
Self-Reported Dietary Management Behaviors and Dietary Intake among Chinese Adults with Diabetes: A Population-Based Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
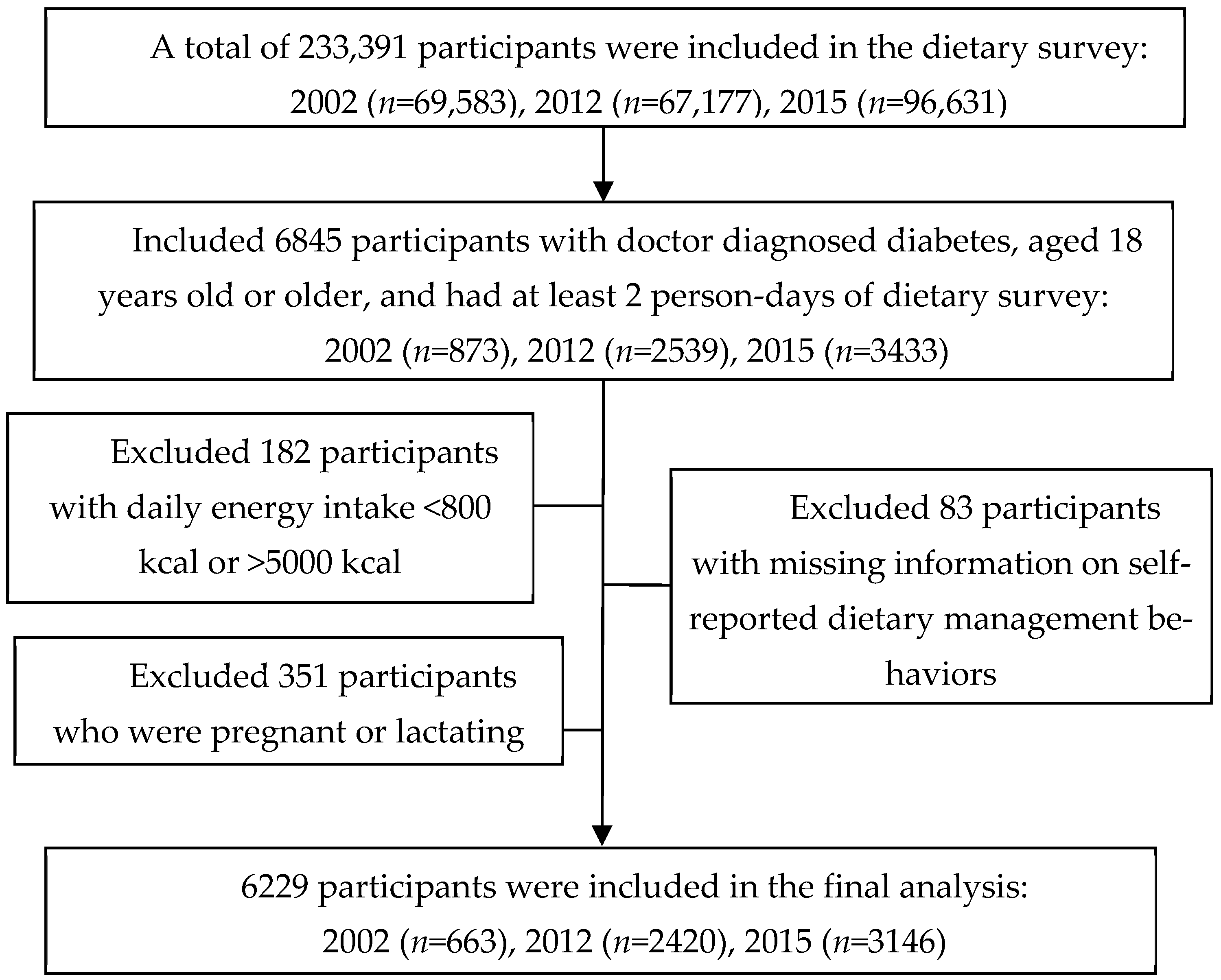
2.1. Study Population and Sampling
2.2. Data Collection and Measurements
2.3. Definitions of Diabetic Patients and Dietary Management
2.4. Dietary Assessment
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Dietary Intake
3.3. Diet Quality Score
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ogurtsova, K.; Guariguata, L.; Barengo, N.C.; Ruiz, P.L.; Sacre, J.W.; Karuranga, S.; Sun, H.; Boyko, E.J.; Magliano, D.J. IDF diabetes Atlas: Global estimates of undiagnosed diabetes in adults for 2021. Diabetes Res. Clin. Pract. 2022, 183, 109118. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Teng, D.; Shi, X.; Qin, G.; Qin, Y.; Quan, H.; Shi, B.; Sun, H.; Ba, J.; Chen, B.; et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: National cross sectional study. BMJ 2020, 369, m997. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 3. Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S32–S36. [Google Scholar] [CrossRef]
- Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China(2020 edition) (part 1). Chin. J. Pract. Intern. Med. 2021, 41, 668–695. [Google Scholar] [CrossRef]
- Akbar, H.; Anderson, D.; Gallegos, D. Predicting intentions and behaviours in populations with or at-risk of diabetes: A systematic review. Prev. Med. Rep. 2015, 2, 270–282. [Google Scholar] [CrossRef]
- Hawley, J.A.; Sassone-Corsi, P.; Zierath, J.R. Chrono-nutrition for the prevention and treatment of obesity and type 2 diabetes: From mice to men. Diabetologia 2020, 63, 2253–2259. [Google Scholar] [CrossRef]
- Katsaridis, S.; Grammatikopoulou, M.G.; Gkiouras, K.; Tzimos, C.; Papageorgiou, S.T.; Markaki, A.G.; Exiara, T.; Goulis, D.G.; Papamitsou, T. Low Reported Adherence to the 2019 American Diabetes Association Nutrition Recommendations among Patients with Type 2 Diabetes Mellitus, Indicating the Need for Improved Nutrition Education and Diet Care. Nutrients 2020, 12, 3516. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Vollenweider, P.; Grange, M.; Guessous, I.; Waeber, G. Dietary intake of subjects with diabetes is inadequate in Switzerland: The CoLaus study. Eur. J. Nutr. 2017, 56, 981–989. [Google Scholar] [CrossRef]
- Saleh, F.; Mumu, S.J.; Ara, F.; Hafez, M.A.; Ali, L. Non-adherence to self-care practices & medication and health related quality of life among patients with type 2 diabetes: A cross-sectional study. BMC Public Health 2014, 14, 431. [Google Scholar] [CrossRef]
