
Factors Associated with Eating in the Absence of Hunger among Children and Adolescents: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
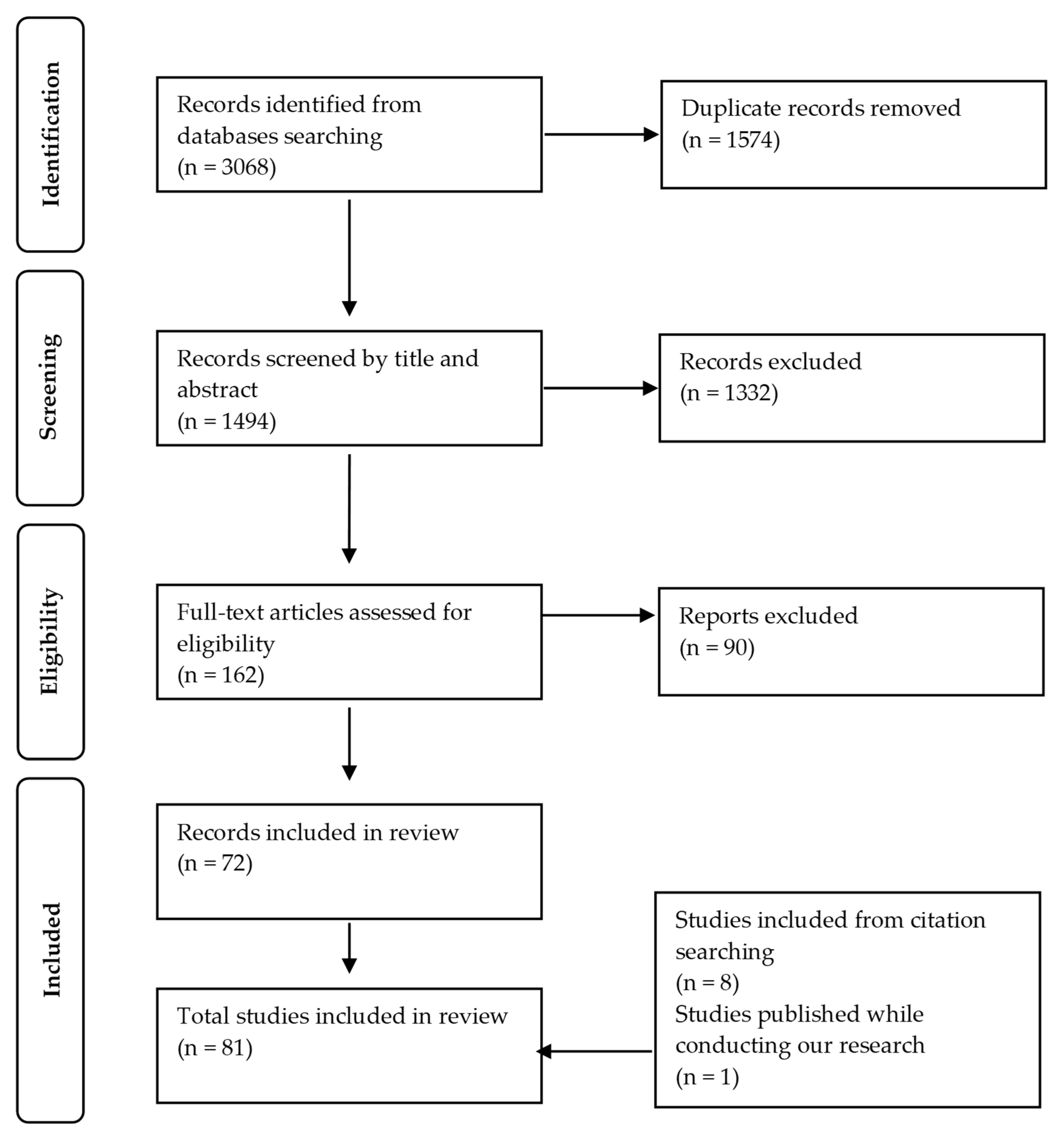
2.3. Screening
2.4. Quality Assessment
2.5. Data Extraction and Synthesis
3. Results
3.1. Study Quality Assessment
3.2. Individual Factors Associated with EAH
3.2.1. Age
3.2.2. Sex/Gender
3.2.3. Adiposity
3.2.4. Exposure to Breastfeeding
3.2.5. In utero Exposure to Maternal Glucose Intolerance
3.2.6. Genetics
3.2.7. Eating Behaviors
3.2.8. Neurobehavioral Measures
3.2.9. Lifestyle Habits
3.2.10. Perceived Sociocultural Pressures and Body Image
3.2.11. Emotional State (Affect)
3.2.12. Brain Activity Measures
3.2.13. Other Individual Factors
3.3. Familial Factors Associated with EAH
3.3.1. Parental Adiposity
3.3.2. Parental Eating Style
3.3.3. Parental Restrictive Feeding Practices
3.3.4. Other Parental Feeding Practices
3.3.5. Parental Demographics
3.3.6. Other Familial Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| EAH | Eating in the absence of hunger |
| kcals | kilocalories |
| EAH-C | EAH questionnaire for children and adolescents |
| EAH-P | parent-report version of the questionnaire |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| U.S. | United States |
| BMI | body mass index |
| GDM | gestational diabetes |
| CEBQ | Children Eating Behavior Questionnaire |
| DEBQ | Dutch Eating Behavior Questionnaire |
| LOC | loss of control |
References
- Fisher, J.O.; Birch, L.L. Restricting access to foods and children’s eating. Appetite 1999, 32, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Lansigan, R.K.; Emond, J.A.; Gilbert-Diamond, D. Understanding eating in the absence of hunger among young children: A systematic review of existing studies. Appetite 2015, 85, 36–47. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Birch, L.L. Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. Am. J. Clin. Nutr. 2002, 76, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Tanofsky-Kraff, M.; Ranzenhofer, L.M.; Yanovski, S.Z.; Schvey, N.A.; Faith, M.; Gustafson, J.; Yanovski, J.A. Psychometric properties of a new questionnaire to assess eating in the absence of hunger in children and adolescents. Appetite 2008, 51, 148–155. [Google Scholar] [CrossRef]
- Madowitz, J.; Liang, J.; Peterson, C.B.; Rydell, S.; Zucker, N.L.; Tanofsky-Kraff, M.; Harnack, L.; Boutelle, K.N. Concurrent and convergent validity of the eating in the absence of hunger questionnaire and behavioral paradigm in overweight children. Int. J. Eat. Disord. 2014, 47, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Shomaker, L.B.; Tanofsky-Kraff, M.; Mooreville, M.; Reina, S.A.; Courville, A.B.; Field, S.E.; Matheson, B.E.; Brady, S.M.; Yanovski, S.Z.; Yanovski, J.A. Links of adolescent- and parent-reported eating in the absence of hunger with observed eating in the absence of hunger. Obesity 2013, 21, 1243–1250. [Google Scholar] [CrossRef]
- WHO. Obesity and Overweight. 9 June 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 17 July 2022).
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.V.; Husby, S.; Skov, L.R.; Perez-Cueto, F.J.A. A systematic review of types of healthy eating interventions in preschools. Nutr. J. 2014, 13, 56. [Google Scholar] [CrossRef]
- Boone-Heinonen, J.; Weeks, H.M.; Sturza, J.; Miller, A.L.; Lumeng, J.C.; Bauer, K.W. Prenatal predictors of objectively measured appetite regulation in low-income toddlers and preschool-age children. Pediatr. Obes. 2019, 14, e12554. [Google Scholar] [CrossRef]
