

Impact of COVID-19 Lockdown on Food Consumption and Behavior in France (COVISTRESS Study)

 , ,
, ,  , ,
, , 
 and
and
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Study Design and Setting
2.3. Variables
2.4. Statistical Analyses
3. Results
3.1. Participants
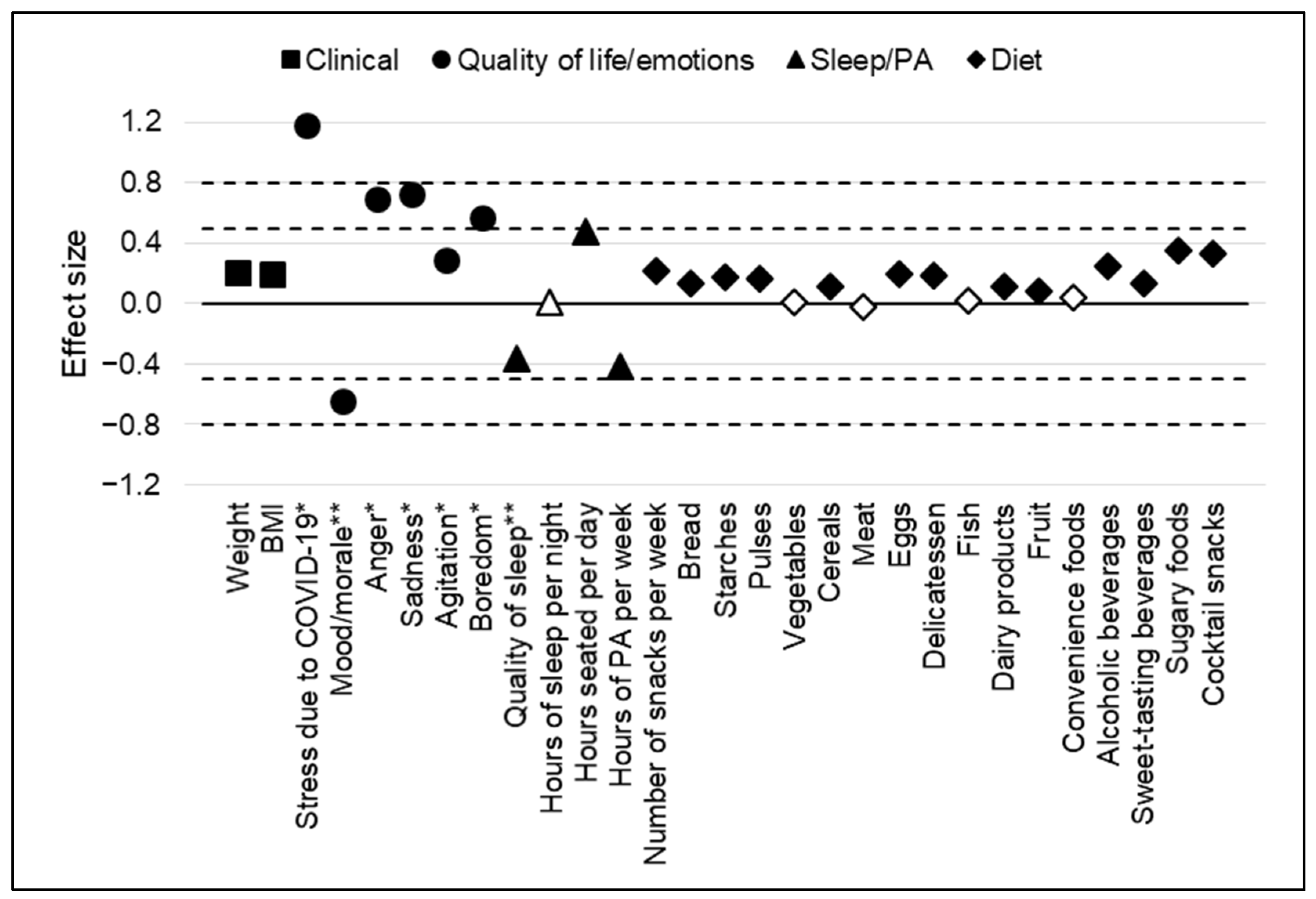
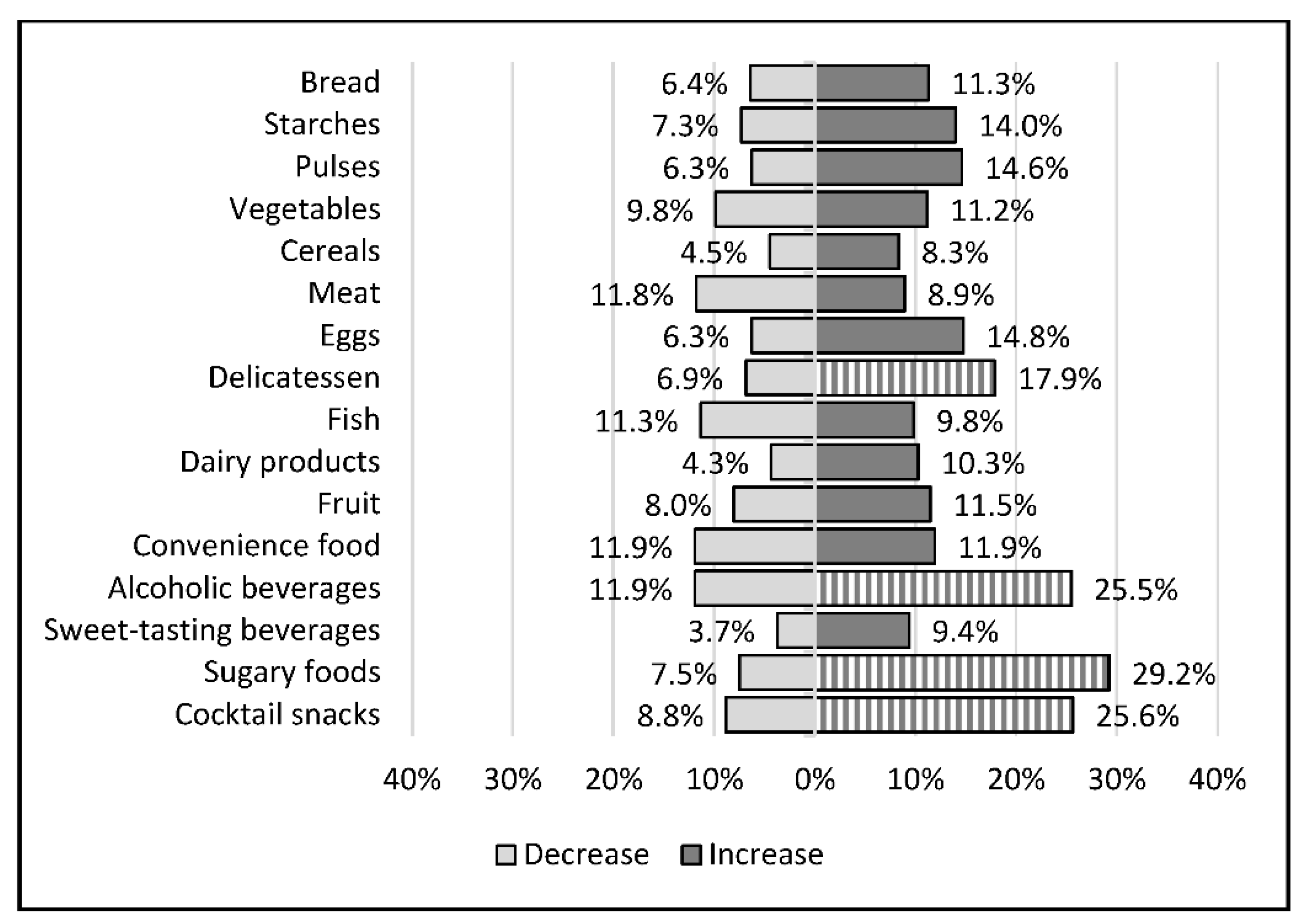
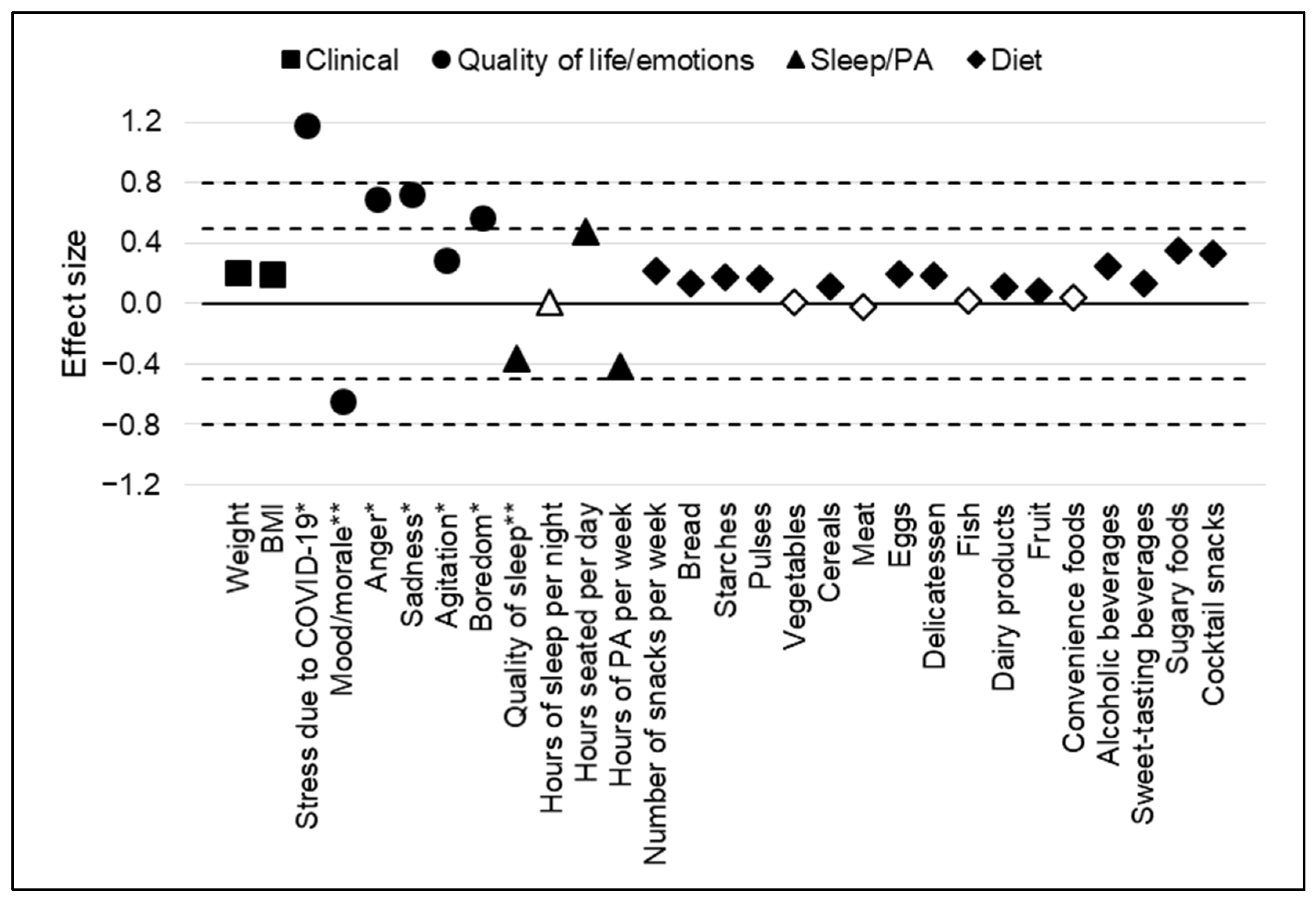
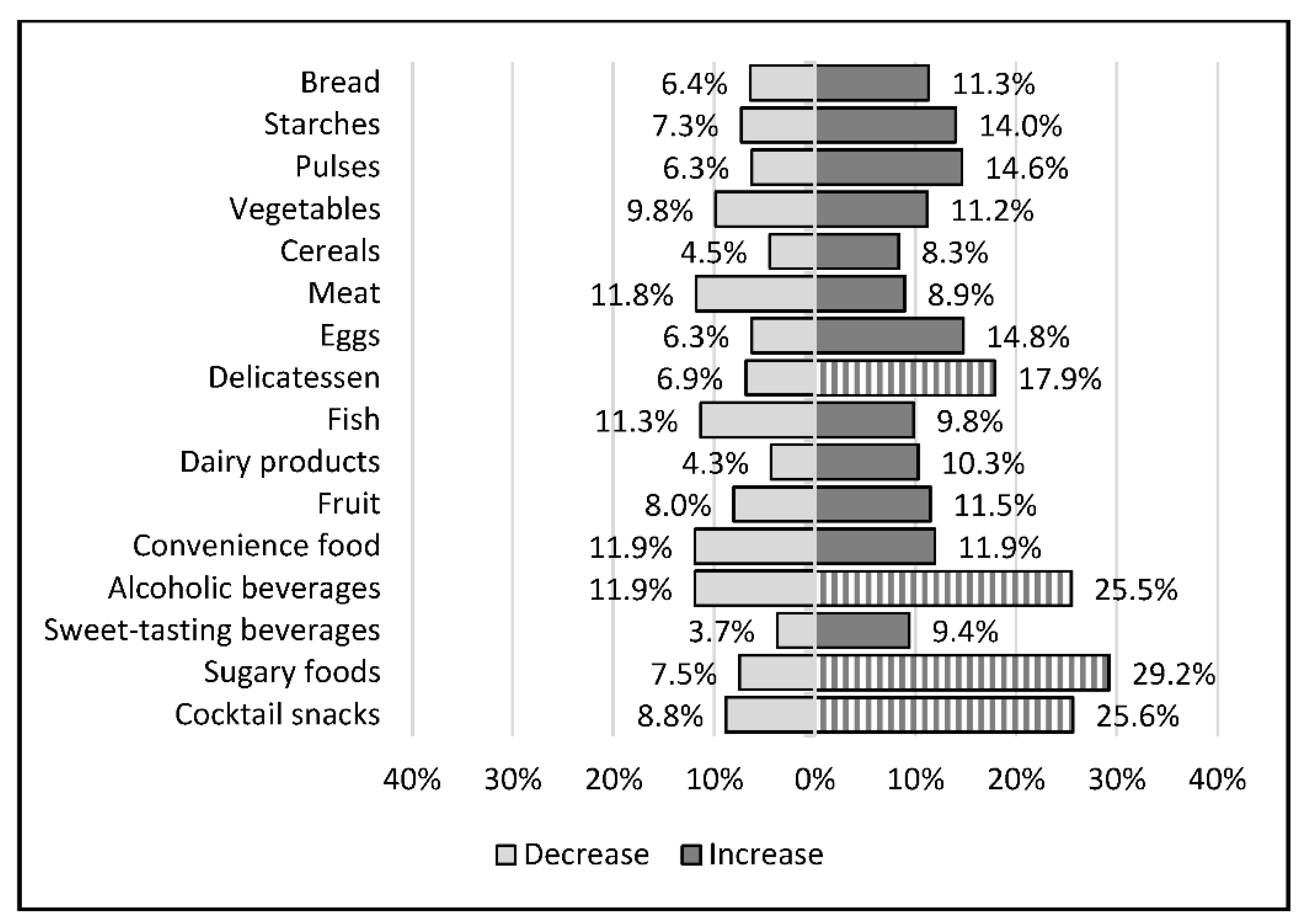
3.2. Change in Eating Habits during the First Lockdown
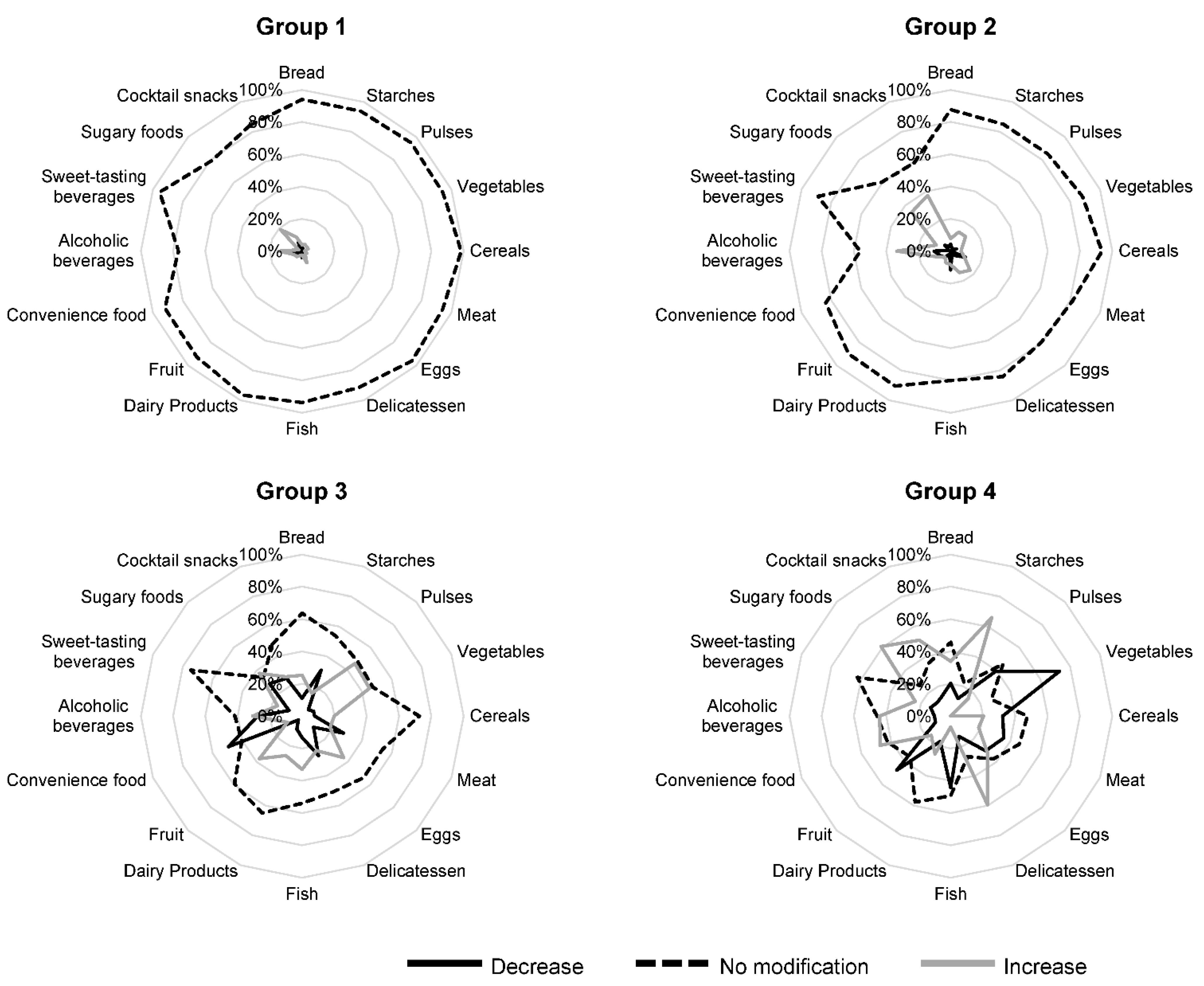
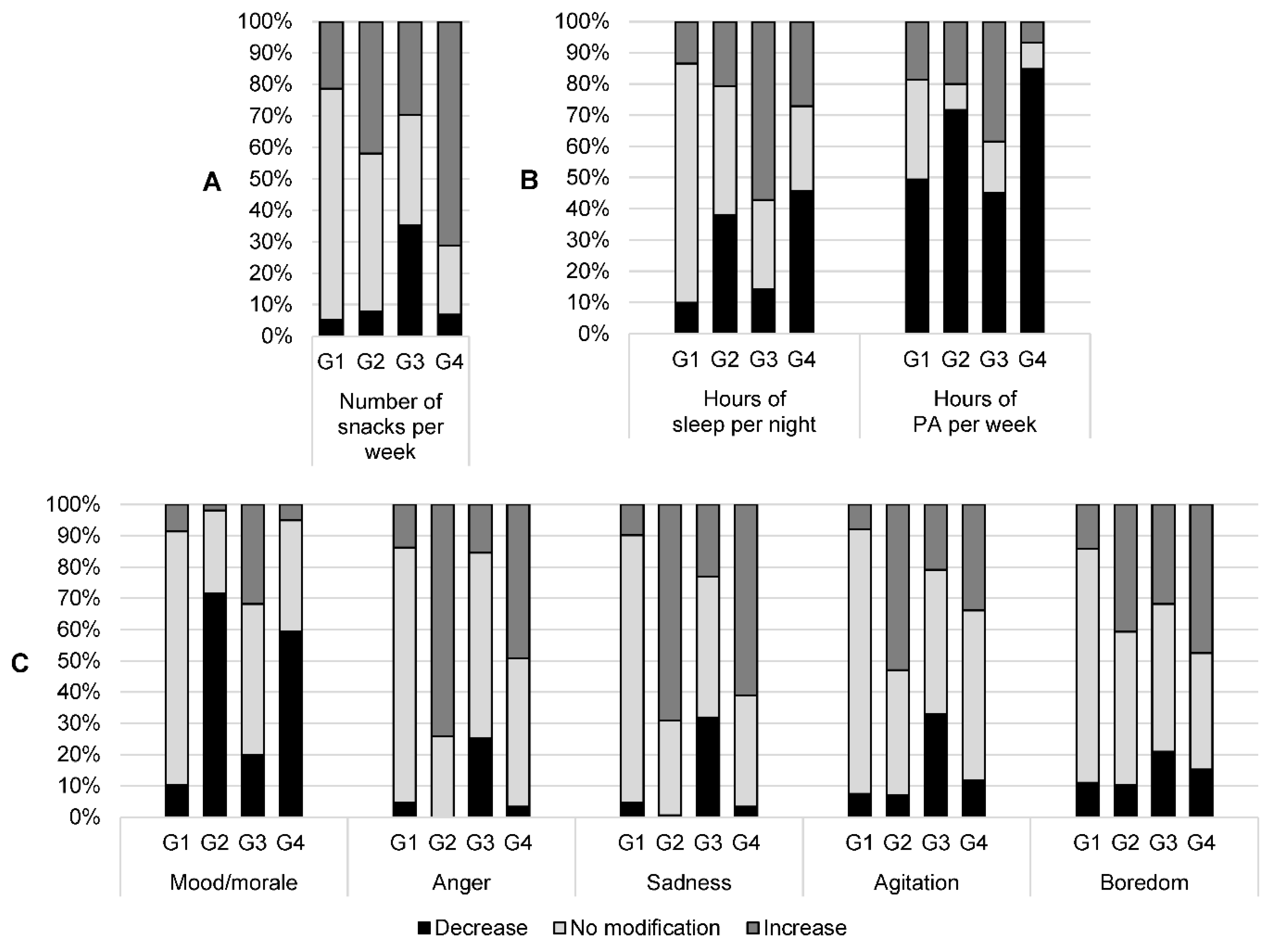
