
Perceived Associations between Excessive Sugar Intake and Health Conditions

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Procedure and Instruments
2.3. Data Analytic Plan
3. Results
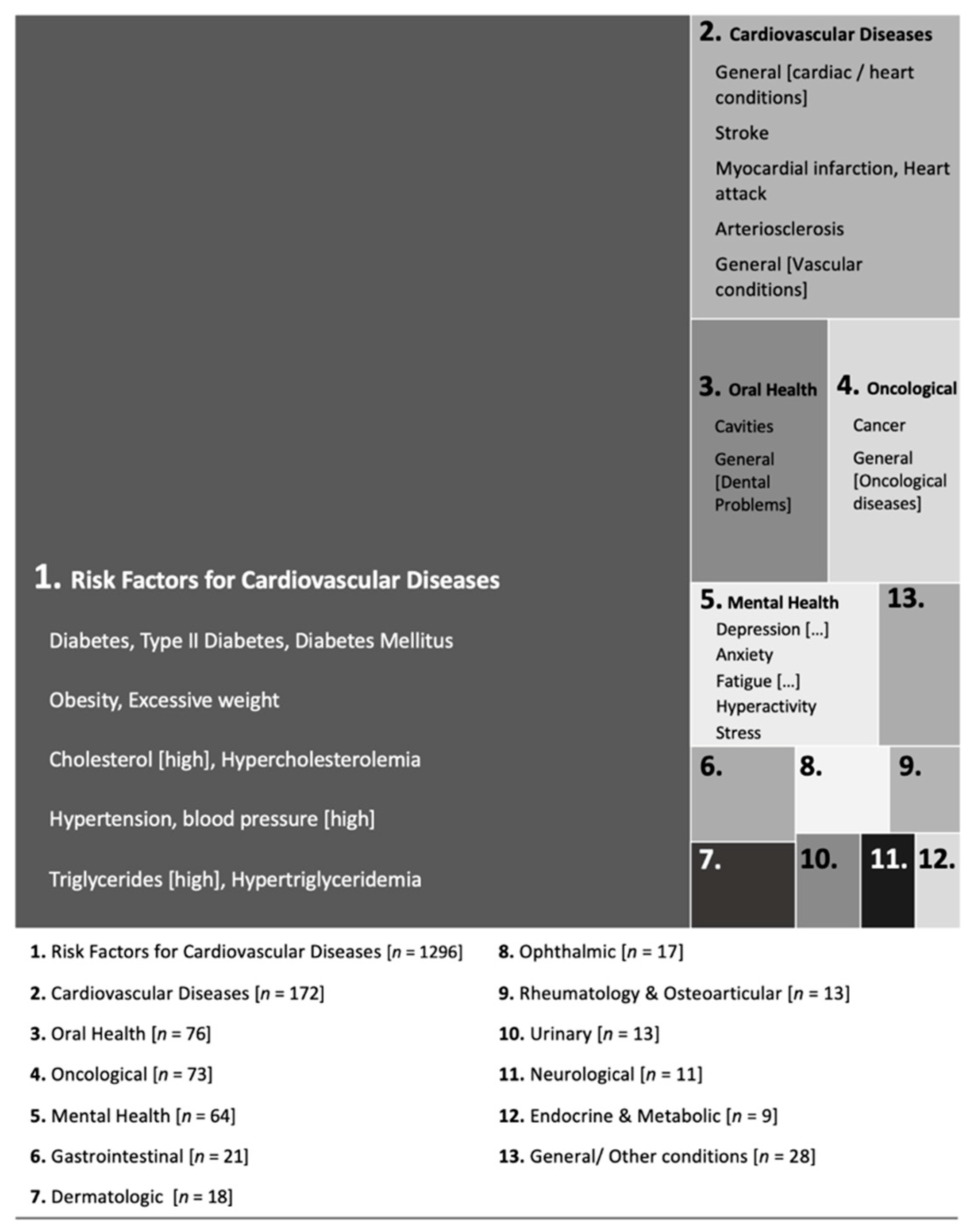
3.1. Excessive Sugar Intake and Health Conditions: Spontaneous Associations
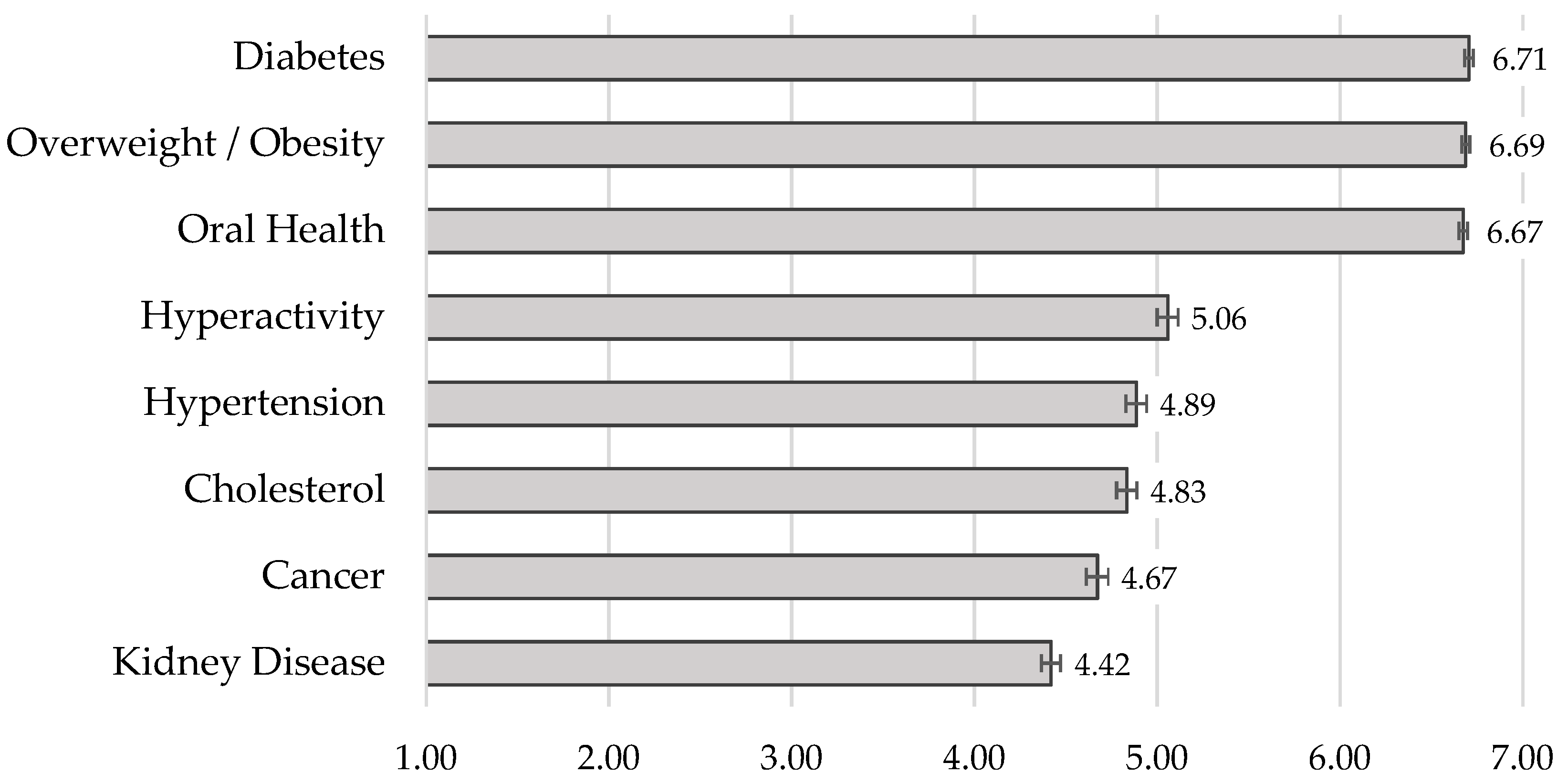
3.2. Excessive Sugar Intake and Health Conditions: Ratings of Strength of Association
3.3. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Greenberg, J.A. Obesity and early mortality in the United States. Obesity 2013, 21, 405–412. [Google Scholar] [CrossRef] [PubMed]
- WHO. Guideline: Sugars Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-069422-4. [Google Scholar]
- Mela, D.J.; Woolner, E.M. Perspective: Total, added, or free? What kind of sugars should we be talking about? Adv. Nutr. 2018, 9, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Hu, F.B. Sugar sweetened beverages, obesity, type 2 diabetes and cardiovascular disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef] [PubMed]
- Te Morenga, L.A.; Howatson, A.J.; Jones, R.M.; Mann, J. Dietary sugars and cardiometabolic risk: Systematic review and meta-analyses of randomized controlled trials of the effects on blood pressure and lipids. Am. J. Clin. Nutr. 2014, 100, 65–79. [Google Scholar] [CrossRef]
- Debras, C.; Chazelas, E.; Srour, B.; Kesse-Guyot, E.; Julia, C.; Zelek, L.; Agaësse, C.; Druesne-Pecollo, N.; Galan, P.; Hercberg, S.; et al. Total and added sugar intakes, sugar types, and cancer risk: Results from the prospective nutrinet-santé cohort. Am. J. Clin. Nutr. 2020, 112, 1267–1279. [Google Scholar] [CrossRef]
- Larsson, S.C.; Bergkvist, L.; Wolk, A. Consumption of sugar and sugar-sweetened foods and the risk of pancreatic cancer in a prospective study. Am. J. Clin. Nutr. 2006, 84, 1171–1176. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W.P.T. A reappraisal of the quantitative relationship between sugar intake and dental caries: The need for new criteria for developing goals for sugar intake. BMC Public Health 2014, 14, 863. [Google Scholar] [CrossRef]
- Rippe, J.M.; Angelopoulos, T.J. Relationship between added sugars consumption and chronic disease risk factors: Current understanding. Nutrients 2016, 8, 697. [Google Scholar] [CrossRef]