- Fisher, J.O.; Cai, G.; Jaramillo, S.J.; Cole, S.A.; Comuzzie, A.G.; Butte, N.F. Heritability of hyperphagic eating behavior and appetite-related hormones among Hispanic children. Obesity 2007, 15, 1484–1495. [Google Scholar] [CrossRef]
- Hughes, S.O.; Power, T.G.; O’Connor, T.M.; Orlet Fisher, J. Executive functioning, emotion regulation, eating self-regulation, and weight status in low-income preschool children: How do they relate? Appetite 2015, 89, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Power, T.G.; Olivera, Y.A.; Hill, R.A.; Beck, A.D.; Hopwood, V.; Garcia, K.S.; Ramos, G.G.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Emotion regulation strategies and childhood obesity in high risk preschoolers. Appetite 2016, 107, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Silva Garcia, K.; Power, T.G.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Latina mothers’ influences on child appetite regulation. Appetite 2016, 103, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Granger, D.A.; Susman, E.J. Adrenocortical regulation, eating in the absence of hunger and BMI in young children. Appetite 2013, 64, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.; Allison, D.B.; Birch, L.L.; Stallings, V.A.; Moore, R.H.; Faith, M.S. Caloric compensation and eating in the absence of hunger in 5- to 12-y-old weight-discordant siblings. Am. J. Clin. Nutr. 2012, 96, 574–583. [Google Scholar] [CrossRef]
- Gilbert-Diamond, D.; Emond, J.A.; Lansigan, R.K.; Rapuano, K.M.; Kelley, W.M.; Heatherton, T.F.; Sargent, J.D. Television food advertisement exposure and FTO rs9939609 genotype in relation to excess consumption in children. Int. J. Obes. 2017, 41, 23–29. [Google Scholar] [CrossRef]
- Liang, J.; Matheson, B.E.; Rhee, K.E.; Peterson, C.B.; Rydell, S.; Boutelle, K.N. Parental control and overconsumption of snack foods in overweight and obese children. Appetite 2016, 100, 181–188. [Google Scholar] [CrossRef]
- Remy, E.; Issanchou, S.; Chabanet, C.; Boggio, V.; Nicklaus, S. Impact of adiposity, age, sex and maternal feeding practices on eating in the absence of hunger and caloric compensation in preschool children. Int. J. Obes. 2015, 39, 925–930. [Google Scholar] [CrossRef]
- Gill, R.; Chen, Q.; D’Angelo, D.; Chung, W.K. Eating in the absence of hunger but not loss of control behaviors are associated with 16p11.2 deletions. Obesity 2014, 22, 2625–2631. [Google Scholar] [CrossRef]
- Moens, E.; Braet, C. Predictors of disinhibited eating in children with and without overweight. Behav. Res. Ther. 2007, 45, 1357–1368. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O.; Davison, K.K. Learning to overeat: Maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. Am. J. Clin. Nutr. 2003, 78, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Birch, L.L. Maternal weight status modulates the effects of restriction on daughters’ eating and weight. Int. J. Obes. 2005, 29, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Ventura, A.K.; Marini, M.; Birch, L.L. Parent overweight predicts daughters’ increase in BMI and disinhibited overeating from 5 to 13 years. Obesity 2007, 15, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- Shunk, J.A.; Birch, L.L. Girls at risk for overweight at age 5 are at risk for dietary restraint, disinhibited overeating, weight concerns, and greater weight gain from 5 to 9 years. J. Am. Diet. Assoc. 2004, 104, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Galindo, L.; Power, T.G.; Beck, A.D.