
Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia




Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Olfactory Function Assessment
2.3. Gustatory Function Assessment
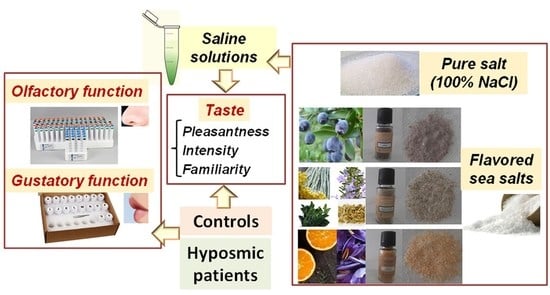
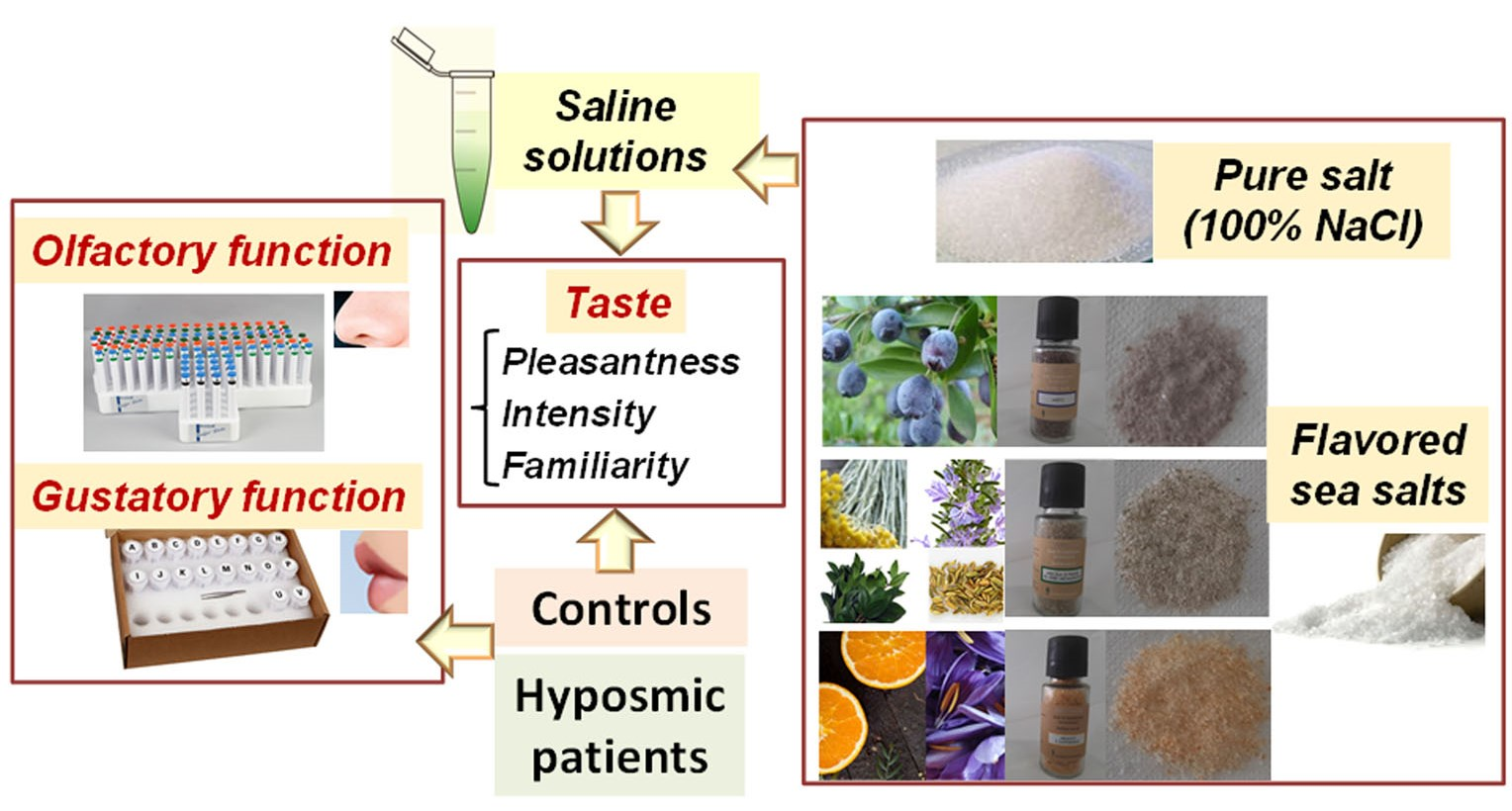
2.4. Gustatory Stimuli
2.5. Procedures to Assess Taste Pleasantness, Intensity, and Familiarity of Sea Salt Solutions
2.6. Statistical Analyses
3. Results
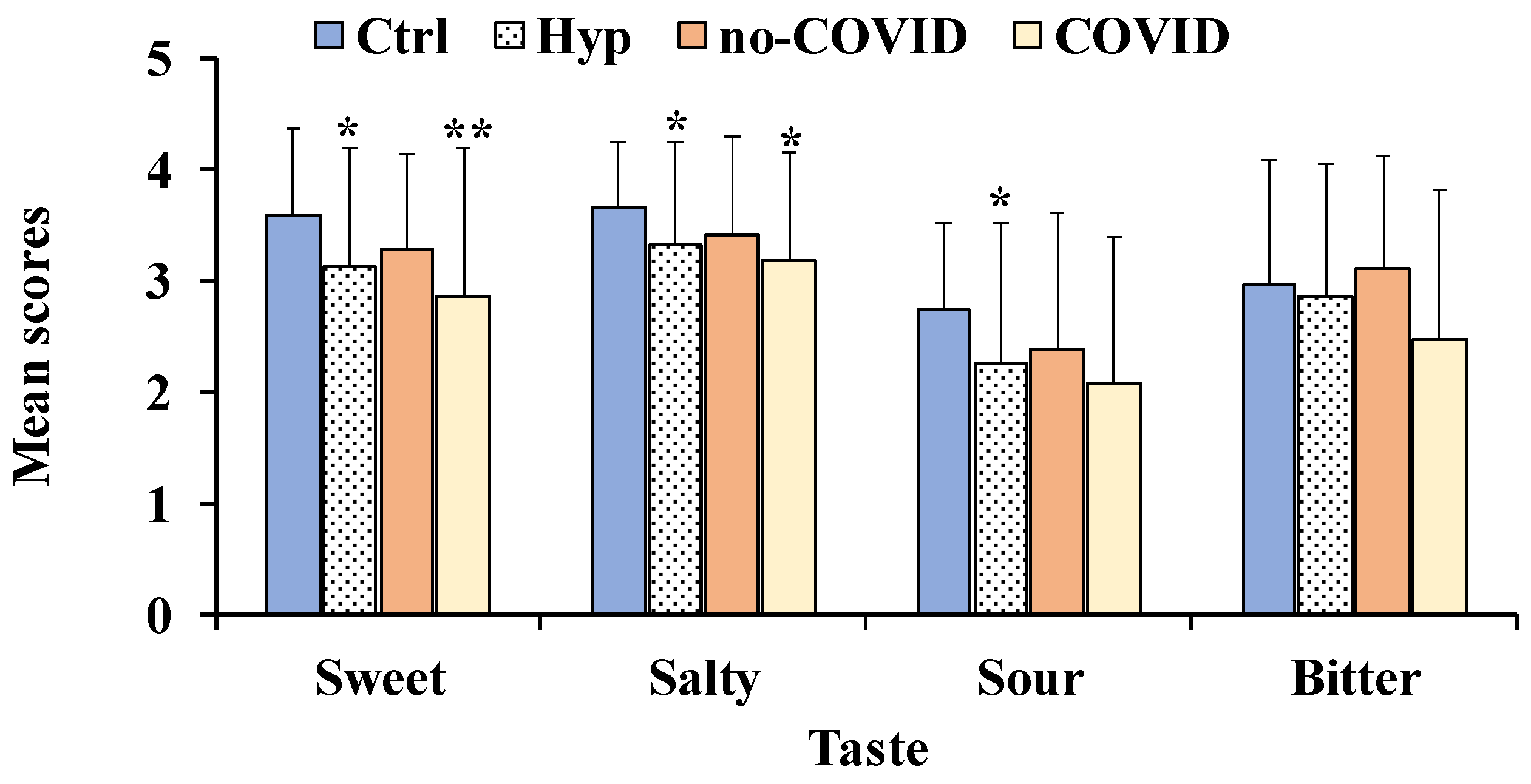
3.1. Differences in Olfactory and Gustatory Function between Total Patients with Hyposmia, No-COVID, and COVID Patients Compared to Healthy Controls
3.2. Correlations between Olfactory Function and Each Taste Perception
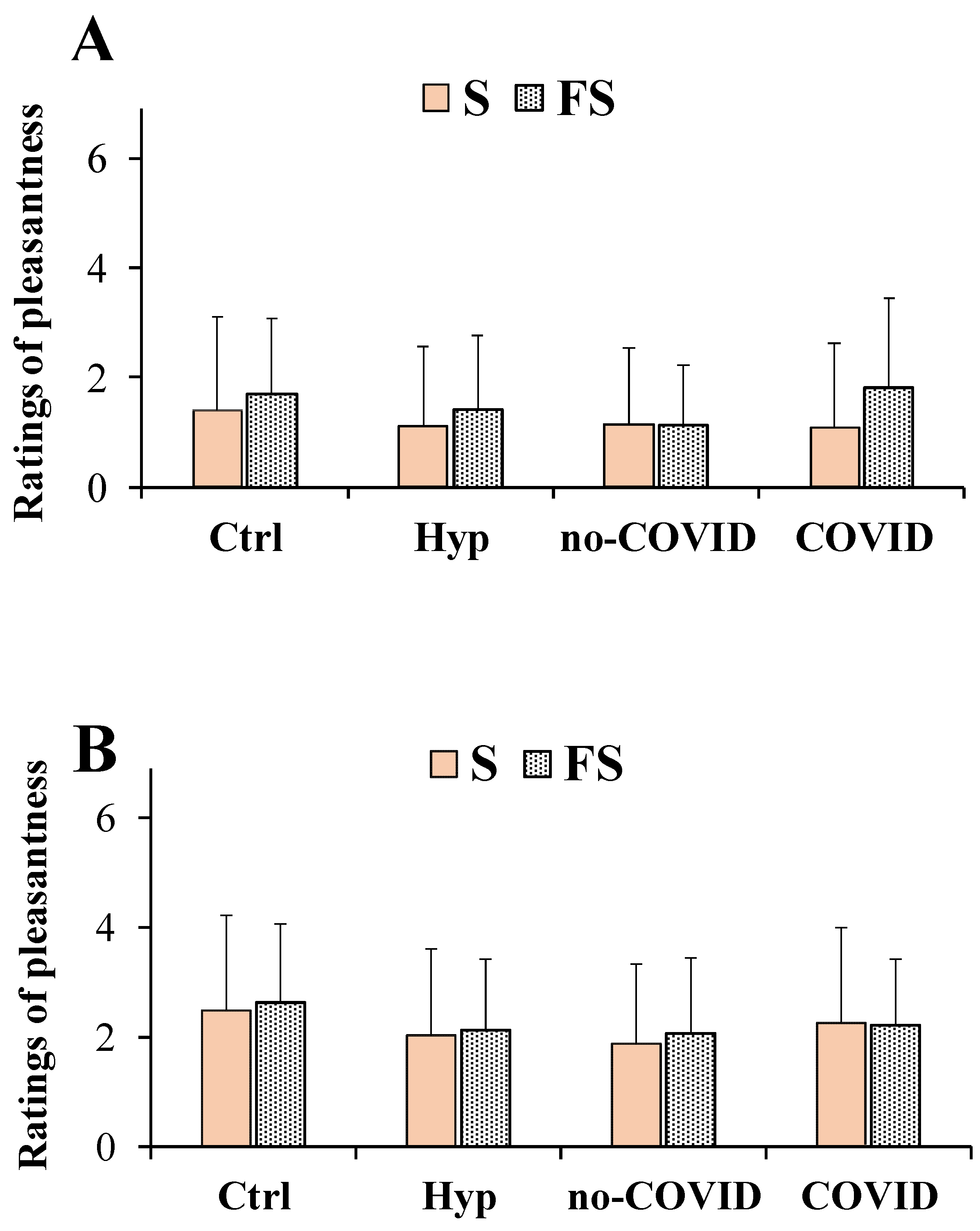
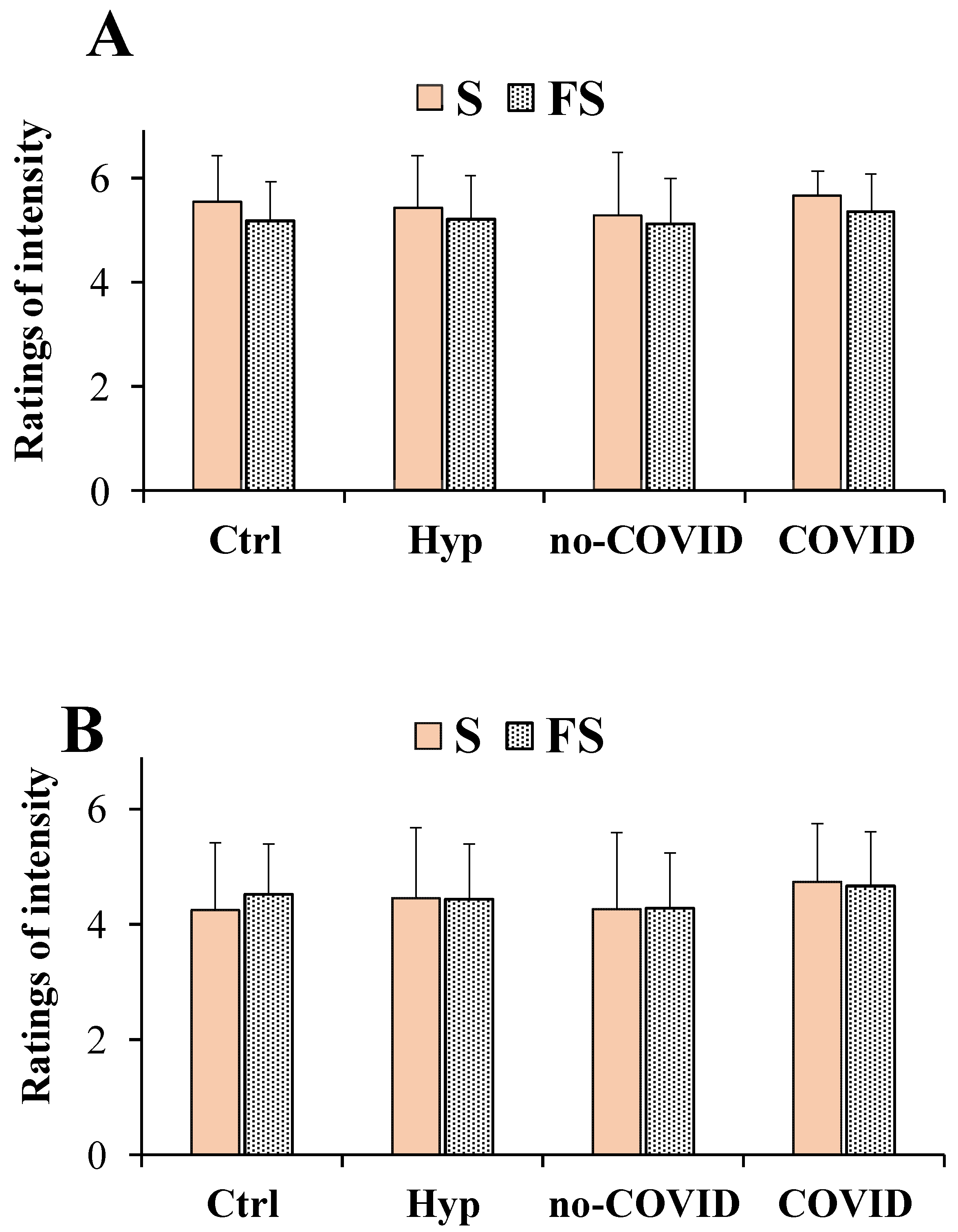
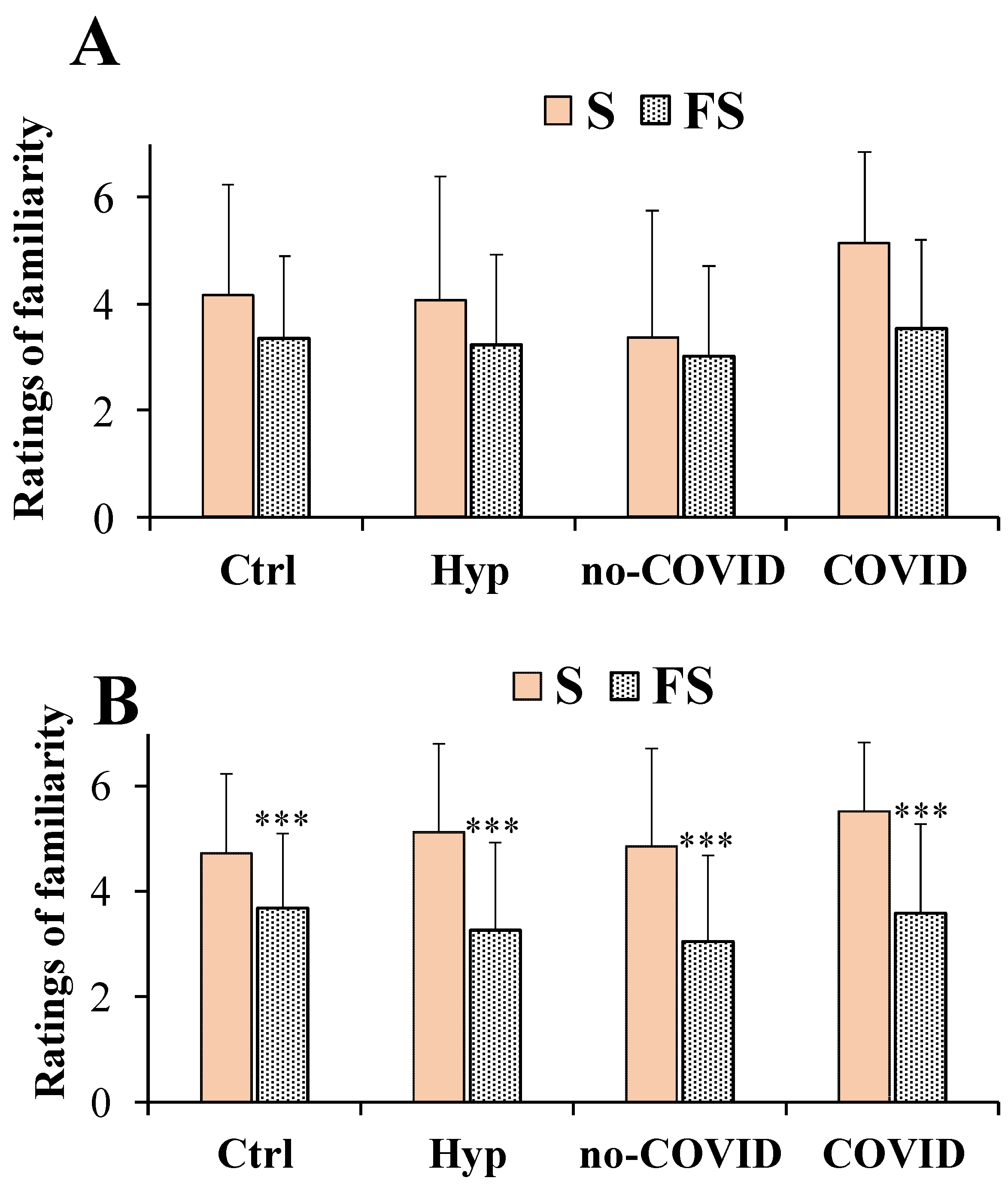
3.3. Ratings of Taste Pleasantness, Intensity, and Familiarity for the Saline Solutions Obtained with Normal Sea Salt and Flavored Salts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bigiani, A. Salt taste, nutrition, and health. Nutrients 2020, 12, 1537. [Google Scholar] [CrossRef] [PubMed]
- WHO. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting. 2007. Available online: https://apps.who.int/iris/bitstream/handle/10665/43653/9789241595377_eng.pdf (accessed on 28 April 2020).
- Rosa, A.; Pinna, I.; Piras, A.; Porcedda, S.; Masala, C. Flavoring of sea salt with Mediterranean aromatic plants affects salty taste perception. J. Sci. Food Agric. 2022, 102, 6005–6013. [Google Scholar] [CrossRef]
- Liem, D.G.; Miremadi, F.; Keast, R.S.J. Reducing sodium in foods: The effect on flavor. Nutrients 2011, 3, 694–711. [Google Scholar] [CrossRef]
