
Healthy Taiwanese Eating Approach (TEA) toward Total Wellbeing and Healthy Longevity


Abstract
:1. Introduction
2. Materials and Methods
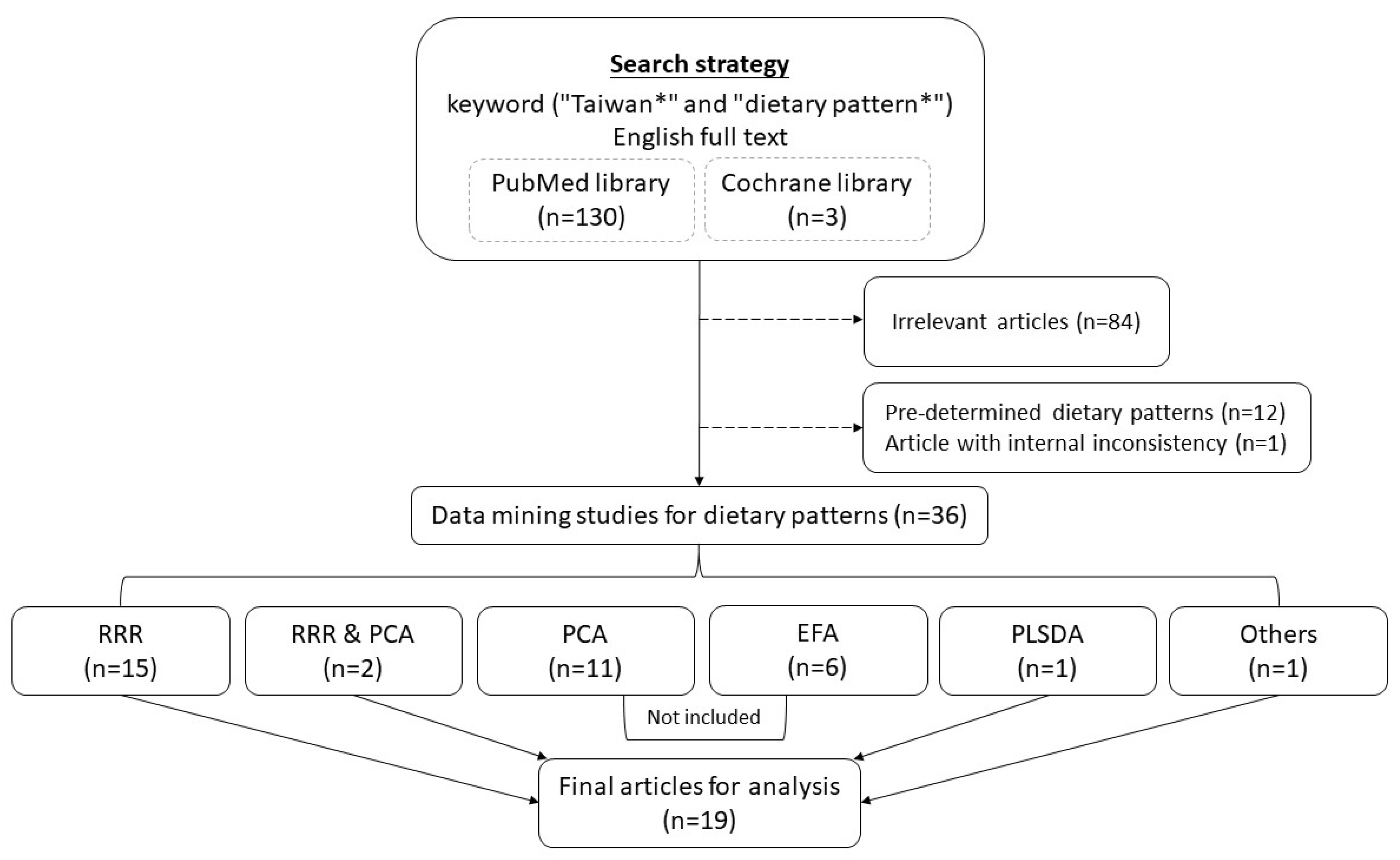
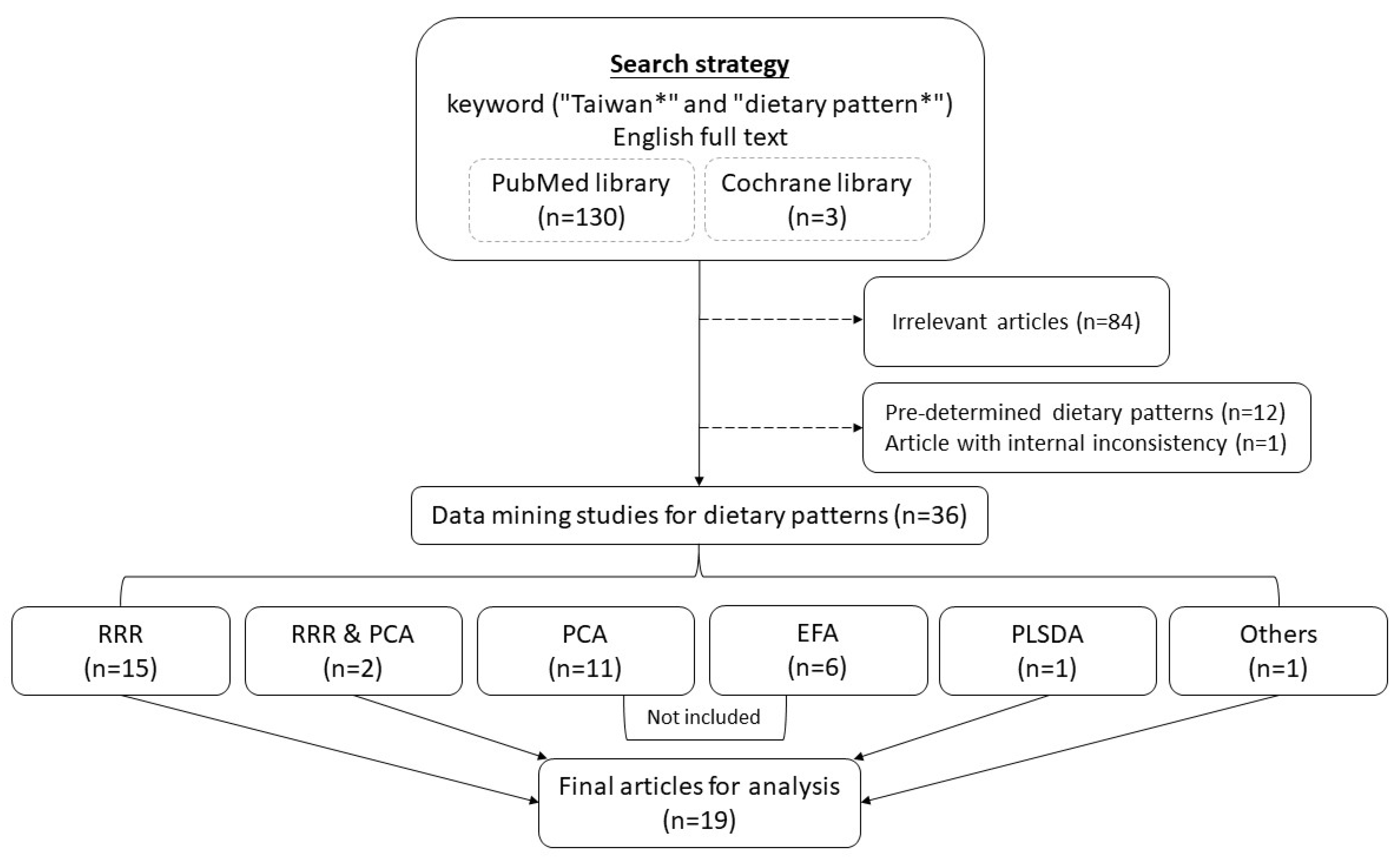
2.1. Strategy to Search Taiwanese Dietary Pattern-Related Literature
2.2. Data Summary and Presentation Method
2.3. Estimating Taiwanese Current Dietary Content
3. Results
3.1. Studied Populations and Design Characteristics of the Taiwanese Dietary Pattern Data Mining Studies
3.2. Health Outcomes of Interest of the Taiwanese Dietary Pattern Data Mining Studies
3.3. Food Items Identified as Inversely Associated with Biomarkers or Disease Outcomes
3.4. Food Items Identified as Positively Associated with Biomarkers or Disease Outcomes
3.5. Food Items Bidirectionally Associated with Biomarkers or Disease Outcomes
3.6. Cooking Methods, Eating Out, and Disease Outcomes
3.7. Recent Dietary Content of Taiwanese Adults
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Phillips, J.A. Dietary Guidelines for Americans, 2020–2025. Workplace Health Saf. 2021, 69, 395. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-J.; Chang, Y.-H.; Wei, I.-L.; Kao, M.-D.; Lin, Y.-C.; Pan, W.-H. Intake levels and major food sources of energy and nutrients in the Taiwanese elderly. Asia Pac. J. Clin. Nutr. 2005, 14, 211–220. [Google Scholar] [PubMed]
- Cempaka, A.R.; Tseng, S.-H.; Yuan, K.-C.; Bai, C.-H.; Tinkov, A.A.; Skalny, A.V.; Chang, J.-S. Dysregulated Iron Metabolism-Associated Dietary Pattern Predicts an Altered Body Composition and Metabolic Syndrome. Nutrients 2019, 11, 2733. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.C.; Yang, H.C.; Chang, H.Y.; Yeh, C.J.; Chen, H.H.; Huang, K.C.; Pan, W.H. Morbid obesity in Taiwan: Prevalence, trends, associated social demographics, and lifestyle factors. PLoS ONE 2017, 12, e0169577. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S.-Y.; Lee, S.-C.; Hsieh, Y.-T.; Pan, W.-H. Trends in hyperuricemia and gout prevalence: Nutrition and Health Survey in Taiwan from 1993–1996 to 2005–2008. Asia Pac. J. Clin. Nutr. 2011, 20, 301–308. [Google Scholar] [PubMed]
