
The Impact of a Mediterranean-like Diet with Controlled Protein Intake on the Onco-Nephrological Scenario: Time for a New Perspective
 , ,
, ,  , ,
, ,
Abstract
1. Introduction
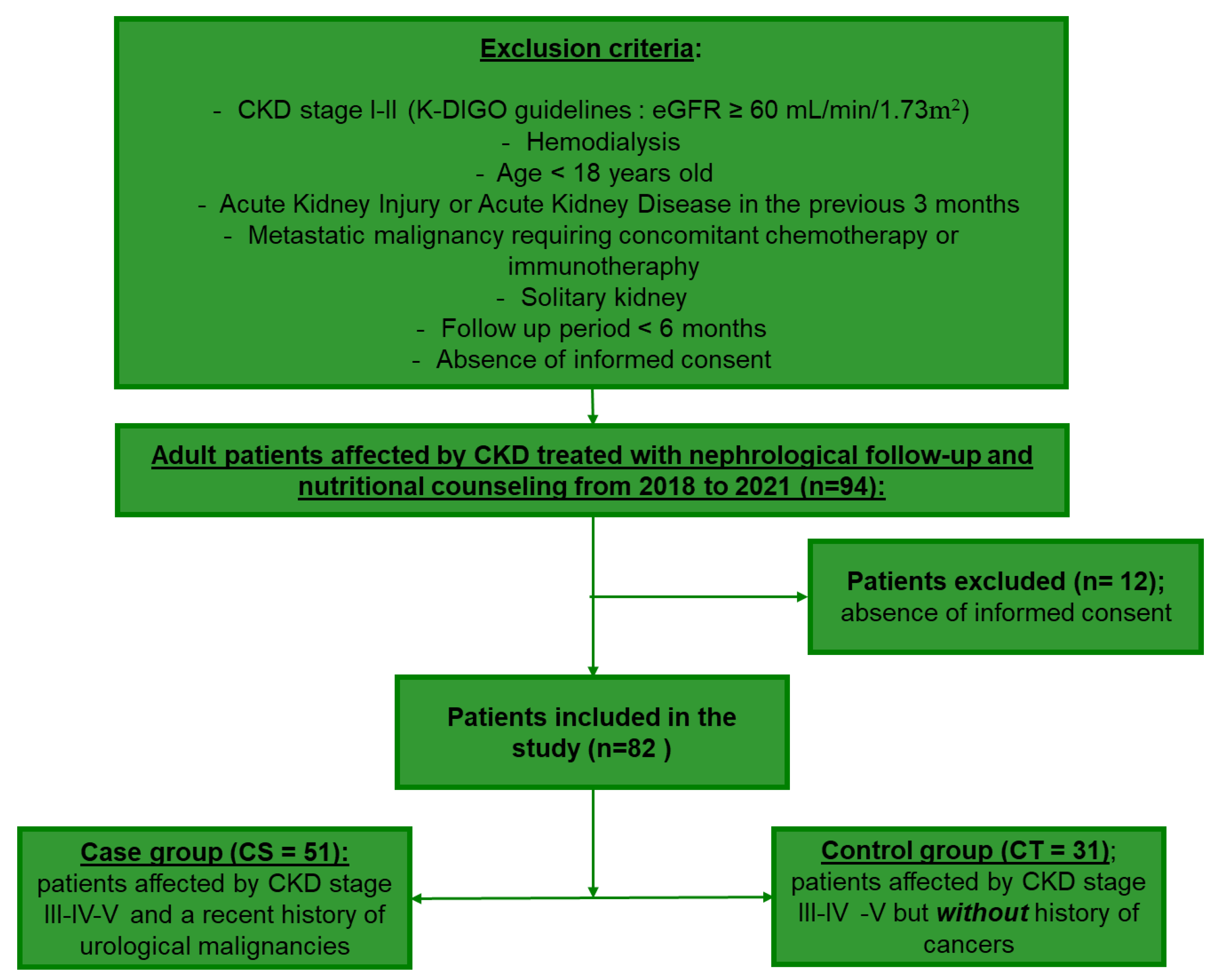
2. Materials and Methods
2.1. Assessment of Nutritional Status and Quality of Life
2.2. Statistical Analysis
3. Results
3.1. Clinical and Demographic Findings of the Patients
3.2. Overall Improvement in the Anthropometric Indices and Parameters following the Nephrologist Nutritionist Combined Approach (NNCA) in Both CS and CT Groups
3.3. NNCA Caused a Decrease in Malnourished Individuals over the Course of the Follow-Up Period in CS Patients but Not in the CT Group
3.4. Circulating Levels of Urea and Vitamin D Are Positively Altered by NNCA in Both CS and CT Patients
3.5. The Stratification of the Outcomes Outlines That the Response of the CS and CT Groups Is Analogous
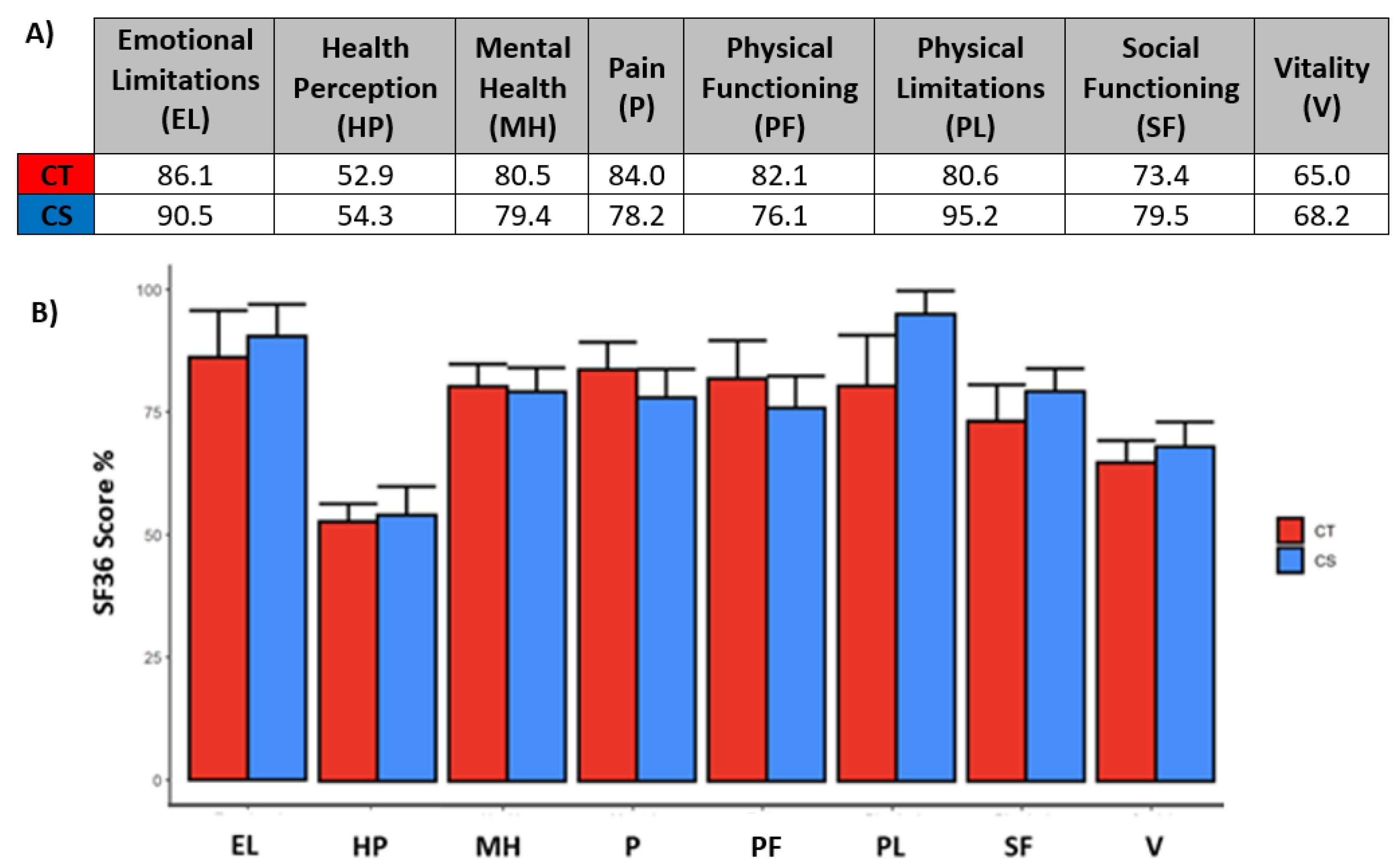
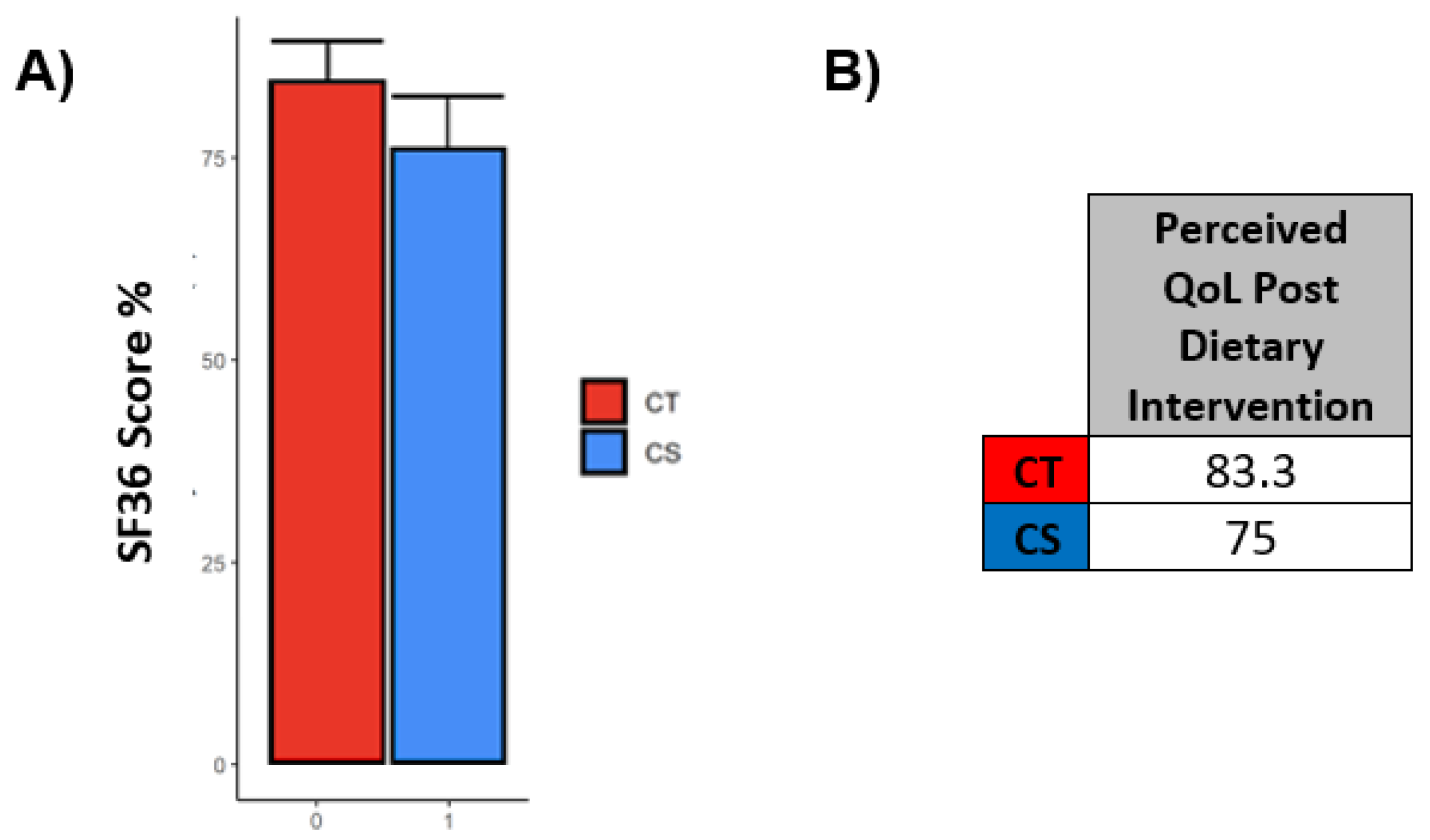
3.6. SF36 Questionnaires Outlined a Good Perceived Quality of Life in the Entire Cohort following NNCA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Dhimal, M. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [PubMed]
- Argiles, J.M. Cancer-Associated malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S39–S50. [Google Scholar] [CrossRef] [PubMed]
- Stengel, B. Chronic kidney disease and cancer: A troubling connection. J. Nephrol. 2010, 23, 253–262. [Google Scholar]
- Malyszko, J.; Tesarova, P.; Capasso, G.; Capasso, A. The link between kidney disease and cancer: Complications and treatment. Lancet 2020, 396, 277–287. [Google Scholar] [CrossRef]
- Rysz, J.; Franczyk, B.; Ciałkowska-Rysz, A.; Gluba-Brzózka, A. The Effect of Diet on the Survival of Patients with Chronic Kidney Disease. Nutrients 2017, 9, 495. [Google Scholar] [CrossRef]
- Hanna, R.M.; Ghobry, L.; Wassef, O.; Rhee, C.M.; Kalantar-Zadeh, K. A Practical Approach to Nutrition, Protein-Energy Wasting, Sarcopenia, and Cachexia in Patients with Chronic Kidney Disease. Blood Purif. 2020, 49, 202–211. [Google Scholar] [CrossRef]