- Kloss, L.; Meyer, J.D.; Graeve, L.; Vetter, W. Sodium intake and its reduction by food reformulation in the European Union—A review. NFS J. 2015, 1, 9–19. [Google Scholar] [CrossRef]
- Mariutti, L.R.; Bragagnolo, N. Influence of salt on lipid oxidation in meat and seafood products: A review. Food Res. Int. 2017, 94, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Ghawi, S.K.; Rowland, I.; Methven, L. Enhancing consumer liking of low salt tomato soup over repeated exposure by herb and spice seasonings. Appetite 2014, 81, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Dougkas, A.; Vannereux, M.; Giboreau, A. The impact of herbs and spices on increasing the appreciation and intake of low-salt legume-based meals. Nutrients 2019, 11, 2901. [Google Scholar] [CrossRef]
- Costa, D.C.; Costa, H.S.; Albuquerque, T.G.; Ramos, F.; Castilho, M.C.; Sanches-Silva, A. Advances in phenolic compounds analysis of aromatic plants and their potential applications. Trends Food Sci. Technol. 2015, 45, 336–354. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, W.; Zhang, H.; Chen, H.; Wang, S.; Sun, B. The Enhancement of the perception of saltiness by odorants selected from Chinese Douchi in salt solution. Foods 2022, 11, 2260. [Google Scholar] [CrossRef]
- Bojanowski, V.; Hummel, T. Retronasal perception of odors. Physiol. Behav. 2012, 107, 484–487. [Google Scholar] [CrossRef]
- Shepherd, G.M. Smell images and the flavour system in the human brain. Nature 2006, 444, 316–321. [Google Scholar] [CrossRef]
