
The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review

 , , , , ,
, , , , , 
Abstract
:1. Introduction
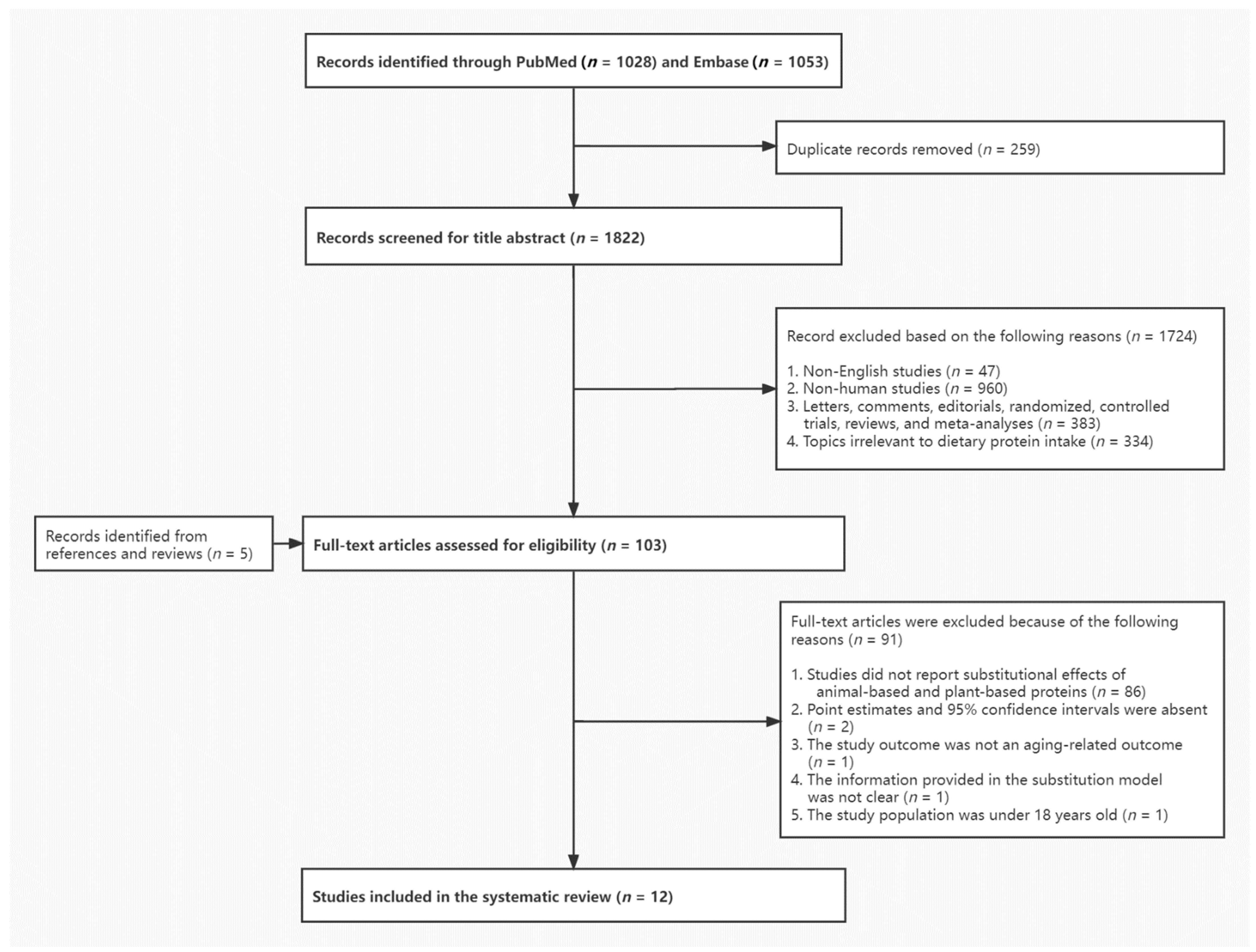
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Substitution of Protein from Animal and Plant Sources and Mortality Outcomes
3.3. Substitution of Plant Protein for Animal Protein and Risk of Aging-Related Diseases
3.4. Substitution of Plant Protein for Animal Protein and Cardiometabolic Risk Markers
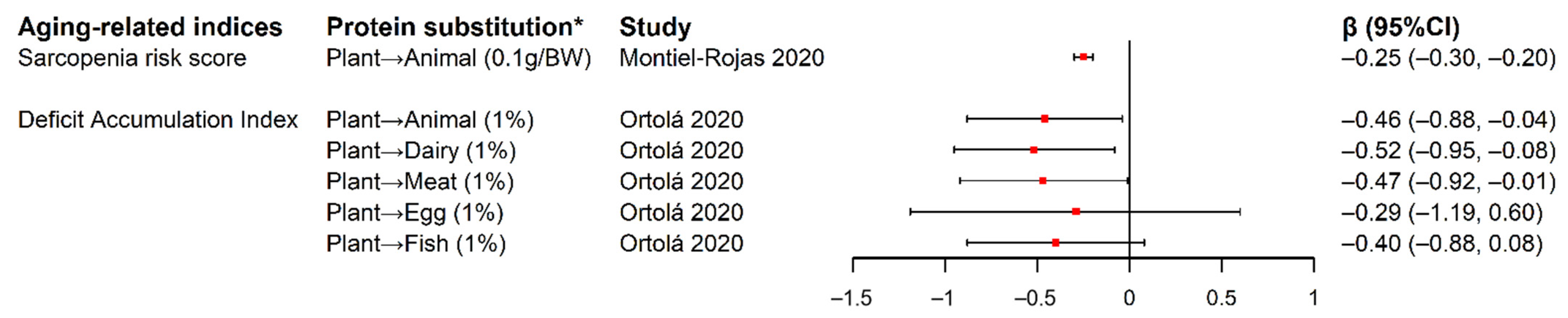
3.5. Substitution of Plant Protein for Animal Protein and Indices Associated with Unhealthy Aging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO Organization Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 29 May 2021).
- Bao, Q.; Pan, J.; Qi, H.; Wang, L.; Qian, H.; Jiang, F.; Shao, Z.; Xu, F.; Tao, Z.; Ma, Q.; et al. Aging and age-related diseases—From endocrine therapy to target therapy. Mol. Cell. Endocrinol. 2014, 394, 115–118. [Google Scholar] [CrossRef]
- Bowen, R.L.; Atwood, C.S. Living and dying for sex. A theory of aging based on the modulation of cell cycle signaling by reproductive hormones. Gerontology 2004, 50, 265–290. [Google Scholar] [CrossRef]
- Chou, Y.-H.; Chen, Y.-M. Aging and Renal Disease: Old Questions for New Challenges. Aging Dis. 2021, 12, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Garagnani, P.; Morsiani, C.; Conte, M.; Santoro, A.; Grignolio, A.; Monti, D.; Capri, M.; Salvioli, S. The Continuum of Aging and Age-Related Diseases: Common Mechanisms but Different Rates. Front. Med. 2018, 5, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Onge, M.-P.; Gallagher, D. Body composition changes with aging: The cause or the result of alterations in metabolic rate and macronutrient oxidation? Nutrition 2010, 26, 152–155. [Google Scholar] [CrossRef] [Green Version]
- Ortolá, R.; Struijk, E.A.; García-Esquinas, E.; Rodríguez-Artalejo, F.; Lopez-Garcia, E. Changes in Dietary Intake of Animal and Vegetable Protein and Unhealthy Aging. Am. J. Med. 2020, 133, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Rutherfurd-Markwick, K.J. Food proteins as a source of bioactive peptides with diverse functions. Br. J. Nutr. 2012, 108 (Suppl. S2), S149–S157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santesso, N.; Akl, E.A.; Bianchi, M.; Mente, A.; Mustafa, R.; Heels-Ansdell, D.; Schünemann, H.J. Effects of higher- versus lower-protein diets on health outcomes: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Wycherley, T.P.; Moran, L.J.; Clifton, P.M.; Noakes, M.; Brinkworth, G.D. Effects of energy-restricted high-protein, low-fat compared with standard-protein, low-fat diets: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 1281–1298. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Satija, A.; Blondin, S.A.; Janiszewski, M.; Emlen, E.; O’Connor, L.E.; Campbell, W.W.; Hu, F.B.; Willett, W.C.; Stampfer, M.J. Meta-Analysis of Randomized Controlled Trials of Red Meat Consumption in Comparison With Various Comparison Diets on Cardiovascular Risk Factors. Circulation 2019, 139, 1828–1845. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food Groups and Risk of Overweight, Obesity, and Weight Gain: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.-X.; Shen, P. Associations of dietary protein intake with all-cause, cardiovascular disease, and cancer mortality: A systematic review and meta-analysis of cohort studies. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Abete, I.; Romaguera, D.; Vieira, A.R.; de Munain, A.L.; Norat, T. Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality: A meta-analysis of cohort studies. Br. J. Nutr. 2014, 112, 762–775. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Pan, A.; Rexrode, K.M.; Stampfer, M.; Hu, F.B.; Mozaffarian, D.; Willett, W.C. Dietary protein sources and the risk of stroke in men and women. Stroke 2012, 43, 637–644. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Glisic, M.; Song, M.; Aliahmad, H.A.; Zhang, X.; Moumdjian, A.C.; Gonzalez-Jaramillo, V.; van der Schaft, N.; Bramer, W.M.; Ikram, M.A.; et al. Dietary protein intake and all-cause and cause-specific mortality: Results from the Rotterdam Study and a meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2020, 35, 411–429. [Google Scholar] [CrossRef] [Green Version]
- Kramer, H. Diet and Chronic Kidney Disease. Adv. Nutr. 2019, 10, S367–S379. [Google Scholar] [CrossRef]
- Turesky, R.J. Mechanistic Evidence for Red Meat and Processed Meat Intake and Cancer Risk: A Follow-up on the International Agency for Research on Cancer Evaluation of 2015. Chimia 2018, 72, 718–724. [Google Scholar] [CrossRef]
- Fan, M.; Li, Y.; Wang, C.; Mao, Z.; Zhou, W.; Zhang, L.; Yang, X.; Cui, S.; Li, L. Dietary Protein Consumption and the Risk of Type 2 Diabetes: ADose-Response Meta-Analysis of Prospective Studies. Nutrients 2019, 11, 2783. [Google Scholar] [CrossRef] [Green Version]