- Mai, T.; Mo, C.; Cai, J.; He, H.; Lu, H.; Tang, X.; Chen, Q.; Xu, X.; Nong, C.; Liu, S.; et al. Adherence to dietary guide for elderly adults and health risks of older adults in ethnic minority areas in China: A cross-sectional study. BMC Public Health 2022, 22, 372. [Google Scholar] [CrossRef]
- Ping, Z.; Bao-zhu, Y.; Xin-xin, L. Compliance of diet therapy and its influence factors among patients with diabetes mellitus. Chin. J. Public Health 2010, 26, 1563–1564. [Google Scholar] [CrossRef]
- Bukhsh, A.; Goh, B.H.; Zimbudzi, E.; Lo, C.; Zoungas, S.; Chan, K.G.; Khan, T.M. Type 2 Diabetes Patients’ Perspectives, Experiences, and Barriers Toward Diabetes-Related Self-Care: A Qualitative Study From Pakistan. Front. Endocrinol. 2020, 11, 534873. [Google Scholar] [CrossRef]
- He, Y.; Zhao, W.; Zhang, J.; Zhao, L.; Yang, Z.; Huo, J.; Yang, L.; Wang, J.; He, L.; Sun, J.; et al. Data Resource Profile: China National Nutrition Surveys. Int. J. Epidemiol. 2019, 48, 368–368f. [Google Scholar] [CrossRef]
- Yang, Y. China Food Composition Tables, 2nd ed.; Peking University Medical Press: Beijing, China, 2009. [Google Scholar]
- Yang, Y. China Food Composition Tables, 2002nd ed.; Peking University Medical Press: Beijing, China, 2002. [Google Scholar]
- Shan, Z.; Rehm, C.D.; Rogers, G.; Ruan, M.; Wang, D.D.; Hu, F.B.; Mozaffarian, D.; Zhang, F.F.; Bhupathiraju, S.N. Trends in Dietary Carbohydrate, Protein, and Fat Intake and Diet Quality Among US Adults, 1999–2016. JAMA 2019, 322, 1178–1187. [Google Scholar] [CrossRef]
- Wang, S.-s.; Lay, S.; Yu, H.-n.; Shen, S.-r. Dietary guidelines for Chinese residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef]
- He, Y.; Fang, Y.; Yang, X. Establishment and application of China healthy diet index. Acta Nutr. Sin. 2017, 39, 436–441. [Google Scholar] [CrossRef]
- Zhu, Z.; Yang, X.; Fang, Y.; Zhang, J.; Yang, Z.; Wang, Z.; Liu, A.; He, L.; Sun, J.; Lian, Y.; et al. Trends and Disparities of Energy Intake and Macronutrient Composition in China: A Series of National Surveys, 1982–2012. Nutrients 2020, 12, 2168. [Google Scholar] [CrossRef]
- Ponzo, V.; Rosato, R.; Tarsia, E.; Goitre, I.; De Michieli, F.; Fadda, M.; Monge, T.; Pezzana, A.; Broglio, F.; Bo, S. Self-reported adherence to diet and preferences towards type of meal plan in patient with type 2 diabetes mellitus. A cross-sectional study. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 642–650. [Google Scholar] [CrossRef]