- Aschenbrenner, K.; Hummel, C.; Teszmer, K.; Krone, F.; Ishimaru, T.; Seo, H.S.; Hummel, T. The influence of olfactory loss on dietary behaviors. Laryngoscope 2008, 118, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Aschenbrenner, K.; Scholze, N.; Joraschky, P.; Hummel, T. Gustatory and olfactory sensitivity in patients with anorexia and bulimia in the course of treatment. J. Psychiatr. Res. 2008, 43, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Walliczek-Dworschak, U.; Hummel, T. The human sense of olfaction. Facial Plast. Surg. 2017, 33, 396–404. [Google Scholar] [PubMed]
- Zang, Y.; Han, P.; Burghardt, S.; Knaapila, A.; Schriever, V.; Hummel, T. Influence of olfactory dysfunction on the perception of food. Eur. Arch. Otorhinolaryngol. 2019, 276, 2811–2817. [Google Scholar] [CrossRef] [PubMed]
- Passàli, G.C.; Ralli, M.; Galli, J.; Calò, L.; Paludetti, G. How relevant is the impairment of smell for the quality of life in allergic rhinitis? Curr. Opin. Allergy Clin. Immunol. 2008, 8, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Henkin, R.I. Effects of smell loss (hyposmia) on salt usage. Nutrition 2014, 30, 690–695. [Google Scholar] [CrossRef]
- Koyama, S.; Kondo, K.; Ueha, R.; Kashiwadani, H.; Heinbockel, T. Possible Use of Phytochemicals for Recovery from COVID-19-Induced Anosmia and Ageusia. Int. J. Mol. Sci. 2021, 22, 8912. [Google Scholar] [CrossRef]
- Masala, C.; Käehling, C.; Fall, F.; Hummel, T. Correlation between olfactory function, trigeminal sensitivity, and nasal anatomy in healthy subjects. Eur. Arch. Otorhinolaryngol. 2019, 276, 1649–1654. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Solla, P.; Liscia, A.; Defazio, G.; Saba, L.; Cannas, A.; Cavazzana, A.; Hummel, T.; Haehner, A. Correlation among olfactory function, motors’ symptoms, cognitive impairment, apathy, and fatigue in patients with Parkinson’s disease. J. Neurol. 2018, 265, 1764–1771. [Google Scholar] [CrossRef]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ sticks’: Olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef]