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Predicting preschool children’s eating in the absence of hunger from maternal pressure to eat: A longitudinal study of low-income, Latina mothers. Appetite 2018, 120, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Rollins, B.Y.; Loken, E.; Savage, J.S.; Birch, L.L. Maternal controlling feeding practices and girls’ inhibitory control interact to predict changes in BMI and eating in the absence of hunger from 5 to 7 y. Am. J. Clin. Nutr. 2014, 99, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Gearhardt, A.N.; Retzloff, L.; Sturza, J.; Kaciroti, N.; Lumeng, J.C. Early Childhood Stress and Child Age Predict Longitudinal Increases in Obesogenic Eating Among Low-Income Children. Acad. Pediatr. 2018, 18, 685–691. [Google Scholar] [CrossRef]
- Schyns, G.; Roefs, A.; Smulders, F.T.Y.; Jansen, A. Cue exposure therapy reduces overeating of exposed and non-exposed foods in obese adolescents. J. Behav. Ther. Exp. Psychiatry 2018, 58, 68–77. [Google Scholar] [CrossRef]
- Annameier, S.K.; Kelly, N.R.; Courville, A.B.; Tanofsky-Kraff, M.; Yanovski, J.A.; Shomaker, L.B. Mindfulness and laboratory eating behavior in adolescent girls at risk for type 2 diabetes. Appetite 2018, 125, 48–56. [Google Scholar] [CrossRef]
- Blanco, E.; Reyes, M.; Burrows, R.; Gahagan, S. Eating in the Absence of Hunger and Obesity Among Adolescents in Santiago, Chile. J. Community Health 2019, 44, 874–880. [Google Scholar] [CrossRef]
- Kelly, N.R.; Shomaker, L.B.; Pickworth, C.K.; Brady, S.M.; Courville, A.B.; Bernstein, S.; Schvey, N.A.; Demidowich, A.P.; Galescu, O.; Yanovski, S.Z.; et al. A prospective study of adolescent eating in the absence of hunger and body mass and fat mass outcomes. Obesity 2015, 23, 1472–1478. [Google Scholar] [CrossRef] [PubMed]
- Kelly, N.R.; Shomaker, L.B.; Pickworth, C.K.; Grygorenko, M.V.; Radin, R.M.; Vannucci, A.; Shank, L.M.; Brady, S.M.; Courville, A.B.; Tanofsky-Kraff, M.; et al. Depressed affect and dietary restraint in adolescent boys’ and girls’ eating in the absence of hunger. Appetite 2015, 91, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Kelly, N.R.; Shomaker, L.B.; Radin, R.M.; Thompson, K.A.; Cassidy, O.L.; Brady, S.; Mehari, R.; Courville, A.B.; Chen, K.Y.; Galescu, O.A.; et al. Associations of sleep duration and quality with disinhibited eating behaviors in adolescent girls at-risk for type 2 diabetes. Eat. Behav. 2016, 22, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.; Moore, R.H.; Stunkard, A.J.; Berkowitz, R.I.; Stettler, N.; Stallings, V.A.; Tanaka, L.M.; Kabay, A.C.; Faith, M.S. Adolescent eating in the absence of hunger and relation to discretionary calorie allowance. J. Am. Diet. Assoc. 2010, 110, 1896–1900. [Google Scholar] [CrossRef] [PubMed]
- Obregón, A.M.; Valladares Vega, M.A.; Goldfield, G.; Llewellyn, C. Genetic variation of the dopamine D2 receptor gene: Association with the reinforcing value of food and eating in the absence of hunger in Chilean children. Nutr. Hosp. 2020, 34, 524–533. [Google Scholar] [CrossRef]
- Radin, R.M.; Shomaker, L.B.; Kelly, N.R.; Pickworth, C.K.; Thompson, K.A.; Brady, S.M.; Demidowich, A.; Galescu, O.; Altschul, A.M.; Shank, L.M.; et al. Cortisol response to an induction of negative affect among adolescents with and without loss of control eating. Pediatr. Obes. 2016, 11, 513–520. [Google Scholar] [CrossRef]
- Reina, S.A.; Shomaker, L.B.; Mooreville, M.; Courville, A.B.; Brady, S.M.; Olsen, C.; Yanovski, S.Z.; Tanofsky-Kraff, M.; Yanovski, J.A. Sociocultural pressures and adolescent eating in the absence of hunger. Body Image 2013, 10, 182–190. [Google Scholar] [CrossRef]