- Hsu, H.J.; Yen, C.H.; Wu, I.W.; Liu, M.H.; Cheng, H.Y.; Lin, Y.T.; Lee, C.-C.; Hsu, K.-H.; Sun, C.-Y.; Chen, C.-Y.; et al. The association between low protein diet and body composition, muscle function, inflammation, and amino acid-based metabolic profile in chronic kidney disease stage 3–5 patients. Clin. Nutr. ESPEN 2021, 46, 405–415. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Kalantar-Zadeh, K. Back to the future: Restricted protein intake for conservative management of CKD, triple goals of renoprotection, uremia mitigation, and nutritional health. Int. Urol. Nephrol. 2016, 48, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Ash, S.; Campbell, K.L.; Bogard, J.; Millichamp, A. Nutrition Prescription to Achieve Positive Outcomes in Chronic Kidney Disease: A Systematic Review. Nutrients 2014, 6, 416–451. [Google Scholar] [CrossRef] [PubMed]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 10, CD001892. [Google Scholar] [CrossRef]
- Mitch, W.E.; Remuzzi, G. Diets for patients with chronic kidney disease, should we reconsider? BMC Nephrol. 2016, 17, 80. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Qader, H.; Kovesdy, C.P.; Kalantar-Zadeh, K. Latest consensus and update on protein-energy wasting in chronic kidney disease. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Moorthi, R.N.; Armstrong, C.L.; Janda, K.; Ponsler-Sipes, K.; Asplin, J.R.; Moe, S.M. The Effect of a Diet Containing 70% Protein from Plants on Mineral Metabolism and Musculoskeletal Health in Chronic Kidney Disease. Am. J. Nephrol. 2014, 40, 582–591. [Google Scholar] [CrossRef]
- Moe, S.M.; Zidehsarai, M.P.; Chambers, M.A.; Jackman, L.A.; Radcliffe, J.S.; Trevino, L.L.; Donahue, S.E.; Asplin, J.R. Vegetarian Compared with Meat Dietary Protein Source and Phosphorus Homeostasis in Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2011, 6, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Palmer, S.C.; Wai, S.N.; Ruospo, M.; Carrero, J.-J.; Campbell, K.; Strippoli, G.F.M. Healthy Dietary Patterns and Risk of Mortality and ESRD in CKD: A Meta-Analysis of Cohort Studies. Clin. J. Am. Soc. Nephrol. 2016, 12, 272–279. [Google Scholar] [CrossRef]
- Haring, B.; Selvin, E.; Liang, M.; Coresh, J.; Grams, M.E.; Petruski-Ivleva, N.; Steffen, L.M.; Rebholz, C.M. Dietary Protein Sources and Risk for Incident Chronic Kidney Disease: Results From the Atherosclerosis Risk in Communities (ARIC) Study. J. Ren. Nutr. 2017, 27, 233–242. [Google Scholar] [CrossRef]
