
Plant-Based Diets Improve Maternal–Fetal Outcomes in CKD Pregnancies

 , ,
, ,  ,
,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Settings of the Study
2.2. Definitions Employed
2.3. Indications for the Diet
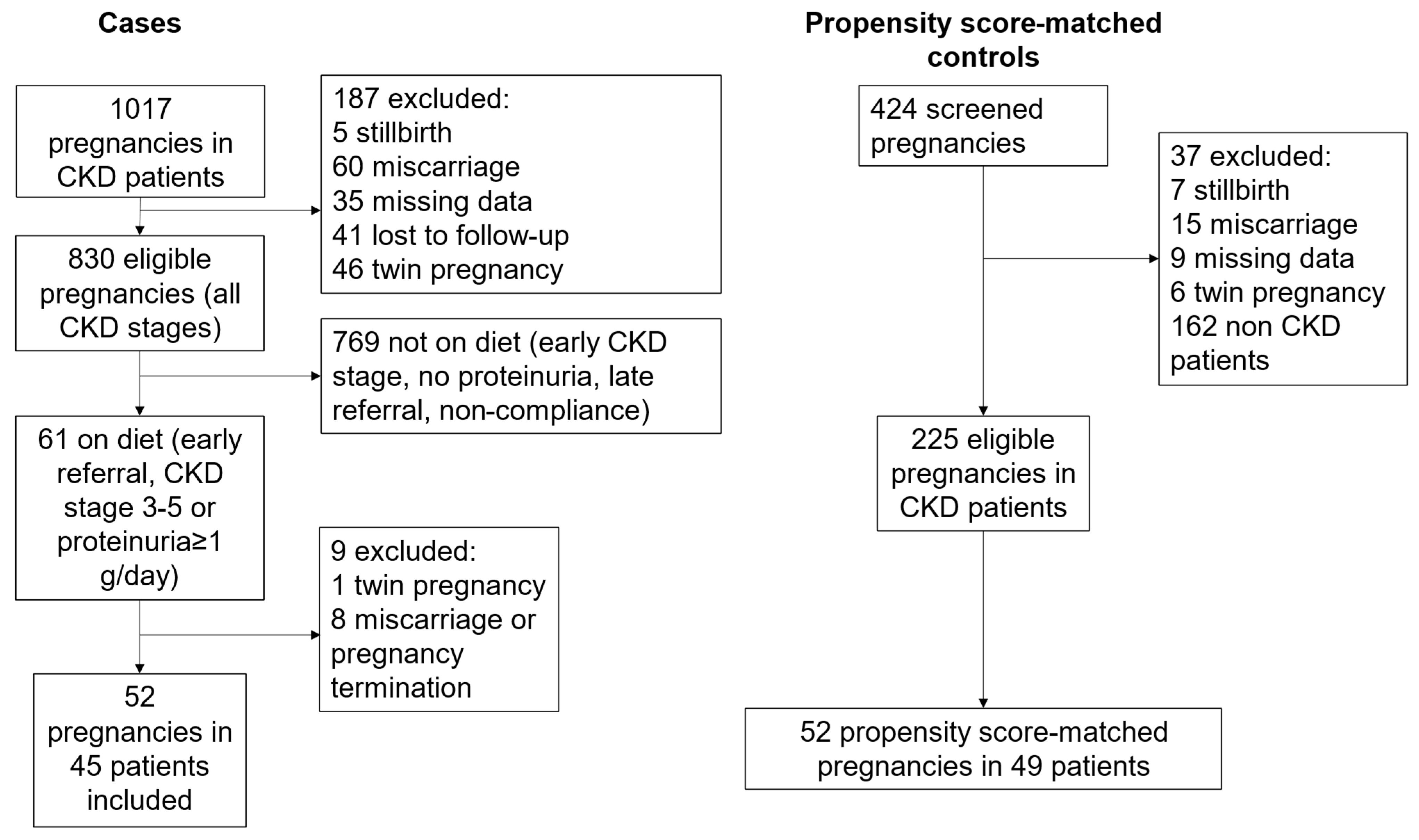
2.4. Selection of the Control Group
2.5. The Plant-Based, Moderately Protein-Restricted Diet
2.6. Statistical Evaluation
2.7. Ethical Issues
3. Results
3.1. Baseline Data
3.2. Pregnancy Outcomes, According to Diet Prescription
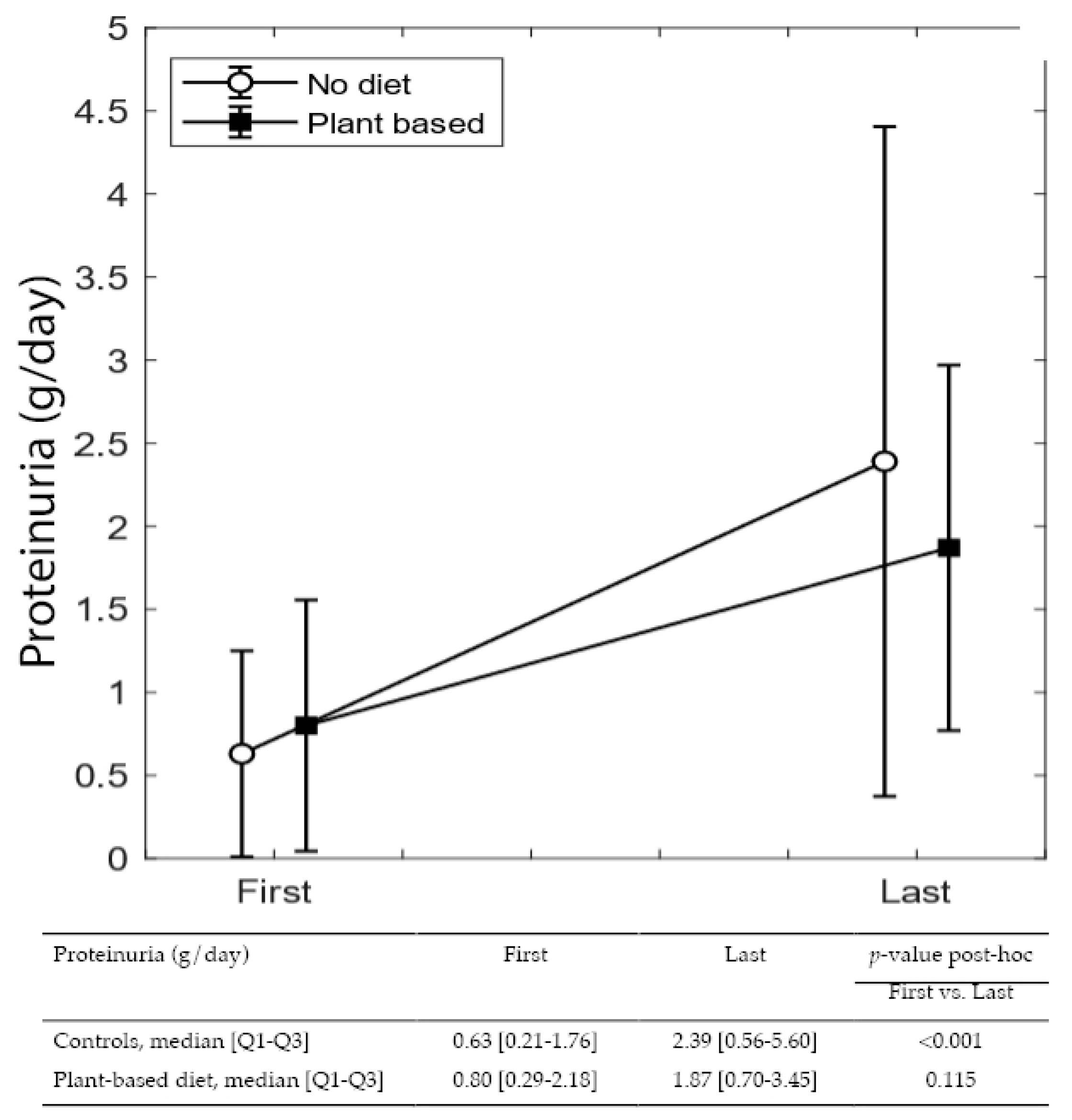
3.3. Variations in Proteinuria and eGFR from the First to Last Control Visit during Pregnancy
3.4. Logistic Regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Inter. Suppl. 2013, 3, 1–150. [Google Scholar]
- Williams, D.; Davison, J. Chronic kidney disease in pregnancy. BMJ 2008, 336, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Webster, P.; Lightstone, L.; McKay, D.B.; Josephson, M.A. Pregnancy in chronic kidney disease and kidney transplantation. Kidney Int. 2017, 91, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Nevis, I.F.; Reitsma, A.; Dominic, A.; McDonald, S.; Thabane, L.; Akl, E.A.; Hladunewich, M.; Akbari, A.; Joseph, G.; Sia, W.; et al. Pregnancy outcomes in women with chronic kidney disease: A systematic review. Clin. J. Am. Soc. Nephrol. 2011, 6, 2587–2598. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Maxia, S.; Lepori, N.; Tuveri, M.; Massidda, M.; Marchi, C.; Mura, S.; et al. Risk of Adverse Pregnancy Outcomes in Women with CKD. J. Am. Soc. Nephrol. 2015, 26, 2011–2022. [Google Scholar] [CrossRef]
- Zhang, J.J.; Ma, X.X.; Hao, L.; Liu, L.J.; Lv, J.C.; Zhang, H. A Systematic Review and Meta-Analysis of Outcomes of Pregnancy in CKD and CKD Outcomes in Pregnancy. Clin. J. Am. Soc. Nephrol. 2015, 10, 1964–1978. [Google Scholar] [CrossRef]
- Tangren, J.S.; Wan Md Adnan, W.A.H.; Powe, C.E.; Ecker, J.; Bramham, K.; Hladunewich, M.A.; Ankers, E.; Karumanchi, S.A.; Thadhani, R. Risk of Preeclampsia and Pregnancy Complications in Women With a History of Acute Kidney Injury. Hypertension 2018, 72, 451–459. [Google Scholar] [CrossRef]
- Sebastian, N.; Czuzoj-Shulman, N.; Spence, A.R.; Abenhaim, H.A. Maternal and fetal outcomes of urolithiasis: A retrospective cohort study. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102161. [Google Scholar] [CrossRef]