- Te Morenga, L.A.; Mallard, S.; Mann, J. Dietary sugars and body weight: Systematic review and meta-analyses of randomised controlled trials and cohort studies. BMJ 2012, 346, e7492. [Google Scholar] [CrossRef]
- Umer, A.; Kelley, G.A.; Cottrell, L.E.; Giacobbi, P.; Innes, K.E.; Lilly, C.L. Childhood obesity and adult cardiovascular disease risk factors: A systematic review with meta-analysis. BMC Public Health 2017, 17, 683. [Google Scholar] [CrossRef] [PubMed]
- Gaio, V.; Antunes, L.; Barreto, M.; Gil, A.; Kyslaya, I.; Namorado, S.; Rodrigues, A.P.; Santos, A.; Nunes, B.; Dias, C.M. Prevalência de excesso de peso e de obesidade em Portugal: Resultados do primeiro Inquérito Nacional de Saúde com Exame Físico (INSEF 2015) [Prevalence of overweight and obesity in Portugal: Results of the first National Health Survey with Physical Examination (INSEF 2015)]. Bol. Epidemiol. Obs. 2018, 7, 29–33. [Google Scholar]
- Deshpande, G.; Mapanga, R.F.; Essop, M.F. Frequent sugar-sweetened beverage consumption and the onset of cardiometabolic diseases: Cause for concern? J. Endocr. Soc. 2017, 1, 1372–1385. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Farhangi, M.A.; Nikniaz, L.; Khodarahmi, M. Sugar-sweetened beverages increases the risk of hypertension among children and adolescence: A Systematic review and dose–response meta-analysis. J. Transl. Med. 2020, 18, 344. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The Global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.P.; Gaio, V.; Kislaya, I.; Graff-Iversen, S.; Cordeiro, E.; Silva, A.C.; Namorado, S.; Barreto, M.; Gil, A.P.; Antunes, L.; et al. Prevalência de hipertensão arterial em Portugal: Resultados do Primeiro Inquérito Nacional com Exame Físico (INSEF 2015) [Prevalence of arterial hypertension in Portugal: Results of the First National Survey with Physical Examination (INSEF 2015)]. Obs. Epidemiol. 2017, 4, 271–278. [Google Scholar]
- Barreto, M.; Kislaya, I.; Gaio, V.; Rodrigues, A.P.; Santos, A.J.; Namorado, S.; Antunes, L.; Gil, A.P.; Boavida, J.M.; Silva, A.C.; et al. Prevalence, awareness and control of diabetes in Portugal: Results from the first National Health Examination Survey. Obs. Epidemiol. 2017, 5, 34–38. [Google Scholar]
- Valenzuela, M.J.; Waterhouse, B.; Aggarwal, V.R.; Bloor, K.; Doran, T. Effect of sugar-sweetened beverages on oral health: A systematic review and meta-analysis. Eur. J. Public Health 2021, 31, 122–129. [Google Scholar] [CrossRef]
