X.; Zhang, D. Association of Total Zinc, Iron, Copper and Selenium Intakes with Depression in the US Adults. J. Affect. Disord. 2018, 228, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, B.; Song, X.; Zhang, D. Dietary Zinc and Iron Intake and Risk of Depression: A Meta-Analysis. Psychiatry Res. 2017, 251, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Wessling-Resnick, M. Iron and Mechanisms of Emotional Behavior. J. Nutr. Biochem. 2014, 25, 1101–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidese, S.; Saito, K.; Asano, S.; Kunugi, H. Association between Iron-Deficiency Anemia and Depression: A Web-Based Japanese Investigation. Psychiatry Clin. Neurosci. 2018, 72, 513–521. [Google Scholar] [CrossRef] [Green Version]
- Shah, H.E.; Bhawnani, N.; Ethirajulu, A.; Alkasabera, A.; Onyali, C.B.; Anim-Koranteng, C.; Mostafa, J.A. Iron Deficiency-Induced Changes in the Hippocampus, Corpus Striatum, and Monoamines Levels That Lead to Anxiety, Depression, Sleep Disorders, and Psychotic Disorders. Cureus 2021, 13, e18138. [Google Scholar] [CrossRef]
- Serefko, A.; Szopa, A.; Poleszak, E. Magnesium and Depression. Magnes. Res. 2016, 29, 112–119. [Google Scholar] [CrossRef]
- Lanza di Scalea, T.; Pearlstein, T. Premenstrual Dysphoric Disorder. Med. Clin. N. Am. 2019, 103, 613–628. [Google Scholar] [CrossRef]
- Rapkin, A.J.; Mikacich, J.A. Premenstrual Dysphoric Disorder and Severe Premenstrual Syndrome in Adolescents: Diagnosis and Pharmacological Treatment. Pediatric Drugs 2013, 15, 191–202. [Google Scholar] [CrossRef]
- Kia, A.S.; Amani, R.; Cheraghian, B. The Association between the Risk of Premenstrual Syndrome and Vitamin D, Calcium, and Magnesium Status among University Students: A Case Control. Health Promot. Perspect. 2015, 5, 225–230. [Google Scholar] [CrossRef] [Green Version]
- Arab, A.; Rafie, N.; Askari, G.; Taghiabadi, M. Beneficial Role of Calcium in Premenstrual Syndrome: A Systematic Review of Current Literature. Int. J. Prev. Med. 2020, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Bertone-Johnson, E.R.; Chocano-Bedoya, P.O.; Zagarins, S.E.; Micka, A.E.; Ronnenberg, A.G. Dietary Vitamin D Intake, 25-Hydroxyvitamin D3 Levels and Premenstrual Syndrome in a College-Aged Population. J. Steroid Biochem. Mol. Biol. 2010, 121, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Jafari, F.; Amani, R.; Tarrahi, M.J. Effect of Zinc Supplementation on Physical and Psychological Symptoms, Biomarkers of Inflammation, Oxidative Stress, and Brain-Derived Neurotrophic Factor in Young Women with Premenstrual Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2020, 194, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Jafari, F.; Tarrahi, M.J.; Farhang, A.; Amani, R. Effect of Zinc Supplementation on Quality of Life and Sleep Quality in Young Women with Premenstrual Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Arch. Gynecol. Obstet. 2020, 302, 657–664. [Google Scholar] [CrossRef] [PubMed]
- McCabe, D.; Lisy, K.; Lockwood, C.; Colbeck, M. The Impact of Essential Fatty Acid, B Vitamins, Vitamin C, Magnesium and Zinc Supplementation on Stress Levels in Women: A Systematic Review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 402–453. [Google Scholar] [CrossRef] [PubMed]
- Chocano-Bedoya, P.O.; Manson, J.A.E.; Hankinson, S.E.; Johnson, S.R.; Chasan-Taber, L.; Ronnenberg, A.G.; Bigelow, C.; Bertone-Johnson, E.R. Intake of Selected Minerals and Risk of Premenstrual Syndrome. Am. J. Epidemiol. 2013, 177, 1118–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klump, K.L.; Keel, P.K.; Racine, S.E.; Burt, A.A.; Neale, M.; Sisk, C.L.; Boker, S.; Hu, J.Y. The Interactive Effects of Estrogen and Progesterone on Changes in Emotional Eating across the Menstrual Cycle. J. Abnorm. Psychol. 2013, 122, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Yen, J.Y.; Liu, T.L.; Chen, I.J.; Chen, S.Y.; Ko, C.H. Premenstrual Appetite and Emotional Responses to Foods among Women with Premenstrual Dysphoric Disorder. Appetite 2018, 125, 18–23. [Google Scholar] [CrossRef]
- Etebary, S.; Nikseresht, S.; Reza Sadeghipour, H.; Reza Zarrindast, M. Postpartum Depression and Role of Serum Trace Elements. Iran. J. Psychiatry 2010, 5, 40–46. [Google Scholar]
- Dennis, C.L.; Chung-Lee, L. Postpartum Depression Help-Seeking Barriers and Maternal Treatment Preferences: A Qualitative Systematic Review. Birth 2006, 33, 323–331. [Google Scholar] [CrossRef]
- Fu, C.W.; Liu, J.T.; Tu, W.J.; Yang, J.Q.; Cao, Y. Association between Serum 25-Hydroxyvitamin D Levels Measured 24 Hours after Delivery and Postpartum Depression. BJOG Int. J. Obstet. Gynaecol. 2015, 122, 1688–1694. [Google Scholar] [CrossRef]
- Accortt, E.E.; Schetter, C.D.; Peters, R.M.; Cassidy-Bushrow, A.E. Lower Prenatal Vitamin D Status and Postpartum Depressive Symptomatology in African American Women: Preliminary Evidence for Moderation by Inflammatory Cytokines. Arch. Women’s Ment. Health 2016, 19, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amini, S.; Amani, R.; Jafarirad, S.; Cheraghian, B.; Sayyah, M.; Hemmati, A.A. The Effect of Vitamin D and Calcium Supplementation on Inflammatory Biomarkers, Estradiol Levels and Severity of Symptoms in Women with Postpartum Depression: A Randomized Double-Blind Clinical Trial. Nutr. Neurosci. 2022, 25, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Amini, S.; Jafarirad, S.; Amani, R. Postpartum Depression and Vitamin D: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2019, 59, 1514–1520. [Google Scholar] [CrossRef]