- Garg, A.X.; Nevis, I.F.; McArthur, E.; Sontrop, J.M.; Koval, J.J.; Lam, N.N.; Hildebrand, A.M.; Reese, P.P.; Storsley, L.; Gill, J.S.; et al. Gestational hypertension and preeclampsia in living kidney donors. N. Engl. J. Med. 2015, 372, 124–133. [Google Scholar] [CrossRef]
- Davis, S.; Dylewski, J.; Shah, P.B.; Holmen, J.; You, Z.; Chonchol, M.; Kendrick, J. Risk of adverse maternal and fetal outcomes during pregnancy in living kidney donors: A matched cohort study. Clin. Transplant. 2019, 33, e13453. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Attini, R.; Vasario, E.; Conijn, A.; Biolcati, M.; D’Amico, F.; Consiglio, V.; Bontempo, S.; Todros, T. Pregnancy and chronic kidney disease: A challenge in all CKD stages. Clin. J. Am. Soc. Nephrol. 2010, 5, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Alsuwaida, A.; Mousa, D.; Al-Harbi, A.; Alghonaim, M.; Ghareeb, S.; Alrukhaimi, M.N. Impact of early chronic kidney disease on maternal and fetal outcomes of pregnancy. J. Matern. Fetal. Neonatal Med. 2011, 24, 1432–1436. [Google Scholar] [CrossRef] [PubMed]
- Imbasciati, E.; Gregorini, G.; Cabiddu, G.; Gammaro, L.; Ambroso, G.; Del Giudice, A.; Ravani, P. Pregnancy in CKD stages 3 to 5: Fetal and maternal outcomes. Am. J. Kidney Dis. 2007, 49, 753–762. [Google Scholar] [CrossRef]
- Hoy, W.E.; Hughson, M.D.; Bertram, J.F.; Douglas-Denton, R.; Amann, K. Nephron number, hypertension, renal disease, and renal failure. J. Am. Soc. Nephrol. 2005, 16, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Luyckx, V.A.; Brenner, B.M. The clinical importance of nephron mass. J. Am. Soc. Nephrol. 2010, 21, 898–910. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional Management of Chronic Kidney Disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Naber, T.; Purohit, S. Chronic Kidney Disease: Role of Diet for a Reduction in the Severity of the Disease. Nutrients 2021, 13, 3277. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Carrero, J.J.; Gonzalez-Ortiz, A.; Avesani, C.M.; Bakker, S.J.L.; Bellizzi, V.; Chauveau, P.; Clase, C.M.; Cupisti, A.; Espinosa-Cuevas, A.; Molina, P.; et al. Plant-based diets to manage the risks and complications of chronic kidney disease. Nat. Rev. Nephrol. 2020, 16, 525–542. [Google Scholar] [CrossRef]