- Chuang, S.-Y.; Lo, Y.-L.; Wu, S.-Y.; Wang, P.-N.; Pan, W.-H. Dietary Patterns and Foods Associated With Cognitive Function in Taiwanese Older Adults: The Cross-sectional and Longitudinal Studies. J. Am. Med. Dir. Assoc. 2019, 20, 544–550.e4. [Google Scholar] [CrossRef]
- Hu, T.-Y.; Chen, Y.C.; Lin, P.; Shih, C.-K.; Bai, C.-H.; Yuan, K.-C.; Lee, S.-Y.; Chang, J.-S. Testosterone-Associated Dietary Pattern Predicts Low Testosterone Levels and Hypogonadism. Nutrients 2018, 10, 1786. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, A.-L.; Hsu, C.-Y.; Chao, J.; Paramastri, R.; Lee, H.-A.; Lai, P.-C.; Hsieh, N.-C.; Wu, S.-F. Association of Testosterone-Related Dietary Pattern with Testicular Function among Adult Men: A Cross-Sectional Health Screening Study in Taiwan. Nutrients 2021, 13, 259. [Google Scholar] [CrossRef]
- Kurniawan, A.L.; Hsu, C.-Y.; Lee, H.-A.; Rau, H.-H.; Paramastri, R.; Syauqy, A.; Chao, J.C.-J. Comparing two methods for deriving dietary patterns associated with risk of metabolic syndrome among middle-aged and elderly Taiwanese adults with impaired kidney function. BMC Med. Res. Methodol. 2020, 20, 255. [Google Scholar] [CrossRef]
- Kurniawan, A.L.; Hsu, C.-Y.; Rau, H.-H.; Lin, L.-Y.; Chao, J.C.-J. Inflammatory Dietary Pattern Predicts Dyslipidemia and Anemia in Middle-Aged and Older Taiwanese Adults with Declined Kidney Function: A Cross-Sectional Population Study from 2008 to 2010. Nutrients 2019, 11, 2052. [Google Scholar] [CrossRef] [Green Version]
- Kurniawan, A.L.; Hsu, C.-Y.; Rau, H.-H.; Lin, L.-Y.; Chao, J.C.-J. Association of kidney function-related dietary pattern, weight status, and cardiovascular risk factors with severity of impaired kidney function in middle-aged and older adults with chronic kidney disease: A cross-sectional population study. Nutr. J. 2019, 18, 27. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-C.; Yang, Y.-H.; Chuang, S.-Y.; Liu, S.-C.; Yang, H.-C.; Pan, W.-H. Risk of asthma associated with energy-dense but nutrient-poor dietary pattern in Taiwanese children. Asia Pac. J. Clin. Nutr. 2012, 21, 73–81. [Google Scholar] [PubMed]
