
The Association of Dietary Magnesium and Prediabetes in Childbearing Chinese Women: Results from China Nutrition and Health Surveillance (2015–2017)

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
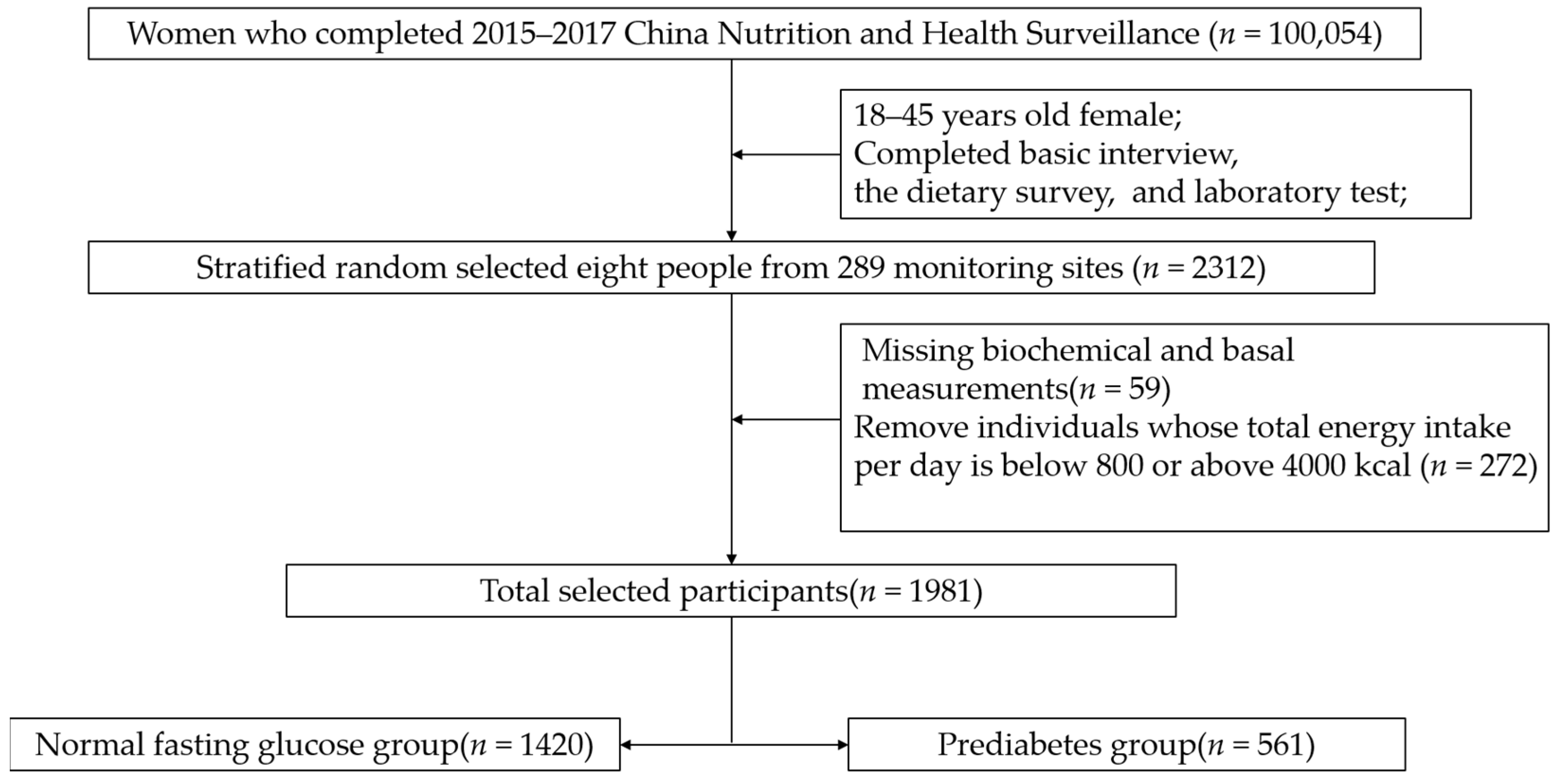
2.1. Subjects
2.2. Data Collection and Variable Classifications
2.3. Laboratory Measurements
2.4. Definition of Prediabetes
2.5. Dietary and Nutrients Intake Assessment
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Clinical Characteristics of NFG and Prediabetes Group Participants
3.3. Mean Daily Nutrients Intake (Energy-Adjusted)
3.4. The Association between Dietary Magnesium and Prediabetes
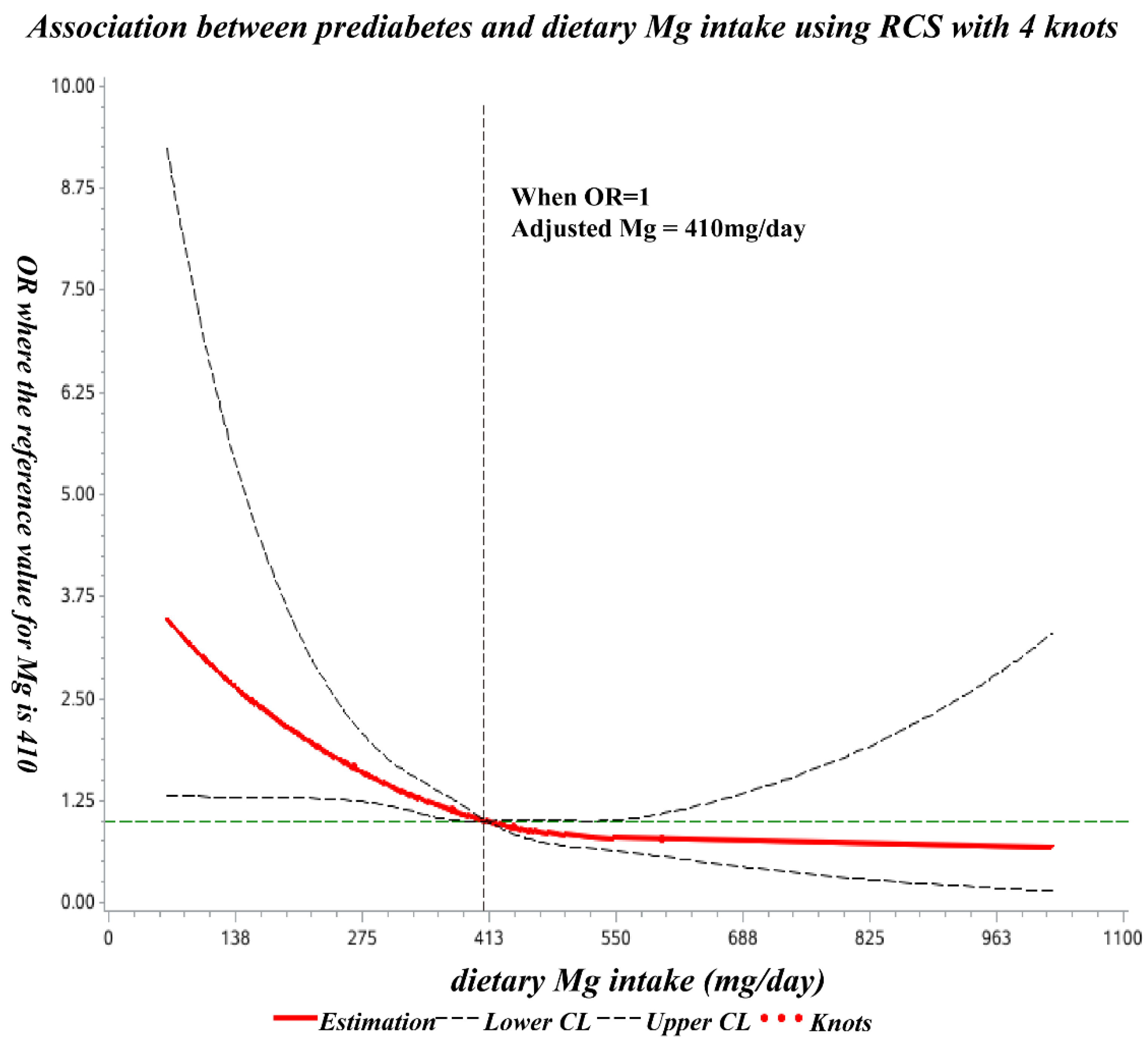
3.5. The Dose-Response Relationship between Dietary Mg Intake and Prediabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, L.; Peng, W.; Zhao, Z.; Zhang, M.; Shi, Z.; Song, Z.; Zhang, X.; Li, C.; Huang, Z.; Sun, X.; et al. Prevalence and Treatment of Diabetes in China, 2013-2018. JAMA 2021, 326, 2498–2506. [Google Scholar] [CrossRef] [PubMed]
- Tabák, A.G.; Herder, C.; Rathmann, W.; Brunner, E.J.; Kivimäki, M. Prediabetes: A high-risk state for diabetes development. Lancet 2012, 379, 2279–2290. [Google Scholar] [CrossRef]
- Brannick, B.; Dagogo-Jack, S. Prediabetes and Cardiovascular Disease: Pathophysiology and Interventions for Prevention and Risk Reduction. Endocrinol. Metab. Clin. N. Am. 2018, 47, 33–50. [Google Scholar] [CrossRef] [PubMed]
- Sales, C.H.; Pedrosa, L.F.; Lima, J.G.; Lemos, T.M.; Colli, C. Influence of magnesium status and magnesium intake on the blood glucose control in patients with type 2 diabetes. Clin. Nutr. 2011, 30, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi Mousavi, S.; Ghoreishy, S.M.; Hemmati, A.; Mohammadi, H. Association between magnesium concentrations and prediabetes: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 24388. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Jin, X.; Liu, J.; Sun, T.; Xie, M.; Bao, W.; Yu, X.; Yang, X.; Zhang, Y.; Zhang, H.; et al. Association of Plasma Magnesium with Prediabetes and Type 2 Diabetes Mellitus in Adults. Sci. Rep. 2017, 7, 12763. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Wang, X.; Wu, W.; Gu, X.; Ye, T.; Deng, H.; Wang, X.; Shen, F. Association of Serum Magnesium Level with Odds of Prediabetes and Diabetes in a Southern Chinese Population: A Prospective Nested Case-Control Study. Biol. Trace Elem. Res. 2016, 172, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Hruby, A.; Meigs, J.B.; O’Donnell, C.J.; Jacques, P.F.; McKeown, N.M. Higher magnesium intake reduces risk of impaired glucose and insulin metabolism and progression from prediabetes to diabetes in middle-aged americans. Diabetes Care 2014, 37, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Akizawa, Y.; Koizumi, S.; Itokawa, Y.; Ojima, T.; Nakamura, Y.; Tamura, T.; Kusaka, Y. Daily magnesium intake and serum magnesium concentration among Japanese people. J. Epidemiol. 2008, 18, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; Hernández-Ronquillo, G.; Rodriguez-Morán, M. Oral magnesium supplementation improves glycaemic status in subjects with prediabetes and hypomagnesaemia: A double-blind placebo-controlled randomized trial. Diabetes Metab. 2015, 41, 202–207. [Google Scholar] [CrossRef]
- Jiao, Y.; Li, W.; Wang, L.; Jiang, H.; Wang, S.; Jia, X.; Wang, Z.; Wang, H.; Zhang, B.; Ding, G. Relationship between Dietary Magnesium Intake and Metabolic Syndrome. Nutrients 2022, 14, 2013. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Sun, Q.; Curhan, G.C.; Taylor, E.N.; Spiegelman, D.; Willett, W.C.; Manson, J.E.; Rexrode, K.M.; Albert, C.M. Dietary and plasma magnesium and risk of coronary heart disease among women. J. Am. Heart Assoc. 2013, 2, e000114. [Google Scholar] [CrossRef]
- Sales, C.H.; Pedrosa Lde, F. Magnesium and diabetes mellitus: Their relation. Clin. Nutr. 2006, 25, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D.; Joshi, S.; Shaw, J. Hypomagnesaemia is associated with diabetes: Not pre-diabetes, obesity or the metabolic syndrome. Diabetes Res. Clin. Pract. 2010, 87, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhao, L.; Zhang, J.; Yang, Z.; Yang, L.; Huang, J.; Fang, H.; Guo, Q.; Xu, X.; Ju, L.; et al. China Nutrition and Health Surveys (1982–2017). China CDC Wkly. 2021, 3, 193–195. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S17–S38. [Google Scholar] [CrossRef]
- Liu, D.; He, L.; Zhang, X.; Zhai, Y.; Zhang, J.; Yang, X.; Chen, J.; Zhao, W. Establishment and application of food frequency questionnaire method among Chinese. Wei Sheng Yan Jiu J. Hyg. Res. 2018, 47, 744–755. [Google Scholar]
