
Emotional Eating and Perfectionism as Predictors of Symptoms of Binge Eating Disorder: The Role of Perfectionism as a Mediator between Emotional Eating and Body Mass Index


Abstract
:1. Introduction
- To confirm the association between BMI, symptoms of EE, BE, and perfectionism.
- To determine the factors that influence BMI and symptoms of BE.
- To investigate how perfectionism affects both EE and BMI.
Method
Participants and Procedure
2. Materials and Methods
3. Results
3.1. Correlation Analysis between Variables
3.2. Predictive Models of BMI and EE Symptoms
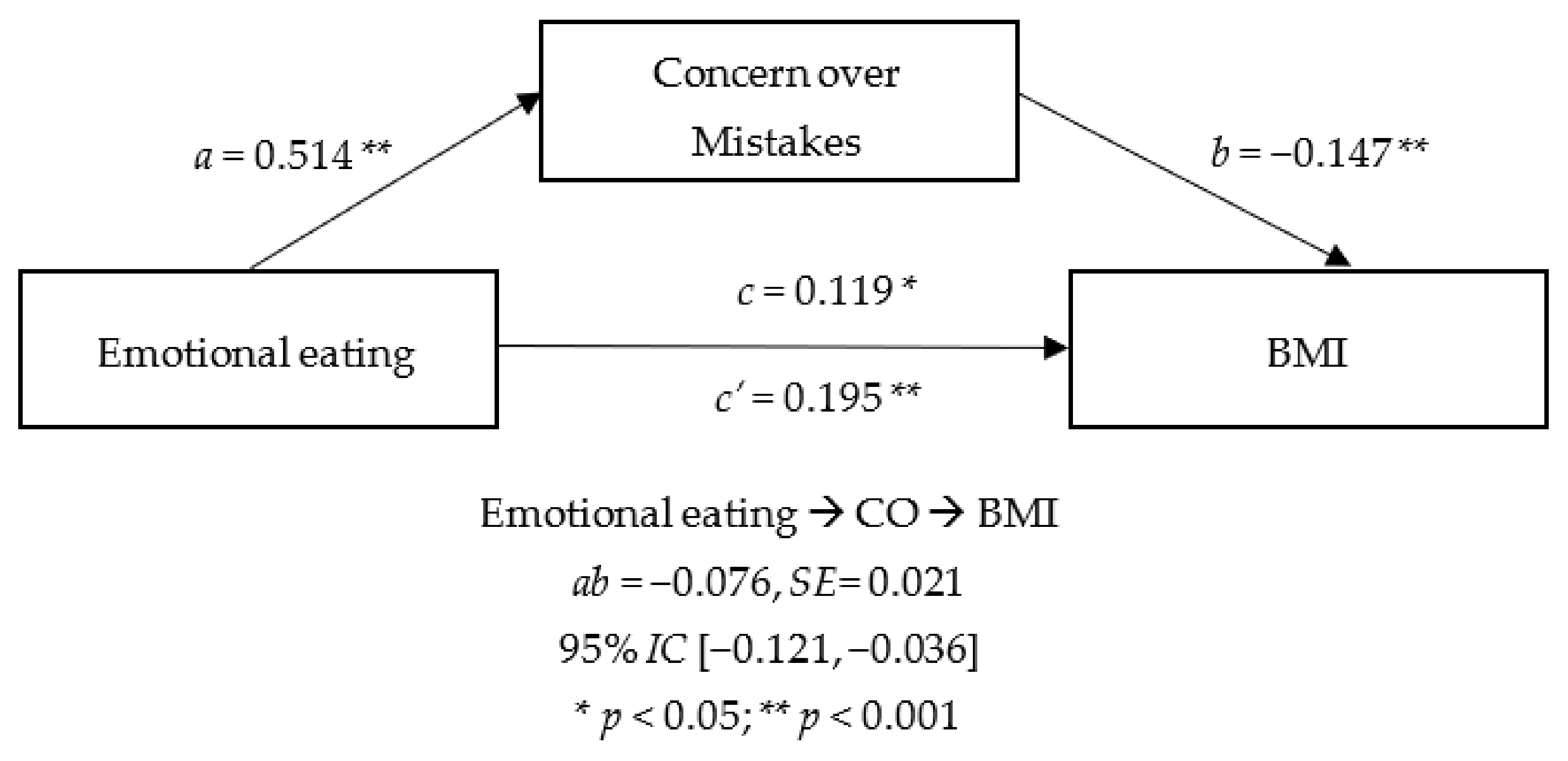
3.3. Mediator Effect of Perfectionism between Emotional Eating and BMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frost, R.O.; Marten, P.; Lahart, C.; Rosenblate, R. The dimensions of perfectionism. Cogn. Ther. Res. 1990, 14, 449–468. [Google Scholar] [CrossRef]
- O’Connor, R.C.; O’Connor, D.B. Predicting hopelessness and psychological distress: The role of perfectionism and coping. J. Couns. Psychol. 2003, 50, 362–372. [Google Scholar] [CrossRef]
- Rice, K.G.; Leever, B.A.; Christopher, J.; Porter, J.D. Perfectionism, stress, and social (dis)connection: A short-term study of hopelessness, depression, and academic adjustment among honors students. J. Couns. Psychol. 2006, 53, 524–534. [Google Scholar] [CrossRef]
- Kawamura, K.Y.; Hunt, S.L.; Frost, R.O.; DiBartolo, P.M. Perfectionism, anxiety, and depression: Are the relationships independent? Cogn. Ther. Res. 2001, 25, 291–301. [Google Scholar] [CrossRef]
- Blatt, S.J.; Bondi, C.M.; Sanislow, C.A.; Zuroff, D.C.; Pilkonis, P.A. When and how perfectionism impedes the brief treatment of depression: Further analyses of the National Institute of Mental Health Treatment of Depression Collaborative Research Program. J. Consult. Clin. Psychol. 1998, 66, 423–428. [Google Scholar] [CrossRef]
- Bardone-Cone, A.M.; Wonderlich, S.A.; Frost, R.O.; Bulik, C.M.; Mitchell, J.E.; Uppala, S.; Simonich, H. Perfectionism and eating disorders: Current status and future directions. Clin. Psychol. Rev. 2007, 27, 384–405. [Google Scholar] [CrossRef]
- Lilenfeld, L.R.R.; Stein, D.; Bulik, C.M.; Strober, M.; Plotnicov, K.; Pollice, C.; Rao, R.; Merikangas, K.R.; Nagy, L.; Kaye, W.H. Personality traits among currently eating disordered, recovered and never ill first-degree female relatives of bulimic and control women. Psychol. Med. 2000, 30, 1399–1410. [Google Scholar] [CrossRef]
- Sutandar-Pinnock, K.; Woodside, D.B.; Carter, J.C.; Olmsted, M.P.; Kaplan, A.S. Perfectionism in anorexia nervosa: A 6-24-month follow-up study. Int. J. Eat. Disord. 2003, 33, 225–229. [Google Scholar] [CrossRef]
- Moor, S.; Vartanian, L.R.; Touyz, S.W.; Beumont, P. Psychopathology of EDNOS patients: To whom do they compare? Clin. Psychol. 2004, 8, 70–75. [Google Scholar] [CrossRef]