- Chauveau, P.; Koppe, L.; Combe, C.; Lasseur, C.; Trolonge, S.; Aparicio, M. Vegetarian diets and chronic kidney disease. Nephrol. Dial. Transplant. 2019, 34, 199–207. [Google Scholar] [CrossRef]
- Joshi, S.; McMacken, M.; Kalantar-Zadeh, K. Plant-Based Diets for Kidney Disease: A Guide for Clinicians. Am J Kidney Dis 2021, 77, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.J.; Mangels, A.R.; American Dietetic, A. Position of the American Dietetic Association: Vegetarian diets. J. Am. Diet. Assoc. 2009, 109, 1266–1282. [Google Scholar] [CrossRef] [PubMed]
- Procter, S.B.; Campbell, C.G. Position of the Academy of Nutrition and Dietetics: Nutrition and lifestyle for a healthy pregnancy outcome. J. Acad. Nutr. Diet. 2014, 114, 1099–1103. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, L.L.; Campbell, C.G.; Academy Positions Committee, W. Practice paper of the Academy of Nutrition and Dietetics abstract: Nutrition and lifestyle for a healthy pregnancy outcome. J. Acad. Nutr. Diet. 2014, 114, 1447. [Google Scholar] [CrossRef] [PubMed]
- Sebastiani, G.; Herranz Barbero, A.; Borras-Novell, C.; Alsina Casanova, M.; Aldecoa-Bilbao, V.; Andreu-Fernandez, V.; Pascual Tutusaus, M.; Ferrero Martinez, S.; Gomez Roig, M.D.; Garcia-Algar, O. The Effects of Vegetarian and Vegan Diet during Pregnancy on the Health of Mothers and Offspring. Nutrients 2019, 11, 557. [Google Scholar] [CrossRef]
- Perry, A.; Stephanou, A.; Rayman, M.P. Dietary factors that affect the risk of pre-eclampsia. BMJ Nutr. Prev. Health 2022, 5, 118–133. [Google Scholar] [CrossRef]
- Helal, I.; Fick-Brosnahan, G.M.; Reed-Gitomer, B.; Schrier, R.W. Glomerular hyperfiltration: Definitions, mechanisms and clinical implications. Nat. Rev. Nephrol. 2012, 8, 293–300. [Google Scholar] [CrossRef]
- Cabiddu, G.; Castellino, S.; Gernone, G.; Santoro, D.; Moroni, G.; Giannattasio, M.; Gregorini, G.; Giacchino, F.; Attini, R.; Loi, V.; et al. A best practice position statement on pregnancy in chronic kidney disease: The Italian Study Group on Kidney and Pregnancy. J. Nephrol. 2016, 29, 277–303. [Google Scholar] [CrossRef]