- Yang, X.; Yuan, L.; Guo, X. Current situation of diet self-management in patients with type 2 diabetes: A multi-centre survey in China. Chin. J. Diabetes Mellit. 2013, 5, 666–669. [Google Scholar] [CrossRef]
- Liu, K.; Zhao, X.; Chen, J. Study on the control rates of type 2 diabetes and its influencing factors in Chuansha community of Shanghai. Chin. J. Health Educ. 2016, 32, 544–546+550. [Google Scholar] [CrossRef]
- Wang, X.; Li, M.A.; Lili, L.I.; School, N. The Current Status and Influencing Factors of Self-management Level in Patients with Type 2 Diabetic in Community. J. Ningxia Med. Univ. 2017, 39, 436–442. [Google Scholar] [CrossRef]
- Alexandre, K.; Campbell, J.; Bugnon, M.; Henry, C.; Schaub, C.; Serex, M.; Elmers, J.; Desrichard, O.; Peytremann-Bridevaux, I. Factors influencing diabetes self-management in adults: An umbrella review of systematic reviews. JBI Evid. Synth. 2021, 19, 1003–1118. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.; Ramachandran, A.; Yancy, W.S., Jr.; Forouhi, N.G. Nutritional basis of type 2 diabetes remission. BMJ 2021, 374, n1449. [Google Scholar] [CrossRef] [PubMed]
- Bagnasco, A.; Di Giacomo, P.; Da Rin Della Mora, R.; Catania, G.; Turci, C.; Rocco, G.; Sasso, L. Factors influencing self-management in patients with type 2 diabetes: A quantitative systematic review protocol. J. Adv. Nurs. 2014, 70, 187–200. [Google Scholar] [CrossRef]
- Gopalan, A.; Kellom, K.; McDonough, K.; Schapira, M.M. Exploring how patients understand and assess their diabetes control. BMC Endocr. Disord. 2018, 18, 79. [Google Scholar] [CrossRef]
- Lambrinou, E.; Hansen, T.B.; Beulens, J.W. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur. J. Prev. Cardiol. 2019, 26, 55–63. [Google Scholar] [CrossRef]
- Diabetes Professional Committee of Chinese Research Hospital Association, S.D.C. Expert Consensus on Diabetes Self-Management Education and Support for Adults with Type 2 Diabetes Mellitus in Primary Healthcare Institutions. Chin. J. Diabetes Mellit. 2022, 14, 307–315. [Google Scholar] [CrossRef]
- Viguiliouk, E.; Stewart, S.E.; Jayalath, V.H.; Ng, A.P.; Mirrahimi, A.; de Souza, R.J.; Hanley, A.J.; Bazinet, R.P.; Blanco Mejia, S.; Leiter, L.A.; et al. Effect of Replacing Animal Protein with Plant Protein on Glycemic Control in Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 9804–9824. [Google Scholar] [CrossRef]
- Breen, C.; Ryan, M.; McNulty, B.; Gibney, M.J.; Canavan, R.; O’Shea, D. High saturated-fat and low-fibre intake: A comparative analysis of nutrient intake in individuals with and without type 2 diabetes. Nutr. Diabetes 2014, 4, e104. [Google Scholar] [CrossRef]