- Breda, J.; Jewell, J.; Keller, A. The importance of the World Health Organization sugar guidelines for dental health and obesity prevention. Caries Res. 2019, 53, 149–152. [Google Scholar] [CrossRef]
- Céu, A.; Ferreira, C.S.; Jordão, M. Programa Nacional de Promoção da Saúde Oral [National Program for the Promotion of Oral Health]; Direção-Geral da Saúde: Lisbon, Portugal, 2019.
- Prada, M.; Rodrigues, D.L.; Godinho, C.; Lopes, D.; Garrido, M.V. Knowledge and acceptance of interventions aimed at reducing sugar intake in Portugal. Public Health Nutr. 2020, 23, 3423–3434. [Google Scholar] [CrossRef]
- Lopes, C.; Torres, C.; Oliveira, A.; Sereno, M.; Alarcão, V.; Guiomar, S.; Mota, J.; Teixeira, P.; Rodrigues, S.; Lobato, L.; et al. Inquérito Alimentar Nacional e de Atividade Física de 2015-2016 [National Food and Physical Activity Survey 2015–2016]; Universidade do Porto: Porto, Portugal, 2017. [Google Scholar]
- Prada, M.; Godinho, C.A.; Garrido, M.V.; Rodrigues, D.L.; Coelho, I.; Lopes, D. A qualitative study about college students’ attitudes, knowledge and perceptions regarding sugar intake. Appetite 2021, 159, 105059. [Google Scholar] [CrossRef] [PubMed]
- Prada, M.; Saraiva, M.; Godinho, C.A.; Tourais, B.; Cavalheiro, B.; Garrido, M.V. Parental perceptions and practices regarding sugar intake by school-aged children: A qualitative study with Portuguese parents. Appetite 2021, 105471. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.; Braunack-Mayer, A.; Wakefield, M.; Roder, D.; O’Dea, K.; Dono, J.; Ettridge, K. “When we were young, it really was a treat; now sugar is just the norm every day”—A qualitative study of parents’ and young adults’ perceptions and consumption of sugary drinks. Health Promot. J. Austr. 2020, 31, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Del-Ponte, B.; Anselmi, L.; Assunção, M.C.F.; Tovo-Rodrigues, L.; Munhoz, T.N.; Matijasevich, A.; Rohde, L.A.; Santos, I.S. Sugar consumption and attention-deficit/hyperactivity disorder (ADHD): A birth cohort study. J. Affect. Disord. 2019, 243, 290–296. [Google Scholar] [CrossRef]
- Miller, C.; Ettridge, K.; Wakefield, M.; Pettigrew, S.; Coveney, J.; Roder, D.; Durkin, S.; Wittert, G.; Martin, J.; Dono, J. An in-depth exploration of knowledge and beliefs associated with soda and diet soda consumption. Nutrients 2020, 12, 2841. [Google Scholar] [CrossRef]