- Shomaker, L.B.; Tanofsky-Kraff, M.; Elliott, C.; Wolkoff, L.E.; Columbo, K.M.; Ranzenhofer, L.M.; Roza, C.A.; Yanovski, S.Z.; Yanovski, J.A. Salience of loss of control for pediatric binge episodes: Does size really matter? Int. J. Eat. Disord. 2010, 43, 707–716. [Google Scholar] [CrossRef]
- Shomaker, L.B.; Tanofsky-Kraff, M.; Zocca, J.M.; Courville, A.; Kozlosky, M.; Columbo, K.M.; Wolkoff, L.E.; Brady, S.M.; Crocker, M.K.; Ali, A.H.; et al. Eating in the absence of hunger in adolescents: Intake after a large-array meal compared with that after a standardized meal. Am. J. Clin. Nutr. 2010, 92, 697–703. [Google Scholar] [CrossRef]
- LeMay-Russell, S.; Tanofsky-Kraff, M.; Schvey, N.A.; Kelly, N.R.; Shank, L.M.; Mi, S.J.; Jaramillo, M.; Ramirez, S.; Altman, D.R.; Rubin, S.G.; et al. Associations of Weekday and Weekend Sleep with Children’s Reported Eating in the Absence of Hunger. Nutrients 2019, 11, 1658. [Google Scholar] [CrossRef]
- Rubin, A.G.; Schvey, N.A.; Shank, L.M.; Altman, D.R.; Swanson, T.N.; Ramirez, E.; Moore, N.A.; Jaramillo, M.; Ramirez, S.; Davis, E.K.; et al. Associations between weight-based teasing and disordered eating behaviors among youth. Eat. Behav. 2021, 41, 101504. [Google Scholar] [CrossRef] [PubMed]
- Shank, L.M.; Tanofsky-Kraff, M.; Kelly, N.R.; Jaramillo, M.; Rubin, S.G.; Altman, D.R.; Byrne, M.E.; LeMay-Russell, S.; Schvey, N.A.; Broadney, M.M.; et al. The association between alexithymia and eating behavior in children and adolescents. Appetite 2019, 142, 104381. [Google Scholar] [CrossRef] [PubMed]
- Pivarunas, B.; Kelly, N.R.; Pickworth, C.K.; Cassidy, O.; Radin, R.M.; Shank, L.M.; Vannucci, A.; Courville, A.B.; Chen, K.Y.; Tanofsky-Kraff, M.; et al. Mindfulness and eating behavior in adolescent girls at risk for type 2 diabetes. Int. J. Eat. Disord. 2015, 48, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Zocca, J.M.; Shomaker, L.B.; Tanofsky-Kraff, M.; Columbo, K.M.; Raciti, G.R.; Brady, S.M.; Crocker, M.K.; Ali, A.H.; Matheson, B.E.; Yanovski, S.Z.; et al. Links between mothers’ and children’s disinhibited eating and children’s adiposity. Appetite 2011, 56, 324–331. [Google Scholar] [CrossRef]
- Reyes, M.; Hoyos, V.; Martinez, S.M.; Lozoff, B.; Castillo, M.; Burrows, R.; Blanco, E.; Gahagan, S. Satiety responsiveness and eating behavior among Chilean adolescents and the role of breastfeeding. Int. J. Obes. 2014, 38, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Derks, I.P.M.; Hivert, M.F.; Rifas-Shiman, S.L.; Gingras, V.; Young, J.G.; Jansen, P.W.; Oken, E. Associations of prenatal exposure to impaired glucose tolerance with eating in the absence of hunger in early adolescence. Int. J. Obes. 2019, 43, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.L.B.; Sauder, K.A.; Tregellas, J.R.; Legget, K.T.; Gravitz, S.L.; Ringham, B.M.; Glueck, D.H.; Johnson, S.L.; Dabelea, D. Exposure to maternal diabetes in utero and offspring eating behavior: The EPOCH study. Appetite 2017, 116, 610–615. [Google Scholar] [CrossRef]
- Savage, J.S.; Adams, E.L.; Rollins, B.Y.; Bleser, J.A.; Marini, M.E. Teaching families to manage intake of candy in the home: Results from a feasibility study using multiphase optimization strategy (MOST). Obes. Sci. Pract. 2020, 6, 649–659. [Google Scholar] [CrossRef]
- Adise, S.; Geier, C.F.; Roberts, N.J.; White, C.N.; Keller, K.L. Is brain response to food rewards related to overeating? A test of the reward surfeit model of overeating in children. Appetite 2018, 128, 167–179. [Google Scholar] [CrossRef]