- Neuenschwander, M.; Ballon, A.; Weber, K.S.; Norat, T.; Aune, D.; Schwingshackl, L.; Schlesinger, S. Role of diet in type 2 diabetes incidence: Umbrella review of meta-analyses of prospective observational studies. BMJ 2019, 366, l2368. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.-M.; Knüppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [Green Version]
- Ahnen, R.T.; Jonnalagadda, S.S.; Slavin, J.L. Role of plant protein in nutrition, wellness, and health. Nutr. Rev. 2019, 77, 735–747. [Google Scholar] [CrossRef]
- Elliott, P.; Stamler, J.; Dyer, A.R.; Appel, L.; Dennis, B.; Kesteloot, H.; Ueshima, H.; Okayama, A.; Chan, Q.; Garside, D.B.; et al. Association between protein intake and blood pressure: The INTERMAP Study. Arch. Intern. Med. 2006, 166, 79–87. [Google Scholar] [CrossRef]
- Naghshi, S.; Sadeghi, O.; Willett, W.C.; Esmaillzadeh, A. Dietary intake of total, animal, and plant proteins and risk of all cause, cardiovascular, and cancer mortality: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2020, 370, m2412. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zeng, R.; Huang, J.; Li, X.; Zhang, J.; Ho, J.C.; Zheng, Y. Dietary Protein Sources and Incidence of Breast Cancer: A Dose-Response Meta-Analysis of Prospective Studies. Nutrients 2016, 8, 730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhan, S.; Ho, S.C. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am. J. Clin. Nutr. 2005, 81, 397–408. [Google Scholar] [CrossRef] [Green Version]
- Song, M.; Giovannucci, E. Substitution analysis in nutritional epidemiology: Proceed with caution. Eur. J. Epidemiol. 2018, 33, 137–140. [Google Scholar] [CrossRef]
- Budhathoki, S.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Goto, A.; Kotemori, A.; Ishihara, J.; Takachi, R.; Charvat, H.; Mizoue, T.; et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality in a Japanese Cohort. JAMA Intern. Med. 2019, 179, 1509–1518. [Google Scholar] [CrossRef]
- Huang, J.; Liao, L.M.; Weinstein, S.J.; Sinha, R.; Graubard, B.I.; Albanes, D. Association Between Plant and Animal Protein Intake and Overall and Cause-Specific Mortality. JAMA Intern. Med. 2020, 180, 1173–1184. [Google Scholar] [CrossRef]