- Lin, P.; Chang, C.-C.; Yuan, K.-C.; Yeh, H.-J.; Fang, S.-U.; Cheng, T.; Teng, K.-T.; Chao, K.-C.; Tang, J.-H.; Kao, W.-Y.; et al. Red Blood Cell Aggregation-Associated Dietary Pattern Predicts Hyperlipidemia and Metabolic Syndrome. Nutrients 2018, 10, 1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.-P.; Kao, Y.-C.; Pan, W.-H.; Yang, Y.-H.; Chen, Y.-C.; Lee, Y. Associations between Respiratory Diseases and Dietary Patterns Derived by Factor Analysis and Reduced Rank Regression. Ann. Nutr. Metab. 2016, 68, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.-L.; Hsieh, Y.-T.; Hsu, L.-L.; Chuang, S.-Y.; Chang, H.-Y.; Hsu, C.-C.; Chen, C.-Y.; Pan, W.-H. Dietary Pattern Associated with Frailty: Results from Nutrition and Health Survey in Taiwan. J. Am. Geriatr. Soc. 2017, 65, 2009–2015. [Google Scholar] [CrossRef]
- Paramastri, R.; Hsu, C.-Y.; Chuang, Y.-K.; Lee, H.-A.; Wiratama, B.S.; Chao, J.C.-J. Synergistic Interaction of Dietary Pattern and Concordance Lifestyle with Abnormal Liver Function among Young Adults in Taiwan: A Population-Based Longitudinal Study. Nutrients 2021, 13, 3591. [Google Scholar] [CrossRef]
- Paramastri, R.; Hsu, C.-Y.; Lee, H.-A.; Lin, L.-Y.; Kurniawan, A.L.; Chao, J.C.-J. Association between Dietary Pattern, Lifestyle, Anthropometric Status, and Anemia-Related Biomarkers among Adults: A Population-Based Study from 2001 to 2015. Int. J. Environ. Res. Public Health 2021, 18, 3438. [Google Scholar] [CrossRef]
- Shiau, M.-H.; Lee, M.-C.; Lin, F.-L.; Hurng, B.-S.; Yeh, C.-J. Cross-Sectional, Short-, Medium-, and Long-Term Effects of Dietary Pattern on Frailty in Taiwan. Int. J. Environ. Res. Public health 2021, 18, 9717. [Google Scholar] [CrossRef]
- Lo, Y.L.; Pan, W.-H.; Hsu, W.-L.; Chien, Y.-C.; Chen, J.-Y.; Hsu, M.-M.; Lou, P.-J.; Chen, I.-H.; Hildesheim, A.; Chen, C.-J. Partial Least Square Discriminant Analysis Discovered a Dietary Pattern Inversely Associated with Nasopharyngeal Carcinoma Risk. PLoS ONE 2016, 11, e0155892. [Google Scholar] [CrossRef] [Green Version]