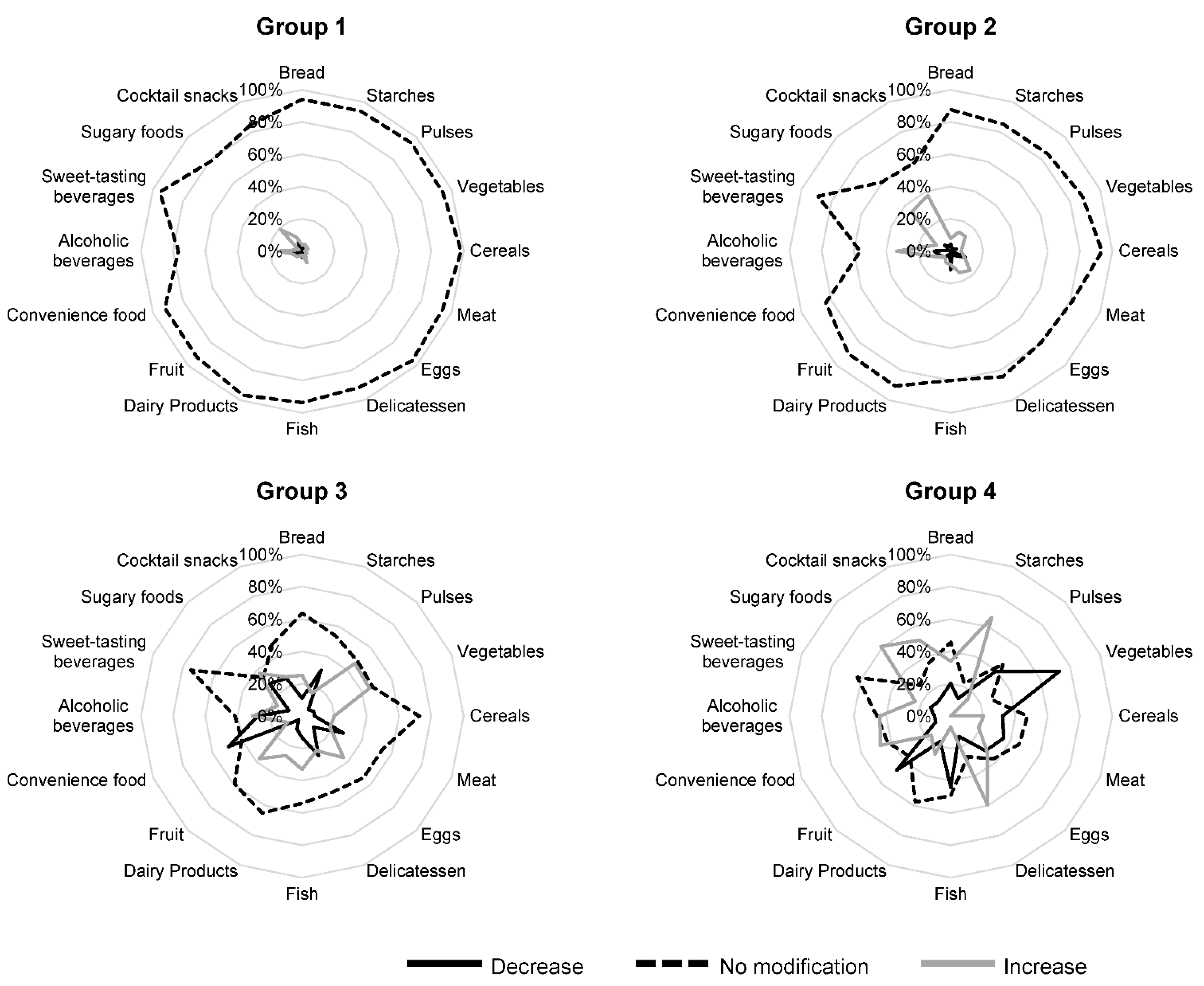
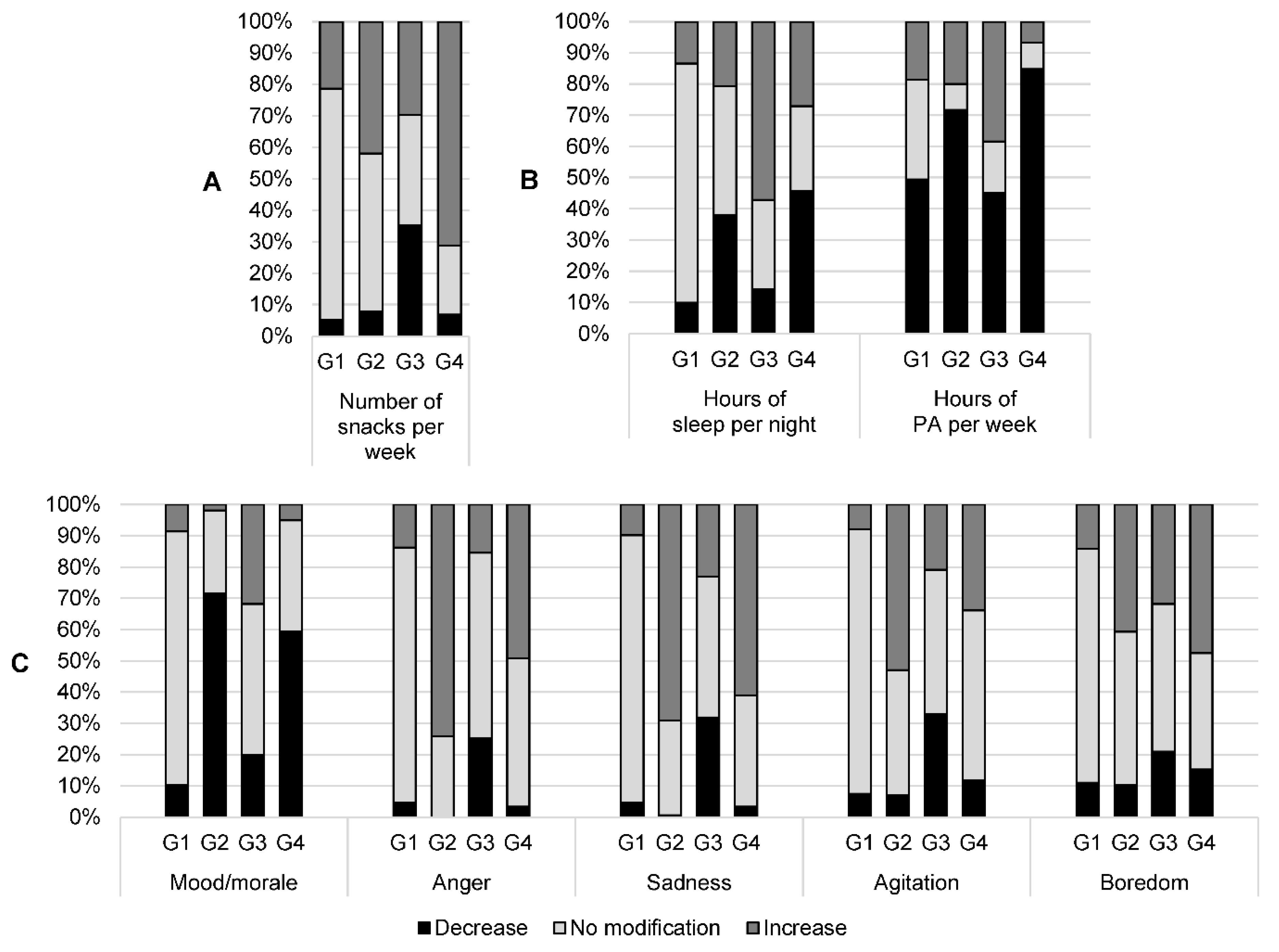
3.3. Multiple-Correspondence Analysis
4. Discussion
4.1. Change in Eating Habits during the First Lockdown
4.2. Specific Profiles of Patients during the First Lockdown
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. Severe Acute Respiratory Syndrome-Related Coronavirus: The Species and Its Viruses—A Statement of the Coronavirus Study Group. bioRxiv 2020. [Google Scholar] [CrossRef]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Coronavirus Disease-2019 (COVID-19): The Epidemic and the Challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 Outbreak: Changes in Diet and Physical Activity Increase the Risk of Cardiovascular Disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef] [PubMed]
- Covid-19: Une Enquête Pour Suivre L’évolution des Comportements et de la Santé Mentale Pendant l’épidémie. Available online: https://www.santepubliquefrance.fr/etudes-et-enquetes/coviprev-une-enquete-pour-suivre-l-evolution-des-comportements-et-de-la-sante-mentale-pendant-l-epidemie-de-covid-19 (accessed on 22 September 2020).