- Kelemen, L.E.; Kushi, L.H.; Jacobs, D.R., Jr.; Cerhan, J.R. Associations of dietary protein with disease and mortality in a prospective study of postmenopausal women. Am. J. Epidemiol. 2005, 161, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.M.; Loftfield, E.; Etemadi, A.; Graubard, B.I.; Sinha, R. Substitution of dietary protein sources in relation to colorectal cancer risk in the NIH-AARP cohort study. Cancer Causes Control 2019, 30, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Li, Y.; Tobias, D.K.; Pan, A.; Hu, F.B. Dietary Protein Intake and Risk of Type 2 Diabetes in US Men and Women. Am. J. Epidemiol. 2016, 183, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Montiel-Rojas, D.; Nilsson, A.; Santoro, A.; Bazzocchi, A.; de Groot, L.; Feskens, E.J.M.; Berendsen, A.A.M.; Madej, D.; Kaluza, J.; Pietruszka, B.; et al. Fighting Sarcopenia in Ageing European Adults: The Importance of the Amount and Source of Dietary Proteins. Nutrients 2020, 12, 3601. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Liu, B.; Snetselaar, L.G.; Wallace, R.B.; Shadyab, A.H.; Kroenke, C.H.; Haring, B.; Howard, B.V.; Shikany, J.M.; Valdiviezo, C.; et al. Association of Major Dietary Protein Sources With All-Cause and Cause-Specific Mortality: Prospective Cohort Study. J. Am. Heart Assoc. 2021, 10, e015553. [Google Scholar] [CrossRef] [PubMed]
- van Baak, M.A.; Larsen, T.M.; Jebb, S.A.; Martinez, A.; Saris, W.H.M.; Handjieva-Darlenska, T.; Kafatos, A.; Pfeiffer, A.F.H.; Kunešová, M.; Astrup, A. Dietary Intake of Protein from Different Sources and Weight Regain, Changes in Body Composition and Cardiometabolic Risk Factors after Weight Loss: The DIOGenes Study. Nutrients 2017, 9, 1326. [Google Scholar] [CrossRef] [Green Version]
- Altorf-Van Der Kuil, W.; Engberink, M.F.; Ijpma, I.; Verberne, L.D.M.; Toeller, M.; Chaturvedi, N.; Fuller, J.H.; Soedamah-Muthu, S.S. Protein intake in relation to risk of hypertension and microalbuminuria in patients with type 1 diabetes: The EURODIAB Prospective Complications Study. J. Hypertens. 2013, 31, 1151–1159. [Google Scholar] [CrossRef]
- Oosterwijk, M.M.; Soedamah-Muthu, S.S.; Geleijnse, J.M.; Bakker, S.J.L.; Navis, G.; Binnenmars, S.H.; Gant, C.M.; Laverman, G.D. High Dietary Intake of Vegetable Protein Is Associated With Lower Prevalence of Renal Function Impairment: Results of the Dutch DIALECT-1 Cohort. Kidney Int. Rep. 2019, 4, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connel, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 31 May 2021).