- Lew, Q.-L.J.; Jafar, T.H.; Koh, H.W.L.; Jin, A.; Chow, K.Y.; Yuan, J.-M.; Koh, W.-P. Red Meat Intake and Risk of ESRD. J. Am. Soc. Nephrol. 2016, 28, 304–312. [Google Scholar] [CrossRef]
- Chen, X.; Wei, G.; Jalili, T.; Metos, J.; Giri, A.; Cho, M.E.; Boucher, R.; Greene, T.; Beddhu, S. The Associations of Plant Protein Intake With All-Cause Mortality in CKD. Am. J. Kidney Dis. 2016, 67, 423–430. [Google Scholar] [CrossRef]
- Metzger, M.; Yuan, W.L.; Haymann, J.-P.; Flamant, M.; Houillier, P.; Thervet, E.; Boffa, J.-J.; Vrtovsnik, F.; Froissart, M.; Bankir, L.; et al. Association of a Low-Protein Diet With Slower Progression of CKD. Kidney Int. Rep. 2017, 3, 105–114. [Google Scholar] [CrossRef]
- Fouque, D.; Laville, M. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2006, 10, CD001892. [Google Scholar] [CrossRef]
- Caria, S.; Cupisti, A.; Sau, G.; Bolasco, P. The incremental treatment of ESRD: A low-protein diet combined with weekly hemodialysis may be beneficial for selected patients. BMC Nephrol. 2014, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Di Iorio, B.; De Nicola, L.; Minutolo, R.; Zamboli, P.; Trucillo, P.; Catapano, F.; Cristofano, C.; Scalfi, L.; Conte, G.; et al. Very low protein diet supplemented with ketoanalogs improves blood pressure control in chronic kidney disease. Kidney Int. 2007, 71, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef] [PubMed]
- Fofi, C.; Festuccia, F. Onconephrology: A New Challenge for the Nephrologist. Nephrol. Public Health Worldw. 2021, 199, 91–105. [Google Scholar] [CrossRef]
- Kala, J.; Finkel, K.W. Onconephrology. Crit. Care Clin. 2021, 37, 365–384. [Google Scholar] [CrossRef]
- MacDonald, A.J.; Johns, N.; Stephens, N.; Greig, C.; Ross, J.A.; Small, A.C.; Husi, H.; Fearon, K.C.H.; Preston, T. Habitual myofibrillar protein synthesis is normalin patients with upper GI cancer cachexia. Clin. Cancer Res. 2015, 21, 1734–1740. [Google Scholar] [CrossRef]
- Winter, A.; MacAdams, J.; Chevalier, S. Normal protein anabolic response to hyperaminoacidemia in insulin-resistant patients with lung cancer cachexia. Clin. Nutr. 2012, 31, 765–773. [Google Scholar] [CrossRef]
- Baracos, V.E. Skeletal muscle anabolism in patients with advanced cancer. Lancet Oncol. 2015, 16, 13–14. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Levin, A.S.; Bilous, R.W.; Coresh, J. Chapter 1: Definition and classification of CKD. Kidney Int. Suppl. 2013, 3, 19–62. [Google Scholar]