- Marty, L.; de Lauzon-Guillain, B.; Labesse, M.; Nicklaus, S. Food Choice Motives and the Nutritional Quality of Diet during the COVID-19 Lockdown in France. Appetite 2021, 157, 105005. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and Physical Activity during the Coronavirus Disease 2019 (COVID-19) Lockdown (March-May 2020): Results from the French NutriNet-Santé Cohort Study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Casas, R.; Raidó-Quintana, B.; Ruiz-León, A.M.; Castro-Barquero, S.; Bertomeu, I.; Gonzalez-Juste, J.; Campolier, M.; Estruch, R. Changes in Spanish Lifestyle and Dietary Habits during the COVID-19 Lockdown. Eur. J. Nutr. 2022, 61, 2417–2434. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Flaudias, V.; Iceta, S.; Zerhouni, O.; Rodgers, R.F.; Billieux, J.; Llorca, P.-M.; Boudesseul, J.; de Chazeron, I.; Romo, L.; Maurage, P.; et al. COVID-19 Pandemic Lockdown and Problematic Eating Behaviors in a Student Population. J. Behav. Addict. 2020, 9, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Grabe, S.; Ward, L.M.; Hyde, J.S. The Role of the Media in Body Image Concerns among Women: A Meta-Analysis of Experimental and Correlational Studies. Psychol. Bull. 2008, 134, 460–476. [Google Scholar] [CrossRef] [PubMed]
- Boudesseul, J.; Zerhouni, O.; Brunault, P.; Flaudias, V. En Perturbant Nos Émotions, Le Confinement Risque de Favoriser Les Troubles Alimentaires. Available online: http://theconversation.com/en-perturbant-nos-emotions-le-confinement-risque-de-favoriser-les-troubles-alimentaires-136633 (accessed on 22 September 2020).
- Bemanian, M.; Mæland, S.; Blomhoff, R.; Rabben, Å.K.; Arnesen, E.K.; Skogen, J.C.; Fadnes, L.T. Emotional Eating in Relation to Worries and Psychological Distress Amid the COVID-19 Pandemic: A Population-Based Survey on Adults in Norway. Int. J. Environ. Res. Public Health 2021, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, E2152. [Google Scholar] [CrossRef] [PubMed]
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-Quarantine and Weight Gain Related Risk Factors during the COVID-19 Pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the First COVID-19 Lockdown on Body Weight: A Combined Systematic Review and a Meta-Analysis. Clin. Nutr. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; vanDellen, M.R.; Cooper, J.A. Longitudinal Weight Gain and Related Risk Behaviors during the COVID-19 Pandemic in Adults in the US. Nutrients 2021, 13, 671. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 671) | |
|---|---|
| Age (years) | 47 ± 13 |
| Female sex | 494 (74) |
| Weight (kg) | 67 [58; 80] |
| BMI (kg/m²) | 23.5 [20.8; 26.9] |
| Employment status | |
| Executive and higher intellectual occupation | 230 (34) |
| Intermediate occupation | 130 (19) |
| Farmer | 4 (1) |
| Artisan, merchant, or entrepreneur | 48 (7) |
| Worker or employee | 109 (16) |
| Student | 24 (4) |
| Job seeker | 39 (6) |
| Retired | 69 (10) |
| MD | 18 (3) |
| Highest educational qualification | |
| School leaving certificate or under | 5 (1) |
| Youth/vocational training | 46 (7) |
| High school graduation | 69 (10) |
| 1st- to 3rd-year university level | 256 (38) |
| 5th-year university level: master 2, MDE, or other | 135 (20) |
| Over 5th year of university level: doctorate or other | 155 (23) |
| MD | 5 (1) |
| Type of housing | |
| House | 431 (64) |
| Flat | 207 (31) |
| MD | 33 (5) |
| Garden | |
| No | 419 (62) |
| Yes | 233 (35) |
| MD | 19 (3) |
| Household composition | |
| 1 person | 128 (19) |
| 2 persons | 181 (27) |
| 3 persons | 143 (21) |
| 4 persons | 106 (16) |
| 5 persons | 52 (8) |
| 6 persons | 14 (2) |
| >6 persons | 6 (1) |
| MD | 41 (6) |
| Pre-Lockdown (n = 671) | During the First Lockdown (n = 671) | |
|---|---|---|
| Weight (kg) | 67 [58; 80] | 67 [58; 80] |
| BMI (kg/m²) | 23.5 [20.8; 26.9] | 23.8 [20.8; 27.5] |
| How do you describe your diet? a | 74 [50; 87] | 73 [50; 88] |
| For you, eating is: b | ||
| Essential for living | 96 [78; 100] | 97 [79; 100] |