- Levey, A.S.; Eckardt, K.-U.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J.; De Zeeuw, D.; Hostetter, T.H.; Lameire, N.; Eknoyan, G. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005, 67, 2089–2100. [Google Scholar] [CrossRef] [Green Version]
- Kokubo, Y.; Iso, H.; Ishihara, J.; Okada, K.; Inoue, M.; Tsugane, S. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in Japanese populations: The Japan Public Health Center-based (JPHC) study cohort I. Circulation 2007, 116, 2553–2562. [Google Scholar] [CrossRef] [Green Version]
- Pan, A.; Franco, O.H.; Ye, J.; Demark-Wahnefried, W.; Ye, X.; Yu, Z.; Li, H.; Lin, X. Soy protein intake has sex-specific effects on the risk of metabolic syndrome in middle-aged and elderly Chinese. J. Nutr. 2008, 138, 2413–2421. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, D.J.; Kendall, C.W.; Connelly, P.W.; Jackson, C.J.; Parker, T.; Faulkner, D.; Vidgen, E. Effects of high- and low-isoflavone (phytoestrogen) soy foods on inflammatory biomarkers and proinflammatory cytokines in middle-aged men and women. Metabolism 2002, 51, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Bhupathy, P.; Haines, C.D.; Leinwand, L.A. Influence of sex hormones and phytoestrogens on heart disease in men and women. Womens Health 2010, 6, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Lin, X.; Ouyang, Y.Y.; Liu, J.; Zhao, G.; Pan, A.; Hu, F.B. Red and processed meat consumption and mortality: Dose-response meta-analysis of prospective cohort studies. Public Health Nutr 2016, 19, 893–905. [Google Scholar] [CrossRef] [Green Version]
- Krittanawong, C.; Narasimhan, B.; Wang, Z.; Virk, H.U.H.; Farrell, A.M.; Zhang, H.; Tang, W.H.W. Association Between Egg Consumption and Risk of Cardiovascular Outcomes: A Systematic Review and Meta-Analysis. Am. J. Med. 2021, 134, 76–83. [Google Scholar] [CrossRef]
- Drouin-Chartier, J.-P.; Chen, S.; Li, Y.; Schwab, A.L.; Stampfer, M.J.; Sacks, F.M.; Rosner, B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Egg consumption and risk of cardiovascular disease: Three large prospective US cohort studies, systematic review, and updated meta-analysis. BMJ 2020, 368, m513. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Preterre, A.L.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food groups and risk of colorectal cancer. Int. J. Cancer 2018, 142, 1748–1758. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.-M.; Knüppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, S.S.; Mejia, S.B.; Lytvyn, L.; Stewart, S.E.; Viguiliouk, E.; Ha, V.; de Souza, R.J.; Leiter, L.A.; Kendall, C.W.C.; Jenkins, D.J.A.; et al. Effect of Plant Protein on Blood Lipids: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [Green Version]
- Viguiliouk, E.; Stewart, S.E.; Jayalath, V.H.; Ng, A.P.; Mirrahimi, A.; de Souza, R.J.; Hanley, A.J.; Bazinet, R.P.; Mejia, S.B.; Leiter, L.A.; et al. Effect of Replacing Animal Protein with Plant Protein on Glycemic Control in Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2015, 7, 9804–9824. [Google Scholar] [CrossRef] [PubMed]
- Richter, C.K.; Skulas-Ray, A.C.; Champagne, C.M.; Kris-Etherton, P.M. Plant protein and animal proteins: Do they differentially affect cardiovascular disease risk? Adv. Nutr. 2015, 6, 712–728. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef]
- Domingo, J.L.; Nadal, M. Carcinogenicity of consumption of red meat and processed meat: A review of scientific news since the IARC decision. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2017, 105, 256–261. [Google Scholar] [CrossRef]
- Etemadi, A.; Sinha, R.; Ward, M.H.; Graubard, B.I.; Inoue-Choi, M.; Dawsey, S.M.; Abnet, C.C. Mortality from different causes associated with meat, heme iron, nitrates, and nitrites in the NIH-AARP Diet and Health Study: Population based cohort study. BMJ 2017, 357, j1957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feskens, E.J.; Sluik, D.; van Woudenbergh, G.J. Meat consumption, diabetes, and its complications. Curr. Diabetes Rep. 2013, 13, 298–306. [Google Scholar] [CrossRef]
- Hollænder, P.L.; Ross, A.B.; Kristensen, M. Whole-grain and blood lipid changes in apparently healthy adults: A systematic review and meta-analysis of randomized controlled studies. Am. J. Clin. Nutr. 2015, 102, 556–572. [Google Scholar] [CrossRef] [Green Version]
- McKeown, N.M.; Meigs, J.B.; Liu, S.; Wilson, P.W.; Jacques, P.F. Whole-grain intake is favorably associated with metabolic risk factors for type 2 diabetes and cardiovascular disease in the Framingham Offspring Study. Am. J. Clin. Nutr. 2002, 76, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Mariotti, F.; Huneau, J.-F. Plant and Animal Protein Intakes Are Differentially Associated with Large Clusters of Nutrient Intake that May Explain Part of Their Complex Relation with CVD Risk. Adv. Nutr. 2016, 7, 559–560. [Google Scholar] [CrossRef] [Green Version]