- Gaspari, F.; Thakar, S.; Carrara, F.; Perna, A.; Trillini, M.; Aparicio, M.C.; Diadei, O.; Ferrari, S.; Cannatá, A.; Stucchi, N.; et al. Safety of Iohexol Administration to Measure Glomerular Filtration Rate in Different Patient Populations: A 25-Year Experience. Nephron 2018, 140, 1–8. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.B. Peer Reviewed: The Rapid Assessment of Physical Activity (RAPA) Among Older Adults. Prev. Chronic Dis. 2006, 3, A118. [Google Scholar]
- Han, B.-G.; Lee, J.Y.; Kim, J.-S.; Yang, J.-W. Clinical Significance of Phase Angle in Non-Dialysis CKD Stage 5 and Peritoneal Dialysis Patients. Nutrients 2018, 10, 1331. [Google Scholar] [CrossRef]
- Ruperto, M.; Sánchez-Muniz, F.J.; Barril, G. Extracellular mass to body cell mass ratio as a potential index of wasting and fluid overload in hemodialysis patients. A case-control study. Clin. Nutr. 2020, 39, 1117–1123. [Google Scholar] [CrossRef]
- Bellizzi, V.; Conservative Treatment of CKD; Study Group of the Italian Society of Nephrology; Cupisti, A.; Locatelli, F.; Bolasco, P.; Brunori, G.; Cancarini, G.; Caria, S.; De Nicola, L.; et al. Low-Protein diets for chronic kidney disease patients: The Italian experience. BMC Nephrol. 2016, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, M.; Bellizzi, V.; Chauveau, P.; Cupisti, A.; Ecder, T.; Fouque, D.; Garneata, L.; Lin, S.; Mitch, W.; Teplan, V.; et al. Do Ketoanalogues Still Have a Role in Delaying Dialysis Initiation in CKD Predialysis Patients? Semin. Dial. 2013, 26, 714–719. [Google Scholar] [CrossRef]
- Rhee, C.M.; Ahmadi, S.-F.; Kovesdy, C.P.; Kalantar-Zadeh, K. Low-Protein diet for conservative management of chronic kidney disease: A systematic review and meta-analysis of controlled trials. J. Cachex- Sarcopenia Muscle 2017, 9, 235–245. [Google Scholar] [CrossRef]
- Kovesdy, C.P.; Anderson, J.E.; Kalantar-Zadeh, K. Association of serum bicarbonate levels with mortality in patients with non-dialysis-dependent CKD. Nephrol. Dial. Transplant. 2008, 24, 1232–1237. [Google Scholar] [CrossRef]
- Yan, B.; Su, X.; Xu, B.; Qiao, X.; Wang, L. Effect of diet protein restriction on progression of chronic kidney disease: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0206134. [Google Scholar] [CrossRef]
