
Oral Intake of L-Ornithine-L-Aspartate Is Associated with Distinct Microbiome and Metabolome Changes in Cirrhosis

 , and
, and 
Abstract
:1. Introduction
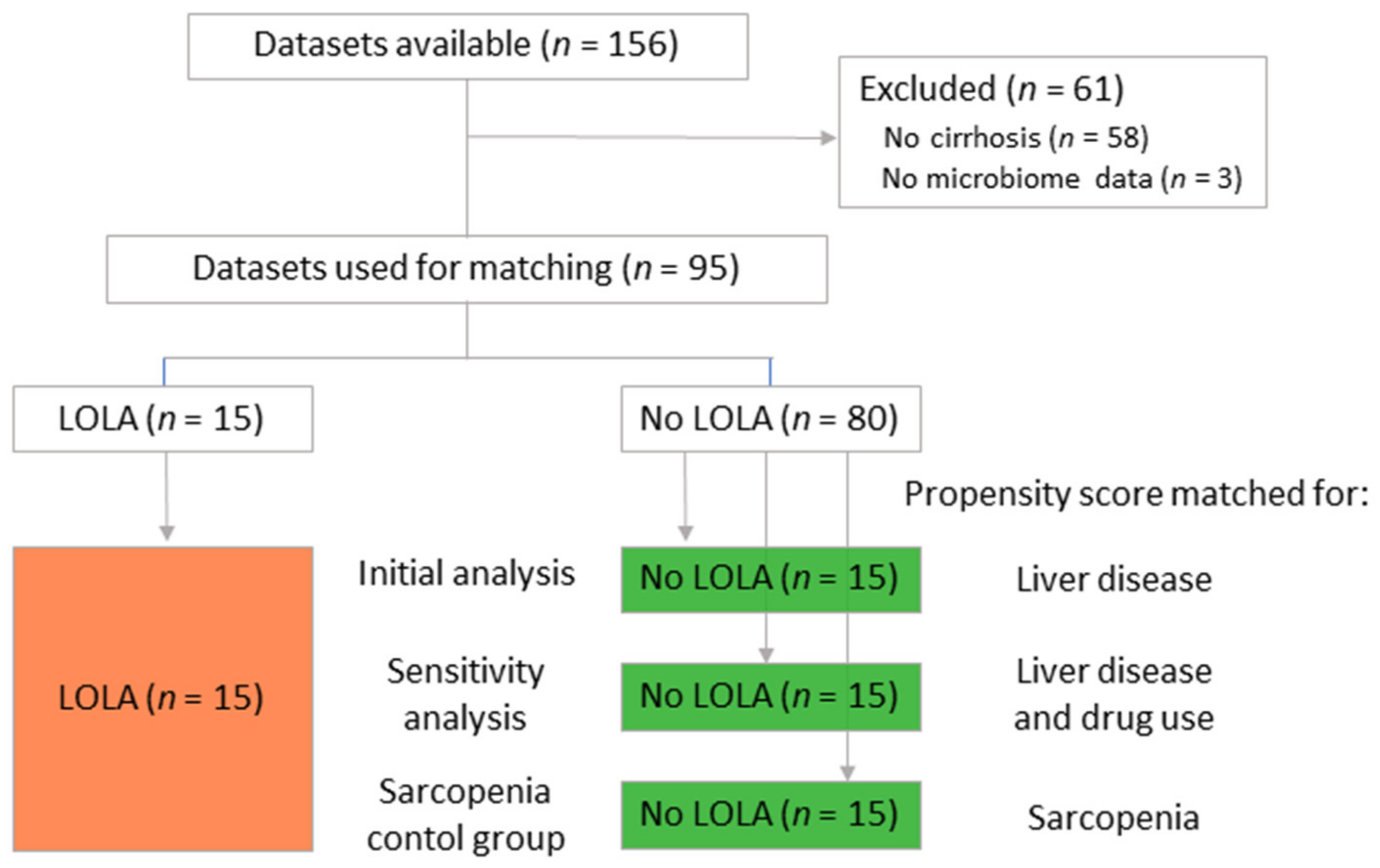
2. Materials and Methods
3. Results
3.1. Patient Characteristics
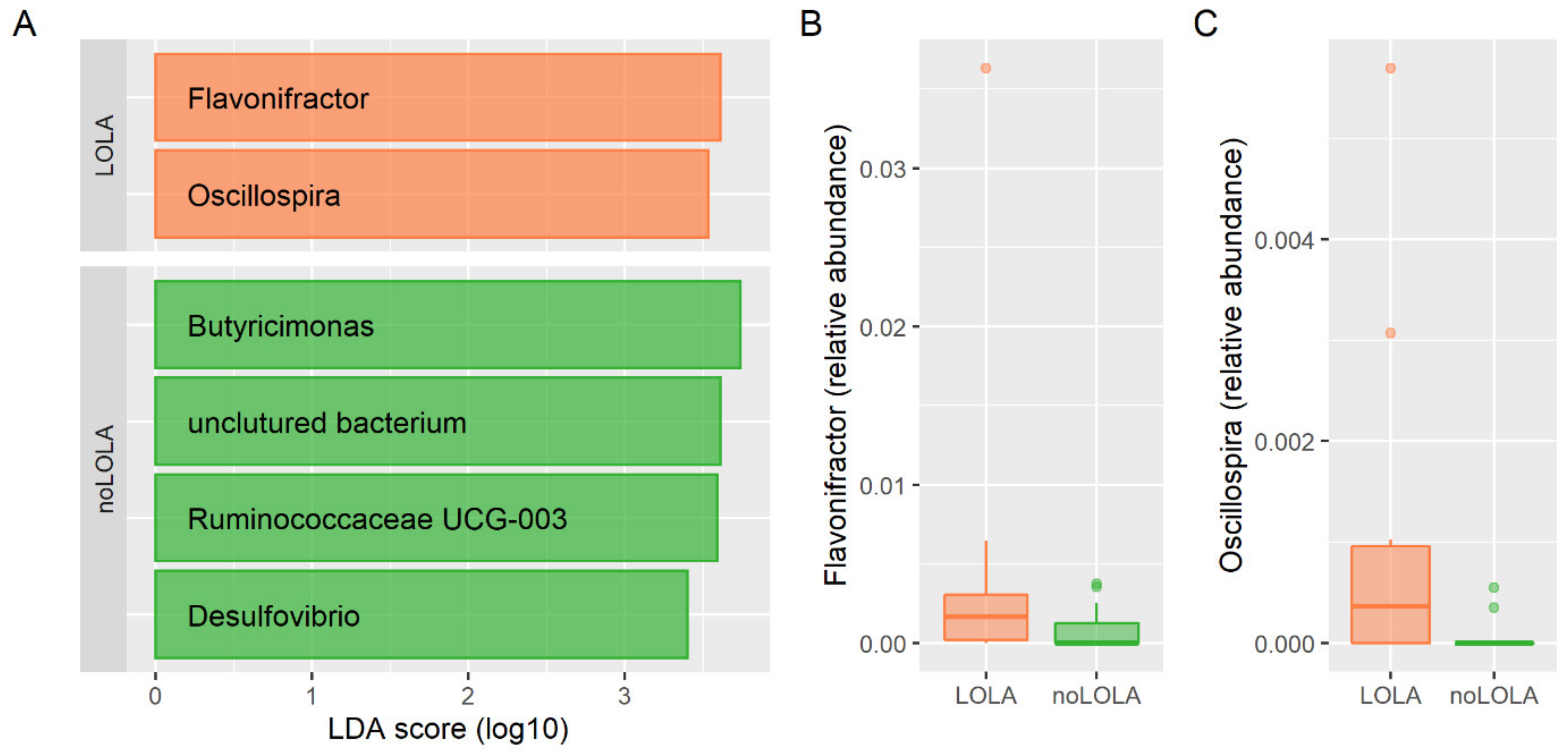
3.2. Association of LOLA Intake with Microbiome Composition
3.3. Metabolomic Analysis of Urine, Stool and Serum Samples
3.3.1. Urine Metabolome
3.3.2. Stool Metabolome
3.3.3. Serum Metabolome
3.4. Serum- and Fecal-Targeted Metabolomics and Clinical Characteristics
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pimpin, L.; on behalf of the HEPAHEALTH Steering Committee. HEPAHEALTH Project Report; Europeal Association for the Study of the Liver: Geneva, Switzerland, 2018. [Google Scholar]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijdicks, E.F. Hepatic Encephalopathy. N. Engl. J. Med. 2016, 375, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Olde Damink, S.W.; Jalan, R.; Dejong, C.H. Interorgan ammonia trafficking in liver disease. Metab. Brain Dis. 2009, 24, 169–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butterworth, R.F. Role of circulating neurotoxins in the pathogenesis of hepatic encephalopathy: Potential for improvement following their removal by liver assist devices. Liver Int. 2003, 23 (Suppl. 3), 5–9. [Google Scholar] [CrossRef]
- Butterworth, R.F. Hepatic encephalopathy in alcoholic cirrhosis. Handb. Clin. Neurol. 2014, 125, 589–602. [Google Scholar] [CrossRef]
- American Association for the Study of Liver; European Association for the Study of the Liver. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef] [Green Version]