- Aghajafari, F.; Letourneau, N.; Mahinpey, N.; Cosic, N.; Giesbrecht, G. Vitamin D Deficiency and Antenatal and Postpartum Depression: A Systematic Review. Nutrients 2018, 10, 478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Liu, N.; Sun, W.; Chen, D.; Zhao, J.; Zhang, W. Association between Vitamin D Deficiency and Antepartum and Postpartum Depression: A Systematic Review and Meta-Analysis of Longitudinal Studies. Arch. Gynecol. Obstet. 2018, 298, 1045–1059. [Google Scholar] [CrossRef] [PubMed]
- Cantor, A.G.; Bougatsos, C.; Dana, T.; Blazina, I.; McDonagh, M. Routine Iron Supplementation and Screening for Iron Deficiency Anemia in Pregnancy: A Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2015, 162, 566–576. [Google Scholar] [CrossRef] [Green Version]
- Dama, M.; van Lieshout, R.J.; Mattina, G.; Steiner, M. Iron Deficiency and Risk of Maternal Depression in Pregnancy: An Observational Study. J. Obstet. Gynaecol. Can. 2018, 40, 698–703. [Google Scholar] [CrossRef]
- Albacar, G.; Sans, T.; Martín-Santos, R.; García-Esteve, L.; Guillamat, R.; Sanjuan, J.; Cañellas, F.; Gratacòs, M.; Cavalle, P.; Arija, V.; et al. An Association between Plasma Ferritin Concentrations Measured 48 h after Delivery and Postpartum Depression. J. Affect. Disord. 2011, 131, 136–142. [Google Scholar] [CrossRef]
- Armony-Sivan, R.; Shao, J.; Li, M.; Zhao, G.; Zhao, Z.; Xu, G.; Zhou, M.; Zhan, J.; Bian, Y.; Ji, C.; et al. No Relationship between Maternal Iron Status and Postpartum Depression in Two Samples in China. J. Pregnancy 2012, 2012, 521431. [Google Scholar] [CrossRef] [Green Version]
- Wassef, A.; Nguyen, Q.D.; St-André, M. Anaemia and Depletion of Iron Stores as Risk Factors for Postpartum Depression: A Literature Review. J. Psychosom. Obstet. Gynaecol. 2019, 40, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Hameed, S.; Naser, I.A.; Ghussein, M.A.; Ellulu, M.S. Is Iron Deficiency a Risk Factor for Postpartum Depression? A Case–Control Study in the Gaza Strip, Palestine. Public Health Nutr. 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hoge, A.; Tabar, V.; Donneau, A.F.; Dardenne, N.; Degée, S.; Timmermans, M.; Nisolle, M.; Guillaume, M.; Castronovo, V. Imbalance between Omega-6 and Omega-3 Polyunsaturated Fatty Acids in Early Pregnancy Is Predictive of Postpartum Depression in a Belgian Cohort. Nutrients 2019, 11, 876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, M.; Ogawa, K.; Morisaki, N.; Tani, Y.; Horikawa, R.; Fujiwara, T. Dietary N-3 Polyunsaturated Fatty Acids in Late Pregnancy and Postpartum Depressive Symptom among Japanese Women. Front. Psychiatry 2017, 8, 241. [Google Scholar] [CrossRef] [Green Version]
- Mocking, R.J.T.; Steijn, K.; Roos, C.; Assies, J.; Bergink, V.; Ruhé, H.G.; Schene, A.H. Omega-3 Fatty Acid Supplementation for Perinatal Depression: A Meta-Analysis. J. Clin. Psychiatry 2020, 81, 19r13106. [Google Scholar] [CrossRef]
- Fard, F.E.; Mirghafourvand, M.; Mohammad-Alizadeh Charandabi, S.; Farshbaf-Khalili, A.; Javadzadeh, Y.; Asgharian, H. Effects of Zinc and Magnesium Supplements on Postpartum Depression and Anxiety: A Randomized Controlled Clinical Trial. Women Health 2017, 57, 1115–1128. [Google Scholar] [CrossRef]
- Miller, E.S.; Sakowicz, A.; Roy, A.; Wang, A.; Yang, A.; Ciolino, J.; Grobman, W.A.; Wisner, K.L.; Yee, L.M. Is Peripartum Magnesium Sulfate Associated with a Reduction in Postpartum Depressive Symptoms? Am. J. Obstet. Gynecol. MFM 2021, 3, 100407. [Google Scholar] [CrossRef]
- Sara, N.; Sahabeh, E.; Morteza, K.; Fatemeh, N.; Reza, Z.M.; Reza, S.H. Acute Administration of Zn, Mg, And Thiamine Improves Postpartum Depression Conditions In Mice. Arch. Iran. Med. 2012, 15, 306–311. [Google Scholar]
- Maki, P.M.; Kornstein, S.G.; Joffe, H.; Bromberger, J.T.; Freeman, E.W.; Athappilly, G.; Bobo, W.V.; Rubin, L.H.; Koleva, H.K.; Cohen, L.S.; et al. Guidelines for the Evaluation and Treatment of Perimenopausal Depression: Summary and Recommendations. Menopause 2018, 25, 1069–1085. [Google Scholar] [CrossRef] [Green Version]
- Bromberger, J.T.; Kravitz, H.M. Mood and Menopause: Findings from the Study of Women’s Health Across the Nation (SWAN) over 10 Years. Obstet. Gynecol. Clin. N. Am. 2011, 38, 609–625. [Google Scholar] [CrossRef] [Green Version]
- Bener, A.; Saleh, N. Low Vitamin D, and Bone Mineral Density with Depressive Symptoms Burden in Menopausal and Postmenopausal Women. J. Mid-Life Health 2015, 6, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Chen, T.; Lei, Y.; Wei, S.; Yu, P.; Cao, Y.; Zhao, Y.; Chen, J. Association Analysis between Vitamin D Level and Depression in Women Perimenopause: A Protocol of Systematic Review and Meta-Analysis. Medicine 2020, 99, e20416. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.A.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Szkup, M.; Jurczak, A.; Brodowska, A.; Brodowska, A.; Noceń, I.; Chlubek, D.; Laszczyńska, M.; Karakiewicz, B.; Grochans, E. Analysis of Relations Between the Level of Mg, Zn, Ca, Cu, and Fe and Depressiveness in Postmenopausal Women. Biol. Trace Elem. Res. 2017, 176, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Chae, M.; Park, K. Association between Dietary Omega-3 Fatty Acid Intake and Depression in Postmenopausal Women. Nutr. Res. Pract. 2021, 15, 468–478. [Google Scholar] [CrossRef]
- Das, L.; Bhaumik, E.; Raychaudhuri, U.; Chakraborty, R. Role of Nutraceuticals in Human Health. J. Food Sci. Technol. 2012, 49, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Borrego, R.; von Schacky, C.; Osorio, M.J.A.; Llaneza, P.; Pinto, X.; Losa, F.; Navarro, M.C.; Lubián, D.; Mendoza, N. Recommendations of the Spanish Menopause Society on the Consumption of Omega-3 Polyunsaturated Fatty Acids by Postmenopausal Women. Maturitas 2017, 103, 71–77. [Google Scholar] [CrossRef]