- Mitch, W.E.; Remuzzi, G. Diets for patients with chronic kidney disease, still worth prescribing. J. Am. Soc. Nephrol. 2004, 15, 234–237. [Google Scholar] [CrossRef]
- Fouque, D.; Aparicio, M. Eleven reasons to control the protein intake of patients with chronic kidney disease. Nat. Clin. Pract. Nephrol. 2007, 3, 383–392. [Google Scholar] [CrossRef]
- Cupisti, A.; D’Alessandro, C.; Morelli, E.; Rizza, G.M.; Galetta, F.; Franzoni, F.; Barsotti, G. Nutritional status and dietary manipulation in predialysis chronic renal failure patients. J. Ren. Nutr. 2004, 14, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Wang, P.; Laville, M.; Boissel, J.P. Low protein diets for chronic renal failure in non diabetic adults. Cochrane Database Syst. Rev. 2000, 15, 1986–1992. [Google Scholar] [CrossRef]
- Verzola, D.; Picciotto, D.; Saio, M.; Aimasso, F.; Bruzzone, F.; Sukkar, S.G.; Massarino, F.; Esposito, P.; Viazzi, F.; Garibotto, G. Low Protein Diets and Plant-Based Low Protein Diets: Do They Meet Protein Requirements of Patients with Chronic Kidney Disease? Nutrients 2020, 13, 83. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Marco, E.; Dávalos-Yerovi, V.; Muns, M.; Tejero-Sánchez, M.; Duarte, E.; Sánchez-Rodríguez, D. Sarcopenia, Malnutrition, and Cachexia: Adapting Definitions and Terminology of Nutritional Disorders in Older People with Cancer. Nutrients 2021, 13, 761. [Google Scholar] [CrossRef]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef]
- Talluri, T.; Lietdke, R.J.; Evangelisti, A.; Talluri, J.; Maggia, G. Fat-Free mass qualitative assessment with bioelectric impedance analysis (BIA). Ann. New York Acad. Sci. 1999, 873, 94–98. [Google Scholar] [CrossRef]
- Noce, A.; Vidiri, M.F.; Marrone, G.; Moriconi, E.; Bocedi, A.; Capria, A.; Rovella, V.; Ricci, G.; De Lorenzo, A.; Di Daniele, N. Is low-protein diet a possible risk factor of malnutrition in chronic kidney disease patients? Cell Death Discov. 2016, 2, 16026. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Marra, M.; Di Gregorio, A.; Pasanisi, F.; Scalfi, L. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: A systematic review. Clin. Nutr. 2020, 40, 3052–3061. [Google Scholar] [CrossRef]