- Blanco Vela, C.I.; Poo Ramirez, J.L. Efficacy of oral L-ornithine L-aspartate in cirrhotic patients with hyperammonemic hepatic encephalopathy. Ann. Hepatol. 2011, 10 (Suppl. 2), S55–S59. [Google Scholar] [CrossRef]
- Kircheis, G.; Luth, S. Pharmacokinetic and Pharmacodynamic Properties of L-Ornithine L-Aspartate (LOLA) in Hepatic Encephalopathy. Drugs 2019, 79, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Gustot, T.; Stadlbauer, V.; Laleman, W.; Alessandria, C.; Thursz, M. Transition to decompensation and acute-on-chronic liver failure: Role of predisposing factors and precipitating events. J. Hepatol. 2021, 75 (Suppl. 1), S36–S48. [Google Scholar] [CrossRef]
- Qin, N.; Yang, F.; Li, A.; Prifti, E.; Chen, Y.; Shao, L.; Guo, J.; Le Chatelier, E.; Yao, J.; Wu, L.; et al. Alterations of the human gut microbiome in liver cirrhosis. Nature 2014, 513, 59–64. [Google Scholar] [CrossRef]
- Stadlbauer, V.; Komarova, I.; Klymiuk, I.; Durdevic, M.; Reisinger, A.; Blesl, A.; Rainer, F.; Horvath, A. Disease severity and proton pump inhibitor use impact strongest on faecal microbiome composition in liver cirrhosis. Liver Int. 2020, 40, 866–877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, L.; Pruteanu, M.; Kuhn, M.; Zeller, G.; Telzerow, A.; Anderson, E.E.; Brochado, A.R.; Fernandez, K.C.; Dose, H.; Mori, H.; et al. Extensive impact of non-antibiotic drugs on human gut bacteria. Nature 2018, 555, 623–628. [Google Scholar] [CrossRef] [PubMed]