- Yang, Y.X. China Food Composition Tables, Standard Edition; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S, discussion 1229S–1231S. [Google Scholar] [CrossRef]
- Desquilbet, L.; Mariotti, F. Dose-response analyses using restricted cubic spline functions in public health research. Stat. Med. 2010, 29, 1037–1057. [Google Scholar] [CrossRef]
- Mirmiran, P.; Shab-Bidar, S.; Hosseini-Esfahani, F.; Asghari, G.; Hosseinpour-Niazi, S.; Azizi, F. Magnesium intake and prevalence of metabolic syndrome in adults: Tehran Lipid and Glucose Study. Public Health Nutr. 2012, 15, 693–701. [Google Scholar] [CrossRef]
- Li, W.; Zhu, X.; Song, Y.; Fan, L.; Wu, L.; Kabagambe, E.K.; Hou, L.; Shrubsole, M.J.; Liu, J.; Dai, Q. Intakes of magnesium, calcium and risk of fatty liver disease and prediabetes. Public Health Nutr. 2018, 21, 2088–2095. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Flores-García, A.; Saldaña-Guerrero, S.; Simental-Mendía, L.E.; Rodríguez-Morán, M. Obesity and hypomagnesemia. Eur. J. Intern. Med. 2016, 34, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Fiorentini, D.; Cappadone, C.; Farruggia, G.; Prata, C. Magnesium: Biochemistry, Nutrition, Detection, and Social Impact of Diseases Linked to Its Deficiency. Nutrients 2021, 13, 1136. [Google Scholar] [CrossRef]
- Glasdam, S.M.; Glasdam, S.; Peters, G.H. The Importance of Magnesium in the Human Body: A Systematic Literature Review. Adv. Clin. Chem. 2016, 73, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Castellanos-Gutiérrez, A.; Sánchez-Pimienta, T.G.; Carriquiry, A.; da Costa, T.H.M.; Ariza, A.C. Higher dietary magnesium intake is associated with lower body mass index, waist circumference and serum glucose in Mexican adults. Nutr. J. 2018, 17, 114. [Google Scholar] [CrossRef]
- Brandão-Lima, P.N.; Carvalho, G.B.; Santos, R.K.F.; Santos, B.D.C.; Dias-Vasconcelos, N.L.; Rocha, V.S.; Barbosa, K.B.F.; Pires, L.V. Intakes of Zinc, Potassium, Calcium, and Magnesium of Individuals with Type 2 Diabetes Mellitus and the Relationship with Glycemic Control. Nutrients 2018, 10, 1948. [Google Scholar] [CrossRef]