- Piccoli, G.B.; Leone, F.; Attini, R.; Parisi, S.; Fassio, F.; Deagostini, M.C.; Ferraresi, M.; Clari, R.; Ghiotto, S.; Biolcati, M.; et al. Association of low-protein supplemented diets with fetal growth in pregnant women with CKD. Clin. J. Am. Soc. Nephrol. 2014, 9, 864–873. [Google Scholar] [CrossRef]
- Attini, R.; Leone, F.; Parisi, S.; Fassio, F.; Capizzi, I.; Loi, V.; Colla, L.; Rossetti, M.; Gerbino, M.; Maxia, S.; et al. Vegan-vegetarian low-protein supplemented diets in pregnant CKD patients: Fifteen years of experience. BMC Nephrol. 2016, 17, 132. [Google Scholar] [CrossRef]
- Attini, R.; Leone, F.; Montersino, B.; Fassio, F.; Minelli, F.; Colla, L.; Rossetti, M.; Rollino, C.; Alemanno, M.G.; Barreca, A.; et al. Pregnancy, Proteinuria, Plant-Based Supplemented Diets and Focal Segmental Glomerulosclerosis: A Report on Three Cases and Critical Appraisal of the Literature. Nutrients 2017, 9, 770. [Google Scholar] [CrossRef] [PubMed]
- Orozco-Guillien, A.O.; Munoz-Manrique, C.; Reyes-Lopez, M.A.; Perichat-Perera, O.; Miranda-Araujo, O.; D’Alessandro, C.; Piccoli, G.B. Quality or Quantity of Proteins in the Diet for CKD Patients: Does “Junk Food” Make a Difference? Lessons from a High-Risk Pregnancy. Kidney Blood Press. Res. 2021, 46, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nava, J.; Moran, S.; Figueroa, V.; Salinas, A.; Lopez, M.; Urbina, R.; Gutierrez, A.; Lujan, J.L.; Orozco, A.; Montufar, R.; et al. Successful pregnancy in a CKD patient on a low-protein, supplemented diet: An opportunity to reflect on CKD and pregnancy in Mexico, an emerging country. J. Nephrol. 2017, 30, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet. Gynecol. 2020, 135, e237–e260. [Google Scholar] [CrossRef] [PubMed]
- Masuyama, H.; Nobumoto, E.; Okimoto, N.; Inoue, S.; Segawa, T.; Hiramatsu, Y. Superimposed preeclampsia in women with chronic kidney disease. Gynecol. Obstet. Investig. 2012, 74, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Cheikh Ismail, L.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Hypertension in pregnancy: Diagnosis and management. NICE Guideline [NG133]. Available online: https://www.nice.org.uk/guidance/ng133 (accessed on 22 April 2022).
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef]
- La gravidanza Fisiologica, Aggiornamento 2011. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_1436_allegato.pdf (accessed on 10 September 2022).