- Stice, E. Risk and maintenance factors for eating pathology: A meta-analytic review. Psychol. Bull. 2002, 128, 825–848. [Google Scholar] [CrossRef]
- Vohs, K.D.; Joiner, T.E.; Bardone, A.M.; Abramson, L.Y.; Heatherton, T.F. Perfectionism, perceived weight status, and self-esteem interact to predict bulimic symptoms: A model of bulimic symptom development. J. Abnorm. Psychol. 1999, 108, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Brosof, L.C.; Vanzhula, I.A.; Bumberry, L.; Zerwas, S.; Bulik, C.M. Perfectionism Group Treatment for Eating Disorders in an Inpatient, Partial Hospitalization, and Outpatient Setting. Eur. Eat. Disord. Rev. 2017, 25, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Lilenfeld, L.R.R.; Wonderlich, S.; Riso, L.P.; Crosby, R.; Mitchell, J. Eating disorders and personality: A methodological and empirical review. Clin. Psychol. Rev. 2006, 26, 299–320. [Google Scholar] [CrossRef] [PubMed]
- Bastiani, A.M.; Rao, R.; Weltzin, T.; Kaye, W.H. Perfectionism in anorexia nervosa. Int. J. Eat. Disord. 1995, 17, 147–152. [Google Scholar] [CrossRef]
- Sullivan, P.F.; Bulik, C.M.; Fear, J.L.; Pickering, A. Outcome of Anorexia Nervosa A Case-Control Study. Am. J. Psychiatry 1998, 155, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, P.L.; Flett, G.L. Perfectionism in the Self and Social Contexts: Conceptualization, Assessment, and Association with Psychopathology. J. Pers. Soc. Psychol. 1991, 60, 456–470. [Google Scholar] [CrossRef] [PubMed]
- Enns, M.W.; Cox, B.J. The nature and assessment of perfectionism: A critical analysis. In Perfectionism: Theory, Research, and Treatment; American Psychological Association: Washington, DC, USA, 2004; pp. 33–62. [Google Scholar] [CrossRef]
- Lindeman, M.; Stark, K. Emotional eating and eating disorder psychopathology. Eat. Disord. 2001, 9, 251–259. [Google Scholar] [CrossRef]
- Annesi, J.J. Psychosocial predictors of decay in healthy eating and physical activity improvements in obese women regaining lost weight: Translation of behavioral theory into treatment suggestions. Transl. Behav. Med. 2016, 6, 169–178. [Google Scholar] [CrossRef]
- Nolan, L.J.; Jenkins, S.M. Food addiction is associated with irrational beliefs via trait anxiety and emotional eating. Nutrients 2019, 11, 1711. [Google Scholar] [CrossRef]
- Milos, G.; Spindler, A.; Schnyder, U. (EDI) Profiles in Eating Disorder Patients. Can. J. Psychiatry 2004, 49, 179–184. [Google Scholar] [CrossRef]
- Fairburn, C.G.; Cooper, Z.; Shafran, R. Cognitive behaviour therapy for eating disorders: A “transdiagnostic” theory and treatment. Behav. Res. Ther. 2003, 41, 509–528. [Google Scholar] [CrossRef]