- R_Core_Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Ho, D.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric Preprocessing for Parametric Causal Inference. J. Stat. Softw. 2011, 42, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Estaki, M.; Jiang, L.; Bokulich, N.A.; McDonald, D.; González, A.; Kosciolek, T.; Martino, C.; Zhu, Q.; Birmingham, A.; Vázquez-Baeza, Y.; et al. QIIME 2 Enables Comprehensive End-to-End Analysis of Diverse Microbiome Data and Comparative Studies with Publicly Available Data. Curr. Protoc. Bioinform. 2020, 70, e100. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski, M.; Proietti, C.; Ellis, J.J.; Hasan, S.; Brion, M.J.; Berger, B.; Krause, L. Calypso: A user-friendly web-server for mining and visualizing microbiome-environment interactions. Bioinformatics 2017, 33, 782–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stryeck, S.; Gastrager, M.; Degoricija, V.; Trbusic, M.; Potocnjak, I.; Radulovic, B.; Pregartner, G.; Berghold, A.; Madl, T.; Frank, S. Serum Concentrations of Citrate, Tyrosine, 2- and 3- Hydroxybutyrate are Associated with Increased 3-Month Mortality in Acute Heart Failure Patients. Sci. Rep. 2019, 9, 6743. [Google Scholar] [CrossRef]
- Zhou, Q.; Kerbl-Knapp, J.; Zhang, F.; Korbelius, M.; Kuentzel, K.B.; Vujić, N.; Akhmetshina, A.; Hörl, G.; Paar, M.; Steyrer, E.; et al. Metabolomic Profiles of Mouse Tissues Reveal an Interplay between Aging and Energy Metabolism. Metabolites 2022, 12, 17. [Google Scholar] [CrossRef]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.E.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Wickham, H.; Bryan, J. Readxl: Read Excel Files. R Package Version 1.3.1. 2019. Available online: https://CRAN.R-project.org/package=readxl (accessed on 21 June 2021).