- Mocking, R.J.T.; Harmsen, I.; Assies, J.; Koeter, M.W.J.; Ruhé, H.G.; Schene, A.H. Meta-Analysis and Meta-Regression of Omega-3 Polyunsaturated Fatty Acid Supplementation for Major Depressive Disorder. Transl. Psychiatry 2016, 6, e756. [Google Scholar] [CrossRef]
- Appleton, K.M.; Sallis, H.M.; Perry, R.; Ness, A.R.; Churchill, R. Omega-3 Fatty Acids for Depression in Adults. Cochrane Database Syst. Rev. 2015, 2015, CD004692. [Google Scholar] [CrossRef]
- van der Burg, K.P.; Cribb, L.; Firth, J.; Karmacoska, D.; Mischoulon, D.; Byrne, G.J.; Bousman, C.; Stough, C.; Murphy, J.; Oliver, G.; et al. EPA and DHA as Markers of Nutraceutical Treatment Response in Major Depressive Disorder. Eur. J. Nutr. 2020, 59, 2439–2447. [Google Scholar] [CrossRef]
- Martinowich, K.; Lu, B. Interaction between BDNF and Serotonin: Role in Mood Disorders. Neuropsychopharmacology 2007, 33, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Park, Y. N-3 Polyunsaturated Fatty Acids and 17β-Estradiol Injection Induce Antidepressant-like Effects through Regulation of Serotonergic Neurotransmission in Ovariectomized Rats. J. Nutr. Biochem. 2015, 26, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.E.; Park, Y. EPA and DHA, but Not ALA, Have Antidepressant Effects with 17β-Estradiol Injection via Regulation of a Neurobiological System in Ovariectomized Rats. J. Nutr. Biochem. 2017, 49, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Malaguarnera, L. Vitamin D and Microbiota: Two Sides of the Same Coin in the Immunomodulatory Aspects. Int. Immunopharmacol. 2020, 79, 106112. [Google Scholar] [CrossRef]
- Schwab, M.; Reynders, V.; Loitsch, S.; Steinhilber, D.; Stein, J.; Schröder, O. Involvement of Different Nuclear Hormone Receptors in Butyrate-Mediated Inhibition of Inducible NFκB Signalling. Mol. Immunol. 2007, 44, 3625–3632. [Google Scholar] [CrossRef]
- Fakhoury, H.M.A.; Kvietys, P.R.; AlKattan, W.; al Anouti, F.; Elahi, M.A.; Karras, S.N.; Grant, W.B. Vitamin D and Intestinal Homeostasis: Barrier, Microbiota, and Immune Modulation. J. Steroid Biochem. Mol. Biol. 2020, 200, 105663. [Google Scholar] [CrossRef]
- Bora, S.A.; Kennett, M.J.; Smith, P.B.; Patterson, A.D.; Cantorna, M.T. The Gut Microbiota Regulates Endocrine Vitamin D Metabolism through Fibroblast Growth Factor 23. Front. Immunol. 2018, 9, 408. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Mocayar Marón, F.J.; Ferder, L.; Reiter, R.J.; Manucha, W. Daily and Seasonal Mitochondrial Protection: Unraveling Common Possible Mechanisms Involving Vitamin D and Melatonin. J. Steroid Biochem. Mol. Biol. 2020, 199, 105595. [Google Scholar] [CrossRef]
- Cheng, T.S.; Loy, S.L.; Cheung, Y.B.; Cai, S.; Colega, M.T.; Godfrey, K.M.; Chong, Y.S.; Tan, K.H.; Shek, L.P.C.; Lee, Y.S.; et al. Plasma Vitamin D Deficiency Is Associated with Poor Sleep Quality and Night-Time Eating at Mid-Pregnancy in Singapore. Nutrients 2017, 9, 340. [Google Scholar] [CrossRef] [Green Version]
- Fallah, M.; Askari, G.; Asemi, Z. Is Vitamin D Status Associated with Depression, Anxiety and Sleep Quality in Pregnancy: A Systematic Review. Adv. Biomed. Res. 2020, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, A.; Avan, A.; Sadeghnia, H.R.; Esmaeili, H.; Tayefi, M.; Ghasemi, F.; Nejati Salehkhani, F.; Arabpour-Dahoue, M.; Rastgar-Moghadam, A.; Ferns, G.A.; et al. High Dose Vitamin D Supplementation Can Improve Menstrual Problems, Dysmenorrhea, and Premenstrual Syndrome in Adolescents. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2018, 34, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Ostadmohammadi, V.; Jamilian, M.; Bahmani, F.; Asemi, Z. Vitamin D and Probiotic Co-Supplementation Affects Mental Health, Hormonal, Inflammatory and Oxidative Stress Parameters in Women with Polycystic Ovary Syndrome. J. Ovarian Res. 2019, 12, 5. [Google Scholar] [CrossRef]
- Cooney, L.G.; Dokras, A. Depression and Anxiety in Polycystic Ovary Syndrome: Etiology and Treatment. Curr. Psychiatry Rep. 2017, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- Young, L.M.; Pipingas, A.; White, D.J.; Gauci, S.; Scholey, A. A Systematic Review and Meta-Analysis of B Vitamin Supplementation on Depressive Symptoms, Anxiety, and Stress: Effects on Healthy and “At-Risk” Individuals. Nutrients 2019, 11, 2232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Cantley, L.C. Toward a Better Understanding of Folate Metabolism in Health and Disease. J. Exp. Med. 2019, 216, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Zaric, B.L.; Obradovic, M.; Bajic, V.; Haidara, M.A.; Jovanovic, M.; Isenovic, E.R. Homocysteine and Hyperhomocysteinaemia. Curr. Med. Chem. 2019, 26, 2948–2961. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Sun, X.; Liu, J.; Xie, X.; Cui, W.; Zhu, Y. Homocysteine Accelerates Senescence of Endothelial Cells via DNA Hypomethylation of Human Telomerase Reverse Transcriptase. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Michels, K.A.; Wactawski-Wende, J.; Mills, J.L.; Schliep, K.C.; Gaskins, A.J.; Yeung, E.H.; Kim, K.; Plowden, T.C.; Sjaarda, L.A.; Chaljub, E.N.; et al. Folate, Homocysteine and the Ovarian Cycle among Healthy Regularly Menstruating Women. Hum. Reprod. 2017, 32, 1743–1750. [Google Scholar] [CrossRef]
- Azziz, R. Polycystic Ovary Syndrome. Obstet. Gynecol. 2018, 132, 321–336. [Google Scholar] [CrossRef]