- Hummel, T.; Kobal, G.; Gudziol, H.; Mackay-Sim, A. Normative data for the “Sniffin’ Sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: An upgrade based on a group of more than 3000 subjects. Eur. Arch. Otorhinolaryngol. 2007, 264, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Oleszkiewicz, A.; Alizadeh, R.; Altundag, A.; Chen, B.; Corrai, A.; Fanari, R.; Farhadi, M.; Gupta, N.; Habel, R.; Hudson, R.; et al. Global study of variability in olfactory sensitivity. Behav. Neurosci. 2020, 134, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Cavazzana, A.; Sanna, F.; Cecchini, M.P.; Zanini, A.; Gasperi, F.; Menghi, L.; Endrizzi, I.; Borgogno, M.; Drago, S.; et al. Correlation between olfactory function, age, sex, and cognitive reserve index in the Italian population. Eur. Arch. Otorhinolaryngol. 2022, 279, 4943–4952. [Google Scholar] [CrossRef]
- Landis, B.N.; Welge-Luessen, A.; Brämerson, A.; Bende, M.; Mueller, C.A.; Nordin, S.; Hummel, T. “Taste Strips”—A rapid, lateralized, gustatory bedside identification test based on impregnated filter papers. J. Neurol. 2009, 256, 242–248. [Google Scholar] [CrossRef]
- Rosa, A.; Putzu, D.; Atzeri, A.; Cesare Marincola, F.; Sarais, G. Sea Salts Flavored with Mediterranean Herbs and Fruits Prevent Cholesterol and Phospholipid Membrane Oxidation and Cell Free Radical Generation. Eur. J. Lipid Sci. Technol. 2018, 120, 1700323. [Google Scholar] [CrossRef]