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Yu, M.K.; Kamal, F.; Chertow, G.M. Updates in Management and Timing of Dialysis in Acute Kidney Injury. J. Hosp. Med. 2019, 14, 232–238. [Google Scholar]
- Sawhney, S.; Fraser, S.D. Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI. Adv. Chronic Kidney Dis. 2017, 24, 194–204. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N (% on Total) | p-Value | ||||
|---|---|---|---|---|---|
| Number of patients | 82 | Onco | 51 (62.2%) | / | |
| Nephro | 31 (37.8%) | ||||
| Age | 69.8 ± 10.3 | Onco | 71.6 (±8.8) | 0.9 1 | |
| Nephro | 66.5 (±12.1) | ||||
| Gender | ♂ 63 (76.8%) | Onco | 41 (65.1%) | 0.327 2 | |
| Nephro | 22 (34.9%) | ||||
| ♀ 19 (23.2%) | Onco | 10 (52.6%) | |||
| Nephro | 9 (47.4%) | ||||
| BMI | 25.9 | Onco | 26.1 (23.6–29.7) | 0.450 2 | |
| Nephro | 25.1 (23.1–29.9) | ||||
| BMI Classification | Underweight (<18.5) | 0 | Onco | 0 | 0.665 2 |
| Nephro | 0 | ||||
| Healthy weight (18.5–24.9) | 36 (43.9%) | Onco | 21 (58.3%) | ||
| Nephro | 15 (41.7%) | ||||
| Overweight (25–29.9) | 26 (31.7%) | Onco | 18 (69.2%) | ||
| Nephro | 8 (30.8%) | ||||
| Obese (>30) | 20 (24.4%) | Onco | 12 (60%) | ||
| Nephro | 8 (40%) | ||||
| CKD | Stage III a | 21 (25.9%) | Onco | 15 (29.4%) | 0.37 2 |
| Nephro | 6 (20%) | ||||
| Stage III b | 32 (39.5%) | Onco | 22 (43.1%) | ||
| Nephro | 10 (33.3%) | ||||
| Stage IV | 28 (34.6%) | Onco | 14 (27.5%) | ||
| Nephro | 14 (46.7%) | ||||
| Diabetes | 10 (12.2%) | Onco | 8 (15.7%) | 0.153 2 | |
| Nephro | 2 (6.5%) | ||||
| Hypertension (HT) | 62 (75.6%) | Onco | 37 (72.5%) | 0.243 2 | |
| Nephro | 25 (80.6%) | ||||
| HT Therapy | ACEi | 13 (21%) | Onco | 9 (69.2%) | 0.63 2 |
| Nephro | 4 (30.2%) | ||||
| Beta-Blockers | 11 (17.7%) | Onco | 9 (81.8%) | 0.19 2 | |
| Nephro | 2 (18.2%) | ||||
| ARBs | 15 (24.2%) | Onco | 9 (60.0%) | 1 2 | |
| Nephro | 6 (40.0%) | ||||
| Calcium Antagonists | 20 (32.3%) | Onco | 10 (50.0%) | 0.43 2 | |
| Nephro | 10 (50.0%) | ||||
| Diuretics | 16 (25.8%) | Onco | 8 (50.0%) | 0.53 2 | |
| Nephro | 8 (50.0%) | ||||
| Vitamin D | No Deficiency | 51 (63.8%) | Onco | 37 (72.5%) | 0.30 1 |
| Nephro | 14 (48.3%) | ||||
| Deficiency | 29 (36.2%) | Onco | 14 (27.5%) | ||
| Nephro | 15 (51.7%) | ||||
| Tumor Location | Total | Surgery Performed | Frequency |
|---|---|---|---|
| Kidney | 26 | Radical Nephrectomy | 16 |
| Partial Nephrectomy | 10 | ||