- Park, S.; Lundeen, E.A.; Pan, L.; Blanck, H.M. Impact of knowledge of health conditions on sugar-sweetened beverage intake varies among US adults. Am. J. Health Promot. 2018, 32, 1402–1408. [Google Scholar] [CrossRef]
- Park, S.; Ayala, G.X.; Sharkey, J.R.; Blanck, H.M. Knowledge of health conditions associated with sugar-sweetened beverage intake is low among US Hispanic adults. Am. J. Health Promot. 2019, 33, 39–47. [Google Scholar] [CrossRef]
- Brownbill, A.L.; Braunack-Mayer, A.J.; Miller, C.L. What makes a beverage healthy? A qualitative study of young adults’ conceptualisation of sugar-containing beverage healthfulness. Appetite 2020, 150, 104675. [Google Scholar] [CrossRef]
- Munsell, C.R.; Harris, J.L.; Sarda, V.; Schwartz, M.B. Parents’ beliefs about the healthfulness of sugary drink options: Opportunities to address misperceptions. Public Health Nutr. 2016, 19, 46–54. [Google Scholar] [CrossRef]
- Prada, M.; Saraiva, M.; Garrido, M.V.; Rodrigues, D.L.; Lopes, D. Knowledge about sugar sources and sugar intake guidelines in Portuguese consumers. Nutrients 2020, 12, 3888. [Google Scholar] [CrossRef]
- Tierney, M.; Gallagher, A.M.; Giotis, E.S.; Pentieva, K. An online survey on consumer knowledge and understanding of added sugars. Nutrients 2017, 9, 37. [Google Scholar] [CrossRef]
- Grimes, C.A.; Riddell, L.J.; Nowson, C.A. Consumer knowledge and attitudes to salt intake and labelled salt information. Appetite 2009, 53, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Kasper, D.L.; Fauci, A.S.; Hauser, S.L.; Longo, D.L.; Jameson, J.L.; Loscalzo, J. Harrison’s Principles of Internal Medicine, 19th ed.; McGraw-Hill Education: New York, NY, USA, 2015. [Google Scholar]
- WHO. International Statistical Classification of Diseases and Related Health Problems; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Miller, A.N.; Bharathan, A.; Duvuuri, V.N.S.; Navas, V.; Luceno, L.; Zraick, R.; Atmakuri, S.; Schmidt-Owens, M.; Deichen, M.; Ayers, T.; et al. Use of seven types of medical jargon by male and female primary care providers at a university health center. Patient Educ. Couns. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, G.; Protheroe, J.; Price, H.; Gann, B.; Rafi, I. Health Literacy: Report from an RCGP-Led Health Literacy Workshop; Royal College of General Practitioners: London, UK, 2014. [Google Scholar]