- Chuang, S.Y.; Chang, H.-Y.; Fang, H.-L.; Lee, S.-C.; Hsu, Y.-Y.; Yeh, W.-T.; Liu, W.-L.; Pan, W.-H. The Healthy Taiwanese Eating Approach is inversely associated with all-cause and cause-specific mortality: A prospective study on the Nutrition and Health Survey in Taiwan, 1993–1996. PLoS ONE 2021, 16, e0251189. [Google Scholar] [CrossRef]
- Hu, T.-Y.; Lee, S.-Y.; Shih, C.-K.; Chou, M.-J.; Wu, M.-C.; Teng, I.-C.; Bai, C.-H.; Sabrina, N.; Tinkov, A.A.; Skalny, A.V.; et al. Soluble CD163-Associated Dietary Patterns and the Risk of Metabolic Syndrome. Nutrients 2019, 11, 940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.Y.; Yeh, N.-H.; Chang, H.-Y.; Wang, C.-F.; Hung, S.-Y.; Wu, S.-J.; Pan, W.-H. Adequate protein intake in older adults in the context of frailty: Cross-sectional results of the Nutrition and Health Survey in Taiwan 2014–2017. Am. J. Clin. Nutr. 2021, 114, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: A series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [Green Version]
- Alasalvar, C.; Salvadó, J.-S.; Ros, E. Bioactives and health benefits of nuts and dried fruits. Food Chem. 2020, 314, 126192. [Google Scholar] [CrossRef]
- Ruxton, C.H.S.; Reed, S.C.; Simpson, M.J.A.; Millington, K.J. The health benefits of omega-3 polyunsaturated fatty acids: A review of the evidence. J. Hum. Nutr. Diet. 2004, 17, 449–459. [Google Scholar] [CrossRef]
- Chatterjee, C.; Gleddie, S.; Xiao, C.W. Soybean Bioactive Peptides and Their Functional Properties. Nutrients 2018, 10, 1211. [Google Scholar] [CrossRef] [Green Version]
- Trevisanato, S.I.; Kim, Y.I. Tea and health. Nutr. Rev. 2000, 58, 1–10. [Google Scholar] [CrossRef]
- Flom, J.D.; Sicherer, S.H. Epidemiology of Cow’s Milk Allergy. Nutrients 2019, 11, 1051. [Google Scholar] [CrossRef] [Green Version]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Otsuka, R.; Tange, C.; Tomida, M.; Nishita, Y.; Kato, Y.; Yuki, A.; Ando, F.; Shimokata, H.; Arai, H. Dietary factors associated with the development of physical frailty in community-dwelling older adults. J. Nutr. Health Aging 2018, 23, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.