| Prostate | 6 | Prostatectomy | 6 |
| Bladder | 17 | Cistectomy | 14 |
| TURBK | 3 | ||
| Urothelium | 6 | Nephroureterectomy | 4 |
| TURBK | 2 |
| Before Dietary Intervention | After Dietary Intervention | p-Value | |
|---|---|---|---|
| Phase Angle (PA) | 5.7° [5.2;6.4] | 5.8° [5.3;6.4] | 0.0082 ** |
| ECM/BCM | 0.9 [0.8;1.0] | 0.9 [0.8;1.0] | 0.0049 ** |
| BCM/h2 | 11 kg/h2 [9.5;12.2] | 11.5 kg/h2 [9.8;12.7] | 0.052 |
| BMI | 25.9 kg/h2 [23.5;29.8] | 25.3 kg/h2 [23.3;28.3] | 0.0015 ** |
| Waist Circumference | 95.8 cm [85.2;105.5] | 93 cm [85.2;100] | 0.00045 *** |
| Waist-Hip Ratio | 0.9 [0.9;1] | 0.9 [0.9;1] | 0.012 * |
| ECW/ICW | 0.9 [0.8;1] | 0.9 [0.7;1] | 0.00044 *** |
| TBW (% on body weight) | 59.3 [54.4;61.8] | 61.1 [56.2;63.6] | 0.0005 *** |
| MAMC | 25.9 mm [24.4;27.7] | 25.5 mm [24;27.7] | 0.17 |
| FM/h2 | 5.2 kg/h2 [3.5;7.2] | 3.8 kg/h2 [2.8;6.1] | 0.000012 *** |
| FFM/h2 | 21 kg/h2 [19.6;22.4] | 21.4 kg/h2 [19.8;23] | 0.0002 *** |
| Nephropathic | Onconephropathic | |||
|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |
| PA < 4.5° | 12.9% | 12.9% | 3.9% | 2% |
| ECM/BCM > 1.2 | 11.5% | 11.5% | 8.9% | 4.4% |
| Before Dietary Intervention | After Dietary Intervention | p-Value | |
|---|---|---|---|
| Creatinine | 1.8 mg/dL [1.5;2.4] | 1.8 mg/dL [1.4;2.5] | 0.94 |
| eGFR (epi 2012) | 37 mL/min/1.73m2 [23.6;46.2] | 35.5 mL/min/1.73m2 [23;44.1] | 0.67 |
| mGFR (Iohexol) | 37.5 mL/min/1.73m2 [32.4;44.1] | 36.4 mL/min/1.73m2 [22.8;46.2] | 0.34 |
| Urea | 68 mg/dL [47.2;92.8] | 52 mg/dL [42;74.8] | 0.0000033 *** |
| Vitamin D | 25.5 ug/dL [18.5;37.4] | 36 ug/dL [31.5;43] | 0.000098 *** |
| Bicarbonates | 24.4 mmol/L [22.8;27.2] | 25.5 mmol/L [22.6;28] | 0.95 |
| Cystatin C | 1.4 mg/L [1.2;1.8] | 1.4 mg/L [1.2;1.9] | 0.15 |
| Uric Acid | 5.5 mg/dL [4.8;6.9] | 5.9 mg/dL [3.7;6.6] | 0.52 |
| Potassium | 4.8 mmol/L [4.3;5.4] | 4.7 mmol/L [4.4;5] | 0.48 |
| Vitamin D | ΔMedian | p-Value |
|---|---|---|
| Supplemented | 5.9 [0.0;17.7] | 0.78 |
| Not Supplemented | 11.0 [−1.2;12.3] |
| Nephropathic | Onconephropathic | |||
|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |
| PA | 5.3° [4.9;6] | 5.4° [5;6.2] | 5.9° [5.4;6.6] | 6° [5.6;6.5] |
| BCM/h2 | 11.1 kg/h2 [9;12.1] | 11 kg/h2 [9.2;12.1] | 11.1 kg/h2 [9.8;12.3] | 11.6 kg/h2 [9.9;12.9] |