- Brutocao, C.; Zaiem, F.; Alsawas, M.; Morrow, A.S.; Murad, M.H.; Javed, A. Psychiatric Disorders in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Endocrine 2018, 62, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Huang, Q.; Yao, L.; Liu, W.; Ruan, J.; Nong, Y.; Chen, Y.; Fan, L.; Wei, J.; Wang, S.; et al. Gestational Folic Acid Administration Alleviated Maternal Postpartum Emotional and Cognitive Dysfunction in Mice. Front. Pharmacol. 2021, 12, 701009. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Liu, Y.; Cao, L.; Zheng, Y.; Li, W.; Huang, G. Association between Duration of Folic Acid Supplementation during Pregnancy and Risk of Postpartum Depression. Nutrients 2017, 9, 1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tako, E. Dietary Trace Minerals. Nutrients 2019, 11, 2823. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.R.; Islam, M.R.; Shalahuddin Qusar, M.M.A.; Islam, M.S.; Kabir, M.H.; Mustafizur Rahman, G.K.M.; Islam, M.S.; Hasnat, A. Alterations of Serum Macro-Minerals and Trace Elements Are Associated with Major Depressive Disorder: A Case-Control Study. BMC Psychiatry 2018, 18, 94. [Google Scholar] [CrossRef] [Green Version]
- Kirkland, A.E.; Sarlo, G.L.; Holton, K.F. The Role of Magnesium in Neurological Disorders. Nutrients 2018, 10, 730. [Google Scholar] [CrossRef] [Green Version]
- Tarleton, E.K.; Littenberg, B.; MacLean, C.D.; Kennedy, A.G.; Daley, C. Role of Magnesium Supplementation in the Treatment of Depression: A Randomized Clinical Trial. PLoS ONE 2017, 12, e0180067. [Google Scholar] [CrossRef] [Green Version]
- Maktabi, M.; Jamilian, M.; Asemi, Z. Magnesium-Zinc-Calcium-Vitamin D Co-Supplementation Improves Hormonal Profiles, Biomarkers of Inflammation and Oxidative Stress in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2018, 182, 21–28. [Google Scholar] [CrossRef]
- Sheikh, M.; Hantoushzadeh, S.; Shariat, M.; Farahani, Z.; Ebrahiminasab, O. The Efficacy of Early Iron Supplementation on Postpartum Depression, a Randomized Double-Blind Placebo-Controlled Trial. Eur. J. Nutr. 2017, 56, 901–908. [Google Scholar] [CrossRef]
- Lomagno, K.A.; Hu, F.; Riddell, L.J.; Booth, A.O.; Szymlek-Gay, E.A.; Nowson, C.A.; Byrne, L.K. Increasing Iron and Zinc in Pre-Menopausal Women and Its Effects on Mood and Cognition: A Systematic Review. Nutrients 2014, 6, 5117. [Google Scholar] [CrossRef] [Green Version]
- Sawada, T.; Yokoi, K. Effect of Zinc Supplementation on Mood States in Young Women: A Pilot Study. Eur. J. Clin. Nutr. 2010, 64, 331–333. [Google Scholar] [CrossRef] [PubMed]
- da Silva, L.E.M.; de Santana, M.L.P.; Costa, P.R.D.F.; Pereira, E.M.; Nepomuceno, C.M.M.; Queiroz, V.A.D.O.; de Oliveira, L.P.M.; da Conceição-Machado, M.E.P.; de Sena, E.P. Zinc Supplementation Combined with Antidepressant Drugs for Treatment of Patients with Depression: A Systematic Review and Meta-Analysis. Nutr. Rev. 2021, 79, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Villegas, A.; Pérez-Cornago, A.; Zazpe, I.; Santiago, S.; Lahortiga, F.; Martínez-González, M.A. Micronutrient Intake Adequacy and Depression Risk in the SUN Cohort Study. Eur. J. Nutr. 2018, 57, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- Sajjadi, S.S.; Foshati, S.; Haddadian-Khouzani, S.; Rouhani, M.H. The Role of Selenium in Depression: A Systematic Review and Meta-Analysis of Human Observational and Interventional Studies. Sci. Rep. 2022, 12, 1045. [Google Scholar] [CrossRef]
- Lauinger, L.; Kaiser, P. Sensing and Signaling of Methionine Metabolism. Metabolites 2021, 11, 83. [Google Scholar] [CrossRef]
- Gao, J.; Cahill, C.M.; Huang, X.; Roffman, J.L.; Lamon-Fava, S.; Fava, M.; Mischoulon, D.; Rogers, J.T. S-Adenosyl Methionine and Transmethylation Pathways in Neuropsychiatric Diseases Throughout Life. Neurotherapeutics 2018, 15, 156–175. [Google Scholar] [CrossRef] [Green Version]
- de Berardis, D.; Orsolini, L.; Serroni, N.; Girinelli, G.; Iasevoli, F.; Tomasetti, C.; de Bartolomeis, A.; Mazza, M.; Valchera, A.; Fornaro, M.; et al. A Comprehensive Review on the Efficacy of S-Adenosyl-L-Methionine in Major Depressive Disorder. CNS Neurol. Disord. Drug Targets 2016, 15, 35–44. [Google Scholar] [CrossRef]
- Gobejishvili, L.; Avila, D.V.; Barker, D.F.; Ghare, S.; Henderson, D.; Brock, G.N.; Kirpich, I.A.; Joshi-Barve, S.; Mokshagundam, S.P.L.; McClain, C.J.; et al. S-Adenosylmethionine Decreases Lipopolysaccharide-Induced Phosphodiesterase 4B2 and Attenuates Tumor Necrosis Factor Expression via CAMP/Protein Kinase A Pathway. J. Pharmacol. Exp. Ther. 2011, 337, 433–443. [Google Scholar] [CrossRef] [Green Version]
- Mischoulon, D.; Alpert, J.E.; Arning, E.; Bottiglieri, T.; Fava, M.; Papakostas, G.I. Bioavailability of S-Adenosyl Methionine and Impact on Response in a Randomized Controlled Trial in Major Depressive Disorder. J. Clin. Psychiatry 2012, 73, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Gerbarg, P.; Bottiglieri, T.; Massoumi, L.; Carpenter, L.L.; Lavretsky, H.; Muskin, P.R.; Brown, R.P.; Mischoulon, D. S-Adenosylmethionine (SAMe) for Neuropsychiatric Disorders: A Clinician-Oriented Review of Research. J. Clin. Psychiatry 2017, 78, e656–e667. [Google Scholar] [CrossRef] [Green Version]
- Sarris, J.; Byrne, G.J.; Stough, C.; Bousman, C.; Mischoulon, D.; Murphy, J.; Macdonald, P.; Adams, L.; Nazareth, S.; Oliver, G.; et al. Nutraceuticals for Major Depressive Disorder- More Is Not Merrier: An 8-Week Double-Blind, Randomised, Controlled Trial. J. Affect. Disord. 2019, 245, 1007–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarris, J.; Price, L.H.; Carpenter, L.L.; Tyrka, A.R.; Ng, C.H.; Papakostas, G.I.; Jaeger, A.; Fava, M.; Mischoulon, D. Is S-Adenosyl Methionine (SAMe) for Depression Only Effective in Males? A Re-Analysis of Data from a Randomized Clinical Trial. Pharmacopsychiatry 2015, 48, 141–144. [Google Scholar] [CrossRef] [Green Version]
- Kreider, R.B.; Stout, J.R. Creatine in Health and Disease. Nutrients 2021, 13, 447. [Google Scholar] [CrossRef] [PubMed]
- Brosnan, J.T.; da Silva, R.P.; Brosnan, M.E. The Metabolic Burden of Creatine Synthesis. Amino Acids 2011, 40, 1325–1331. [Google Scholar] [CrossRef] [PubMed]