-P.; Chen, S.; Li, Y.; Schwab, A.L.; Stampfer, M.J.; Sacks, F.M.; Rosner, B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Egg consumption and risk of cardiovascular disease: Three large prospective US cohort studies, systematic review, and updated meta-analysis. BMJ 2020, 368, m513. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Ref. | Participants’ Characteristics | Outcome | Data Set | Study Design | Methods and Cut-Off Point |
|---|---|---|---|---|---|
| [12] | n = 2082, 7–12 y | Asthma | NAHSIT 2001–2002 (NAHSIT Children) | Cross-sectional | RRR, >0.24 and <−0.27 |
| [14] | n = 2397 4th graders | Respiratory diseases | Taiwan Children Health Study 2011 | Cross-sectional | RRR, 0.3 |
| [19] | n = 372 controls and 378 cases <75 y with incident, primary, histologically confirmed NPC | NPC | The National Taiwan University and MacKay Memorial Hospitals patients 1991–1994 | Case-control | PLSDA, 0.2 |
| [8] | n = 3283, men | Poor testicular function | MJHID 2009–2015 | Cross-sectional | RRR, 0.2 |
| [20] | n = 2475, 18~65 y | All-cause and cause-specific mortality | NAHSIT 1993–1996 | Prospective | Significant univariate predictive food item, p < 0.05 |
| [17] | n = 118,924, 20–45 y | Anemia | MJHID 2001–2015 | Cross-sectional | RRR, 0.2 |
| [16] | 62,645 participants met the criteria: (1) aged between 20 and 45 years, (2) free of chronic diseases, (3) having normal levels of serum liver enzymes at baseline and no history of receiving hepatic treatment, (4) having at least one follow-up visit, and (5) having complete data at baseline. 11,506 participants developed abnormal liver function (18.4%). | Abnormal Liver Function | MJHID 2001–2015 | Longitudinal | RRR, 0.2 |
| [13] | n = 212 adults, 20–64 y | Hyperlipidemia and Metabolic syndrome | TMUH 2015–2016 patients at the Division of Gastroenterology and Hepatobiliary Diseases, Department of Internal Medicine, | Cross-sectional | RRR, 0.2 |
| [7] | n = 125, 20–64 y men | Hypogonadism | TMUH 2015 patients at the Division of Gastroenterology and Hepatobiliary Diseases, Department of Internal Medicine, | Cross-sectional | RRR, 0.2 |
