
Feasibility of Food FARMacia: Mobile Food Pantry to Reduce Household Food Insecurity in Pediatric Primary Care

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Food FARMacia Pilot Program: Mobile Food Pantry Intervention to Reduce Food Insecurity
2.3. Outcome Measurements
2.3.1. Reach and Feasibility of Food FARMacia Pilot Program and Longitudinal Study
2.3.2. Feasibility of Food FARMacia Pilot Program and Longitudinal Study
2.4. Statistical Analysis
3. Results
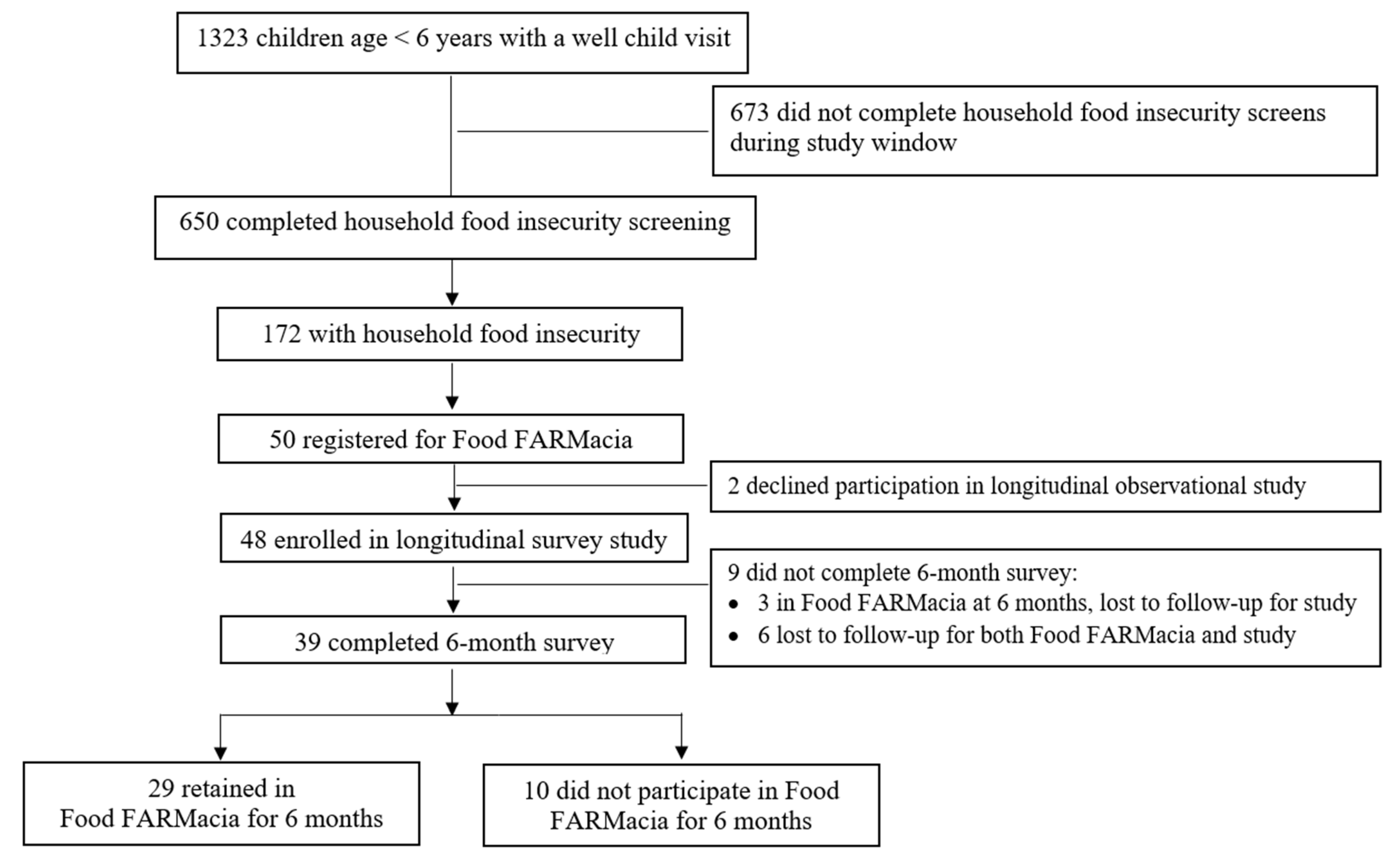
3.1. Reach of Food FARMacia Pilot Program
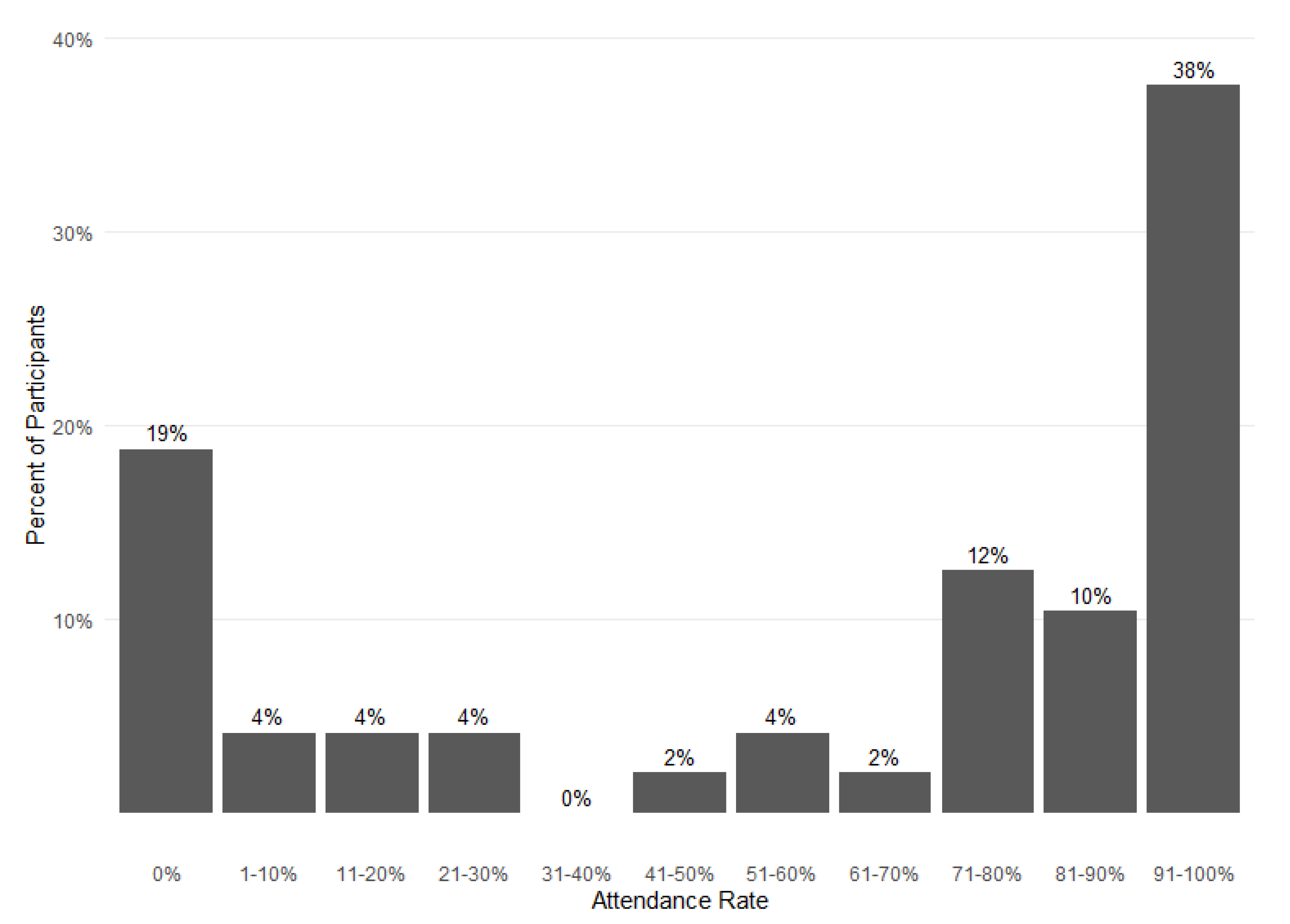
3.2. Feasibility of the Food FARMacia Pilot Program and Longitudinal Study
3.3. Characteristics of Participants Retained in The Food FARMacia Program
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Office of Disease Prevention and Health Promotion. Social Determinants of Health. Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health (accessed on 28 January 2019).