| Useful for maintaining health | 97 [82; 100] | 97 [83; 100] |
| A pleasure | 96 [79; 100] | 95 [76; 100] |
| A moment of sharing | 97 [80; 100] | 88 [50; 99] |
| A constraint | 5 [1; 23] | 5 [1; 25] |
| Hours of sleep per night (n = 667/667) | 7 [7; 8] | 7 [6; 8] |
| Number of snacks per week (n = 655/644) | 2 [0; 3] | 2 [0; 4] |
| Do you consider that you have a problem b | ||
| With your weight? (n = 665/662) | 42 [4; 68] | 50 [5; 73] |
| With your diet? (n = 661/660) | 22 [3; 50] | 30 [4; 64] |
| What is your level of: | ||
| Stress due to COVID-19 c (n = 641/641) | 3 [0; 18] | 64 [23; 86] |
| Quality of sleep d (n = 631/638) | 70 [48; 94] | 50 [27; 83] |
| Mood/morale d (n = 637/640) | 78 [50; 92] | 50 [30; 76] |
| Number of cigarettes per day (n = 670/668) | 0 [0; 0] | 0 [0; 0] |
| Number of drinks (alcohol) per week (n = 670/667) | 2.5 [0.0; 2.5] | 2.5 [0.0; 2.5] |
| Number of cannabis uses per week (n = 671/670) | 0 [0; 0] | 0 [0; 0] |
| Number of hours seated per day (n = 647/647) | 5 [3; 8] | 7 [4; 9] |
| Number of hours of physical activity per week (n = 643/643) | 3.5 [2.0; 6.0] | 2.0 [0.5; 5.0] |
| Number of minutes per day using social media | ||
| 0 | 96 (15) | 85 (13) |
| 1 to 60 | 336 (52) | 212 (33) |
| >60 | 215 (33) | 349 (54) |
| Emotions felt c | ||
| Anger (n = 626/638) | 31 [16; 50] | 56 [39; 76] |
| Sadness (n = 627/634) | 28 [16; 50] | 50 [34; 72] |
| Agitation (n = 624/632) | 43 [20; 50] | 50 [25; 66] |
| Boredom (n = 635/642) | 14 [3; 29] | 32 [7; 60] |
| G1 (n = 253) | G2 (n = 155) | G3 (n = 91) | G4 (n = 59) | p | |
|---|---|---|---|---|---|
| Age (years) | <0.001 | ||||
| 18 to 29 | 34 (13) | 9 (6) | 22 (24) | 8 (14) | |
| 30 to 44 | 65 (26) | 49 (32) | 33 (36) | 20 (34) | |
| 45 to 59 | 107 (42) | 56 (36) | 28 (31) | 24 (41) | |
| 60 to 78 | 47 (19) | 41 (26) | 8 (9) | 7 (12) | |
| Female sex | 159 (63) | 140 (90) | 67 (74) | 49 (83) | <0.001 |
| BMI (kg/m²) | <0.001 | ||||
| <25 | 159 (63) | 117 (75) | 47 (52) | 29 (49) | |
| 25 to 30 | 61 (24) | 15 (10) | 24 (26) | 22 (37) | |
| ≥30 | 33 (13) | 23 (15) | 20 (22) | 8 (14) | |
| Smoking | 42 (17) | 18 (12) | 18 (20) | 12 (20) | 0.25 |
| Employment status | 0.02 | ||||
| Executive and superior intellectual occupation | 100 (40) | 55 (35) | 24 (26) | 20 (34) | |
| Intermediate occupation | 35 (14) | 36 (23) | 22 (24) | 12 (20) | |
| Artisan, merchant, or entrepreneur | 16 (6) | 14 (9) | 10 (11) | 3 (5) | |
| Worker or employee | 55 (22) | 13 (8) | 17 (19) | 10 (17) | |
| Unemployed a | 47 (19) | 37 (24) | 18 (20) | 14 (24) | |
| Type of housing | <0.001 | ||||
| House | 189 (75) | 107 (69) | 51 (56) | 28 (47) | |
| Flat | 64 (25) | 48 (31) | 40 (44) | 31 (53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouget, M.; Clinchamps, M.; Lambert, C.; Pereira, B.; Farigon, N.; Gentes, E.; Miolanne, M.; Picard, M.; Tyrode, A.; Alligier, M.; et al. Impact of COVID-19 Lockdown on Food Consumption and Behavior in France (COVISTRESS Study). Nutrients 2022, 14, 3739. https://doi.org/10.3390/nu14183739
Pouget M, Clinchamps M, Lambert C, Pereira B, Farigon N, Gentes E, Miolanne M, Picard M, Tyrode A, Alligier M, et al. Impact of COVID-19 Lockdown on Food Consumption and Behavior in France (COVISTRESS Study). Nutrients. 2022; 14(18):3739. https://doi.org/10.3390/nu14183739
Chicago/Turabian StylePouget, Mélanie, Maëlys Clinchamps, Céline Lambert, Bruno Pereira, Nicolas Farigon, Elodie Gentes, Magalie Miolanne, Mathilde Picard, Anne Tyrode, Maud Alligier, and et al. 2022. "Impact of COVID-19 Lockdown on Food Consumption and Behavior in France (COVISTRESS Study)" Nutrients 14, no. 18: 3739. https://doi.org/10.3390/nu14183739
APA StylePouget, M., Clinchamps, M., Lambert, C., Pereira, B., Farigon, N., Gentes, E., Miolanne, M., Picard, M., Tyrode, A., Alligier, M., COVISTRESS Network, Dutheil, F., & Boirie, Y. (2022). Impact of COVID-19 Lockdown on Food Consumption and Behavior in France (COVISTRESS Study). Nutrients, 14(18), 3739. https://doi.org/10.3390/nu14183739