- Rosa, A.; Isola, R.; Nieddu, M.; Masala, C. The Role of Lipid Composition in the Sensory Attributes and Acceptability of the Salted and Dried Mullet Roes (Bottarga): A Study in Human and Animal Models. Nutrients 2020, 12, 3454. [Google Scholar] [CrossRef] [PubMed]
- Drake, S.L.; Drake, M.A. Comparison of salty taste and time intensity of sea and land salts fromaround the world. J. Sens. Stud. 2011, 26, 25–34. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position paper on olfactory dysfunction. Rhinol. Suppl. 2017, 54, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Gudziol, H.; Rahneberg, K.; Burkert, S. Anosmics are more poorly able to taste than normal persons. Laryngorhinootologie 2007, 86, 640–643. [Google Scholar] [CrossRef] [PubMed]
- Landis, B.N.; Scheibe, M.; Weber, C.; Berger, R.; Brämerson, A.; Bende, M.; Nordin, S.; Hummel, T. Chemosensory interaction: Acquired olfactory impairment is associated with decreased taste function. J. Neurol. 2010, 257, 1303–1308. [Google Scholar] [CrossRef]
- Bathaie, S.Z.; Bolhassani, A.; Tamanoi, F. Anticancer Effect and Molecular Targets of Saffron Carotenoids. Enzyme 2014, 36, 57–86. [Google Scholar]
- Satyal, P.; Jones, T.H.; Lopez, E.M.; McFeeters, R.L.; Ali, N.A.; Mansi, I.; Al-Kaf, A.G.; Setzer, W.N. Chemotypic Characterization and Biological Activity of Rosmarinus officinalis. Foods 2017, 6, 20. [Google Scholar] [CrossRef]
- Rosa, A.; Deiana, M.; Atzeri, A.; Corona, G.; Incani, A.; Melis, M.P.; Appendino, G.; Dessì, M.A. Evaluation of the antioxidant and cytotoxic activity of arzanol, a prenylated alpha-pyrone-phloroglucinol etherodimer from Helichrysum italicum subsp. microphyllum. Chem. Biol. Interact. 2007, 165, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Oka, Y.; Butnaru, M.; von Buchholtz, L.; Ryba, N.J.; Zuker, C.S. High salt recruits aversive taste pathways. Nature 2013, 494, 472–475. [Google Scholar] [CrossRef]