- Vitale, M.; Masulli, M.; Cocozza, S.; Anichini, R.; Babini, A.C.; Boemi, M.; Bonora, E.; Buzzetti, R.; Carpinteri, R.; Caselli, C.; et al. Sex differences in food choices, adherence to dietary recommendations and plasma lipid profile in type 2 diabetes—The TOSCA.IT study. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 879–885. [Google Scholar] [CrossRef]
- Ewers, B.; Trolle, E.; Jacobsen, S.S.; Vististen, D.; Almdal, T.P.; Vilsboll, T.; Bruun, J.M. Dietary habits and adherence to dietary recommendations in patients with type 1 and type 2 diabetes compared with the general population in Denmark. Nutrition 2019, 61, 49–55. [Google Scholar] [CrossRef]
- Mehta, S.N.; Haynie, D.L.; Higgins, L.A.; Bucey, N.N.; Rovner, A.J.; Volkening, L.K.; Nansel, T.R.; Laffel, L.M. Emphasis on carbohydrates may negatively influence dietary patterns in youth with type 1 diabetes. Diabetes Care 2009, 32, 2174–2176. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Hattori, M.; Wada, S.; Iwase, H.; Kadono, M.; Tatsumi, H.; Kuwahata, M.; Fukui, M.; Hasegawa, G.; Nakamura, N.; et al. Assessment of daily food and nutrient intake in Japanese type 2 diabetes mellitus patients using dietary reference intakes. Nutrients 2013, 5, 2276–2288. [Google Scholar] [CrossRef]
- Burch, E.; Ball, L.; Somerville, M.; Williams, L.T. Dietary intake by food group of individuals with type 2 diabetes mellitus: A systematic review. Diabetes Res. Clin. Pract. 2018, 137, 160–172. [Google Scholar] [CrossRef]
- Lopez-Olmedo, N.; Jonnalagadda, S.; Basto-Abreu, A.; Reyes-Garcia, A.; Alish, C.J.; Shamah-Levy, T.; Barrientos-Gutierrez, T. Adherence to Dietary Guidelines in Adults by Diabetes Status: Results From the 2012 Mexican National Health and Nutrition Survey. Nutrients 2020, 12, 3464. [Google Scholar] [CrossRef]
- Huang, F.; Wang, Z.; Wang, L.; Wang, H.; Zhang, J.; Du, W.; Su, C.; Jia, X.; Ouyang, Y.; Wang, Y.; et al. Evaluating adherence to recommended diets in adults 1991-2015: Revised China dietary guidelines index. Nutr. J. 2019, 18, 70. [Google Scholar] [CrossRef]
- He, Y.; Li, Y.; Yang, X.; Hemler, E.C.; Fang, Y.; Zhao, L.; Zhang, J.; Yang, Z.; Wang, Z.; He, L.; et al. The dietary transition and its association with cardiometabolic mortality among Chinese adults, 1982–2012: A cross-sectional population-based study. Lancet Diabetes Endocrinol. 2019, 7, 540–548. [Google Scholar] [CrossRef]