- Piccoli, G.B.; Attini, R.; Vasario, E.; Gaglioti, P.; Piccoli, E.; Consiglio, V.; Deagostini, C.; Oberto, M.; Todros, T. Vegetarian supplemented low-protein diets. A safe option for pregnant CKD patients: Report of 12 pregnancies in 11 patients. Nephrol. Dial. Transplant. 2011, 26, 196–205. [Google Scholar] [CrossRef]
- Most, J.; Dervis, S.; Haman, F.; Adamo, K.B.; Redman, L.M. Energy Intake Requirements in Pregnancy. Nutrients 2019, 11, 1812. [Google Scholar] [CrossRef]
- Attini, R.; Montersino, B.; Leone, F.; Minelli, F.; Fassio, F.; Rossetti, M.M.; Colla, L.; Masturzo, B.; Barreca, A.; Menato, G.; et al. Dialysis or a Plant-Based Diet in Advanced CKD in Pregnancy? A Case Report and Critical Appraisal of the Literature. J. Clin. Med. 2019, 8, 123. [Google Scholar] [CrossRef]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. Matching as Nonparametric Preprocessing for Reducing Model Dependence in Parametric Causal Inference. Political Anal. 2007, 15, 199–236. [Google Scholar] [CrossRef]
- Brenner, B.M.; Lawler, E.V.; Mackenzie, H.S. The hyperfiltration theory: A paradigm shift in nephrology. Kidney Int. 1996, 49, 1774–1777. [Google Scholar] [CrossRef] [PubMed]
- Esposito, P.; Garibotto, G.; Picciotto, D.; Costigliolo, F.; Viazzi, F.; Conti, N.E. Nutritional Challenges in Pregnant Women with Renal Diseases: Relevance to Fetal Outcomes. Nutrients 2020, 12, 873. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Lopez, M.A.; Piccoli, G.B.; Leone, F.; Orozco-Guillen, A.; Perichart-Perera, O. Nutrition care for chronic kidney disease during pregnancy: An updated review. Eur. J. Clin. Nutr. 2020, 74, 983–990. [Google Scholar] [CrossRef]
- Chen, Z.; Qian, F.; Liu, G.; Li, M.; Voortman, T.; Tobias, D.K.; Ley, S.H.; Bhupathiraju, S.N.; Li, L.J.; Chavarro, J.E.; et al. Prepregnancy plant-based diets and the risk of gestational diabetes mellitus: A prospective cohort study of 14,926 women. Am. J. Clin. Nutr. 2021, 114, 1997–2005. [Google Scholar] [CrossRef]
- Craig, W.J.; Mangels, A.R.; Fresan, U.; Marsh, K.; Miles, F.L.; Saunders, A.V.; Haddad, E.H.; Heskey, C.E.; Johnston, P.; Larson-Meyer, E.; et al. The Safe and Effective Use of Plant-Based Diets with Guidelines for Health Professionals. Nutrients 2021, 13, 4144. [Google Scholar] [CrossRef]
- Nieddu, A.; Vindas, L.; Errigo, A.; Vindas, J.; Pes, G.M.; Dore, M.P. Dietary Habits, Anthropometric Features and Daily Performance in Two Independent Long-Lived Populations from Nicoya peninsula (Costa Rica) and Ogliastra (Sardinia). Nutrients 2020, 12, 1621. [Google Scholar] [CrossRef]