- DiNicolantonio, J.J.; Bhutani, J.; O’Keefe, J.H. Added sugars drive chronic kidney disease and its consequences: A comprehensive review. J. Insul. Resist. 2016, 1, 6. [Google Scholar] [CrossRef]
- Behrens, D.; Lear, J.G. Strengthening children’s oral health: Views from the field. Health Aff. 2011, 30, 2208–2213. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- WHO. Diet and Oral Health; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Krummel, D.A.; Seligson, F.H.; Guthrie, H.A.; Gans, D.D.A. Hyperactivity: Is candy causal? Crit. Rev. Food Sci. Nutr. 1996, 36, 31–47. [Google Scholar] [CrossRef]
- Andreeva, V.A.; Salanave, B.; Castetbon, K.; Deschamps, V.; Vernay, M.; Kesse-Guyot, E.; Hercberg, S. Comparison of the sociodemographic characteristics of the large nutrinet-santé e-cohort with French census data: The issue of volunteer bias revisited. J. Epidemiol. Community Health 2015, 69, 893–898. [Google Scholar] [CrossRef]
- Ball, L.; Leveritt, M.; Cass, S.; Chaboyer, W. Effect of nutrition care provided by primary health professionals on adults’ dietary behaviours: A systematic review. Fam. Pract. 2015, 32, 605–617. [Google Scholar] [CrossRef]
- VanFrank, B.K.; Park, S.; Foltz, J.L.; McGuire, L.C.; Harris, D.M. Physician characteristics associated with sugar-sweetened beverage counseling practices. Am. J. Health Promot. 2018, 32, 1365–1374. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.D. Unrealistic optimism about future life events. J. Pers. Soc. Psychol. 1980, 39, 806–820. [Google Scholar] [CrossRef]
- Dono, J.; Ettridge, K.A.; Wakefield, M.; Pettigrew, S.; Coveney, J.; Roder, D.; Durkin, S.; Wittert, G.; Martin, J.; Miller, C.L. Intentions to reduce sugar-sweetened beverage consumption: The importance of perceived susceptibility to health risks. Public Health Nutr. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Measure | Item | Scale Anchors |
|---|---|---|
| Attention to sugar content information [34] | “How often do you look at the sugar content in the nutritional table?” | 1 = Never to 7 = Always |
| Frequency of high sugary foods intake | “How often do you consume drinks and foods with a high sugar content?” | 1 = Never or less than once a month to 7 = More than once a day |
| Concern about sugar intake (adapted from [35]) | “I am not concerned with the amount of sugar present in my diet”. | 1 = Strongly Disagree to 7 = Strongly Agree * |