- Embuscado, M.E. Spices and herbs: Natural sources of antioxidants—A mini review. J. Funct. Foods 2015, 18, 811–819. [Google Scholar] [CrossRef]
- Barnett, S.M.; Sablani, S.S.; Tang, J.; Ross, C.F. Utilizing Herbs and Microwave-Assisted Thermal Sterilization to Enhance Saltiness Perception in a Chicken Pasta Meal. J. Food Sci. 2019, 84, 2313–2324. [Google Scholar] [CrossRef] [PubMed]
- Vincis, R.; Fontanini, A. Central taste anatomy and physiology. Handb. Clin. Neurol. 2019, 164, 187–204. [Google Scholar] [PubMed]
- Small, D.M.; Green, B.G. A Proposed Model of a Flavor Modality. In The Neural Bases of Multisensory Processes; Murray, M.M., Wallace, M.T., Eds.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2012. [Google Scholar]
- Thomas-Danguin, T.; Guichard, E.; Salles, C. Cross-modal interactions as a strategy to enhance salty taste and to maintain liking of low-salt food: A review. Food Funct. 2019, 10, 5269–5281. [Google Scholar] [CrossRef]
- Distel, H.; Ayabe-Kanamura, S.; Martínez-Gómez, M.; Schicker, I.; Kobayakawa, T.; Saito, S.; Hudson, R. Perception of Everyday Odors—Correlation between Intensity, Familiarity and Strength of Hedonic Judgement. Chem. Senses 1999, 24, 191–199. [Google Scholar] [CrossRef]
- Maggi, M.A.; Bisti, S.; Picco, C. Saffron: Chemical composition and neuroprotective activity. Molecules 2020, 25, 5618. [Google Scholar] [CrossRef] [PubMed]
- Asadi, M.M.; Shankayi, Z.; Bahrami, F.; Mohammadzadeh, T.; Amini, H.; Naderi, M. Quantitative analysis of taste disorder in COVID-19 patients, the hypersensitivity to salty quality. New Microbes New Infect. 2021, 43, 100919. [Google Scholar] [CrossRef] [PubMed]