- Thanopoulou, A.; Karamanos, B.; Angelico, F.; Assaad-Khalil, S.; Barbato, A.; Del Ben, M.; Djordjevic, P.; Dimitrijevic-Sreckovic, V.; Gallotti, C.; Katsilambros, N.; et al. Nutritional habits of subjects with Type 2 diabetes mellitus in the Mediterranean Basin: Comparison with the non-diabetic population and the dietary recommendations. Multi-Centre Study of the Mediterranean Group for the Study of Diabetes (MGSD). Diabetologia 2004, 47, 367–376. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Liu, W.; Ji, L.; Mendez, M.A.; Du, S.; Crandell, J.; Rosamond, W.; Mayer-Davis, E.J. Diabetes nutrition therapy and dietary intake among individuals with Type 1 diabetes in China. Diabet. Med. 2015, 32, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Vijan, S.; Stuart, N.S.; Fitzgerald, J.T.; Ronis, D.L.; Hayward, R.A.; Slater, S.; Hofer, T.P. Barriers to following dietary recommendations in Type 2 diabetes. Diabet. Med. 2005, 22, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, Y.; Li, L. Diabetes Management in China: Types and Reflections. Chin. Gen. Pract. 2021, 24, 3019–3025. [Google Scholar] [CrossRef]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall n = 6229 | Dietary Management: Yes n = 4857 | Dietary Management: No n = 1372 | p |
|---|---|---|---|---|
| Gender | ||||
| Male | 2801 (48.7) | 2118 (47.1) | 683 (54.3) | <0.001 |
| Female | 3428 (51.3) | 2739 (52.9) | 689 (45.7) | |
| Age group (years) | ||||
| 18–39 | 150 (6.3) | 113 (6.1) | 37 (6.9) | 0.250 |
| 40–64 | 3681 (61.6) | 2844 (61.1) | 837 (63.4) | |
| ≥65 | 2398 (32.1) | 1900 (32.8) | 498 (29.7) | |
| Area | ||||
| Urban | 4133 (69.2) | 3332 (71.2) | 801 (62.3) | <0.001 |
| Rural | 2096 (30.8) | 1525 (28.8) | 571 (37.7) | |
| Annual income per capita | ||||
| Very low | 1089 (17.4) | 788 (16.2) | 301 (21.6) | 0.002 |
| Low | 1150 (18.4) | 867 (18.0) | 283 (19.9) | |
| Middle | 1257 (20.9) | 982 (21.0) | 275 (20.6) | |
| High | 1161 (20.1) | 936 (20.5) | 225 (18.7) | |
| Very high | 1398 (23.2) | 1145 (24.3) | 253 (19.2) | |
| Education level | ||||
| Under primary | 912 (12.7) | 693 (12.4) | 219 (14.0) | 0.646 |
| Primary school | 1329 (21.0) | 1024 (20.7) | 305 (21.6) | |
| Junior high school | 1574 (26.0) | 1231 (26.3) | 343 (24.9) | |
| Senior high school | 1463 (23.9) | 1148 (22.9) | 315 (24.1) | |
| Junior college and above | 951 (16.4) | 761 (16.7) | 190 (15.4) | |
| Marital status | ||||
| Single | 36 (1.3) | 25 (1.1) | 11 (2.2) | 0.073 |
| Married/Cohabiting | 5571 (88.8) | 4352 (89.2) | 1219 (87.3) | |
| Widowed/Divorced/Separated | 621 (9.9) | 479 (9.7) | 142 (10.5) | |
| Body mass index (kg/m2) | ||||
| <18.5 | 95 (1.7) | 74 (1.8) | 21 (1.6) | 0.217 |
| 18.5–23.9 | 1925 (32.3) | 1537 (33.1) | 388 (29.1) | |
| 24–27.9 | 2607 (42.9) | 2018 (42.2) | 589 (45.4) | |