- Jennings, A.; MacGregor, A.; Welch, A.; Chowienczyk, P.; Spector, T.; Cassidy, A. Amino Acid Intakes Are Inversely Associated with Arterial Stiffness and Central Blood Pressure in Women. J. Nutr. 2015, 145, 2130–2138. [Google Scholar] [CrossRef] [PubMed]
- Windey, K.; De Preter, V.; Verbeke, K. Relevance of protein fermentation to gut health. Mol. Nutr. Food Res. 2012, 56, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Klipfell, E.; Bennett, B.J.; Koeth, R.; Levison, B.S.; Dugar, B.; Feldstein, A.E.; Britt, E.B.; Fu, X.; Chung, Y.-M.; et al. Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472, 57–63. [Google Scholar] [CrossRef] [Green Version]
- Chan, R.; Leung, J.; Woo, J.; Kwok, T. Associations of dietary protein intake on subsequent decline in muscle mass and physical functions over four years in ambulant older Chinese people. J. Nutr. Health Aging 2014, 18, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Gardener, H.; Caunca, M.R. Mediterranean Diet in Preventing Neurodegenerative Diseases. Curr. Nutr. Rep. 2018, 7, 10–20. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria |
|---|---|
| Population | Adults aged over 18 (including mean age) at baseline for cohort studies |
| Intervention/exposure | Isocaloric substitution of plant-based and animal-based protein or protein from food sources, as defined in the context of nutritional substitution model |
| Comparison | Continuous (e.g., 3% or 5% of total energy from plant protein substituted for animal protein) or categorical (e.g., highest vs. lowest level of percentage of energy from plant protein substituted for animal protein) |
| Outcomes | Aging-related health outcomes which included mortality outcomes, aging-related disorders such as cancer, type-2 diabetes, chronic kidney diseases, cardiometabolic diseases and risk markers, as well as aging-related indices |
| Study design | Original research studies of any observational design were eligible. Systematic or narrative reviews, intervention studies, conference or dissertations, editorials, case reports or other descriptive studies were excluded |
| Reference | Study Design (Location) | Number of Cases a/Total Individuals at Risk b | Mean Age (Range) | Mean or Median Follow-Up Time for Cohort Study | Diet Assessment Instrument/Assessment Period/Whether Assessment of Validity and Reproducibility | Substitutional Model | Aging-Related Outcomes | Variables for Adjustment c |
|---|---|---|---|---|---|---|---|---|
| Kelemen et al. (2004) [31] | Cohort study (USA) | 4843 total incident cancer cases and 3978 total deaths/29,017 participants | 55–69 | Mean = 11.4 years | 131-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | Highest versus lowest quintile of percentage of energy from total plant protein substituted for total animal protein while holding constant the intake of total energy, carbohydrate and fat | 1. Mortality from the following causes: all-cause, CHD, total cancer; 2. Total cancer incidence | Age, total energy, carbohydrate, saturated fat, polyunsaturated fat, monounsaturated fat, trans-fat, total fiber, dietary cholesterol, dietary methionine, alcohol drink, smoking status, activity level, BMI, history of hypertension, postmenopausal hormone use, multivitamin use, vitamin E supplement use, education, and family history of cancer |
| der Kuil et al. (2013) [37] | Cohort study (16 European countries) | 298 incident hypertension cases/1319 participants with type-1 DM | 31.0 (15–60) | Mean = 7 years | 3-day food record/within a 2-week period at baseline/NA | 1.Substitution of 3% of energy intake form total animal protein for total plant protein holding constant the intake of total energy, carbohydrate and fat; 2. Substitution of 3% of energy intake from total plant protein for total animal protein holding constant the intake of total energy, carbohydrate and fat | Hypertension and microalbuminuria incidence | Age, sex, diabetes duration, HbA1c, BMI, smoking status, physical activity, total energy intake, energy densities from fat, carbohydrate and alcohol |
| 135 incident microalbuminuria cases/1045 participants with type-1 DM | ||||||||