- IOM (Institute of Medicine). Capturing Social and Behavioral Domains and Measures in Electronic Health Records: Phase 2; National Academies Press: Washington, DC, USA, 2014. [Google Scholar]
- Daniel, H.; Bornstein, S.S.; Kane, G.C. Addressing Social Determinants to Improve Patient Care and Promote Health Equity: An American College of Physicians Position Paper. Ann. Intern. Med. 2018, 168, 577–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Council on Community Pediatrics. Poverty and Child Health in the United States. Pediatrics 2016, 137, e20160339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Marchis, E.H.; Torres, J.M.; Benesch, T.; Fichtenberg, C.; Allen, I.E.; Whitaker, E.M.; Gottlieb, L.M. Interventions Addressing Food Insecurity in Health Care Settings: A Systematic Review. Ann. Fam. Med. 2019, 17, 436–447. [Google Scholar] [CrossRef] [Green Version]
- Crossa, A.; Baquero, M.; Etheredge, A.J.; Seidl, L.; Nieves, C.; Dannefer, R.; Solomon, E.; Prasad, D.; Jasek, J.; Dongchung, T.Y.; et al. Food Insecurity and Access in New York City during the COVID-19 Pandemic, 2020. 2021. Available online: https://www1.nyc.gov/assets/doh/downloads/pdf/epi/databrief128.pdf (accessed on 14 February 2022).
- Suglia, S.F.; Duarte, C.S.; Chambers, E.C.; Boynton-Jarrett, R. Cumulative social risk and obesity in early childhood. Pediatrics 2012, 129, e1173–e1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmingsson, E.; Johansson, K.; Reynisdottir, S. Effects of childhood abuse on adult obesity: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 882–893. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Bateson, P.; Beedle, A.S.; Law, C.M.; Bhutta, Z.A.; Anokhin, K.V.; Bougneres, P.; Chandak, G.R.; Dasgupta, P.; et al. Towards a new developmental synthesis: Adaptive developmental plasticity and human disease. Lancet 2009, 373, 1654–1657. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J.; Osmond, C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet 1986, 1, 1077–1081. [Google Scholar] [CrossRef]
- Food Research & Action Center. Available online: https://frac.org/aaptoolkit (accessed on 17 February 2022).
- Black, M.M.; Quigg, A.M.; Cook, J.; Casey, P.H.; Cutts, D.B.; Chilton, M.; Meyers, A.; Ettinger de Cuba, S.; Heeren, T.; Coleman, S.; et al. WIC participation and attenuation of stress-related child health risks of household food insecurity and caregiver depressive symptoms. Arch. Pediatrics Adolesc. Med. 2012, 166, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Gany, F.; Lee, T.; Loeb, R.; Ramirez, J.; Moran, A.; Crist, M.; McNish, T.; Leng, J.C. Use of Hospital-Based Food Pantries among Low-Income Urban Cancer Patients. J. Community Health 2015, 40, 1193–1200. [Google Scholar] [CrossRef] [Green Version]
- Berkowitz, S.A.; Delahanty, L.M.; Terranova, J.; Steiner, B.; Ruazol, M.P.; Singh, R.; Shahid, N.N.; Wexler, D.J. Medically Tailored Meal Delivery for Diabetes Patients with Food Insecurity: A Randomized Cross-over Trial. J. Gen. Intern. Med. 2019, 34, 396–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bryce, R.; Guajardo, C.; Ilarraza, D.; Milgrom, N.; Pike, D.; Savoie, K.; Valbuena, F.; Miller-Matero, L.R. Participation in a farmers’ market fruit and vegetable prescription program at a federally qualified health center improves hemoglobin A1C in low income