| ECW/ICW | 0.9 [0.8;1] | 0.9 [0.8;1] | 0.8 [0.8;1] | 0.8 [0.7;0.9] |
| FFM/h2 | 21.2 kg/h2 [19;23.2] | 21.4 kg/h2 [19.2;23.3] | 21 kg/h2 [19.8;22] | 21.2 kg/h2 [20;23] |
| eGFR (epi 2012) | 32.3 mL/min/1.73m2 [20.8;45] | 36.7 mL/min/1.73m2 [21.6;42.6] | 38.8 mL/min/1.73m2 [24.6;46.1] | 34.5 mL/min/1.73m2 [23.8;46.7] |
| mGFR (Iohexol) | 37.5 mL/min/1.73m2 [26.3;41.8] | 38.3 mL/min/1.73m2 [21.9;45.3] | 37.5 mL/min/1.73m2 [33;45] | 36.4 mL/min/1.73m2 [23;46.2] |
| Urea | 87 mg/dL [43;119.5] | 58 mg/dL [42.5;79.5] | 63 mg/dL [48;91] | 51 mg/dL [42;69] |
| Vitamin D | 32.2 ug/dL [21.6;42.6] | 36.6 ug/dL [28.9;42.8] | 24 ug/dL [15.7;35] | 35.8 ug/dL [32;43] |
| Bicarbonates | 23.6 mmol/L [22.5;24.3] |
25 mmol/L [22.1;27.2] |
25.8 mmol/L [24;28] | 26.6 mmol/L [24.6;28.4] |
| Uric Acid | 5.5 mg/dL [4.5;7.3] | 4.6 mg/dL [3.6;6.5] | 5.5 mg/dL [5.3;6.8] | 6.2 mg/dL [4.5;6.6] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bettiga, A.; Fiorio, F.; Liguori, F.; Marco, F.D.; Quattrini, G.; Vago, R.; Giannese, D.; Salonia, A.; Montorsi, F.; Trevisani, F. The Impact of a Mediterranean-like Diet with Controlled Protein Intake on the Onco-Nephrological Scenario: Time for a New Perspective. Nutrients 2022, 14, 5193. https://doi.org/10.3390/nu14235193
Bettiga A, Fiorio F, Liguori F, Marco FD, Quattrini G, Vago R, Giannese D, Salonia A, Montorsi F, Trevisani F. The Impact of a Mediterranean-like Diet with Controlled Protein Intake on the Onco-Nephrological Scenario: Time for a New Perspective. Nutrients. 2022; 14(23):5193. https://doi.org/10.3390/nu14235193
Chicago/Turabian StyleBettiga, Arianna, Francesco Fiorio, Francesca Liguori, Federico Di Marco, Giulia Quattrini, Riccardo Vago, Domenico Giannese, Andrea Salonia, Francesco Montorsi, and Francesco Trevisani. 2022. "The Impact of a Mediterranean-like Diet with Controlled Protein Intake on the Onco-Nephrological Scenario: Time for a New Perspective" Nutrients 14, no. 23: 5193. https://doi.org/10.3390/nu14235193
APA StyleBettiga, A., Fiorio, F., Liguori, F., Marco, F. D., Quattrini, G., Vago, R., Giannese, D., Salonia, A., Montorsi, F., & Trevisani, F. (2022). The Impact of a Mediterranean-like Diet with Controlled Protein Intake on the Onco-Nephrological Scenario: Time for a New Perspective. Nutrients, 14(23), 5193. https://doi.org/10.3390/nu14235193