- Tessier, S.; Gerber, M. Comparison between Sardinia and Malta: The Mediterranean diet revisited. Appetite 2005, 45, 121–126. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | No Diet | Plant-Based Diet | p-Values | |
|---|---|---|---|---|
| Overall data CKD | ||||
| N | 104 | 52 | 52 | |
| Baseline data | ||||
| Age (years), median [Q1–Q3] | 34 [31.75–38] | 34.5 [33–38] | 34 [30.75–38] | 0.533 |
| Parity (primiparous), n (%) | 66 (63.46%) | 36 (69.23%) | 30 (57.69%) | 0.222 |
| BMI (kg/m2), median [Q1–Q3] | 23.15 [20.9–26.62] | 22.9 [20.19–26.04] | 23.63 [21.48–26.62] | 0.485 |
| BMI ≥ 30 kg/m2, n (%) | 14 (13.46%) | 7 (13.46%) | 7 (13.46%) | 1 |
| Ethnicity (non-Caucasian), n (%) | 95 (91.35%) | 1 (1.92%) | 8 (15.39%) | 0.015 |
| Baseline kidney function data | ||||
| Serum creatinine, median [Q1–Q3] | 1.02 [0.73–1.39] | 0.99 [0.65–1.31] | 1.04 [0.79–1.41] | 0.301 |
| eGFR CKD-EPI (mL/min), median [Q1–Q3] | 71.21 [40.42–106.40] | 72.04 [50.75–113.48] | 69.72 [48.68–98.37] | 0.435 |
| Stage 1, n (%) | 31 (29.81%) | 16 (30.77%) | 15 (28.85%) | 0.514 |
| Stage 2, n (%) | 33 (31.73%) | 16 (30.77%) | 17 (32.69%) | |
| Stage 3, n (%) | 19 (18.27%) | 11 (21.15%) | 8 (15.39%) | |
| Stage 4, n (%) | 15 (14.42%) | 8 (15.39%) | 7 (13.46%) | |
| Stage 5, n (%) | 6 (5.775) | 1 (1.92%) | 5 (9.62%) | |
| Proteinuria (g/24 h), median [Q1–Q3] | 0.705 [0.24–2.06] | 0.63 [0.21–1.76] | 0.80 [0.29–2.18] | 0.196 |
| Proteinuria < 0.5 g/24 h, n (%) | 38 (36.54%) | 20 (38.46%) | 18 (34.62%) | 0.739 |
| Proteinuria 0.5–1 g/24 h, n (%) | 24 (23.08%) | 12 (23.08%) | 12 (23.08%) | |
| Proteinuria 1–3 g/24 h, n (%) | 26 (25%) | 14 (26.92%) | 12 (23.08%) | |
| Proteinuria ≥ 3 g/24 h, n (%) | 16 (15.39%) | 6 (11.54%) | 10 (19.23%) | |
| Timing of referral | ||||
| Week at referral, median [Q1–Q3] | 8 [6–12] | 9 [7–12.25] | 7.5 [6–12] | 0.201 |
| <12 gestational weeks, n (%) | 73 (70.195) | 36 (69.23%) | 37 (71.15%) | 0.757 |
| 13–23 gestational weeks, n (%) | 8 (7.69%) | 5 (9.62%) | 3 (5.77%) | |
| ≥24 gestational weeks, n (%) | 23 (22.12%) | 11 (21.15%) | 12 (23.08%) | |
| Cause of CKD | ||||
| Glomerular (primary and secondary GN), n (%) | 54 (51.92%) | 27 (51.92%) | 27 (51.92%) | 1 |
| Single kidney, n (%) | 3 (2.89%) | 2 (3.85%) | 1 (1.93%) | 0.558 |