- Spoor, S.T.P.; Bekker, M.H.J.; Van Strien, T.; van Heck, G.L. Relations between negative affect, coping, and emotional eating. Appetite 2007, 48, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Van Engels, R.C.M.E.; Van Leeuwe, J.; Snoek, H.M. The Stice model of overeating: Tests in clinical and non-clinical samples. Appetite 2005, 45, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Presnell, K.; Spangler, D. Risk factors for binge eating onset in adolescent girls: A 2-year prospective investigation. Health Psychol. 2002, 21, 131–138. [Google Scholar] [CrossRef]
- Villarejo, C.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Peñas-Lledó, E.; Granero, R.; Penelo, E.; Tinahones, F.J.; Sancho, C.; Vilarrasa, N.; Montserrat-Gil De Bernabé, M.; et al. Lifetime obesity in patients with eating disorders: Increasing prevalence, clinical and personality correlates. Eur. Eat. Disord. Rev. 2012, 20, 250–254. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.A.; Chiu, W.T.; Deitz, A.C.; Hudson, J.I.; Shahly, V.; Aguilar-gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Benjet, C. The Prevalence and Correlates of Binge Eating Disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatry 2014, 73, 904–914. [Google Scholar] [CrossRef]
- Duncan, L.; Yilmaz, Z.; Walters, R.; Goldstein, J.; Anttila, V.; Bulik-Sullivan, B.; Ripke, S.; Thornton, L.; Hinney, A.; Daly, M.; et al. Genome-Wide Association Study Reveals First Locus for Anorexia Nervosa and Metabolic Correlations. Am. J. Psychiatry 2017, 174, 850–858. [Google Scholar] [CrossRef]
- Mustelin, L.; Bulik, C.M.; Kaprio, J.; Keski-Rahkonen, A. Prevalence and correlates of binge eating disorder related features in the community. Appetite 2017, 109, 165–171. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240. [Google Scholar] [CrossRef]
- Chung, Y.L.; Rhie, Y.J. Severe Obesity in Children and Adolescents: Metabolic Effects, Assessment, and Treatment. J. Obes. Metab. Syndr. 2021, 30, 326–335. [Google Scholar] [CrossRef]
- Tachikawa, H.; Yamaguchi, N.; Hatanaka, K.; Kobayashi, J.; Sato, S.; Mizumaki, K.; Asada, T.; Sugie, M. The Eating Disorder Inventory-2 in Japanese clinical and non-clinicalsamples: Psychometric properties and cross-cultural implications. Eat. Weight Disord. 2004, 9, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Doll, H.A.; Welch, S.L.; Hay, P.J.; Davies, B.A.; O’Connor, M.E. Risk Factors for Binge Eating Disorder. Arch. Gen. Psychiatry 1998, 55, 425. [Google Scholar] [CrossRef] [PubMed]