- Ooms, J. writexl: Export Data Frames to Excel ‘xlsx’ Format. R Package Version 1.3.1. 2020. Available online: https://CRAN.R-project.org/package=writexl (accessed on 21 June 2021).
- Alboukadel, K. ggpubr: ‘ggplot2’ Based Publication Ready Plots. R Package Version 0.4.0. 2020. Available online: https://CRAN.R-project.org/package=ggpubr (accessed on 21 June 2021).
- Mikami, A.; Ogita, T.; Namai, F.; Shigemori, S.; Sato, T.; Shimosato, T. Oral Administration of Flavonifractor plautii, a Bacteria Increased with Green Tea Consumption, Promotes Recovery From Acute Colitis in Mice via Suppression of IL-17. Front. Nutr. 2020, 7, 610946. [Google Scholar] [CrossRef]
- Rosés, C.; Cuevas-Sierra, A.; Quintana, S.; Riezu-Boj, J.I.; Martínez, J.A.; Milagro, F.I.; Barceló, A. Gut Microbiota Bacterial Species Associated with Mediterranean Diet-Related Food Groups in a Northern Spanish Population. Nutrients 2021, 13, 636. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Wen, S.W.; Kaminga, A.C.; Liu, A. Gut metabolites and inflammation factors in non-alcoholic fatty liver disease: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 8848. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Sun, C.; Li, Y.; Wang, T.; Jia, L.; Lai, S.; Yang, Y.; Luo, P.; Dai, D.; Yang, Y.Q.; et al. GMrepo: A database of curated and consistently annotated human gut metagenomes. Nucleic Acids Res. 2020, 48, D545–D553. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Dhakan, D.B.; Maji, A.; Saxena, R.; Vishnu Prasoodanan, K.V.; Mahajan, S.; Pulikkan, J.; Kurian, J.; Gomez, A.M.; Scaria, J.; et al. Association of Flavonifractor plautii, a Flavonoid-Degrading Bacterium, with the Gut Microbiome of Colorectal Cancer Patients in India. mSystems 2019, 4, e00438-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.R.; Zheng, H.M.; Zhang, G.X.; Chen, F.L.; Chen, L.D.; Yang, Z.C. High Oscillospira abundance indicates constipation and low BMI in the Guangdong Gut Microbiome Project. Sci. Rep. 2020, 10, 9364. [Google Scholar] [CrossRef] [PubMed]
- Konikoff, T.; Gophna, U. Oscillospira: A Central, Enigmatic Component of the Human Gut Microbiota. Trends Microbiol. 2016, 24, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Trieb, M.; Rainer, F.; Stadlbauer, V.; Douschan, P.; Horvath, A.; Binder, L.; Trakaki, A.; Knuplez, E.; Scharnagl, H.; Stojakovic, T.; et al. HDL-related biomarkers are robust predictors of survival in patients with chronic liver failure. J. Hepatol. 2020, 73, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Trieb, M.; Horvath, A.; Birner-Gruenberger, R.; Spindelboeck, W.; Stadlbauer, V.; Taschler, U.; Curcic, S.; Stauber, R.E.; Holzer, M.; Pasterk, L.; et al. Liver disease alters high-density lipoprotein composition, metabolism and function. Biochim. Biophys. Acta 2016, 1861, 630–638. [Google Scholar] [CrossRef] [Green Version]