| Malik et al. (2016) [33] | Cohort studies (USA) d | 7214 incident type-2 DM cases/72,992 participants | 30–55 | Mean = 20.2 years | 131-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | Substitution of 5% of energy intake from total plant protein for total animal protein holding constant the intake of total energy and fat | Type-2 diabetes incidence | Age, family history of diabetes, smoking status, alcohol intake, physical activity, race/ethnicity, postmenopausal hormone use, oral contraceptive use, total energy intake, percentage of energy from fat, dietary cholesterol, dietary fiber, glycemic index, and BMI |
| 5032 incident type-2 DM cases/92,088 participants | 24–42 | |||||||
| 3334 incident type-2 DM cases/40,722 participants | 40–75 | |||||||
| Song et al. (2016) [10] | Cohort study (USA) | 36,115 total deaths/131,342 participants | 49 (30–75) | Mean = 27.0 years | 131-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | Substitution of 3% of energy intake from total plant protein for animal proteins from various animal-based food sources (i.e., processed red meat, unprocessed red meat, poultry, fish, egg, dairy) holding constant the intake of total energy, and fat | Mortality from the following causes: all-cause, CVD, total cancer | Total caloric intake, age, sex, percentage of energy from saturated fat, polyunsaturated fat, monounsaturated fat, trans-fat, multivitamin use, smoking status, pack-years of smoking, BMI, physical activity, alcohol consumption, history of hypertension diagnosis, glycemic index, and intake of whole grains, total fiber, fruits and vegetables. |
| Van Baak et al. (2017) [36] | Cross-sectional study (8 European countries) | 489 overweight or obese participants | 42.3 (<65) | NA | 3-day food record/Four weeks after the start of WM phase and in the last week of WM phase e/NA | Substitution of 1% of total protein intake from total animal protein for total plant protein holding constant the intake of total protein | Change in body weight, body fat, waist circumference, SBP, DBP, total cholesterol, HDL-C, LDL-C, triglycerides, fasting glucose, fasting insulin, HOMA-IR, matsuda index, CRP, adiponectin during the WM phase | BMI at randomization, changes in the anthropometrics, blood pressure and metabolic parameters during the weight loss phase, gender, type of center, dietary protein intake, glycemic index, dietary fat intake and fiber intake |
| Budhathoki et al. (2019) [29] | Cohort study (Japan) | 12,381 total deaths/70,696 participants | 55.7 (45–74) | Mean = 18 years | 138-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | Substitution of 3% of energy intake from total plant protein for animal proteins from various animal-based food sources (i.e., red meat, processed meat, chicken, egg, dairy, fish) holding constant the intake of total energy, carbohydrate and fat | Mortality from the following causes: all-cause, CVD, total cancer | Total energy, percentage of energy from fats and carbohydrates, age, sex, BMI, smoking status, alcohol use, physical activity, occupation status, and intake of green tea and coffee. |
| Liao et al. (2019) [32] | Cohort study (USA) | 8995 incident colorectal cancer cases/489,625 participants | 50–71 | Median = 15.5 years | 124-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | 1. Highest versus lowest quintile of amount of total plant protein substituted for animal protein from various animal-based food sources (all animal foods, red meat, white meat, other animal foods) holding constant the intake of total energy and protein; 2. Highest versus lowest quintile of amount of plant protein from various plant-based food sources (bread, cereal and pasta; nuts; beans and legumes; other plant sources) substituted for red meat protein holding constant the intake of total energy and protein | Colorectal cancer, colon cancer, proximal colon cancer, distal colon cancer, and rectal cancer incidence | Age, total protein, total energy, sex, education, marriage status, family history of colon cancer, race, BMI, smoking status, frequency of vigorous physical activity, alcohol intake, fruit intake, vegetable intake, total calcium intake, total folate intake, dietary fiber intake. |
| Oosterwijk et al. (2019) [38] | Cross-sectional study (Netherland) | 99 renal function impairment cases/420 participants with type-2 DM | 63 | NA | 177-item self-administered FFQ/in the past month/only validity was assessed | 1. Substitution of 3% of energy intake from total plant protein for total animal protein holding constant the intake of total energy, fat and carbohydrate; 2. Substitution of 3% of energy intake from total animal protein for total plant protein holding constant the intake of total energy, fat and carbohydrate. | Renal function impairment prevalence | Age, gender, diabetes duration, BMI, smoking status, physical activity, alcohol intake, saturated fat intake, unsaturated fat intake, intake of mono- and disaccharides, intake of polysaccharides, intake of fiber and intake of trans fatty acids. |