- Fang, X.; Han, H.; Li, M.; Liang, C.; Fan, Z.; Aaseth, J.; He, J.; Montgomery, S.; Cao, Y. Dose-Response Relationship between Dietary Magnesium Intake and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Regression Analysis of Prospective Cohort Studies. Nutrients 2016, 8, 739. [Google Scholar] [CrossRef]
- Xu, T.; Chen, G.C.; Zhai, L.; Ke, K.F. Nonlinear Reduction in Risk for Type 2 Diabetes by Magnesium Intake: An Updated Meta-Analysis of Prospective Cohort Studies. Biomed. Environ. Sci. 2015, 28, 527–534. [Google Scholar] [CrossRef]
- Ma, B.; Lawson, A.B.; Liese, A.D.; Bell, R.A.; Mayer-Davis, E.J. Dairy, magnesium, and calcium intake in relation to insulin sensitivity: Approaches to modeling a dose-dependent association. Am. J. Epidemiol. 2006, 164, 449–458. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rascón-Pacheco, R.A.; Rodríguez-Morán, M.; de la Peña, J.E.; Wacher, N. Hypomagnesaemia and risk for metabolic glucose disorders: A 10-year follow-up study. Eur. J. Clin. Investig. 2008, 38, 389–396. [Google Scholar] [CrossRef]
- Villegas, R.; Gao, Y.T.; Dai, Q.; Yang, G.; Cai, H.; Li, H.; Zheng, W.; Shu, X.O. Dietary calcium and magnesium intakes and the risk of type 2 diabetes: The Shanghai Women’s Health Study. Am. J. Clin. Nutr. 2009, 89, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Manson, J.E.; Buring, J.E.; Liu, S. Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 2004, 27, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Hu, F.B. Primary prevention of diabetes: What can be done and how much can be prevented? Annu. Rev. Public Health 2005, 26, 445–467. [Google Scholar] [CrossRef] [PubMed]
- Cruz, K.J.; de Oliveira, A.R.; Pinto, D.P.; Morais, J.B.; Lima Fda, S.; Colli, C.; Torres-Leal, F.L.; Marreiro, D.d.N. Influence of magnesium on insulin resistance in obese women. Biol. Trace Elem. Res. 2014, 160, 305–310. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total (n = 1981) | NFG (n = 1420) | Prediabetes (n = 561) | p-Value |
|---|---|---|---|---|
| Mean ± SD/n | Mean ± SD/n (%) | Mean ± SD/n (%) | ||
| Age(years) | 32.4 ± 7.8 | 30.9 ± 7.5 | 36.4 ± 6.9 | <0.001 |
| Age group | <0.001 | |||
| 18–<26 | 551 | 494 (34.80%) | 57 (10.20%) | |
| 26–<36 | 671 | 498 (35.10%) | 173 (30.80%) | |
| 36–<45 | 759 | 428 (30.10%) | 331 (59.00%) | |
| BMI (kg/m2) | 23.59 ± 3.79 | 22.88 ± 3.53 | 25.38 ± 3.83 | <0.001 |
| BMI Group | <0.001 | |||
| <18.5 | 134 | 125 (8.80%) | 9 (1.60%) | |