- Pazini, F.L.; Cunha, M.P.; Rodrigues, A.L.S. The Possible Beneficial Effects of Creatine for the Management of Depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Bakian, A.V.; Huber, R.S.; Scholl, L.; Renshaw, P.F.; Kondo, D. Dietary Creatine Intake and Depression Risk among U.S. Adults. Transl. Psychiatry 2020, 10, 52. [Google Scholar] [CrossRef] [Green Version]
- Allen, P.J.; D’Anci, K.E.; Kanarek, R.B.; Renshaw, P.F. Chronic Creatine Supplementation Alters Depression-like Behavior in Rodents in a Sex-Dependent Manner. Neuropsychopharmacology 2009, 35, 534–546. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.; Kim, J.E.; Hwang, J.; Kim, T.S.; Kang, H.J.; Namgung, E.; Ban, S.; Oh, S.; Yang, J.; Renshaw, P.F.; et al. Effects of Creatine Monohydrate Augmentation on Brain Metabolic and Network Outcome Measures in Women With Major Depressive Disorder. Biol. Psychiatry 2016, 80, 439–447. [Google Scholar] [CrossRef]
- Smith-Ryan, A.E.; Cabre, H.E.; Eckerson, J.M.; Candow, D.G. Creatine Supplementation in Women’s Health: A Lifespan Perspective. Nutrients 2021, 13, 877. [Google Scholar] [CrossRef]
- Islam, M.R.; Islam, M.R.; Ali, S.; Karmoker, J.R.; Kadir, M.F.; Ahmed, M.U.; Nahar, Z.; Islam, S.M.A.; Islam, M.S.; Hasnat, A.; et al. Evaluation of Serum Amino Acids and Non-Enzymatic Antioxidants in Drug-Naïve First-Episode Major Depressive Disorder. BMC Psychiatry 2020, 20, 333. [Google Scholar] [CrossRef]
- Lindseth, G.; Helland, B.; Caspers, J. The Effects of Dietary Tryptophan on Affective Disorders. Arch. Psychiatr. Nurs. 2015, 29, 102–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi, A.M.; Tanabe, A.; Iwahori, Y. A Systematic Review of the Effect of L-Tryptophan Supplementation on Mood and Emotional Functioning. J. Diet. Suppl. 2020, 18, 316–333. [Google Scholar] [CrossRef] [PubMed]
- Gibson, E.L. Tryptophan Supplementation and Serotonin Function: Genetic Variations in Behavioural Effects. Proc. Nutr. Soc. 2018, 77, 174–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelenberg, A.J.; Wojcik, J.D.; Falk, W.E.; Baldessarini, R.J.; Zeisel, S.H.; Schoenfeld, D.; Mok, G.S. Tyrosine for Depression: A Double-Blind Trial. J. Affect. Disord. 1990, 19, 125–132. [Google Scholar] [CrossRef]
- Guaadaoui, A.; Benaicha, S.; Elmajdoub, N.; Bellaoui, M.; Hamal, A. What Is a Bioactive Compound? A Combined Definition for a Preliminary Consensus. Int. J. Nutr. Food Sci. 2014, 3, 174–179. [Google Scholar] [CrossRef]
- Gorzkiewicz, J.; Bartosz, G.; Sadowska-Bartosz, I. The Potential Effects of Phytoestrogens: The Role in Neuroprotection. Molecules 2021, 26, 2954. [Google Scholar] [CrossRef]
- Hritcu, L.; Ionita, R.; Postu, P.A.; Gupta, G.K.; Turkez, H.; Lima, T.C.; Carvalho, C.U.S.; de Sousa, D.P. Antidepressant Flavonoids and Their Relationship with Oxidative Stress. Oxidative Med. Cell. Longev. 2017, 2017, 5762172. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Choi, J.; Lee, H.J. Flavonoid-Rich Orange Juice Intake and Altered Gut Microbiome in Young Adults with Depressive Symptom: A Randomized Controlled Study. Nutrients 2020, 12, 1815. [Google Scholar] [CrossRef]
- Barfoot, K.L.; Forster, R.; Lamport, D.J. Mental Health in New Mothers: A Randomised Controlled Study into the Effects of Dietary Flavonoids on Mood and Perceived Quality of Life. Nutrients 2021, 13, 2383. [Google Scholar] [CrossRef]
- Li, J.; Li, H.; Yan, P.; Guo, L.; Li, J.; Han, J.; Qiu, J.; Yang, K. Efficacy and Safety of Phytoestrogens in the Treatment of Perimenopausal and Postmenopausal Depressive Disorders: A Systematic Review and Meta-Analysis. Int. J. Clin. Pract. 2021, 75, e14360. [Google Scholar] [CrossRef]
- Socała, K.; Szopa, A.; Serefko, A.; Poleszak, E.; Wlaź, P. Neuroprotective Effects of Coffee Bioactive Compounds: A Review. Int. J. Mol. Sci. 2020, 22, 107. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Micek, A.; Castellano, S.; Pajak, A.; Galvano, F. Coffee, Tea, Caffeine and Risk of Depression: A Systematic Review and Dose–Response Meta-Analysis of Observational Studies. Mol. Nutr. Food Res. 2016, 60, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.S.; Deng, R.; Fan, Y.; Li, K.; Meng, F.; Li, X.; Liu, R. Low Dose of Caffeine Enhances the Efficacy of Antidepressants in Major Depressive Disorder and the Underlying Neural Substrates. Mol. Nutr. Food Res. 2017, 61, 1600910. [Google Scholar] [CrossRef] [PubMed]
- López-Cruz, L.; Salamone, J.D.; Correa, M. Caffeine and Selective Adenosine Receptor Antagonists as New Therapeutic Tools for the Motivational Symptoms of Depression. Front. Pharmacol. 2018, 9, 526. [Google Scholar] [CrossRef]
- Driscoll, I.; Shumaker, S.A.; Snively, B.M.; Margolis, K.L.; Manson, J.E.; Vitolins, M.Z.; Rossom, R.C.; Espeland, M.A. Relationships Between Caffeine Intake and Risk for Probable Dementia or Global Cognitive Impairment: The Women’s Health Initiative Memory Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1596–1602. [Google Scholar] [CrossRef] [Green Version]
- Lucas, M.; Mirzaei, F.; Pan, A.; Okereke, O.I.; Willett, W.C.; O’Reilly, É.J.; Koenen, K.; Ascherio, A. Coffee, Caffeine, and Risk of Depression among Women. Arch. Intern. Med. 2011, 171, 1571–1578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arciero, P.J.; Ormsbee, M.J. Relationship of Blood Pressure, Behavioral Mood State, and Physical Activity Following Caffeine Ingestion in Younger and Older Women. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2009, 34, 754–762. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, L.M.; Mazyck, P.J.; Hunter, M.H. Premenstrual Syndrome. Am. Fam. Physician 2003, 67, 1743–1752. [Google Scholar]