uncontrolled diabetics. Prev. Med. Rep. 2017, 7, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.A.; Choi, S.K.; Hurley, T.; Anadu, E.; Hébert, J.R. A farmers’ market at a federally qualified health center improves fruit and vegetable intake among low-income diabetics. Prev. Med. 2013, 56, 288–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downer, S.; Berkowitz, S.A.; Harlan, T.S.; Olstad, D.L.; Mozaffarian, D. Food is medicine: Actions to integrate food and nutrition into healthcare. Bmj 2020, 369, m2482.19. [Google Scholar] [CrossRef] [PubMed]
- Wright, B.N.; Bailey, R.L.; Craig, B.A.; Mattes, R.D.; McCormack, L.; Stluka, S.; Franzen-Castle, L.; Henne, B.; Mehrle, D.; Remley, D.; et al. Daily Dietary Intake Patterns Improve after Visiting a Food Pantry among Food-Insecure Rural Midwestern Adults. Nutrients 2018, 10, 583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, K.S.; Wu, R.; Wolff, M.; Colantonio, A.G.; Grady, J. A novel food pantry program: Food security, self-sufficiency, and diet-quality outcomes. Am. J. Prev. Med. 2013, 45, 569–575. [Google Scholar] [CrossRef]
- Eicher-Miller, H.A. A review of the food security, diet and health outcomes of food pantry clients and the potential for their improvement through food pantry interventions in the United States. Physiol. Behav. 2020, 220, 112871. [Google Scholar] [CrossRef]
- An, R.; Wang, J.; Liu, J.; Shen, J.; Loehmer, E.; McCaffrey, J. A systematic review of food pantry-based interventions in the USA. Public Health Nutr. 2019, 22, 1704–1716. [Google Scholar] [CrossRef]
- Marmash, D.; Ha, K.; Sakaki, J.R.; Gorski, I.; Rule, B.; Foster, J.; Puglisi, M.; Chun, O.K. Diet Quality, Nutritional Adequacy, and Sociodemographic Characteristics of Mobile Food Pantry Users in Northeastern Connecticut. Nutrients 2021, 13, 1099. [Google Scholar] [CrossRef]
- City of New York. New York City Census Fact Finder. Available online: https://popfactfinder.planning.nyc.gov/#12.25/40.724/-73.9868 (accessed on 18 July 2016).
- Billioux, A.; Verlander, K.; Anthony, S.; Alley, D.E. Standardized Screening for Health-Related Social Needs in Clinical Settings: The Accountable Health Communities Screening Tool; National Academy of Medicine: Washington, DC, USA, 2017. [Google Scholar] [CrossRef] [Green Version]
- Hager, E.R.; Quigg, A.M.; Black, M.M.; Coleman, S.M.; Heeren, T.; Rose-Jacobs, R.; Cook, J.T.; Ettinger de Cuba, S.A.; Casey, P.H.; Chilton, M.; et al. Development and validity of a 2-item screen to identify families at risk for food insecurity. Pediatrics 2010, 126, e26–e32. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.; Malinak, D.; Chang, J.; Perez, M.; Perez, S.; Settlecowski, E.; Rodriggs, T.; Hsu, M.; Abrew, A.; Aedo, S. Implementation of a food insecurity screening and referral program in student-run free clinics in San Diego, California. Prev. Med. Rep. 2017, 5, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Hickey, E.; Phan, M.; Beck, A.F.; Burkhardt, M.C.; Klein, M.D. A Mixed-Methods Evaluation of a Novel Food Pantry in a Pediatric Primary Care Center. Clin. Pediatrics 2020, 59, 278–284. [Google Scholar] [CrossRef]
- Center on Budget and Policy Priorities. Available online: https://www.cbpp.org/research/food-assistance/wic-works-addressing-the-nutrition-and-health-needs-of-low-income-families (accessed on 14 February 2022).