| Health benefits from reducing sugar intake (adapted from [35]) | “My health would improve if I reduced the amount of sugar in my diet”. | 1 = Strongly Disagree to 7 = Strongly Agree |
| Intention to reduce sugar intake | “I plan to reduce the amount of sugar in my diet”. | 1 = Strongly Disagree to 7 = Strongly Agree |
| Importance of reducing sugar intake in Portugal [33] | “In your opinion, reducing sugar consumption in the Portuguese population is …” | 1 = Not very important to 7 = Very important |
| Health Condition | n | %P | Health Condition | n | %P |
|---|---|---|---|---|---|
| 1. Risk Factors for Cardiovascular Diseases | 1296 | 7. Dermatologic Conditions | 19 | ||
| Diabetes, type II diabetes, diabetes mellitus | 727 | 72.0 | Skin, dermatological (issues), acne, pimples | 16 | 1.6 |
| Obesity, overweight | 419 | 41.5 | Hidradenitis suppurativa | 2 | 0.2 |
| Cholesterol (high), hypercholesterolemia | 67 | 6.6 | Skin inflammation | 1 | 0.1 |
| Hypertension, blood pressure (high) | 59 | 5.8 | |||
| Triglycerides (high), hypertriglyceridemia | 10 | 1.0 | 8. Ophthalmic Diseases | 17 | |
| Dyslipidemia | 9 | 0.9 | Blindness | 4 | 0.4 |
| Blood glucose | 5 | 0.5 | Glaucoma | 4 | 0.4 |
| Retinopathy, diabetic retinopathy | 4 | 0.4 | |||
| 2. Cardiovascular Diseases | 172 | Myopia | 3 | 0.3 | |
| General (cardiovascular, cardiac, heart conditions) | 116 | 11.5 | General (eye problems) | 2 | 0.2 |
| Stroke | 24 | 2.4 | |||
| Myocardial infarction, Heart attack | 11 | 1.1 | 9. Rheumatology and Osteoarticular Pathology | 13 | |
| Arteriosclerosis | 6 | 0.6 | Gout, uric acid (high) | 2 | 0.2 |
| General (vascular conditions) | 5 | 0.5 | Osteoarticular, bones or joints (problems) | 8 | 0.8 |
| Circulatory problems | 4 | 0.4 | Osteoporosis | 2 | 0.2 |
| Thrombosis | 3 | 0.3 | Rheumatoid arthritis | 1 | 0.1 |
| Blood coagulation | 1 | 0.1 | |||
| Micro and macro vasculopathy | 1 | 0.1 | 10. Urinary System Diseases | 13 | |
| Ischemic fingers | 1 | 0.1 | Kidney or renal (issues, diseases), nephropathy | 12 | 1.2 |
| Cystitis | 1 | 0.1 | |||
| 3. Oral Health Problems | 76 | ||||
| Cavities | 63 | 6.2 | 11. Neurological Diseases | 11 | |
| General (dental problems) | 13 | 1.3 | Neurodegenerative diseases | 3 | 0.3 |
| Headaches, migraines | 3 | 0.3 | |||
| 4. Oncological Diseases | 73 | Polyneuropathy | 3 | 0.3 | |