- Rusconi, A.C.; Valeriani, G.; Carluccio, G.M.; Majorana, M.; Carlone, C.; Raimondo, P.; Ripà, S.; Marino, P.; de Fornari, M.A.C.; Biondi, M. Coffee Consumption in Depressive Disorders: It’s Not One Size Fits All. Riv. Psichiatr. 2014, 49, 164–171. [Google Scholar] [CrossRef]
- Kalt, W.; Cassidy, A.; Howard, L.R.; Krikorian, R.; Stull, A.J.; Tremblay, F.; Zamora-Ros, R. Recent Research on the Health Benefits of Blueberries and Their Anthocyanins. Adv. Nutr. 2020, 11, 224–236. [Google Scholar] [CrossRef]
- Tian, L.; Tan, Y.; Chen, G.; Wang, G.; Sun, J.; Ou, S.; Chen, W.; Bai, W. Metabolism of Anthocyanins and Consequent Effects on the Gut Microbiota. Crit. Rev. Food Sci. Nutr. 2019, 59, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Morais, C.A.; Oyama, L.M.; de Moura Conrado, R.; de Rosso, V.V.; do Nascimento, C.O.; Pisani, L.P. Polyphenols-Rich Fruit in Maternal Diet Modulates Inflammatory Markers and the Gut Microbiota and Improves Colonic Expression of ZO-1 in Offspring. Food Res. Int. 2015, 77, 186–193. [Google Scholar] [CrossRef]
- Lee, Y.M.; Yoon, Y.; Yoon, H.; Park, H.M.; Song, S.; Yeum, K.J. Dietary Anthocyanins against Obesity and Inflammation. Nutrients 2017, 9, 1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- do Rosario, V.A.; Fitzgerald, Z.; Broyd, S.; Paterson, A.; Roodenrys, S.; Thomas, S.; Bliokas, V.; Potter, J.; Walton, K.; Weston–Green, K.; et al. Food Anthocyanins Decrease Concentrations of TNF-α in Older Adults with Mild Cognitive Impairment: A Randomized, Controlled, Double Blind Clinical Trial. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 950–960. [Google Scholar] [CrossRef]
- Bowtell, J.L.; Aboo-Bakkar, Z.; Conway, M.E.; Adlam, A.L.R.; Fulford, J. Enhanced Task-Related Brain Activation and Resting Perfusion in Healthy Older Adults after Chronic Blueberry Supplementation. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Et Metab. 2017, 42, 773–779. [Google Scholar] [CrossRef]
- Aboonabi, A.; Meyer, R.R.; Gaiz, A.; Singh, I. Anthocyanins in Berries Exhibited Anti-Atherogenicity and Antiplatelet Activities in a Metabolic Syndrome Population. Nutr. Res. 2020, 76, 82–93. [Google Scholar] [CrossRef]
- Malhotra, A.; Bath, S.; Elbarbry, F. An Organ System Approach to Explore the Antioxidative, Anti-Inflammatory, and Cytoprotective Actions of Resveratrol. Oxidative Med. Cell. Longev. 2015, 2015, 803971. [Google Scholar] [CrossRef]
- Moore, A.; Beidler, J.; Hong, M.Y. Resveratrol and Depression in Animal Models: A Systematic Review of the Biological Mechanisms. Molecues 2018, 23, 2197. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.H.; Madhana, R.M.; Athira, K.V.; Kasala, E.R.; Bodduluru, L.N.; Pitta, S.; Mahareddy, J.R.; Lahkar, M. Resveratrol Ameliorates Depressive-like Behavior in Repeated Corticosterone-Induced Depression in Mice. Steroids 2015, 101, 37–42. [Google Scholar] [CrossRef]
- Ge, L.; Liu, L.; Liu, H.; Liu, S.; Xue, H.; Wang, X.; Yuan, L.; Wang, Z.; Liu, D. Resveratrol Abrogates Lipopolysaccharide-Induced Depressive-like Behavior, Neuroinflammatory Response, and CREB/BDNF Signaling in Mice. Eur. J. Pharmacol. 2015, 768, 49–57. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Z.; You, W.; Zhang, X.; Li, S.; Barish, P.A.; Vernon, M.M.; Du, X.; Li, G.; Pan, J.; et al. Antidepressant-like Effect of Trans-Resveratrol: Involvement of Serotonin and Noradrenaline System. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2010, 20, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Ma, Y.; Zhang, R.; Zhong, H.; Wang, L.; Zhao, J.; Yang, L.; Fan, X. Resveratrol Ameliorates Estrogen Deficiency-Induced Depression- and Anxiety-like Behaviors and Hippocampal Inflammation in Mice. Psychopharmacology 2019, 236, 1385–1399. [Google Scholar] [CrossRef] [PubMed]
- Davinelli, S.; Scapagnini, G.; Marzatico, F.; Nobile, V.; Ferrara, N.; Corbi, G. Influence of Equol and Resveratrol Supplementation on Health-Related Quality of Life in Menopausal Women: A Randomized, Placebo-Controlled Study. Maturitas 2017, 96, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Zaw, J.J.T.; Howe, P.R.C.; Wong, R.H.X. Long-Term Resveratrol Supplementation Improves Pain Perception, Menopausal Symptoms, and Overall Well-Being in Postmenopausal Women: Findings from a 24-Month Randomized, Controlled, Crossover Trial. Menopause 2020, 28, 40–49. [Google Scholar] [CrossRef]
- Farzaei, M.H.; Rahimi, R.; Nikfar, S.; Abdollahi, M. Effect of Resveratrol on Cognitive and Memory Performance and Mood: A Meta-Analysis of 225 Patients. Pharmacol. Res. 2018, 128, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; Sarhadi, K.J.; Soula, M.; Zafar, A.; Quadri, S.A. Current Application of Cannabidiol (CBD) in the Management and Treatment of Neurological Disorders. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 3085–3098. [Google Scholar] [CrossRef]
- Silote, G.P.; Sartim, A.; Sales, A.; Eskelund, A.; Guimarães, F.S.; Wegener, G.; Joca, S. Emerging Evidence for the Antidepressant Effect of Cannabidiol and the Underlying Molecular Mechanisms. J. Chem. Neuroanat. 2019, 98, 104–116. [Google Scholar] [CrossRef]
- Calapai, G.; Mannucci, C.; Chinou, I.; Cardia, L.; Calapai, F.; Sorbara, E.E.; Firenzuoli, B.; Ricca, V.; Gensini, G.F.; Firenzuoli, F. Preclinical and Clinical Evidence Supporting Use of Cannabidiol in Psychiatry. Evid. Based Complement. Altern. Med. 2019, 2019, 2509129. [Google Scholar] [CrossRef] [Green Version]
- Mistry, M.; Simpson, P.; Morris, E.; Fritz, A.-K.; Karavadra, B.; Lennox, C.; Prosser-Snelling, E. Cannabidiol for the Management of Endometriosis and Chronic Pelvic Pain. J. Minim. Invasive Gynecol. 2022, 29, 169–176. [Google Scholar] [CrossRef]