| ≥28 | 1397 (23.1) | 1073 (22.9) | 324 (23.9) | |
| HbA1c (%) | 6.8 ± 1.8 | 6.8 ± 1.8 | 6.8 ± 1.8 | 0.411 |
| Fasting Plasma Glucose (mmol/L) | 8.3 ± 3.2 | 8.2 ± 3.2 | 8.4 ± 3.5 | 0.134 |
| Variable | Guideline Targets 1 | Weighted Mean (95% CI) | p | Adjusted p-Value 2 | |
|---|---|---|---|---|---|
| Dietary Management: Yes | Dietary Management: No | ||||
| Energy and nutrients 3 | |||||
| Energy intake, kcal/day | 1756.0 | 1821.1 | 0.007 | 0.186 | |
| (1734.2–1777.9) | (1778.8–1864.2) | ||||
| Total carbohydrates, E% | 50–65 | 52.0 | 53.5 | 0.004 | 0.001 |
| (51.5–52.5) | (52.6–54.4) | ||||
| High-quality carbohydrates, E% | 5.3 | 4.6 | <0.001 | 0.026 | |
| (5.1–5.5) | (4.3–5.0) | ||||
| Low-quality carbohydrates, E% | 46.7 | 48.8 | <0.001 | <0.001 | |
| (46.2–47.1) | (47.9–49.8) | ||||
| Total protein, E% | 15–20 | 13.1 | 12.8 | 0.007 | 0.178 |
| (13.0–13.3) | (12.5–13.0) | ||||
| Animal protein, E% | 4.8 | 4.3 | <0.001 | 0.015 | |
| (4.7–4.9) | (4.0–4.5) | ||||
| Plant protein, E% | 7.4 | 7.5 | 0.176 | 0.030 | |
| (7.3–7.5) | (7.3–7.7) | ||||
| Total fat, E% | 20–30 | 35.4 | 33.8 | 0.001 | <0.001 |
| (35.0–35.9) | (32.9–34.7) | ||||
| Saturated fatty acids, E% | 8.7 | 8.3 | 0.006 | 0.006 | |
| (8.5–8.8) | (8.0–8.5) | ||||
| Monounsaturated fatty acids, E% | 14.2 | 13.5 | 0.007 | 0.002 | |
| (14.0–14.5) | (13.1–14.0) | ||||
| Polyunsaturated fatty acids, E% | 11.2 | 10.3 | <0.001 | 0.002 | |
| (10.9–11.4) | (9.9–10.7) | ||||
| Fiber, g/1000 kcal | >14 | 8.6 | 8.4 | 0.269 | 0.618 |
| (8.4–8.7) | (8.0–8.7) | ||||
| Food groups | |||||
| Cereals and tubers, g/day | 250–400 | 330.2 | 363.1 | <0.001 | <0.001 |
| (324.5–324.5) | (351.1–375.6) | ||||
| Soybeans and nuts, g/day | 25–35 | 59.0 | 50.4 | 0.002 | 0.060 |
| (56.0–62.0) | (45.8–54.9) | ||||
| Vegetables, g/day | 300–500 | 281.2 | 256.4 | <0.001 | <0.001 |
| (274.8–287.7) | (245.2–267.6) | ||||
| Fruits, g/day | 200–350 | 105.1 | 117.7 | 0.345 | 0.506 |
| (84.5–130.8) | (63.3–218.9) | ||||
| Livestock and poultry meats, g/day | 40–75 | 83.5 | 79.4 | 0.231 | 0.076 |
| (80.3–86.7) | (73.0–85.8) | ||||
| Dairy products, g/day | >300 | 141.9 | 134.6 | 0.452 | 0.815 |
| (133.6–150.6) | (119.1–152.1) | ||||
| Eggs, g/day | 40–50 | 48.1 | 49.3 | 0.626 | 0.411 |
| (41.0–56.3) | (35.3–68.8) | ||||
| Aquatic products, g/day | 40–75 | 39.1 | 35.0 | 0.137 | 0.588 |
| (36.5–41.7) | (30.4–39.7) | ||||
| Oil, g/day | 25–30 | 31.9 | 31.1 | 0.414 | 0.046 |
| (31.0–32.8) | (29.5–32.8) | ||||
| Salt, g/day | <6 | 7.6 | 8.1 | 0.079 | 0.187 |
| (7.5–7.9) | (7.7–8.5) | ||||