- Boots, S.B.; Tiggemann, M.; Corsini, N. Eating in the absence of hunger in young children: The role of maternal feeding strategies. Appetite 2018, 130, 45–49. [Google Scholar] [CrossRef]
- Fogel, A.; McCrickerd, K.; Goh, A.T.; Fries, L.R.; Chong, Y.S.; Tan, K.H.; Yap, F.; Shek, L.P.; Meaney, M.J.; Cai, S.; et al. Associations between inhibitory control, eating behaviours and adiposity in 6-year-old children. Int. J. Obes. 2019, 43, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Llewellyn, C.H.; Saxton, J.; Webber, L.; Semmler, C.; Carnell, S.; van Jaarsveld, C.H.; Boniface, D.; Wardle, J. Adiposity and ‘eating in the absence of hunger’ in children. Int. J. Obes. 2008, 32, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.E.; Moore, R.H.; Chittams, J.; O’Malley, L.; Jones, E.; Quinn, R.J.; Fisher, J.O. Does eating in the absence of hunger extend to healthy snacks in children? Pediatr. Obes. 2020, 15, e12659. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.; Mallan, K.M.; Nambiar, S.; Daniels, L.A. The relationship between controlling feeding practices and boys’ and girls’ eating in the absence of hunger. Eat. Behav. 2014, 15, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Cutting, T.M.; Fisher, J.O.; Grimm-Thomas, K.; Birch, L.L. Like mother, like daughter: Familial patterns of overweight are mediated by mothers’ dietary disinhibition. Am. J. Clin. Nutr. 1999, 69, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Mallan, K.M.; Nambiar, S.; Magarey, A.M.; Daniels, L.A. Satiety responsiveness in toddlerhood predicts energy intake and weight status at four years of age. Appetite 2014, 74, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Obregón, A.M.; Valladares, M.; Goldfield, G. Association of the dopamine D2 receptor rs1800497 polymorphism and eating behavior in Chilean children. Nutrition 2017, 35, 139–145. [Google Scholar] [CrossRef]
- Obregón Rivas, A.M.; Santos, J.L.; Valladares, M.A.; Cameron, J.; Goldfield, G. Association of the FTO fat mass and obesity-associated gene rs9939609 polymorphism with rewarding value of food and eating behavior in Chilean children. Nutrition 2018, 54, 105–110. [Google Scholar] [CrossRef]
- Gearhardt, A.N.; Miller, A.L.; Sturza, J.; Epstein, L.H.; Kaciroti, N.; Lumeng, J.C. Behavioral Associations with Overweight in Low-Income Children. Obesity 2017, 25, 2123–2127. [Google Scholar] [CrossRef]
- Miller, A.L.; Riley, H.; Domoff, S.E.; Gearhardt, A.N.; Sturza, J.; Kaciroti, N.; Lumeng, J.C. Weight status moderates stress-eating in the absence of hunger associations in children. Appetite 2019, 136, 184–192. [Google Scholar] [CrossRef]
- Balantekin, K.N.; Birch, L.L.; Savage, J.S. Eating in the absence of hunger during childhood predicts self-reported binge eating in adolescence. Eat. Behav. 2017, 24, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Mestre, Z.L.; Bischoff-Grethe, A.; Eichen, D.M.; Wierenga, C.E.; Strong, D.; Boutelle, K.N. Hippocampal atrophy and altered brain responses to pleasant tastes among obese compared with healthy weight children. Int. J. Obes. 2017, 41, 1496–1502. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, K.N.; Wierenga, C.E.; Bischoff-Grethe, A.; Melrose, A.J.; Grenesko-Stevens, E.; Paulus, M.P.; Kaye, W.H. Increased brain response to appetitive tastes in the insula and amygdala in obese compared with healthy weight children when sated. Int. J. Obes. 2015, 39, 620–628. [Google Scholar] [CrossRef]