| Cancer | 65 | 6.4 | Alzheimer’s disease | 1 | 0.1 |
| General (oncological diseases) | 6 | 0.6 | Epileptic seizures | 1 | 0.1 |
| Leukemia | 1 | 0.1 | |||
| Tumors (malignant) | 1 | 0.1 | 12. General/Other Conditions | 37 | |
| Endocrine and metabolic disorders | 9 | 0.9 | |||
| 5. Mental Health Conditions | 64 | Inflammatory processes | 9 | 0.9 | |
| Depression, mood disorders | 13 | 1.3 | Immune system (weakened) | 3 | 0.3 |
| Anxiety | 10 | 1.0 | Fungal infections, candidiasis | 3 | 0.3 |
| Fatigue, burnout, tiredness | 9 | 0.9 | Autoimmune diseases | 3 | 0.3 |
| Hyperactivity | 8 | 0.8 | Respiratory system diseases | 3 | 0.3 |
| Stress | 7 | 0.7 | General malaise | 1 | 0.1 |
| Attention (deficit) | 5 | 0.5 | Aging (faster) | 1 | 0.1 |
| Addiction | 4 | 0.4 | Aesthetic (consequences) | 1 | 0.1 |
| Sleep disorders, Insomnia | 2 | 0.2 | Morbidity | 1 | 0.1 |
| General (mental health/psychological conditions) | 2 | 0.2 | Fluid retention | 1 | 0.1 |
| Memory (diminished) | 2 | 0.2 | Ulcers | 1 | 0.1 |
| Self-esteem (low) | 1 | 0.1 | Chronic diseases | 1 | 0.1 |
| Irritability | 1 | 0.1 | |||
| 6. Gastrointestinal System Diseases | 21 | ||||
| Intestine or stomach diseases | 9 | 0.9 | |||
| Liver diseases | 11 | 1.1 | |||
| Pancreas diseases | 1 | 0.1 |
| Gender | Children in the Household | Expertise in Health or Nutrition 1 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Men (n = 231) | Women (n = 775) | p | No (n = 672) | Yes (n = 338) | p | Non-Experts (n = 690) | Experts (n = 105) | p | |
| M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | M (SD) | ||||
| Diabetes | 6.70 (0.66) | 6.71 (0.78) | 0.876 | 6.70 (0.75) | 6.71 (0.76) | 0.810 | 6.69 (0.75) | 6.81 (0.46) | 0.024 |
| Overweight/Obesity | 6.57 (0.75) | 6.72 (0.68) | 0.007 | 6.68 (0.71) | 6.70 (0.67) | 0.719 | 6.68 (0.66) | 6.81 (0.46) | 0.015 |
| Oral Health | 6.57 (0.78) | 6.71 (0.72) | 0.016 | 6.66 (0.73) | 6.71 (0.73) | 0.270 | 6.70 (0.65) | 6.70 (0.77) | 0.896 |
| Hyperactivity | 4.72 (1.94) | 5.16 (1.82) | 0.001 | 4.93 (1.90) | 5.31 (1.74) | 0.002 | 5.10 (1.82) | 5.10 (1.76) | 0.962 |
| Hypertension | 4.85 (1.77) | 4.89 (1.81) | 0.774 | 4.91 (1.82) | 4.84 (1.76) | 0.541 | 4.92 (1.75) | 4.90 (1.74) | 0.873 |
| Cholesterol | 4.72 (1.84) | 4.87 (1.76) | 0.284 | 4.83 (1.80) | 4.83 (1.73) | 0.993 | 4.84 (1.74) | 4.89 (1.70) | 0.798 |