- Forbush, K.T.; Heatherton, T.F.; Keel, P. Relationships Between Perfectionism and Specific Disordered Eating Behaviors. Int. J. Eat. Disord. 2007, 40, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Fitzsimmons-Craft, E.E.; Bardone-Cone, A.M.; Brownstone, L.M.; Harney, M.B. Evaluating the roles of anxiety and dimensions of perfectionism in dieting and binge eating using weekly diary methodology. Eat. Behav. 2012, 13, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Garaulet, M.; Canteras, M.; Morales, E.; López-Guimera, G.; Sánchez-Carracedo, D.; Corbalán-Tutau, M.D. Validation of a questionnaire on emotional eating for use in cases of obesity: The Emotional Eater Questionnaire (EEQ). Nutr. Hosp. 2012, 27, 645–651. [Google Scholar] [CrossRef]
- Bernabéu, E.; Marchena, C.; Iglesias, M.T. Factor Structure and Psychometric Properties of Emotional Eater Questionnaire (EEQ) in Spanish Colleges. Int. J. Environ. Res. Public Health 2020, 17, 9090. [Google Scholar] [CrossRef]
- Frost, R.O.; Marten, P.A. Perfectionism and evaluative threat. Cogn. Ther. Res. 1990, 14, 559–572. [Google Scholar] [CrossRef]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Escrivá-Martínez, T.; Galiana, L.; Rodríguez-Arias, M.; Baños, R.M. The binge eating scale: Structural equation competitive models, invariance measurement between sexes, and relationships with food addiction, impulsivity, binge drinking, and body mass index. Front. Psychol. 2019, 10, 530. [Google Scholar] [CrossRef]
- Hawkins, C.C.; Watt, H.M.G.; Sinclair, K.E. Psychometric properties of the frost multidimensional perfectionism scale with Australian adolescent girls: Clarification of multidimensionality and perfectionist typology. Educ. Psychol. Meas. 2006, 66, 1001–1022. [Google Scholar] [CrossRef]
- Yahghoubi, H.; Mohammadzadeh, A. Comparison of perfectionism and related positive-negative dimension in people with high traits on obsessive compulsive and eating disorder characteristics. Iran. J. Psychiatry Behav. Sci. 2015, 9, e264. [Google Scholar] [CrossRef] [PubMed]
- Péneau, S.; Ménard, E.; Méjean, C.; Bellisle, F.; Hercberg, S. Sex and dieting modify the association between emotional eating and weight status. Am. J. Clin. Nutr. 2013, 97, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, B.A.; Cassin, S.E. Disordered Eating Among Individuals with Excess Weight: A Review of Recent Research. Curr. Obes. Rep. 2019, 8, 112–127. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, H.; Van Strien, T.; Männistö, S.; Jousilahti, P.; Haukkala, A. Depression, emotional eating and long-term weight changes: A population-based prospective study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 28. [Google Scholar] [CrossRef] [PubMed]
- Frayn, M.; Knäuper, B. Emotional Eating and Weight in Adults: A Review. Curr. Psychol. 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Bulik, C.M.; Tozzi, F.; Anderson, C.; Mazzeo, S.E.; Aggen, S.; Sullivan, P.F. The relation between eating disorders and components of perfectionism. Am. J. Psychiatry 2003, 160, 366–368. [Google Scholar] [CrossRef]