- Fogel, A.; McCrickerd, K.; Fries, L.R.; Goh, A.T.; Quah, P.L.; Chan, M.J.; Toh, J.Y.; Chong, Y.S.; Tan, K.H.; Yap, F.; et al. Eating in the absence of hunger: Stability over time and associations with eating behaviours and body composition in children. Physiol. Behav. 2018, 192, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Farrow, C.V.; Haycraft, E.; Blissett, J.M. Teaching our children when to eat: How parental feeding practices inform the development of emotional eating--a longitudinal experimental design. Am. J. Clin. Nutr. 2015, 101, 908–913. [Google Scholar] [CrossRef] [PubMed]
- Pang, W.W.; McCrickerd, K.; Quah, P.L.; Fogel, A.; Aris, I.M.; Yuan, W.L.; Fok, D.; Chua, M.C.; Lim, S.B.; Shek, L.P.; et al. Is breastfeeding associated with later child eating behaviours? Appetite 2020, 150, 104653. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Llewellyn, C.; Sanderson, S.; Plomin, R. The FTO gene and measured food intake in children. Int. J. Obes. 2009, 33, 42–45. [Google Scholar] [CrossRef]
- Ho-Urriola, J.; Guzmán-Guzmán, I.P.; Smalley, S.V.; González, A.; Weisstaub, G.; Domínguez-Vásquez, P.; Valladares, M.; Amador, P.; Hodgson, M.I.; Obregón, A.M.; et al. Melanocortin-4 receptor polymorphism rs17782313: Association with obesity and eating in the absence of hunger in Chilean children. Nutrition 2014, 30, 145–149. [Google Scholar] [CrossRef]
- Obregón, A.M.; Oyarce, K.; Santos, J.L.; Valladares, M.; Goldfield, G. Association of the melanocortin 4 receptor gene rs17782313 polymorphism with rewarding value of food and eating behavior in Chilean children. J. Physiol. Biochem. 2017, 73, 29–35. [Google Scholar] [CrossRef]
- Giuliani, N.R.; Kelly, N.R. Delay of Gratification Predicts Eating in the Absence of Hunger in Preschool-Aged Children. Front. Psychol. 2021, 12, 650046. [Google Scholar] [CrossRef]
- Fisher, J.O.; Birch, L.L. Parents’ restrictive feeding practices are associated with young girls’ negative self-evaluation of eating. J. Am. Diet. Assoc. 2000, 100, 1341–1346. [Google Scholar] [CrossRef]
- Orlet Fisher, J.; Rolls, B.J.; Birch, L.L. Children’s bite size and intake of an entrée are greater with large portions than with age-appropriate or self-selected portions. Am. J. Clin. Nutr. 2003, 77, 1164–1170. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.Y.; Lumeng, J.C.; Kaciroti, N.A.; Chen, Y.P.; Rosenblum, K.; Miller, A.L. Surgency and negative affectivity, but not effortful control, are uniquely associated with obesogenic eating behaviors among low-income preschoolers. Appetite 2014, 78, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Morrison, S.; Galland, B.C.; Haszard, J.J.; Jackson, R.; McIntosh, D.R.; Beebe, D.W.; Elder, D.E.; Ward, A.L.; Meredith-Jones, K.; Taylor, R.W. Eating in the absence of hunger in children with mild sleep loss: A randomized crossover trial with learning effects. Am. J. Clin. Nutr. 2021, 114, 1428–1437. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Haycraft, E.; Farrow, C. Inducing preschool children’s emotional eating: Relations with parental feeding practices. Am. J. Clin. Nutr. 2010, 92, 359–365. [Google Scholar] [CrossRef]
- Shapiro, A.L.B.; Johnson, S.L.; Sutton, B.; Legget, K.T.; Dabelea, D.; Tregellas, J.R. Eating in the absence of hunger in young children is related to brain reward network hyperactivity and reduced functional connectivity in executive control networks. Pediatr. Obes. 2019, 14, e12502. [Google Scholar] [CrossRef]
- Faith, M.S.; Berkowitz, R.I.; Stallings, V.A.; Kerns, J.; Storey, M.; Stunkard, A.J. Eating in the absence of hunger: A genetic marker for childhood obesity in prepubertal boys? Obesity 2006, 14, 131–138. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.; Sanderson, S.; Birch, L.; Plomin, R. Food and activity preferences in children of lean and obese parents. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 971–977. [Google Scholar] [CrossRef]