- Ercoli, T.; Masala, C.; Pinna, I.; Orofino, G.; Solla, P.; Rocchi, L.; Defazio, G. Qualitative smell/taste disorders as sequelae of acute COVID-19. Neurol. Sci. 2021, 42, 4921–4926. [Google Scholar] [CrossRef] [PubMed]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and taste dysfunction in patients with COVID-19: A systematic review and meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Enache, R.; Sarafoleanu, D. Taste and smell disorders. Rom. J. Rhinol. 2012, 2, 187. [Google Scholar]
- Pepino, M.Y.; Finkbeiner, S.; Beauchamp, G.K.; Mennella, J.A. Obese women have lower monosodium glutamate taste sensitivity and prefer higher concentrations than do normal-weight women. Obesity 2010, 18, 959–965. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Commercial Name | Composition as Indicated on the Labels (100 g of Product) | |
|---|---|---|---|
 | FS 1 | Salt of myrtle | Sardinian sea salt, myrtle essential oil, extract of myrtle (water, berries and leaves of Myrtus communis) (6%) |
 | FS 2 | Salt of Mediterranean herbs and plants | Sardinian sea salt, extract of mixed herbs (helichrysum, rosemary, liquorice, fennel seeds, and myrtle leaves) (15%) |
 | FS 3 | Salt of oranges and saffron | Sardinian sea salt, extract of oranges and saffron (peels and juice of oranges fruits, Crocus sativus) (30%) |
| Parameters | Control (n = 91) | Hyposmia (n = 57) | No-COVID (n = 34) | COVID (n = 23) |
|---|---|---|---|---|
| Mean age | 31.4 ± 13.6 | 35.7 ± 14.8 | 36.3 ± 16.1 | 34.9 ± 13.1 |
| Sex | 62 W/29 M | 35 W/22 M | 21 W/13 M | 14 W/9 M |
| Weight (kg) | 62.9 ± 12.7 | 65.8 ± 16.1 | 63.9 ± 17.7 | 68.6 ± 17.9 |