| CHDI Component | Score Range | Standard for Maximum Score | Standard for Minimum Score of Zero | Weighted Mean ± SD | p | Adjusted p-Value 1 | |
|---|---|---|---|---|---|---|---|
| Dietary Management: Yes | Dietary Management: No | ||||||
| Food variety | 0–10 | ≥12 kind | ≤5 kind | 6.0 ± 2.9 | 5.5 ± 3.0 | <0.001 | 0.002 |
| Refined grains | 0–5 | ≥100 g/1000 kcal | 0 | 4.6 ± 0.9 | 4.7 ± 0.8 | 0.033 | 0.047 |
| Whole grain, dry bean, and tuber | 0–5 | ≥40 g/1000 kcal | 0 | 2.7 ± 2.1 | 2.7 ± 2.1 | 0.983 | 0.738 |
| Total vegetables | 0–5 | ≥180 g/1000 kcal | 0 | 3.6 ± 1.4 | 3.3 ± 1.4 | <0.001 | <0.001 |
| Dark green and orange vegetables | 0–5 | ≥90 g/1000 kcal | 0 | 2.4 ± 1.9 | 2.0 ± 1.8 | <0.001 | <0.001 |
| Fruit | 0–10 | ≥110 g/1000 kcal | 0 | 1.8 ± 1.4 | 1.8 ± 1.4 | 0.801 | 0.114 |
| Dairy | 0–10 | ≥100 g/1000 kcal | 0 | 6.4 ± 1.9 | 6.3 ± 1.8 | 0.670 | 0.917 |
| Soybean | 0–10 | ≥10 g/1000 kcal | 0 | 5.7 ± 4.8 | 5.6 ± 4.8 | 0.335 | 0.192 |
| Meat and egg | 0–5 | ≥50 g/1000 kcal | 0 | 3.9 ± 1.6 | 3.6 ± 1.8 | <0.001 | <0.001 |
| Fish, shellfish and mollusk | 0–5 | ≥30 g/1000 kcal | 0 | 3.6 ± 1.9 | 3.5 ± 1.9 | 0.872 | 0.171 |
| Calories from SFAs | 0–10 | <10% | ≥15% | 8.5 ± 2.9 | 8.7 ± 2.7 | 0.091 | 0.022 |
| Sodium | 0–10 | ≤1 g/1000 kcal | ≥4 g/1000 kcal | 4.5 ± 3.3 | 4.5 ± 3.3 | 0.958 | 0.690 |
| Empty calories | 0–10 | ≤20% | ≥40% | 8.5 ± 2.9 | 8.7 ± 2.8 | 0.279 | 0.123 |
| Total | 0–100 | 56.3 ± 12.7 | 54.1 ± 12.3 | <0.001 | 0.016 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Yu, D.; Luo, J.; Cai, S.; Ye, P.; Yao, Z.; Luo, M.; Zhao, L. Self-Reported Dietary Management Behaviors and Dietary Intake among Chinese Adults with Diabetes: A Population-Based Study. Nutrients 2022, 14, 5178. https://doi.org/10.3390/nu14235178
Liu Y, Yu D, Luo J, Cai S, Ye P, Yao Z, Luo M, Zhao L. Self-Reported Dietary Management Behaviors and Dietary Intake among Chinese Adults with Diabetes: A Population-Based Study. Nutrients. 2022; 14(23):5178. https://doi.org/10.3390/nu14235178
Chicago/Turabian StyleLiu, Yixu, Dongmei Yu, Jiayou Luo, Shuya Cai, Ping Ye, Zhenzhen Yao, Miyang Luo, and Liyun Zhao. 2022. "Self-Reported Dietary Management Behaviors and Dietary Intake among Chinese Adults with Diabetes: A Population-Based Study" Nutrients 14, no. 23: 5178. https://doi.org/10.3390/nu14235178
APA StyleLiu, Y., Yu, D., Luo, J., Cai, S., Ye, P., Yao, Z., Luo, M., & Zhao, L. (2022). Self-Reported Dietary Management Behaviors and Dietary Intake among Chinese Adults with Diabetes: A Population-Based Study. Nutrients, 14(23), 5178. https://doi.org/10.3390/nu14235178