- Sarrafpour, S.; Urits, I.; Powell, J.; Nguyen, D.; Callan, J.; Orhurhu, V.; Simopoulos, T.; Viswanath, O.; Kaye, A.D.; Kaye, R.J.; et al. Considerations and Implications of Cannabidiol Use During Pregnancy. Curr. Pain Headache Rep. 2020, 24, 38. [Google Scholar] [CrossRef]
- Lombardi, V.C.; de Meirleir, K.L.; Subramanian, K.; Nourani, S.M.; Dagda, R.K.; Delaney, S.L.; Palotás, A. Nutritional Modulation of the Intestinal Microbiota; Future Opportunities for the Prevention and Treatment of Neuroimmune and Neuroinflammatory Disease. J. Nutr. Biochem. 2018, 61, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tian, P.; O’Riordan, K.J.; Lee, Y.K.; Wang, G.; Zhao, J.; Zhang, H.; Cryan, J.F.; Chen, W. Towards a Psychobiotic Therapy for Depression: Bifidobacterium Breve CCFM1025 Reverses Chronic Stress-Induced Depressive Symptoms and Gut Microbial Abnormalities in Mice. Neurobiol. Stress 2020, 12, 100216. [Google Scholar] [CrossRef] [PubMed]
- Buffington, S.A.; di Prisco, G.V.; Auchtung, T.A.; Ajami, N.J.; Petrosino, J.F.; Costa-Mattioli, M. Microbial Reconstitution Reverses Maternal Diet-Induced Social and Synaptic Deficits in Offspring. Cell 2016, 165, 1762–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega, M.A.; Alvarez-Mon, M.A.; García-Montero, C.; Fraile-Martinez, O.; Guijarro, L.G.; Lahera, G.; Monserrat, J.; Valls, P.; Mora, F.; Rodríguez-Jiménez, R.; et al. Gut Microbiota Metabolites in Major Depressive Disorder—Deep Insights into Their Pathophysiological Role and Potential Translational Applications. Metabolites 2022, 12, 50. [Google Scholar] [CrossRef]
- Jamilian, M.; Mansury, S.; Bahmani, F.; Heidar, Z.; Amirani, E.; Asemi, Z. The Effects of Probiotic and Selenium Co-Supplementation on Parameters of Mental Health, Hormonal Profiles, and Biomarkers of Inflammation and Oxidative Stress in Women with Polycystic Ovary Syndrome. J. Ovarian Res. 2018, 11, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi, A.; Noorbala, A.A.; Azam, K.; Eskandari, M.H.; Djafarian, K. Effect of Probiotic and Prebiotic vs Placebo on Psychological Outcomes in Patients with Major Depressive Disorder: A Randomized Clinical Trial. Clin. Nutr. 2019, 38, 522–528. [Google Scholar] [CrossRef]
- Aslam, H.; Green, J.; Jacka, F.N.; Collier, F.; Berk, M.; Pasco, J.; Dawson, S.L. Fermented Foods, the Gut and Mental Health: A Mechanistic Overview with Implications for Depression and Anxiety. Nutr. Neurosci. 2018, 23, 659–671. [Google Scholar] [CrossRef]
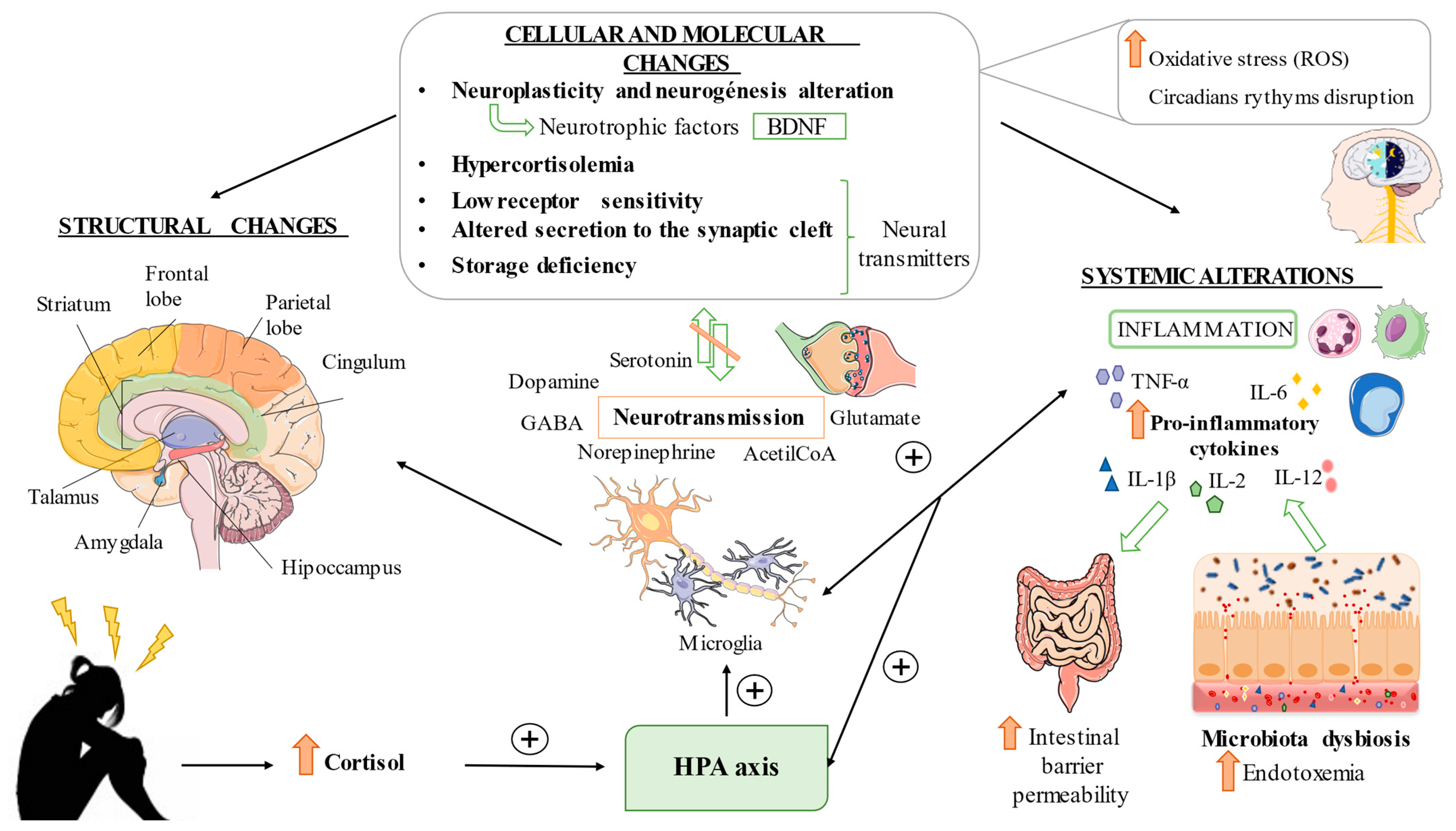
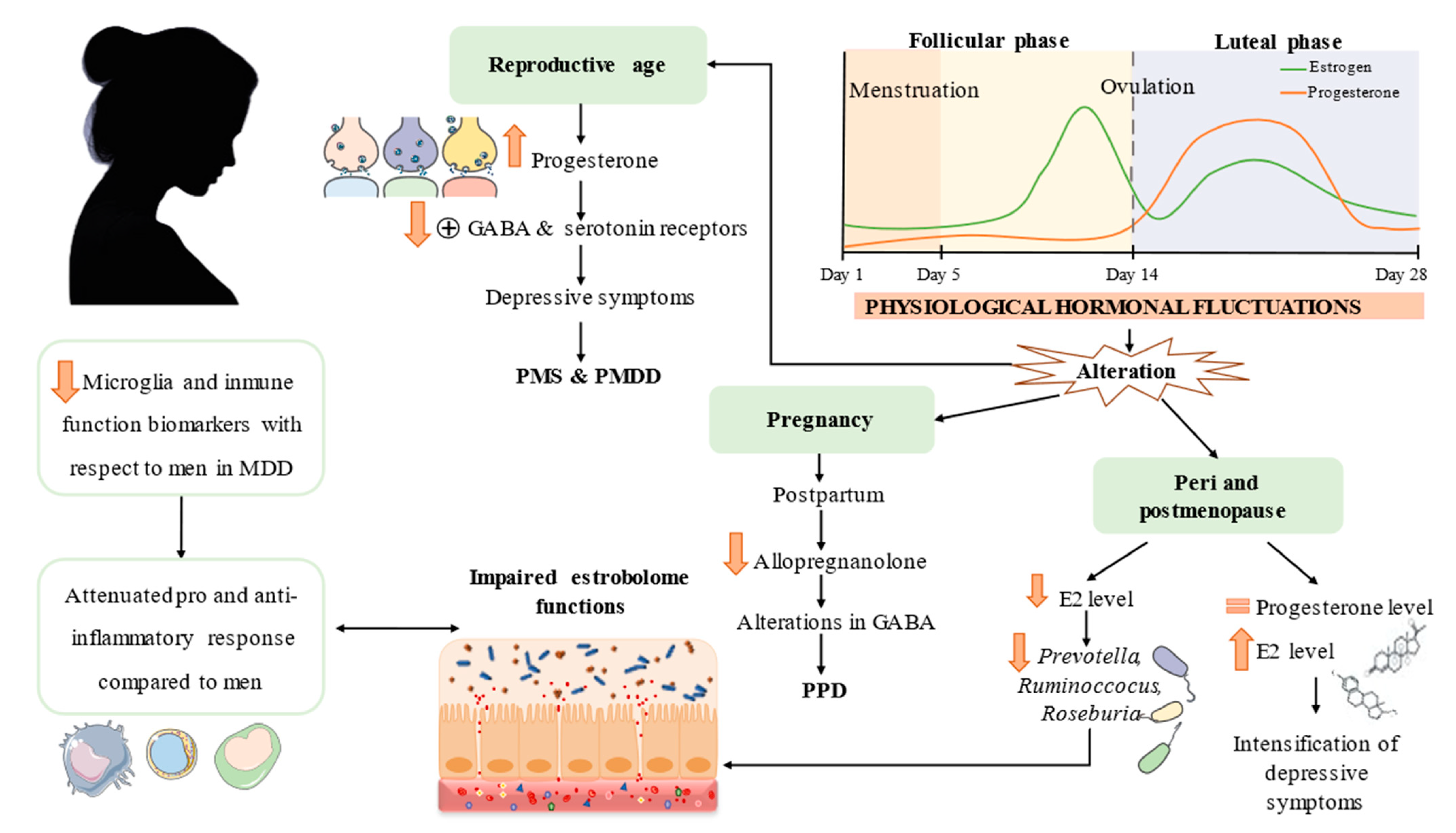


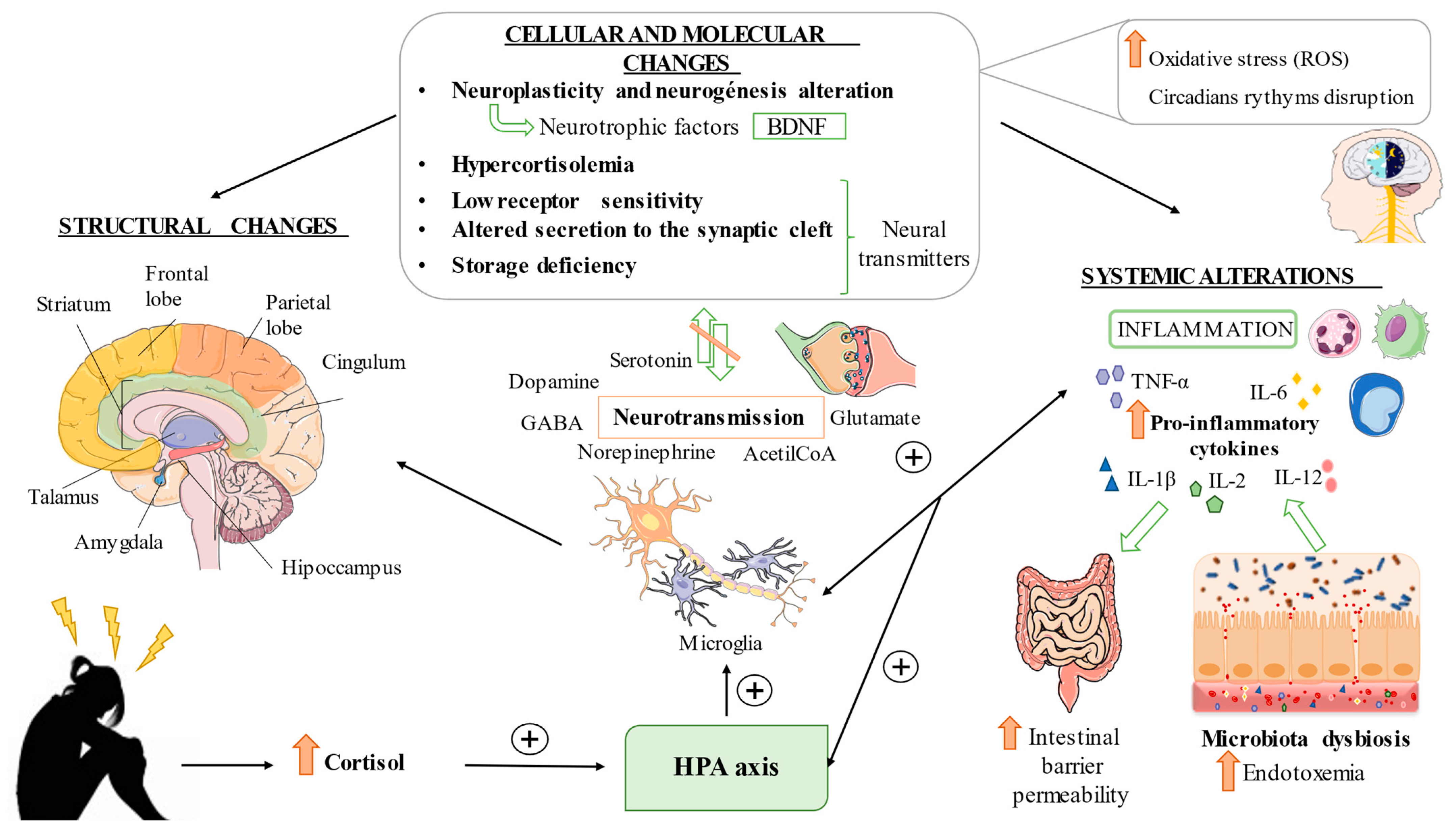{kind=link}
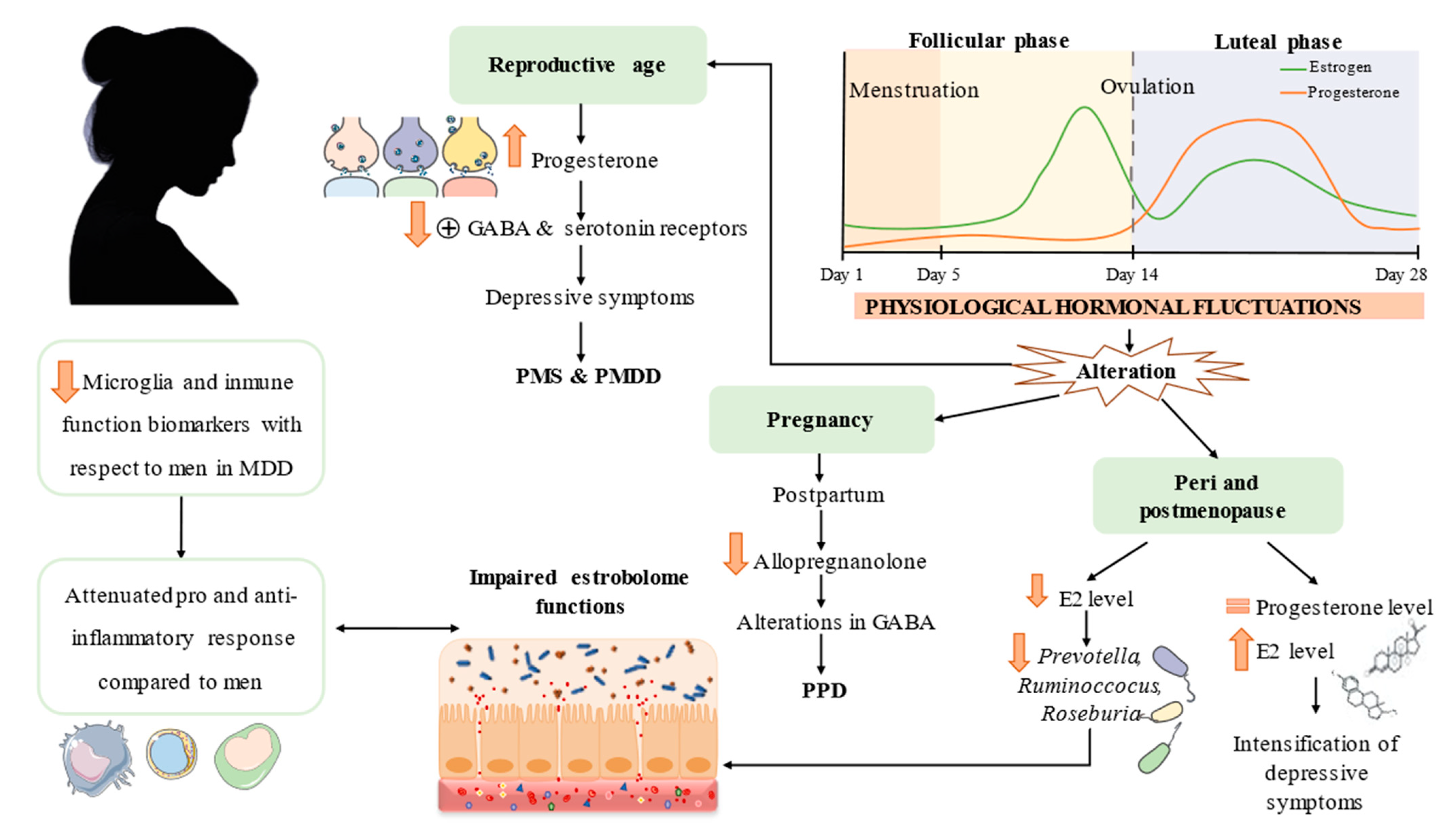{kind=link}
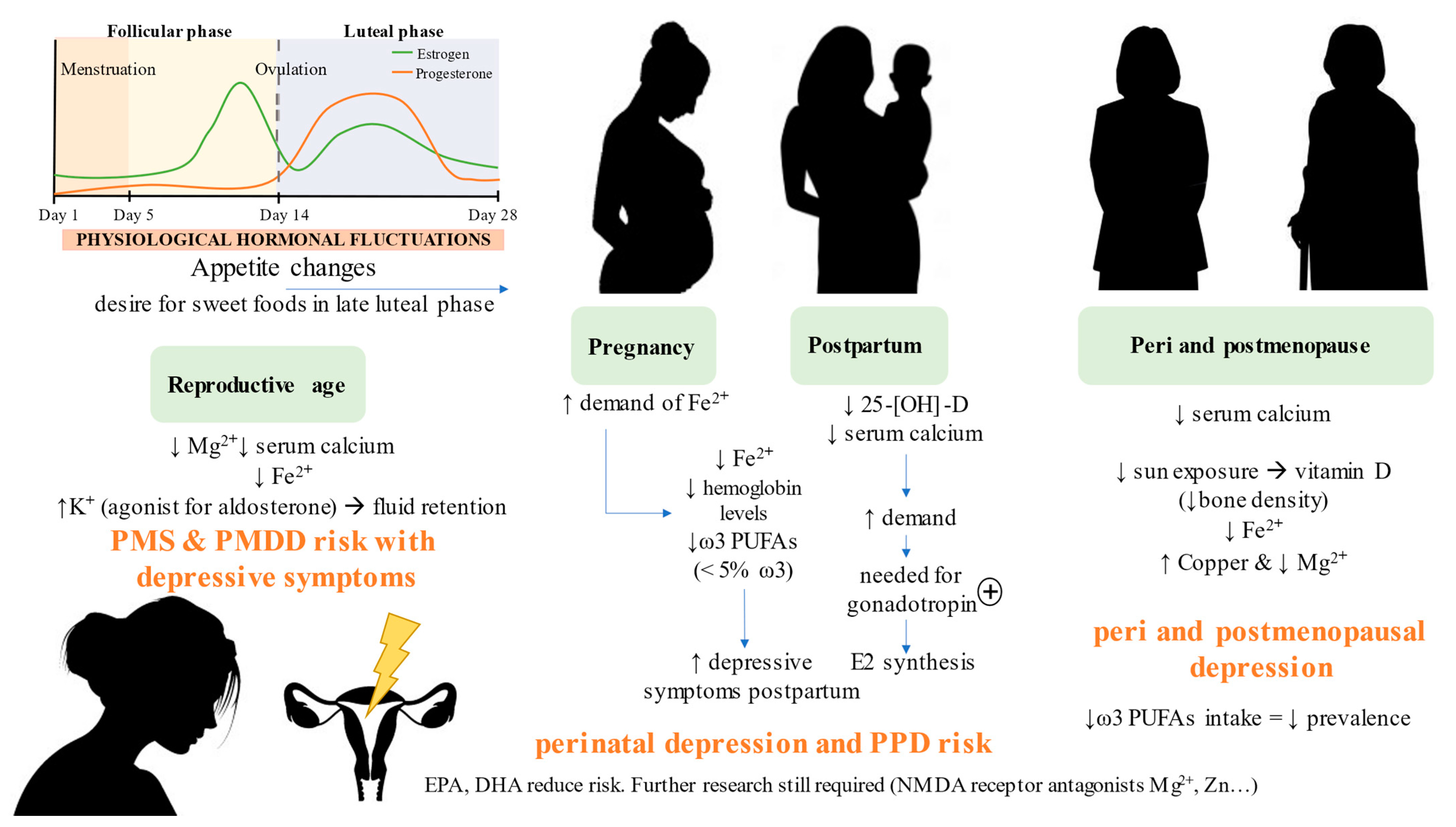{kind=link}
| Nutraceutical | Main Dietary Sources | Probable Antidepressant Effects | Clinical Evidence in MDD Patients | Specific Evidence in Women with MDD | References |
|---|---|---|---|---|---|
| ω-3 PUFAs | Nuts, seeds, oily fish and shellfish | EPA and DHA components of cell walls; neurotransmission and cell signaling; serotonin modulation via CREB; BDFN activation; anti-inflammatory; synergy with estradiol | Increased EPA and DHA in cell walls improve depressive symptoms and response to treatment; homeostasis ratio FA ω-6/ω-3 could be beneficial in patients with MDD | >5% FA ω-3 intake during pregnancy decreases the risk of PPD. Diets high in FA ω-3, mainly EPA, reduce prevalence of postmenopausal depression and improve depressive symptoms | [222,223,224,225,226,227,228] |
| Vitamin D | Oily fish, milk, some vegetables | Involved in neurological development; serotonin synthesis via tryptophan hydrolase 2; hippocampal integrity; balance in neuronal excitation and inhibition pathways; interaction with the intestinal microbiota, leading to joint action in the proinflammatory regulation and signaling of NFĸB; maintenance of antimicrobial peptides | - | Balance of the microbial ecosystem; reduction of inflammation produced by estrogenic fluctuations. <50 nmol/L of 25-[OH]-D in DPP alters sleep-wake patterns and timing of eating. 50,000 IU/week of cholecalciferol led to a drop in the incidence of PMS, dysmenorrhea and associated psychological and physical symptoms. Improves symptoms associated with PCOS | [23,229,230,231,232,233,234,235,236,237,238,239] |
| Vitamin B (B6, B9, B12) | Spices, nuts, liver, fish, meat, soybeans, vegetables, endogenous synthesis, supplementation | Involved in methylation processes; neurotransmitters and phospholipids synthesis; anti-inflammatory effect; homocysteine antagonist; SAMe precursor | - | Treatment for the improvement of alterations typical of PCOS. Folate supplementation during pregnancy decreases the risk of PPD | [240,241,242,243,244,245,246,247] |
| SAMe | Endogenous synthesis or supplementation | Power methylation processes; regulation of monoamine synthesis; anti-inflammatory effects; relation to the gut-brain axis | Effective adjuvant of antidepressants, also in patients with treatment resistance. Another trial determined the use of SAMe as a viable monotherapy | No improvements in severity measured with the Hamilton scale are observed in women. Scarce research makes it difficult to determine its possible benefits in this group | [260,261,262,263,264,265,266,267] |
| Magnesium | Whole grains, green leafy vegetables, nuts | NMDA antagonist; antioxidant; anti-inflammatory; involved in neurogenesis (BDNF) | 248 mg/day of Mg improves mild-moderate MDD with rapid power of action and low toxicity | 100 mg magnesium, 4 mg zinc, 400 mg calcium plus 200 IU vitamin D for 12 weeks had beneficial effects on hormonal profiles, biomarkers of inflammation, and oxidative stress in women with PCOS. | [251,252,253] |
| Iron | Legumes, seeds, seafood | Tyrosine and tryptophan cofactor; monoamine synthesis | - | 50 mg of ferrous sulfate can improve PPD | [254,255] |