- Hempel, J.M.; Greif-Higer, G.; Kaufmann, T.; Beutel, M.E. Detection of alcohol consumption in patients with alcoholic liver cirrhosis during the evaluation process for liver transplantation. Liver Transpl. 2012, 18, 1310–1315. [Google Scholar] [CrossRef]
- Braune, A.; Blaut, M. Bacterial species involved in the conversion of dietary flavonoids in the human gut. Gut Microbes 2016, 7, 216–234. [Google Scholar] [CrossRef] [Green Version]
- Candry, P.; Ulcar, B.; Petrognani, C.; Rabaey, K.; Ganigué, R. Ethanol:propionate ratio drives product selectivity in odd-chain elongation with Clostridium kluyveri and mixed communities. Bioresour. Technol. 2020, 313, 123651. [Google Scholar] [CrossRef] [PubMed]
- Bloom, P.P.; Luévano, J.M., Jr.; Miller, K.J.; Chung, R.T. Deep stool microbiome analysis in cirrhosis reveals an association between short-chain fatty acids and hepatic encephalopathy. Ann. Hepatol. 2021, 25, 100333. [Google Scholar] [CrossRef] [PubMed]
- Holecek, M. Ammonia and amino acid profiles in liver cirrhosis: Effects of variables leading to hepatic encephalopathy. Nutrition 2015, 31, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.; Michalak, A.; Rao, K.V.; Quack, G.; Kircheis, G.; Butterworth, R.F. L-ornithine-L-aspartate lowers plasma and cerebrospinal fluid ammonia and prevents brain edema in rats with acute liver failure. Hepatology 1999, 30, 636–640. [Google Scholar] [CrossRef]
- Kowalski, P.; Bieniecki, M. Pharmacokinetics and bioavailability study of L-ornithine-L-aspartate in healthy volunteers--a comparative study of two oral formulations. J. Pharm. Biomed. Anal. 2006, 41, 1061–1064. [Google Scholar] [CrossRef]
- Butterworth, R.F. L-Ornithine L-Aspartate for the Treatment of Sarcopenia in Chronic Liver Disease: The Taming of a Vicious Cycle. Can. J. Gastroenterol. Hepatol. 2019, 2019, 8182195. [Google Scholar] [CrossRef]
- Cheng, C.H.; Yang, F.F.; Liao, S.A.; Miao, Y.T.; Ye, C.X.; Wang, A.L. Effect of acute ammonia exposure on expression of GH/IGF axis genes GHR1, GHR2 and IGF-1 in pufferfish (Takifugu obscurus). Fish. Physiol. Biochem. 2015, 41, 495–507. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | LOLA (n = 15) | noLOLA (n = 15) | p Value |
|---|---|---|---|
| Age | 63 (6.5) | 61 (15.1) | 0.9 |
| Sex (m/f) | 13/2 (87/13%) | 11/4 (73/27%) | 0.7 |
| Etiology (Alc/Non-alc) | 10/5 (67/33%) | 9/6 (60/40%) | 0.7 |
| Child-Pugh score | 7 (1.5) * | 7 (1.5) * | >0.99 |
| MELD score | 12.8 (3.3) | 11.9 (2.7) | 0.5 |
| PPI use/non-use | 7/8 (47/53%) | 6/9 (40/60%) | >0.99 |