| 18.5–<24 | 1053 | 844 (59.40%) | 209 (37.30%) | |
| 24–<28 | 530 | 317 (22.30%) | 213 (38.00%) | |
| 28- | 264 | 134 (9.40%) | 130 (23.20%) | |
| Nationality | 0.626 | |||
| Han | 1745 | 1254 (88.30%) | 491 (87.50%) | |
| Ethnic minorities | 236 | 166 (11.70%) | 70 (12.50%) | |
| Education | <0.001 | |||
| Primary | 562 | 335 (23.60%) | 227 (40.50%) | |
| Medium | 1120 | 834 (58.70%) | 286 (51.00%) | |
| Advanced | 299 | 251 (17.70%) | 48 (8.60%) | |
| District | 0.034 | |||
| Eastern | 651 | 459 (32.30%) | 192 (34.20%) | |
| Central | 668 | 503 (35.40%) | 165 (29.40%) | |
| Western | 662 | 458 (32.30%) | 204 (36.40%) | |
| Residences | <0.001 | |||
| City | 905 | 604 (42.50%) | 301 (53.70%) | |
| Rural area | 1076 | 816 (57.50%) | 260 (46.30%) | |
| Smoke | 0.202 | |||
| yes | 24 | 20 (1.40%) | 4 (0.70%) | |
| no | 1957 | 1400 (98.60%) | 557 (99.30%) | |
| Drink | 0.374 | |||
| yes | 414 | 304 (21.40%) | 110 (19.60%) | |
| no | 1567 | 1116 (78.60%) | 451 (80.40%) |
| Index | Total (n = 1981) | NFG (n = 1420) | Prediabetes (n = 561) | p-Value |
|---|---|---|---|---|
| SBP (mmHg) | 118.89 ± 15.03 | 116.17 ± 13.45 | 125.76 ± 16.58 | <0.001 |
| DBP (mmHg) | 72.85 ± 9.92 | 71.29 ± 9.13 | 76.79 ± 10.71 | <0.001 |
| Waist (cm) | 77.84 ± 9.82 | 76.14 ± 9.34 | 82.14 ± 9.70 | <0.001 |
| Height (cm) | 156.98 ± 6.16 | 157.27 ± 6.15 | 156.27 ± 6.16 | <0.001 |
| Weight (kg) | 58.19 ± 10.3 | 56.67 ± 9.81 | 62.04 ± 10.51 | <0.001 |
| TG (mmol/L) | 1.20 ± 0.90 | 1.07 ± 0.74 | 1.54 ± 1.16 | <0.001 |
| TC (mmol/L) | 4.38 ± 0.88 | 4.26 ± 0.83 | 4.68 ± 0.93 | <0.001 |
| LDL-C (mmol/L) | 2.62 ± 0.77 | 2.51 ± 0.73 | 2.92 ± 0.81 | <0.001 |
| HDL-C (mmol/L) | 1.30 ± 0.30 | 1.32 ± 0.29 | 1.25 ± 0.31 | <0.001 |
| UA (µmol/L) | 265.16 ± 68.74 | 260.45 ± 66.16 | 277.08 ± 73.59 | <0.001 |
| FPG (mmol/L) | 5.21 ± 0.80 | 4.79 ± 0.45 | 6.28 ± 0.39 | <0.001 |
| HbA1c (%) | 4.79 ± 0.52 | 4.69 ± 0.46 | 5.03 ± 0.60 | <0.001 |
| Mg (mmol/L) | 0.87 ± 0.08 | 0.88 ± 0.08 | 0.86 ± 0.09 | <0.001 |
| Nutrients | Total (n = 1981) | NFG (n = 1420) | Prediabetes (n = 561) | p-Value |
|---|---|---|---|---|
| Energy(kcal) | 1955.85 ± 749.68 | 1939.24 ± 752.84 | 1997.89 ± 740.62 | 0.117 |
| Protein(g) | 60.03 ± 15.98 | 60.36 ± 16.37 | 59.18 ± 14.92 | 0.138 |
| Fat(g) | 25.78 ± 20.32 | 26.11 ± 20.50 | 24.95 ± 19.85 | 0.256 |