- Brosof, L.C.; Levinson, C.A. Social appearance anxiety and dietary restraint as mediators between perfectionism and binge eating: A six month three wave longitudinal study. Appetite 2017, 108, 335–342. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obesity and Overweight. Available online: www.who.int/%0Anews-room/fact-sheets/detail/obesity-and-overweight (accessed on 15 September 2021).
- Van Strien, T. Causes of Emotional Eating and Matched Treatment of Obesity. Curr. Diabetes Rep. 2018, 18, 35. [Google Scholar] [CrossRef]
- Koenders, P.G.; Van Strien, T. Emotional eating, rather than lifestyle behavior, drives weight gain in a prospective study in 1562 employees. J. Occup. Environ. Med. 2011, 53, 1287–1293. [Google Scholar] [CrossRef]
- Sherry, S.B.; Hewitt, P.L.; Besser, A.; McGee, B.J.; Flett, G.L. Self-Oriented and Socially Prescribed Perfectionism in the Eating Disorder Inventory Perfectionism Subscale. Int. J. Eat. Disord. 2004, 35, 69–79. [Google Scholar] [CrossRef]
- Lloyd, S.; Yiend, J.; Schmidt, U.; Tchanturia, K. Perfectionism in anorexia nervosa: Novel performance based evidence. PLoS ONE 2014, 9, 111697. [Google Scholar] [CrossRef] [PubMed]
- Sherry, S.B.; Sabourin, B.C.; Hall, P.A.; Hewitt, P.L.; Flett, G.L.; Gralnick, T.M. The perfectionism model of binge eating: Testing unique contributions, mediating mechanisms, and cross-cultural similarities using a daily diary methodology. Psychol. Addict. Behav. 2014, 28, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Yiend, J.; Savulich, G.; Coughtrey, A.; Shafran, R. Biased interpretation in perfectionism and its modification. Behav. Res. Ther. 2011, 49, 892–900. [Google Scholar] [CrossRef]
- Shafran, R.; Lee, M.; Payne, E.; Fairnburn, C. The impact of manipulating personal standards on eating attitudes and behaviour. Behav. Res. Ther. 2006, 44, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Boone, L.; Soenens, B.; Vansteenkiste, M.; Braet, C. Is there a perfectionist in each of us? An experimental study on perfectionism and eating disorder symptoms. Appetite 2012, 59, 531–540. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| n = 212 | |
|---|---|
| Mean age | 32.04 (SD = 11.86) |
| Education | |
| Without studies | 4 (1.3%) |
| Primary studies | 26 (8.3%) |
| Secondary studies | 88 (28.2%) |
| University studies | 194 (62.2%) |
| Marital status | |
| Single | 137 (43.9%) |
| With partner | 97 (31.1%) |
| Married | 69 (22.1%) |
| Separated | 9 (2.9%) |
| Employment status | |
| Student | 84 (26.9%) |
| Unemployed | 42 (13.5%) |
| Self-employed | 33 (10.6%) |
| Salaried | 153 (49.0%) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Emotional Eater | - | ||||||||