| Zinc | Meat, seafood, egg, some vegetables | NMDA antagonist; interaction with monoamines; neuroplasticity | Antidepressants together with zinc provides greater efficacy | 7 mg/day of Zn + 1 multi-vitamin capsule for 7 weeks reduces anger, depression and discouragement. | [255,256,257] |
| Selenium | Nuts, red meat, grains, garlic | Antioxidant: anti-inflammatory | Diets with adequate amounts of Se and other micronutrients have a moderate impact on the inhibition of development of MDD | Possible protective effect of DPP | [258,259] |
| Tryptophan | Legumes, nuts, seeds | Serotonin synthesis | Reversal of anxious and depressive symptoms after treatment. Balanced diet plus tryptophan improves mood in healthy people | Sex-dependent differences, genotype S/S′ in women presents greater neuroprotection, decreased cortisol and consequent mood repair. | [276,277,278] |
| Creatine | Red meat, fish | Synthesis of energy intermediaries | Several clinical studies show the improvement of the pathology after supplementation | Sex-dependent differences: coadjuvant of antidepressant drugs, improvement of neuronal integrity and increased connection of neural networks. In another study, the increase in creatine was directly linked to a higher level of monoamines. Muscle and bone fortification, protection from brain damage in pregnancy and preservation of cognition and sleep hygiene | [268,269,270,271,272,273,274] |
| Phytoestrogens | Soy, legumes, vegetables | Antioxidant; anti-inflammatory; GABAergic and monoaminergic genesis and transmission; regulation of the gut microbiota | 5.4 mg/day of flavonoids improves depressive symptoms and increases the Lachnospiraceae species, implicated in the activation of BDNF | Flavone supplementation in the postnatal period showed benefits in parameters of anxiety and quality of life. Doses of 25 mg/day–100 mg/day of phytoestrogens could alleviate depressive symptoms | [281,282,283,284,285] |
| Caffeine | Coffee, tea | Neuroprotection; dopaminergic regulation | Its consumption reduces the risk of depression and increases the effectiveness of pharmacological treatment. High doses could alter some factors related to health (circadian rhythms, anxiety, mixed affective states) | Differences in efficacy according to age: Doses > 261 mg of caffeine reduce the risk of developing dementia and cognitive disorders in later life. In young women, its benefit is not so decisive. Reduces irritability and insomnia in PMS. | [286,287,288,289,290,291,292,293,294] |
| Anthocyanins | Red fruits, red apple, cherry, black soybeans | Bidirectional relationship with the intestinal microbiota; possible prebiotic agent; anti-inflammatory; antioxidant | Increased beneficial flora (Lactobacillus spp. and Bifidobacterium spp.) 201 mg/day of anthocyanins produced the reduction of TNF-α, related to cognitive improvement | Decreased C-reactive protein in women with metabolic syndrome | [295,296,297,298,299,300,301] |
| Resveratrol | Red grape, red wine, nuts | Antioxidant; anti-inflammatory; cryoprotective; interaction with the HPA axis; neurogenesis; involved in the regulation of monoamines | Clinical trials demonstrate its power to improve fatigue, anhedonia or sleep quality. There is no specific evidence of improvement of MDD in humans | Increased quality of life, benefit in somatic and physical symptoms in menopausal women | [302,303,304,305,306,307,308,309] |
| CBD | Supplements | Implicated in neurogenesis and neuroplasticity; neurotransmission | - | - | [311,312,313,314,315] |
| Prebiotics and probiotics | Yogurt, kefir, tempeh, miso, legumes, fruits, vegetables | Benefits for the development of a healthy bacterial ecosystem; modulation of neurotrophic factors (BDNF); gut-brain axis regulation; | Supplementation with commercial formulas of probiotics improves mood and memory. Prebiotics by themselves do not intervene in the state of health, but they are key for the optimization of probiotics | In women with PCOS, the combination of bacteria of the genus Lactobacillus and Bifidobacterium +200 μg/day of selenium had antioxidant and anti-inflammatory power and resulted in higher scores on the mental health questionnaires. | [316,317,318,319,320,321,322] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Montero, C.; Ortega, M.A.; Alvarez-Mon, M.A.; Fraile-Martinez, O.; Romero-Bazán, A.; Lahera, G.; Montes-Rodríguez, J.M.; Molina-Ruiz, R.M.; Mora, F.; Rodriguez-Jimenez, R.; et al. The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective. Nutrients 2022, 14, 1107. https://doi.org/10.3390/nu14051107
García-Montero C, Ortega MA, Alvarez-Mon MA, Fraile-Martinez O, Romero-Bazán A, Lahera G, Montes-Rodríguez JM, Molina-Ruiz RM, Mora F, Rodriguez-Jimenez R, et al. The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective. Nutrients. 2022; 14(5):1107. https://doi.org/10.3390/nu14051107
Chicago/Turabian StyleGarcía-Montero, Cielo, Miguel A. Ortega, Miguel Angel Alvarez-Mon, Oscar Fraile-Martinez, Adoración Romero-Bazán, Guillermo Lahera, José Manuel Montes-Rodríguez, Rosa M. Molina-Ruiz, Fernando Mora, Roberto Rodriguez-Jimenez, and et al. 2022. "The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective" Nutrients 14, no. 5: 1107. https://doi.org/10.3390/nu14051107
APA StyleGarcía-Montero, C., Ortega, M. A., Alvarez-Mon, M. A., Fraile-Martinez, O., Romero-Bazán, A., Lahera, G., Montes-Rodríguez, J. M., Molina-Ruiz, R. M., Mora, F., Rodriguez-Jimenez, R., Quintero, J., & Álvarez-Mon, M. (2022). The Problem of Malnutrition Associated with Major Depressive Disorder from a Sex-Gender Perspective. Nutrients, 14(5), 1107. https://doi.org/10.3390/nu14051107