| Height (m) | 1.6 ± 0.1 | 1.6 ± 0.2 | 1.6 ± 0.1 | 1.6 ± 0.1 |
| BMI | 23.2 ± 3.8 | 23.9 ± 4.8 | 23.3 ± 3.8 | 24.7 ± 5.8 |
| OT | 10.2 ± 4.2 | 3.7 ± 2.3 *** | 3.6 ± 1.9 *** | 3.6 ± 2.6 *** |
| OD | 12.4 ± 1.3 | 10.1 ± 2.5 *** | 10.8 ± 1.8 *** | 9.1 ± 3.1 *** §§ |
| OI | 13.2 ± 1.3 | 11.6 ± 2.1 *** | 11.9 ± 1.4 *** | 11.1 ± 2.7 *** |
| TDI score | 35.8 ± 3.9 | 25.5 ± 4.3 *** | 26.4 ± 2.6 *** | 23.8 ± 5.7 *** § |
| Gustatory Function | TDI Score |
|---|---|
| Sweet | r = 0.243, p < 0.01 |
| Salty | r = 0.285, p < 0.01 |
| Sour | r = 0.321, p < 0.01 |
| Bitter | r = 0.001, p > 0.05 |
| Parameters | Unstandardized Coefficients | Standard Coefficients | |||
|---|---|---|---|---|---|
| B | Std Error | β | t | Significance | |
| Sweet | 0.917 | 0.607 | 0.132 | 1.512 | p > 0.05 |
| Salty | 2.056 | 0.707 | 0.242 | 2.910 | p < 0.01 |
| Sour | 1.733 | 0.525 | 0.274 | 3.300 | p < 0.01 |
| Bitter | −0.613 | 0.467 | −0.109 | −1.312 | p > 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosa, A.; Loy, F.; Pinna, I.; Masala, C. Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia. Nutrients 2022, 14, 4976. https://doi.org/10.3390/nu14234976
Rosa A, Loy F, Pinna I, Masala C. Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia. Nutrients. 2022; 14(23):4976. https://doi.org/10.3390/nu14234976
Chicago/Turabian StyleRosa, Antonella, Francesco Loy, Ilenia Pinna, and Carla Masala. 2022. "Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia" Nutrients 14, no. 23: 4976. https://doi.org/10.3390/nu14234976
APA StyleRosa, A., Loy, F., Pinna, I., & Masala, C. (2022). Role of Aromatic Herbs and Spices in Salty Perception of Patients with Hyposmia. Nutrients, 14(23), 4976. https://doi.org/10.3390/nu14234976