| Lactulose use/non-use | 5/10 (33/67%) | 3/12 (20/80%) | 0.7 |
| Non-absorbable antibiotics use/non-use | 4/11 (36/64%) | 0/15 (0/100%) | 0.1 |
| Sarcopenia diagnosis (no/pre-/sarcopenia) | 3/3/9 (20/20/60%) | 6/3/6 (40/20/40%) | 0.4 |
| LOLA (n = 15) | noLOLA (n = 15) | p Value | |
|---|---|---|---|
| Age (years) | 63 (6.5) | 62 (7.7) | 0.5 |
| Gender (m/f) | 13/2 (87/13%) | 10/5 (67/33%) | 0.4 |
| Etiology (Alc/Non-alc) | 10/5 (67/33%) | 10/5 (67/33%) | >0.99 |
| Child-Pugh score | 7 (1.5) * | 7 (2.5) * | 0.3 |
| MELD score | 12.8 (3.3) | 12.7 (4.3) | 0.9 |
| PPI use/non-use | 7/8 (47/53%) | 7/8 (47/53%) | >0.99 |
| Lactulose use/non-use | 5/10 (33/67%) | 4/11 (36/64%) | >0.99 |
| Non-absorbable antibiotics use/non-use | 4/11 (36/64%) | 0/15 (0/100%) | 0.1 |
| Sarcopenia diagnosis (no/pre-/sarcopenia) | 3/3/9 (20/20/60%) | 7/3/5 (47/20/33%) | 0.3 |
| Initial Analysis | Sensitivity Analysis | |||||
|---|---|---|---|---|---|---|
| Biomarker | LOLA | noLOLA | AUROC (95%CI) | LOLA | noLOLA | AUROC (95%CI) |
| Ethanol to acetic acid ratio | −0.59 (0.85) | 0.30 (0.51) | 0.83 (0.61–0.95) | −0.46 (0.78) | 0.07 (0.64) | 0.76 (0.54–0.92) |
| Ethanol | −0.11 (0.60) | 0.00 (0.63) | 0.60 (0.37–0.80) | −0.02 (0.54) | −0.16 (0.84) | 0.53 (0.31–0.78) |
| Acetic acid | 0.42 (0.91) | −0.27 (0.79) | 0.68 (0.46–0.87) | 0.42 (0.87) | −0.24 (0.8) | 0.69 (0.78–0.88) |
| Initial Analysis | Sensitivity Analysis | |||||
|---|---|---|---|---|---|---|
| Biomarker/Ratio | LOLA | noLOLA | AUROC (95%CI) | LOLA | noLOLA | AUROC (95%CI) |
| Propylene glycerol to isopropyl alcohol | 0.54 (0.77) | −0.62 (0.93) | 0.84 (0.65–0.96) | 0.46 (0.77) | −0.67 (1.00) | 0.78 (0.56–0.93) |
| Propylene glycerol to valeric acid | 0.59 (1.01) | −0.40 (0.86) | 0.74 (0.52–0.89) | 0.57 (0.91) | −0.28 (0.85) | 0.76 (0.53–0.90) |
| Valeric acid to glycerol | −0.23 (1.00) | 0.41 (0.78) | 0.73 (0.51–0.90) | −0.19 (0.98) | 0.12 (0.63) | 0.72 (0.49–0.89) |
| Propylene glycerol | 0.30 (1.30) | −0.08 (0.70) | 0.65 (0.42–0.82) | 0.31 (0.98) | −0.25 (1.02) | 0.65 (0.40–0.84) |
| Isopropyl alcohol | −0.21 (1.04) | 0.44 (0.83) | 0.69 (0.47–0.87) | −0.06 (0.88) | 0.24 (1.22) | 0.62 (0.38–0.82) |
| Valeric acid | −0.27 (1.28) | 0.32 (0.74) | 0.36 (0.19–0.58) | −0.13 (0.87) | −0.03 (1.21) | 0.67 (0.47–0.88) |
| Glycerol | 0.07 (1.09) | −0.24 (0.85) | 0.62 (0.42–0.82) | 0.08 (0.97) | −0.15 (1.02) | 0.61 (0.39–0.81) |
| Initial Analysis | Sensitivity Analysis | |||||
|---|---|---|---|---|---|---|
| Biomarkers/Ratios | LOLA | noLOLA | AUROC (95%CI) | LOLA | noLOLA | AUROC (95%CI) |
| Ornithine | 0.53 (1.06) | –0.42 (0.85) | 0.76 (0.57–0.93) | 0.54 (1.04) | –0.38 (0.87) | 0.78 (0.59–0.93) |