| Cancer | 4.02 (1.84) | 4.87 (1.91) | <0.001 | 4.54 (1.95) | 4.94 (1.90) | 0.002 | 4.59 (1.91) | 5.61 (1.42) | <0.001 |
| Kidney Disease | 4.35 (1.72) | 4.44 (1.68) | 0.465 | 4.38 (1.67) | 4.51 (1.73) | 0.244 | 4.41 (1.62) | 4.96 (1.71) | 0.001 |
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Overall association with health conditions a | 5.49 | 0.85 | - | ||||||||
| 2. Intention to reduce sugar intake | 5.07 | 1.91 | 0.18 *** | - | |||||||
| 3. Attention to sugar information | 5.11 | 1.86 | 0.21 *** | 0.18 *** | - | ||||||
| 4. Frequency of sugar intake | 3.23 | 1.55 | −0.09 ** | −0.01 | −0.25 *** | - | |||||
| 5. Concern about sugar intake | 5.31 | 2.04 | 0.07 * | 0.25 *** | 0.22 *** | −0.10 ** | - | ||||
| 6. Health benefits from reducing sugar intake | 5.23 | 1.98 | 0.16 *** | 0.60 *** | 0.11 ** | 0.09 ** | 0.15 *** | - | |||
| 7. Importance of reducing sugar intake in Portugal | 6.73 | 0.69 | 0.20 *** | 0.23 *** | 0.19 ** | −0.16 *** | 0.21 *** | 0.14 ** | - | ||
| 8. Overall activity | 4.27 | 1.54 | 0.03 | −0.05 | 0.10 ** | −0.12 *** | 0.00 | −0.13 ** | 0.04 | - | |
| 9. Overall health status | 5.25 | 1.04 | 0.06 * | −0.04 | 0.17 *** | −0.19 *** | 0.02 | −0.16 ** | 0.09 * | 0.40 *** | - |
| 10. Age | 36.33 | 13.22 | −0.02 | −0.05 | 0.02 | −0.17 *** | −0.04 | −0.04 | 0.78 * | 0.00 | −0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prada, M.; Saraiva, M.; Garrido, M.V.; Sério, A.; Teixeira, A.; Lopes, D.; Silva, D.A.; Rodrigues, D.L. Perceived Associations between Excessive Sugar Intake and Health Conditions. Nutrients 2022, 14, 640. https://doi.org/10.3390/nu14030640
Prada M, Saraiva M, Garrido MV, Sério A, Teixeira A, Lopes D, Silva DA, Rodrigues DL. Perceived Associations between Excessive Sugar Intake and Health Conditions. Nutrients. 2022; 14(3):640. https://doi.org/10.3390/nu14030640
Chicago/Turabian StylePrada, Marília, Magda Saraiva, Margarida V. Garrido, Ana Sério, Ana Teixeira, Diniz Lopes, Diana A. Silva, and David L. Rodrigues. 2022. "Perceived Associations between Excessive Sugar Intake and Health Conditions" Nutrients 14, no. 3: 640. https://doi.org/10.3390/nu14030640
APA StylePrada, M., Saraiva, M., Garrido, M. V., Sério, A., Teixeira, A., Lopes, D., Silva, D. A., & Rodrigues, D. L. (2022). Perceived Associations between Excessive Sugar Intake and Health Conditions. Nutrients, 14(3), 640. https://doi.org/10.3390/nu14030640