| 2. Perfectionism | 0.297 ** | ||||||||
| 3. CM | 0.411 * | 0.836 ** | |||||||
| 4. PS | 0.113 * | 0.749 ** | 0.519 ** | ||||||
| 5. PE | 0.098 | 0.676 ** | 0.395 ** | 0.37 ** | |||||
| 6. PC | 0.26 ** | 0.706 ** | 0.553 ** | 0.33 ** | 0.639 ** | ||||
| 7. DA | 0.355 ** | 0.72 ** | 0.642 ** | 0.419 ** | 0.329 ** | 0.485 ** | |||
| 8. O | −0.091 | 0.37 ** | 0.09 | 0.267** | 0.165** | 0.031 | 0.122 * | ||
| 9. Binge Eating | 0.799 ** | 0.269 ** | 0.411 ** | 0.095 | 0.036 | 0.214 ** | 0.35 ** | −0.092 | |
| 10. BMI | 0.163 ** | −0.179 ** | −0.143 * | −0.130 * | −0.084 | −0.043 | −0.246 ** | −0.092 | 0.169 ** |
| Model | Variables | β | t | R2 | ΔR | Change in F |
|---|---|---|---|---|---|---|
| 1 | Age | 0.271 | 4.96 ** | 0.074 | 0.071 ** | 24.64 |
| 2 | Age | 0.297 | 5.61 ** | 0.146 | 0.14 ** | 26.01 |
| Gender | 0.269 | 5.1 ** | ||||
| 3 | Age | 0.325 | 6.33 ** | 0.207 | 0.199 ** | 23.77 |
| Gender | 0.32 | 6.15 ** | ||||
| Emotional eater | 0.254 | 4.87 ** | ||||
| 4 | Age | 0.281 | 5.6 ** | 0.267 | 0.257 ** | 25.00 |
| Gender | 0.287 | 5.68 ** | ||||
| Emotional eater | 0.338 | 6.39 ** | ||||
| DA | −0.267 | −5.00 ** |
| Model | Variables | β | t | R2 | ΔR | Change in F |
|---|---|---|---|---|---|---|
| 1 | Emotional Eater | 0.799 | 23.38 ** | 0.638 | 0.637 ** | 546.64 |
| 2 | Emotional Eater | 0.758 | 20.42 ** | 0.646 | 0.644 ** | 7.098 |
| CM | 0.099 | 2.66 * | ||||
| 3 | Emotional Eater | 0.751 | 20.33 ** | 0.653 | 0.65 ** | 6.13 |
| CM | 0.138 | 3.44 * | ||||
| PE | −0.091 | 0.014 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernabéu-Brotóns, E.; Marchena-Giráldez, C. Emotional Eating and Perfectionism as Predictors of Symptoms of Binge Eating Disorder: The Role of Perfectionism as a Mediator between Emotional Eating and Body Mass Index. Nutrients 2022, 14, 3361. https://doi.org/10.3390/nu14163361
Bernabéu-Brotóns E, Marchena-Giráldez C. Emotional Eating and Perfectionism as Predictors of Symptoms of Binge Eating Disorder: The Role of Perfectionism as a Mediator between Emotional Eating and Body Mass Index. Nutrients. 2022; 14(16):3361. https://doi.org/10.3390/nu14163361
Chicago/Turabian StyleBernabéu-Brotóns, Elena, and Carlos Marchena-Giráldez. 2022. "Emotional Eating and Perfectionism as Predictors of Symptoms of Binge Eating Disorder: The Role of Perfectionism as a Mediator between Emotional Eating and Body Mass Index" Nutrients 14, no. 16: 3361. https://doi.org/10.3390/nu14163361
APA StyleBernabéu-Brotóns, E., & Marchena-Giráldez, C. (2022). Emotional Eating and Perfectionism as Predictors of Symptoms of Binge Eating Disorder: The Role of Perfectionism as a Mediator between Emotional Eating and Body Mass Index. Nutrients, 14(16), 3361. https://doi.org/10.3390/nu14163361