| Isoleucine | −0.54 (1.23) | 0.37 (0.59) | 0.79 (0.57–0.93) | –0.51 (0.98) | 0.46 (0.88) | 0.76 (0.54–0.92) |
| Leucine | –0.37 (1.24) | 0.36 (0.57) | 0.74 (0.52–0.92) | –0.35 (1.07) | 0.54 (0.7) | 0.73 (0.50–0.90) |
| Isoleucine to ornithine | –0.7 (0.9) | 0.52 (0.77) | 0.88 (0.70–0.97) | –0.8 (0.94) | 0.62 (0.62) | 0.91 (0.77–1.00) |
| Acetone to ornithine | –0.58 (0.97) | 0.51 (0.83) | 0.83 (0.63–0.95) | –0.52 (0.99) | 0.37 (0.76) | 0.75 (0.54–0.92) |
| Lysine to ornithine | –0.53 (1.04) | 0.46 (0.71) | 0.82 (0.63–0.96) | –0.54 (1.10) | 0.53 (0.72) | 0.82 (0.64–0.98) |
| Leucine to ornithine | –0.55 (1.16) | 0.46 (0.61) | 0.84 (0.67–0.90) | –0.58 (1.16) | 0.56 (0.64) | 0.87 (0.70–0.98) |
| Ethanol to ornithine | –0.54 (0.95) | 0.49 (0.87) | 0.81 (0.61–0.95) | –0.52 (1.03) | 0.46 (0.84) | 0.80 (0.60–0.95) |
| Ornithine to threonine | 0.55 (1.05) | –0.52 (0.77) | 0.83 (0.66–0.96) | 0.64 (0.93) | –0.49 (0.72) | 0.90 (0.75–0.98) |
| Aspartic acid to ornithine | –0.62 (1.1) | 0.46 (0.71) | 0.82 (0.62–0.97) | –0.6 (1.07) | 0.38 (0.60) | 0.79 (0.58–0.93) |
| Ornithine to serine | 0.56 (1.08) | –0.5 (0.74) | 0.82 (0.61–0.95) | 0.59 (0.95) | –0.34 (0.63) | 0.86 (0.65–0.97) |
| Valine to ornithine | –0.57 (1.14) | 0.41 (0.66) | 0.78 (0.60–0.93) | –0.62 (1.19) | 0.52 (0.59) | 0.85 (0.66–0.99) |
| Arginine to ornithine | –0.49 (1.07) | 0.41 (0.73) | 0.78 (0.57–0.92) | –0.52 (1.06) | 0.37 (0.63) | 0.82 (0.64–0.97) |
| Acetone | –0.27 (0.75) | 0.37 (1.05) | 0.70 (0.46–0.88) | 0.05 (0.74) | 0.01 (1.00) | 0.54 (0.31–0.75) |
| Lysine | –0.18 (0.63) | 0.25 (0.90) | 0.72 (0.48–0.90) | –0.07 (0.53) | 0.38 (0.90) | 0.72 (0.50–0.89) |
| Ethanol | –0.05 (0.85) | 0.27 (0.88) | 0.61 (0.41–0.81) | 0.21 (0.74) | 0.13 (1.04) | 0.50 (0.29–0.74) |
| Threonine | –0.07 (1.11) | 0.22 (0.92) | 0.63 (0.36–0.83) | –0.30 (0.92) | 0.28 (0.85) | 0.74 (0.51–0.89) |
| Aspartic acid | –0.29 (0.80) | 0.17 (1.19) | 0.56 (0.34–0.76) | –0.25 (0.76) | 0.09 (1.21) | 0.55 (0.34–0.75) |
| Serine | 0.03 (1.12) | 0.12 (0.83) | 0.46 (0.23–0.68) | –0.17 (0.90) | –0.07 (0.86) | 0.62 (0.41–0.82) |
| Valine | –0.44 (1.23) | 0.26 (0.62) | 0.70 (0.49–0.90) | –0.40 (1.05) | 0.43 (0.92) | 0.73 (0.52–0.90) |
| Arginine | –0.11 (1.02) | 0.15 (0.42) | 0.56 (0.34–0.78) | –0.15 (0.86) | 0.10 (0.88) | 0.67 (0.42–0.86) |
| Parameter | LOLA (n = 15) | noLOLA (n = 15) | p Value |
|---|---|---|---|
| Alanine aminotransferase (U/L) | 38.8 (22.8) | 39.5 (15.6) | 0.6 |
| Aspartate aminotransferase (U/L) | 67.7 (41.9) | 66.2 (35) | 0.9 |
| Alkaline phosphatase (U/L) | 137.7 (59.2) | 125.7 (68.8) | 0.3 |
| Gamma-glutamyltransferase (U/L) | 134.5 (92.8) | 121.9 (105.3) | 0.6 |
| Albumin (g/dL) | 3.2 (0.5) | 3.3 (0.5) | 0.4 |