- Masciale, M.; Lopez, M.A.; Yu, X.; Domínguez, J.; Fredricks, K.; Haq, H.; Raphael, J.L.; Bocchini, C. Public Benefit Use and Social Needs in Hospitalized Children with Undocumented Parents. Pediatrics 2021, 148, e2020021113. [Google Scholar] [CrossRef] [PubMed]
- Pelto, D.J.; Ocampo, A.; Garduño-Ortega, O.; Barraza López, C.T.; Macaluso, F.; Ramirez, J.; González, J.; Gany, F. The Nu-trition Benefits Participation Gap: Barriers to Uptake of SNAP and WIC among Latinx American Immigrant Families. J. Community Health 2020, 45, 488–491. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.W.; Hoffnagle, E.E.; Lindsay, A.C.; Lofink, H.E.; Hoffman, V.A.; Turrell, S.; Willett, W.C.; Blumenthal, S.J. A qual-itative study of diverse experts’ views about barriers and strategies to improve the diets and health of Supplemental Nutrition Assistance Program (SNAP) beneficiaries. J. Acad. Nutr. Diet. 2013, 113, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, L.; Gundersen, C.; Baylis, K.; Saksena, M. The Use of Charitable Food Assistance among Low-Income Households in the United States. J. Acad. Nutr. Diet. 2021, 121, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Twersky, S.E. Restrictive state laws aimed at immigrants: Effects on enrollment in the food stamp program by U.S. citizen children in immigrant families. PLoS ONE 2019, 14, e0215327. [Google Scholar] [CrossRef] [Green Version]
- Ettinger de Cuba, S.A.; Bovell-Ammon, A.R.; Cook, J.T.; Coleman, S.M.; Black, M.M.; Chilton, M.M.; Casey, P.H.; Cutts, D.B.; Heeren, T.C.; Sandel, M.T.; et al. SNAP, Young Children’s Health, and Family Food Security and Healthcare Access. Am. J. Prev. Med. 2019, 57, 525–532. [Google Scholar] [CrossRef]
- Criss, S.; Woo Baidal, J.A.; Goldman, R.E.; Perkins, M.; Cunningham, C.; Taveras, E.M. The Role of Health Information Sources in Decision-Making among Hispanic Mothers during Their Children’s First 1000 Days of Life. Matern. Child Health J. 2015, 19, 2536–2543. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Child Characteristics | Overall Patient Population (N = 650) | Patients with Household Food Insecurity (N = 172) | Food FARMacia Participants (N = 50) |
|---|---|---|---|
| Child Age, mean (SD), months | 19.6 (20.5) | 21.1 (22.1) | 22.0 (18.4) |
| Child Age, n (%), years | |||
| 0 to <1 | 324 (49.8) | 84 (49) | 17 (34) |
| 1 to <2 | 107 (16.5) | 25 (15) | 12 (24) |
| 2 to <6 | 219 (33.7) | 63 (37) | 21 (42) |
| Female, n (%) | 326 (50.2) | 88 (51) | 20 (40) |
| Race/ethnicity, n (%) a | |||
| Hispanic/Latino | 546 (90.5) | 148 (91) | 44 (88) |
| White, not Hispanic/Latino | 15 (2.5) | 1 (1) | 1 (2) |
| Black, not Hispanic/Latino | 28 (4.7) | 10 (6) | 4 (8) |
| Other, not Hispanic/Latino | 14 (2.3) | 4 (2) | 1 (2) |
| Household Characteristics | |||
| Household size, mean (SD) | 4.1 (1.4) | 4.2 (1.5) | 4.2 (1.2) |
| Annual household income, n (%) | |||
| <USD 10 k | 174 (26.8) | 58 (34) | 18 (36) |
| USD 10 k to <20 k | 166 (25.5) | 44 (26) | 10 (20) |
| >USD 20 k | 225 (34.6) | 38 (22) | 9 (18) |
| Missing | 85 (13.1) | 32 (18) | 13 (26) |
| Health Related Social Needs (HRSN) | |||
| ≥2 ED visits past year, n (%) d | 120 (18.7) | 40 (24) | 11 (25) |
| HRSN Type, n (%) | |||
| Household food insecurity | 172 (26.5) | 172 (100) | 50 (100) |
| Housing needs b | 133 (20.7) | 74 (45) | 18 (39) |
| Kitchen problems b | 51 (7.9) | 22 (13) | 1 (2) |
| Transportation needs c | 68 (10.6) | 47 (29) | 7 (16) |