- Warkentin, S.; Mais, L.A.; Ranganath, K.; Jansen, E.; Carnell, S. Controlling and less controlling feeding practices are differentially associated with child food intake and appetitive behaviors assessed in a school environment. Pediatr. Obes. 2020, 15, e12714. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Mothers’ child-feeding practices influence daughters’ eating and weight. Am. J. Clin. Nutr. 2000, 71, 1054–1061. [Google Scholar] [CrossRef]
- Kral, T.V.E.; Chittams, J.; Moore, R.H. Relationship between food insecurity, child weight status, and parent-reported child eating and snacking behaviors. J. Spec. Pediatr. Nurs. 2017, 22, e12177. [Google Scholar] [CrossRef] [PubMed]
- Fogel, A.; McCrickerd, K.; Aris, I.M.; Goh, A.T.; Chong, Y.S.; Tan, K.H.; Yap, F.; Shek, L.P.; Meaney, M.J.; Broekman, B.F.P.; et al. Eating behaviors moderate the associations between risk factors in the first 1000 days and adiposity outcomes at 6 years of age. Am. J. Clin. Nutr. 2020, 111, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and environmental influences on adolescent eating behaviors. J. Am. Diet. Assoc. 2002, 102, S40–S51. [Google Scholar] [CrossRef]
- Kininmonth, A.; Smith, A.; Carnell, S.; Steinsbekk, S.; Fildes, A.; Llewellyn, C. The association between childhood adiposity and appetite assessed using the Child Eating Behavior Questionnaire and Baby Eating Behavior Questionnaire: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13169. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, U.; Weisstaub, G.; Santos, J.L.; Corvalán, C.; Uauy, R. GOCS cohort: Children’s eating behavior scores and BMI. Eur. J. Clin. Nutr. 2016, 70, 925–928. [Google Scholar] [CrossRef]
- Müller, M.J.; Mast, M.; Asbeck, I.; Langnäse, K.; Grund, A. Prevention of obesity--is it possible? Obes. Rev. 2001, 2, 15–28. [Google Scholar] [CrossRef]
- Dehghan, M.; Akhtar-Danesh, N.; Merchant, A.T. Childhood obesity, prevalence and prevention. Nutr. J. 2005, 4, 24. [Google Scholar] [CrossRef]
- Saavedra, J.M.; Deming, D.; Dattilo, A.; Reidy, K. Lessons from the feeding infants and toddlers study in North America: What children eat, and implications for obesity prevention. Ann. Nutr. Metab. 2013, 62 (Suppl. S3), 27–36. [Google Scholar] [CrossRef]
- Disantis, K.I.; Collins, B.N.; Fisher, J.O.; Davey, A. Do infants fed directly from the breast have improved appetite regulation and slower growth during early childhood compared with infants fed from a bottle? Int. J. Behav. Nutr. Phys. Act. 2011, 8, 89. [Google Scholar] [CrossRef]
- Ergang, B.C.; da Silva, C.H.; Goldani, M.Z.; Hagen, M.E.K.; Bernardi, J.R. Is the duration of breastfeeding associated with eating behavior in early childhood? Physiol. Behav. 2021, 242, 113607. [Google Scholar] [CrossRef]
- Yelverton, C.A.; Geraghty, A.A.; O’Brien, E.C.; Killeen, S.L.; Horan, M.K.; Donnelly, J.M.; Larkin, E.; Mehegan, J.; McAuliffe, F.M. Breastfeeding and maternal eating behaviours are associated with child eating behaviours: Findings from the ROLO Kids Study. Eur. J. Clin. Nutr. 2021, 75, 670–679. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Lee, M. Breastfeeding during the first year promotes satiety responsiveness in children aged 18-24 months. Pediatr. Obes. 2012, 7, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Mazzantini, S.; Zuccotti, G.V. Nutrition in the First 1000 Days: The Origin of Childhood Obesity. Int. J. Environ. Res. Public Health 2016, 13, 838. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Qiao, Y.; Zhao, P.; Li, W.; Katzmarzyk, P.T.; Chaput, J.P.; Fogelholm, M.; Kuriyan, R.; Lambert, E.V.; Maher, C.; et al. Breastfeeding and childhood obesity: A 12-country study. Matern. Child Nutr. 2020, 16, e12984. [Google Scholar] [CrossRef] [PubMed]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Zeggini, E.; Freathy, R.M.; Lindgren, C.M.; Perry, J.R.; Elliott, K.S.; Lango, H.; Rayner, N.W.; et al. A common variant in the FTO gene is associated with body mass index and predisposes to childhood and adult obesity. Science 2007, 316, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, K.N.; Zucker, N.; Peterson, C.B.; Rydell, S.; Carlson, J.; Harnack, L.J. An intervention based on Schachter’s externality theory for overweight children: The regulation of cues pilot. J. Pediatr. Psychol. 2014, 39, 405–417. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Zucker, N.L.; Peterson, C.B.; Rydell, S.A.; Cafri, G.; Harnack, L. Two novel treatments to reduce overeating in overweight children: A randomized controlled trial. J. Consult. Clin. Psychol. 2011, 79, 759–771. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Kuckertz, J.M.; Carlson, J.; Amir, N. A pilot study evaluating a one-session attention modification training to decrease overeating in obese children. Appetite 2014, 76, 180–185. [Google Scholar] [CrossRef]
- Lee, R.E.; Parker, N.H.; Soltero, E.G.; Ledoux, T.A.; Mama, S.K.; McNeill, L. Sustainability via Active Garden Education (SAGE): Results from two feasibility pilot studies. BMC Public Health 2017, 17, 242. [Google Scholar] [CrossRef]
- Rhee, K.E.; Kessl, S.; Manzano, M.A.; Strong, D.R.; Boutelle, K.N. Cluster randomized control trial promoting child self-regulation around energy-dense food. Appetite 2019, 133, 156–165. [Google Scholar] [CrossRef]


{kind=link}
| Individual Factors | In Childhood (≤12 Years Old) | In Adolescence (>12 Years Old) |
|---|---|---|
| Age |
|
|
| Sex |
|
|
| Adiposity |
|
|
| Exposure to breastfeeding |
|
|
| In utero exposure to maternal glucose intolerance | – |
|
| Genetics |
| – |
| Eating behaviors |
|
|
| Neurobehavioral measures |
|
|
| Lifestyle habits |
|
|
| Sociocultural pressures and body image | – |
|
| Emotional state (affect) |
|
|
| Brain activity measures |
| – |
| Other individual factors |
|
|
| Familial Factors | In Childhood (≤12 Years Old) | In Adolescence (>12 Years Old) |
|---|---|---|
| Parental adiposity |
|
|
| Parental eating style |
|
|
| Parental restrictive feeding practices |
|
|
| Other parental feeding practices |
|
|
| Parental demographics |
| – |
| Other familial factors |
| – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savard, C.; Bégin, S.; Gingras, V. Factors Associated with Eating in the Absence of Hunger among Children and Adolescents: A Systematic Review. Nutrients 2022, 14, 4715. https://doi.org/10.3390/nu14224715
Savard C, Bégin S, Gingras V. Factors Associated with Eating in the Absence of Hunger among Children and Adolescents: A Systematic Review. Nutrients. 2022; 14(22):4715. https://doi.org/10.3390/nu14224715
Chicago/Turabian StyleSavard, Catherine, Stéphanie Bégin, and Véronique Gingras. 2022. "Factors Associated with Eating in the Absence of Hunger among Children and Adolescents: A Systematic Review" Nutrients 14, no. 22: 4715. https://doi.org/10.3390/nu14224715
APA StyleSavard, C., Bégin, S., & Gingras, V. (2022). Factors Associated with Eating in the Absence of Hunger among Children and Adolescents: A Systematic Review. Nutrients, 14(22), 4715. https://doi.org/10.3390/nu14224715