| Diabetic nephropathy, n (%) | 14 (13.46%) | 5 (9.62%) | 9 (17.31%) | 0.250 |
| ADPKD, n (%) | 6 (5.77%) | 4 (7.69%) | 2 (3.85%) | 0.400 |
| Kidney graft, n (%) | 9 (8.65%) | 5 (9.62%) | 4 (7.69%) | 0.727 |
| Interstitial (includes interstitial nephropathies, kidney stones, CAKUT and urologic malformations), n (%) | 10 (9.62%) | 5 (9.62%) | 5 (9.62%) | 1 |
| Other, n (%) | 8 (7.96%) | 4 (7.69%) | 4 (7.69%) | 1 |
| All | No Diet | Plant-Based Diet | p-Values | |
|---|---|---|---|---|
| Overall data CKD | ||||
| N | 104 | 52 | 52 | |
| Renal data at last control visit | ||||
| Serum creatinine, median [Q1–Q3] | 1.1 [0.74–1.64] | 1 [0.7–1.56] | 1.18 [0.81–1.65] | 0.194 |
| Proteinuria (g/24 h), median [Q1–Q3] | 1.97 [0.58–4.46] | 2.39 [0.56–5.6] | 1.87 [0.70–3.45] | 0.338 |
| eGFR CKD-EPI (mL/min), median [Q1–Q3] | 65.62 [41.66–105.01] | 72.93 [42.8–113.22] | 62.16 [40.65–95.20] | 0.302 |
| Stage shift (increase of at least 1 CKD stage), n (%) | 21 (20.19%) | 11 (21.15%) | 10 (19.23%) | 0.807 |
| Delivery | ||||
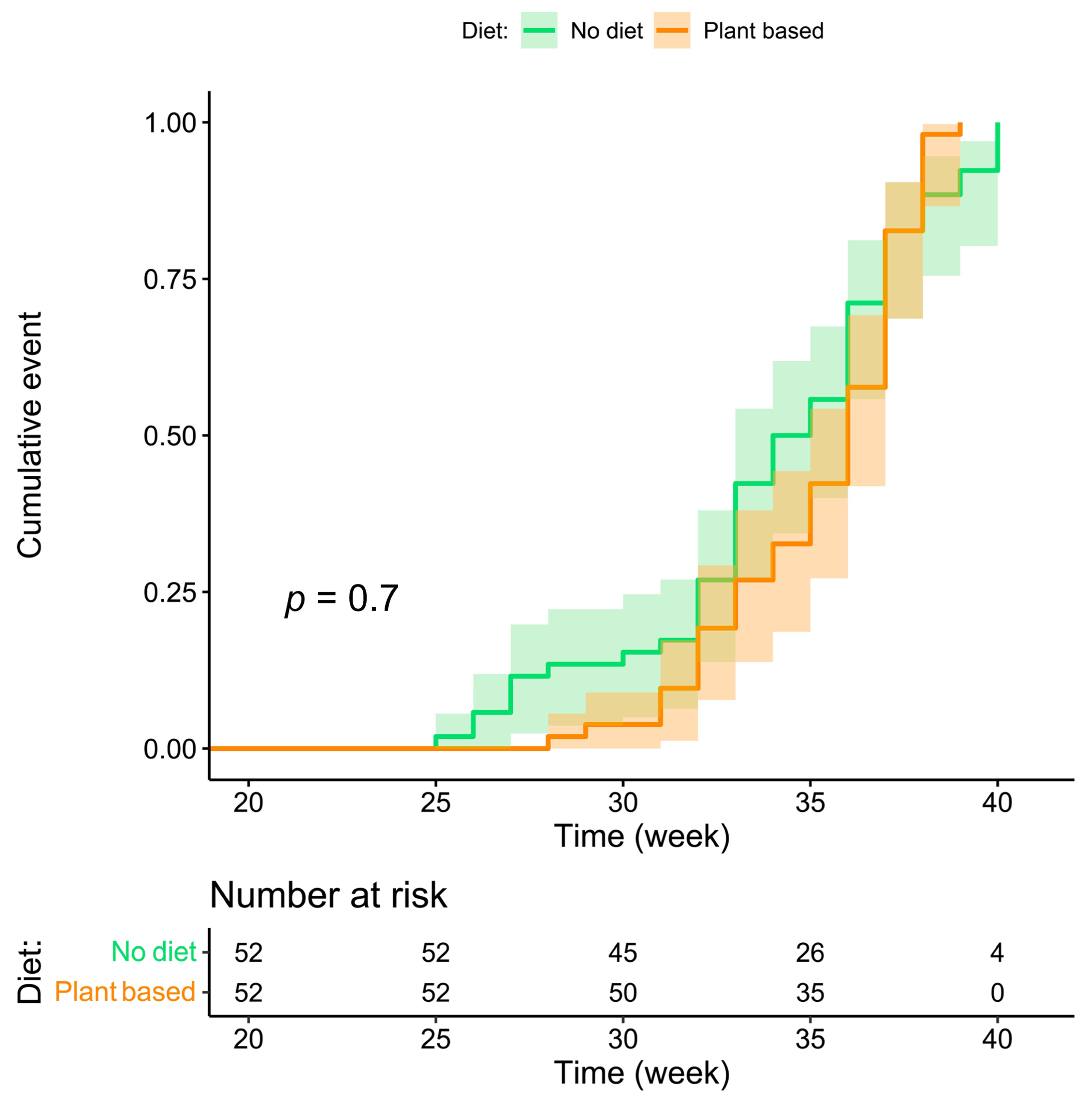
| Week of delivery, median [Q1–Q3] | 36 [33–37] | 34.5 [32–37] | 36 [33–37] | 0.164 |
| Term ≥ 37 gw, n (%) | 37 (35.58%) | 15 (28.85%) | 22 (42.31%) | 0.152 |
| Term < 34 gw, n (%) | 36 (34.62%) | 22 (42.31%) | 14 (26.92%) | 0.099 |
| Term < 32 gw, n (%) | 14 (13.46%) | 9 (17.31%) | 5 (9.62%) | 0.250 |
| Term < 28 gw, n (%) | 6 (5.77%) | 6 (11.54%) | 0 | 0.012 |
| Offspring data | ||||
| Weight at delivery, median [Q1–Q3] | 2380 [1797–2820] | 2350 [1737.5–2727.5] | 2537.5 [1957.5–2872.5] | 0.254 |
| Weight < 2500 g, n (%) | 54 (51.92%) | 29 (55.77%) | 25 (48.08%) | 0.432 |
| Weight < 1500 g, n (%) | 15 (14.42%) | 10 (19.23%) | 5 (9.62%) | 0.163 |
| Centile, median [Q1–Q3] | 36.30 [9.45–59.03] | 32.84 [6.29–57.33] | 38.81 [14.74–62.08] | 0.270 |
| Centile < 10, n (%) | 28 (26.92%) | 18 (34.62%) | 10 (19.23) | 0.077 |
| Centile < 5, n (%) | 19 (18.27%) | 12 (23.08%) | 7 (13.46%) | 0.205 |
| Pregnancy-related outcomes | ||||
| PE, n (%) | 3 (2.89%) | 3 (5.77) | 0 | 0.079 |
| Combined outcomes | ||||
| Term < 37 gw or Centile < 10, n (%) | 74 (71.15%) | 42 (80.77%) | 32 (61.54%) | 0.030 |
| Term < 34 gw or Centile < 10, n (%) | 50 (48.08%) | 29 (55.77%) | 21 (40.39%) | 0.116 |
| Term < 34 gw or Centile < 5, n (%) | 43 (41.35%) | 24 (46.15%) | 19 (36.54%) | 0.319 |
| Term < 28 gw or Centile < 5, n (%) | 20 (19.23%) | 13 (25%) | 7 (13.46%) | 0.135 |