| Utility needs d | 40 (6.2) | 27 (16) | 7 (16) |
| Safety concerns b | 7 (1.1) | 5 (3) | 1 (2) |
| Number of HRSN, n (%) | |||
| None | 394 (60.6) | 0 | 0 |
| 1 HRSN | 145 (22.3) | 71 (41) | 25 (50) |
| 2 HRSN | 71 (10.9) | 62 (36) | 19 (38) |
| 3 HRSN | 30 (4.6) | 29 (17) | 4 (8) |
| 4 HRSN | 7 (1.1) | 7 (4) | 2 (4) |
| 5 HRSN | 3 (0.5) | 3 (2) | 0 |
| Food FARMacia at 6 Months | ||||
|---|---|---|---|---|
| Overall (N = 48) | Retained (N = 32) | Attrition (N = 16) | p-Value a | |
| Child Baseline Characteristics | ||||
| Child Age, mean (SD), months | 21.8 (18.4) | 26.7 (18.7) | 12.1 (13.8) | 0.01 |
| Child Age, n (%), years | 0.01 | |||
| 0 to <1 | 17 (35) | 9 (28) | 8 (50) | |
| 1 to <2 | 11 (23) | 5 (16) | 6 (38) | |
| 2 to <6 | 20 (42) | 18 (56) | 2 (12) | |
| Female, n (%) | 19 (40) | 12 (38) | 7 (44) | 0.92 |
| Race/ethnicity, n (%) | <0.01 | |||
| Hispanic/Latino | 42 (88) | 31 (97) | 11 (69) | |
| White, not Hispanic/Latino | 1 (2) | 1 (3) | 0 (0) | |
| Black, not Hispanic/Latino | 4 (8) | 0 (0) | 4 (25) | |
| Other, not Hispanic/Latino | 1 (2) | 0 (0) | 1 (6) | |
| Parental Baseline Characteristics | ||||
| Female, n (%) | 48 (100) | 32 (100) | 16 (100) | 1.00 |
| Spanish Language, n (%) | 36 (75) | 26 (81) | 10 (63) | 0.18 |
| Education level | 0.54 | |||
| Elementary School or less | 11 (23) | 9 (28) | 2 (12) | |
| Some High School | 11 (23) | 6 (19) | 5 (31) | |
| High School Graduate | 15 (31) | 11(34) | 4 (25) | |
| Some college | 7 (15) | 4 (12) | 3 (19) | |
| College graduate | 4 (8) | 2 (6) | 2 (12) | |
| Household Characteristic | ||||
| Household size, mean (SD) | 4.2 (1.3) | 4.5 (1.1) | 3.7 (1.4) | 0.04 |
| Annual household income, n (%) | 0.29 | |||
| <USD 10 k | 18 (38) | 10 (31) | 8 (50) | |
| USD 10 k or more | 17 (35) | 13 (41) | 4 (25) | |
| Missing/Unknown | 13 (27) | 9 (28) | 4 (25) | |
| WIC Enrollment, Yes, n (%) | 47 (98) | 31 (97) | 16 (100) | 1.00 |
| SNAP Enrollment, n (%) | 0.16 | |||
| Yes | 26 (54) | 17 (53) | 9 (56) | |
| No, but received in past | 12 (25) | 6 (19) | 6 (38) | |
| Never | 10 (21) | 9 (28) | 1 (6) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo Baidal, J.A.; Meyer, D.; Partida, I.; Duong, N.; Rosenthal, A.; Hulse, E.; Nieto, A.; on behalf of the HERALD Collaborative. Feasibility of Food FARMacia: Mobile Food Pantry to Reduce Household Food Insecurity in Pediatric Primary Care. Nutrients 2022, 14, 1059. https://doi.org/10.3390/nu14051059
Woo Baidal JA, Meyer D, Partida I, Duong N, Rosenthal A, Hulse E, Nieto A, on behalf of the HERALD Collaborative. Feasibility of Food FARMacia: Mobile Food Pantry to Reduce Household Food Insecurity in Pediatric Primary Care. Nutrients. 2022; 14(5):1059. https://doi.org/10.3390/nu14051059
Chicago/Turabian StyleWoo Baidal, Jennifer A., Dodi Meyer, Ivette Partida, Ngoc Duong, Alyson Rosenthal, Emma Hulse, Andres Nieto, and on behalf of the HERALD Collaborative. 2022. "Feasibility of Food FARMacia: Mobile Food Pantry to Reduce Household Food Insecurity in Pediatric Primary Care" Nutrients 14, no. 5: 1059. https://doi.org/10.3390/nu14051059
APA StyleWoo Baidal, J. A., Meyer, D., Partida, I., Duong, N., Rosenthal, A., Hulse, E., Nieto, A., & on behalf of the HERALD Collaborative. (2022). Feasibility of Food FARMacia: Mobile Food Pantry to Reduce Household Food Insecurity in Pediatric Primary Care. Nutrients, 14(5), 1059. https://doi.org/10.3390/nu14051059