| Huang et al. (2020) [30] | Cohort study (USA) | 77,614 total deaths/416,104 participants | 62.1 (50–71) | Median = 15.5 years | 124-item self-administered FFQ/in the past year/validity and reproducibility were both assessed | 1. Substitution of 3% of energy from total plant protein for animal proteins from various animal-based food sources (all animal foods, red meat, white meat, dairy, egg) holding constant the intake of total energy and fat; 2. Substitution of 3% of energy from plant protein from various plant-based food sources (bread, cereal and pasta; nuts; beans and legumes; other plant foods) for egg and red meat protein holding constant the intake of total energy and fat. | Mortality from the following causes: all-cause, CVD, total cancer, heart disease, stroke, respiratory disease | Age at entry, BMI, alcohol consumption, smoking status, physical activity, race or ethnic group, educational level, marital status, diabetes, health status, vitamin supplement use, daily dietary total energy, animal protein, saturated fat, polyunsaturated fat, monounsaturated fat, trans fat, fiber, vegetables, and fruits, and postmenopausal hormone replacement therapy. |
| Ortolá et al. (2020) [7] | Cohort study (Spain) | 812 participants | 68.6 (>60) | Median = 8.2 years | 900-item computerized diet history/in the past year/ only validity was assessed | 1% change in energy from total plant protein substituted for animal protein from various animal-based sources (total animal foods, dairy, meat, egg and fish) from wave 0 (2008–2010) to wave 1 (2012) holding constant the intake of total energy, carbohydrate and fat | Change in DAI between wave 0 (2008–2010) and wave 3 (2017) f | Sex, age, educational level, DAI at wave 0, changes in energy intake, vegetable protein intake, animal protein intake from all sources except the one being examined, fat intake, carbohydrate intake and alcohol intake from wave 0 to wave 1, changes in smoking status, alcohol consumption status, leisure-time physical activity, sedentary behavior, and BMI from wave 0 to wave 3. |
| Montiel-Rojas et al. (2020) [34] | Cross-sectional study (4 European countries) | 986 participants | 65–79 | NA | 1-week food record/at baseline/ NA | Substitution of 0.1g/BW increase of total plant protein for total animal protein holding constant the intake of total energy and protein | Sarcopenia risk score g | Total protein intake, plant protein intake, total energy intake, age, recruiting center, medication, smoking habits, prevalence of MetS, adherence to PA guidelines, and fiber intake. |
| Sun et al. (2021) [35] | Cohort study (USA) | 25,976 total deaths/102,521 participants | 50–79 | Mean = 18.1 years | 122-item self-administered FFQ/in the past three months/validity and reproducibility were both assessed | Substitution of 5% of energy from total plant protein for total animal protein holding constant the intake of total energy and fat | Mortality from the following causes: all-cause, CVD, total cancer, dementia | Age at baseline, race/ethnicity, education, income, Observational Study/Clinical Trials, hormone use history, smoking status, physical activity, baseline diabetes mellitus status and high blood cholesterol status, and family history of heart attack/stroke, alcohol intake, total energy intake, percentage of energy from saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids and trans-fatty acids, dietary fiber intake, and glycemic load. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, J.; Zhu, T.; Yang, G.; Zhao, L.; Li, F.; Park, Y.-M.; Tabung, F.K.; Steck, S.E.; Li, X.; Wang, H. The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review. Nutrients 2022, 14, 272. https://doi.org/10.3390/nu14020272
Zheng J, Zhu T, Yang G, Zhao L, Li F, Park Y-M, Tabung FK, Steck SE, Li X, Wang H. The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review. Nutrients. 2022; 14(2):272. https://doi.org/10.3390/nu14020272
Chicago/Turabian StyleZheng, Jiali, Tianren Zhu, Guanghuan Yang, Longgang Zhao, Fangyu Li, Yong-Moon Park, Fred K. Tabung, Susan E. Steck, Xiaoguang Li, and Hui Wang. 2022. "The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review" Nutrients 14, no. 2: 272. https://doi.org/10.3390/nu14020272
APA StyleZheng, J., Zhu, T., Yang, G., Zhao, L., Li, F., Park, Y.-M., Tabung, F. K., Steck, S. E., Li, X., & Wang, H. (2022). The Isocaloric Substitution of Plant-Based and Animal-Based Protein in Relation to Aging-Related Health Outcomes: A Systematic Review. Nutrients, 14(2), 272. https://doi.org/10.3390/nu14020272