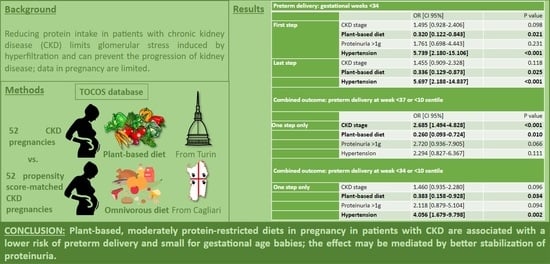
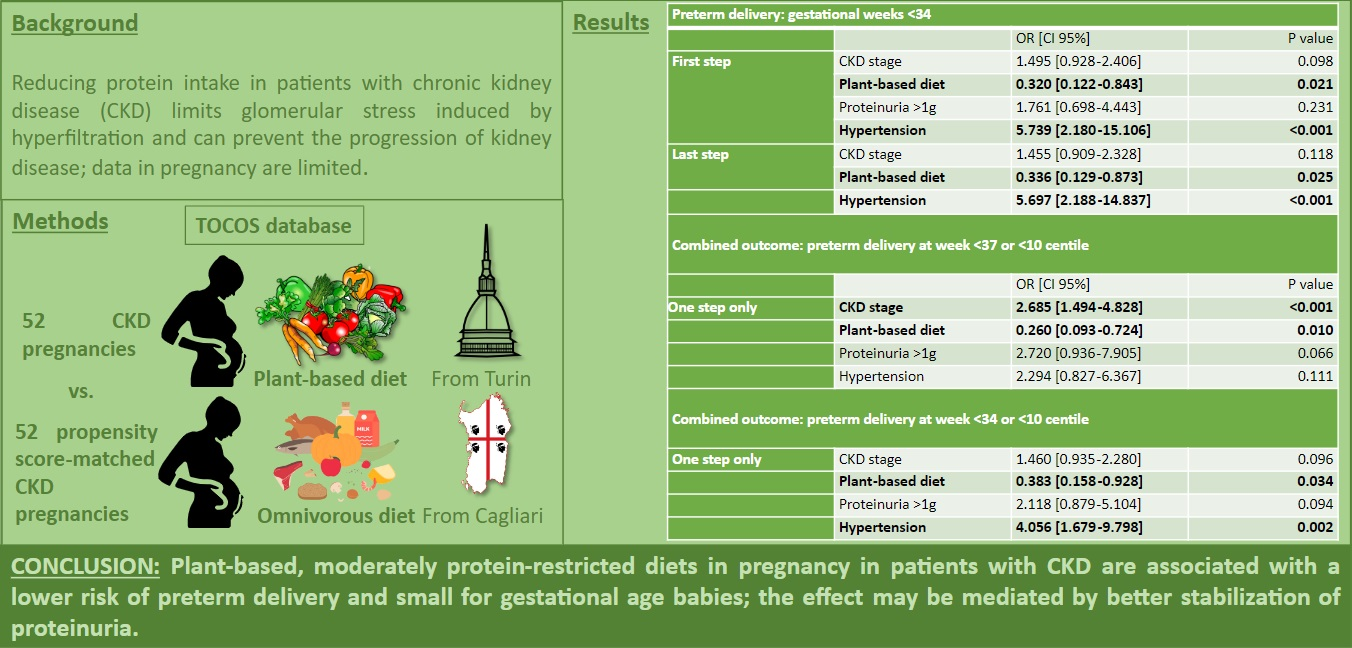
| Preterm Delivery: Gestational Weeks <34 | |||
|---|---|---|---|
| OR [CI 95%] | p Value | ||
| First step | CKD stage | 1.495 [0.928–2.406] | 0.098 |
| Plant-based diet | 0.320 [0.122–0.843] | 0.021 | |
| Proteinuria > 1 g | 1.761 [0.698–4.443] | 0.231 | |
| Hypertension | 5.739 [2.180–15.106] | <0.001 | |
| Last step | CKD stage | 1.455 [0.909–2.328] | 0.118 |
| Plant-based diet | 0.336 [0.129–0.873] | 0.025 | |
| Hypertension | 5.697 [2.188–14.837] | <0.001 | |
| Combined Outcome: Preterm Delivery at Week <37 or <10 Centile | |||
| OR [CI 95%] | p value | ||
| One step only | CKD stage | 2.685 [1.494–4.828] | <0.001 |
| Plant-based diet | 0.260 [0.093–0.724] | 0.010 | |
| Proteinuria > 1 g | 2.720 [0.936–7.905] | 0.066 | |
| Hypertension | 2.294 [0.827–6.367] | 0.111 | |
| Combined Outcome: Preterm Delivery at Week <34 or <10 Centile | |||
| One step only | CKD stage | 1.460 [0.935–2.280] | 0.096 |
| Plant-based diet | 0.383 [0.158–0.928] | 0.034 | |
| Proteinuria > 1 g | 2.118 [0.879–5.104] | 0.094 | |
| Hypertension | 4.056 [1.679–9.798] | 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Attini, R.; Leone, F.; Chatrenet, A.; Longhitano, E.; Casula, V.; Tomasi Cont, A.; Zaccaria, G.; Dalmasso, E.; Manzione, A.M.; Masturzo, B.; et al. Plant-Based Diets Improve Maternal–Fetal Outcomes in CKD Pregnancies. Nutrients 2022, 14, 4203. https://doi.org/10.3390/nu14194203
Attini R, Leone F, Chatrenet A, Longhitano E, Casula V, Tomasi Cont A, Zaccaria G, Dalmasso E, Manzione AM, Masturzo B, et al. Plant-Based Diets Improve Maternal–Fetal Outcomes in CKD Pregnancies. Nutrients. 2022; 14(19):4203. https://doi.org/10.3390/nu14194203
Chicago/Turabian StyleAttini, Rossella, Filomena Leone, Antoine Chatrenet, Elisa Longhitano, Viola Casula, Alice Tomasi Cont, Gaia Zaccaria, Eleonora Dalmasso, Ana Maria Manzione, Bianca Masturzo, and et al. 2022. "Plant-Based Diets Improve Maternal–Fetal Outcomes in CKD Pregnancies" Nutrients 14, no. 19: 4203. https://doi.org/10.3390/nu14194203
APA StyleAttini, R., Leone, F., Chatrenet, A., Longhitano, E., Casula, V., Tomasi Cont, A., Zaccaria, G., Dalmasso, E., Manzione, A. M., Masturzo, B., Torreggiani, M., Revelli, A., Cabiddu, G., & Piccoli, G. B. (2022). Plant-Based Diets Improve Maternal–Fetal Outcomes in CKD Pregnancies. Nutrients, 14(19), 4203. https://doi.org/10.3390/nu14194203