| Carbohydrate(g) | 413.19 ± 66.84 | 414.39 ± 68.34 | 410.16 ± 62.85 | 0.205 |
| Calcium(mg) | 372.01 ± 285.81 | 381.17 ± 292.46 | 348.84 ± 267.10 | 0.023 |
| Magnesium(mg) | 413.66 ± 102.12 | 419.21 ± 102.01 | 399.61 ± 101.15 | <0.001 |
| Ca/Mg ratio | 0.91 ± 0.68 | 0.91 ± 0.67 | 0.89 ± 0.73 | 0.552 |
| Model | β (Per 100 mg of Mg Intake) | 95%CI | p-Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Model 1 | −0.056 | −0.090 | −0.021 | 0.001 |
| Model 2 | −0.049 | −0.082 | −0.016 | 0.004 |
| Model 3 | −0.052 | −0.085 | −0.019 | 0.002 |
| Model | Q1 | Q2 | Q3 | Q4 | p-Value |
|---|---|---|---|---|---|
| <350.10 | 350.10–<405.41 | 405.41–<466.80 | >466.89 | ||
| (NFG/Prediabetes) | (332/163) | (343/153) | (378/117) | (367/128) | - |
| Model 1 | 1 (ref) | 0.91 (0.70,1.19) | 0.63 (0.48,0.83) | 0.71 (0.54,0.94) | 0.016 |
| Model 2 | 1 (ref) | 0.85 (0.63,1.13) | 0.63 (0.46,0.85) | 0.71 (0.52,0.96) | 0.004 |
| Model 3 | 1 (ref) | 0.81 (0.60,1.11) | 0.63 (0.46,0.88) | 0.64 (0.46,0.90) | 0.020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Zhang, H.; Cao, Y.; Shan, X.; Feng, J.; Lu, J.; Cai, S.; Zhao, L.; Yang, L. The Association of Dietary Magnesium and Prediabetes in Childbearing Chinese Women: Results from China Nutrition and Health Surveillance (2015–2017). Nutrients 2022, 14, 4580. https://doi.org/10.3390/nu14214580
Yang J, Zhang H, Cao Y, Shan X, Feng J, Lu J, Cai S, Zhao L, Yang L. The Association of Dietary Magnesium and Prediabetes in Childbearing Chinese Women: Results from China Nutrition and Health Surveillance (2015–2017). Nutrients. 2022; 14(21):4580. https://doi.org/10.3390/nu14214580
Chicago/Turabian StyleYang, Jingxin, Huidi Zhang, Yang Cao, Xiaoyun Shan, Jie Feng, Jiaxi Lu, Shuya Cai, Liyun Zhao, and Lichen Yang. 2022. "The Association of Dietary Magnesium and Prediabetes in Childbearing Chinese Women: Results from China Nutrition and Health Surveillance (2015–2017)" Nutrients 14, no. 21: 4580. https://doi.org/10.3390/nu14214580
APA StyleYang, J., Zhang, H., Cao, Y., Shan, X., Feng, J., Lu, J., Cai, S., Zhao, L., & Yang, L. (2022). The Association of Dietary Magnesium and Prediabetes in Childbearing Chinese Women: Results from China Nutrition and Health Surveillance (2015–2017). Nutrients, 14(21), 4580. https://doi.org/10.3390/nu14214580