| Bilirubin (mg/dL) | 2.3 (1.8) | 2.4 (1.9) | >0.99 |
| Prothrombin time international normalized ratio | 1.4 (0.2) | 1.3 (0.2) | 0.2 |
| Total protein (g/dL) | 6.8 (0.9) | 7 (0.9) | 0.3 |
| Fecal calprotectin (ng/mL) | 101.4 (103.9) | 80.3 (64.6) | 0.7 |
| Fecal zonulin (ng/mL) | 161.2 (219.9) | 205.2 (203.5) | 0.036 |
| Diamine oxidase (U/mL) | 24 (11.9) | 23.3 (15.3) | 0.6 |
| LPS binding protein (µg/mL) | 16.7 (7) | 20.4 (9.8) | 0.4 |
| C-reactive protein (mg/L) | 10.3 (13.6) | 8.1 (15.2) | 0.4 |
| soluble Cluster of Differentiation 14 (µg/mL) | 1.8 (0.4) | 2 (0.8) | 0.7 |
| Fibroblast growth factor (ng/mL) | 0.3 (0.6) | 0.3 (0.2) | 0.3 |
| Irisin (µg/mL) | 2 (1.5) | 1.9 (1) | 0.8 |
| Myostatin (ng/mL) | 44 (34.1) | 38.6 (15.2) | 0.8 |
| Insulin-like growth factor 1 (ng/mL) | 48.3 (28.1) | 75.5 (38.4) | 0.029 |
| Chair rise test (s) | 25 (15.9) | 16.7 (3.8) | 0.1 |
| Gait speed (m/s) | 0.8 (0.3) | 1.1 (0.3) | 0.049 |
| Midarm muscle circumference (mm) | 256.6 (63.7) | 260.4 (48.1) | 0.7 |
| Hand grip strength (kg) | 30.6 (10.6) | 28.8 (5.8) | 0.5 |
| Body mass index (kg/m2) | 27.5 (6) | 28.5 (5.8) | 0.6 |
| Resting burst of neutrophils (% of neutrophils) | 2.4 (0.9) | 2.6 (1.9) | 0.7 |
| Resting burst of neutrophils (GMFI) | 174 (102.9) | 239.8 (223.3) | 0.4 |
| Neutrophil priming (% of neutrophils) | 3.2 (1.4) | 2.7 (1.2) | 0.5 |
| Neutrophil priming (GMFI) | 148.7 (58.7) | 194.8 (99.1) | 0.1 |
| ROS production after E. coli stimulation (% of neutrophils) | 96.7 (5.2) | 96.8 (4.5) | 0.6 |
| ROS production after E. coli stimulation (GMFI) | 1034.2 (547.1) | 753.7 (340.1) | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horvath, A.; Traub, J.; Aliwa, B.; Bourgeois, B.; Madl, T.; Stadlbauer, V. Oral Intake of L-Ornithine-L-Aspartate Is Associated with Distinct Microbiome and Metabolome Changes in Cirrhosis. Nutrients 2022, 14, 748. https://doi.org/10.3390/nu14040748
Horvath A, Traub J, Aliwa B, Bourgeois B, Madl T, Stadlbauer V. Oral Intake of L-Ornithine-L-Aspartate Is Associated with Distinct Microbiome and Metabolome Changes in Cirrhosis. Nutrients. 2022; 14(4):748. https://doi.org/10.3390/nu14040748
Chicago/Turabian StyleHorvath, Angela, Julia Traub, Benard Aliwa, Benjamin Bourgeois, Tobias Madl, and Vanessa Stadlbauer. 2022. "Oral Intake of L-Ornithine-L-Aspartate Is Associated with Distinct Microbiome and Metabolome Changes in Cirrhosis" Nutrients 14, no. 4: 748. https://doi.org/10.3390/nu14040748
APA StyleHorvath, A., Traub, J., Aliwa, B., Bourgeois, B., Madl, T., & Stadlbauer, V. (2022). Oral Intake of L-Ornithine-L-Aspartate Is Associated with Distinct Microbiome and Metabolome Changes in Cirrhosis. Nutrients, 14(4), 748. https://doi.org/10.3390/nu14040748