| [21] | n = 166, 20–64 y | Metabolic syndrome | TMUH 2015 | Cross-sectional | RRR, 0.2 |
| [3] | n = 208, 20–65 y | Central obesity and Metabolic syndrome | TMUH 2015–2016 patients at the Division of Gastroenterology and Hepatobiliary Diseases, Department of Internal Medicine, | Cross-sectional | RRR, 0.2 |
| [5] | n = 2979 and 1661 | Hyperuricemia | NAHSIT 1993–1996, 2005–2008 | Cross-sectional | RRR, 0.2 |
| [4] | n = 3071, 1673, 1440, all over 19 y | Morbid obesity | NAHSIT 1993–1996, 2005–2008, 2013–2014 | Cross-sectional | RRR, 0.15 |
| [10] | n = 41,128, eGFR <90 mL/min/1.73 m2 and positive urinary protein | Dyslipidemia in males and anemia | MJHID 2008–2010 | Cross-sectional | RRR, 0.2 |
| [11] | n = 41,128, eGFR <90 mL/min/1.73 m2 and proteinuria | Weight status, increased cardiovascular risk, and severity of impaired kidney function | MJHID 2008–2010 | Cross-sectional | RRR, 0.2 |
| [9] | n = 25,569 over 40 y, eGFR <90 mL/min/1.73 m2, and positive urinary protein | Metabolic syndrome | MJ 2008~2010 | Cross-sectional | RRR, 0.2 |
| [18] | n = 3486, 53 y and above | Frailty | TLSA (1999, 2003, 2007, and 2011) | Cross-sectional | RRR, 0.2 |
| [15] | n = 1440, 65 y and above | Frailty | NAHSIT 2014–2016 | Cross-sectional | RRR, 0.2 |
| [6] | n = 1245, 65 y and above | Mild cognitive impairment | NAHSIT 2014–2016 | Cross-sectional | RRR, 0.2 |
| Factor Loading for Each Food Item (Protective Counts, Risky Counts) | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. | Age (y) | Outcome b | Response Variables | Vegetable (15,0) | Fruit (12, 0) | Seafood, Fish, or Both (11,0) | Bean or Soy Bean Product (6,0) | Tea (6,0) | Whole Grains (5,0) | Nuts (4,0) | Coffee (5,1) | Rice (r) or Noodle (n) Not Fried (3,3) | Dairy (9,3) | Egg (5,3) | Bread & Pastry (2,1) | Jam or Honey (0,1) | Bamboo Shoots (0,2) | Refined Dessert (0,3) | Fried Rice or Noodle Product (0,4) | Sauce (0,4) | Fast Food (0,6) | Meat (2,7) | Sugary Drinks or Candies (0,7) | Internal Organs or Marble Meat (0,8) | Processed Products (0,10) | Healthy Cooking Methods (3,0) | Eating at Home (1,1) | Eating Out (0,2) |
| [12] | 7–12 | Asthma | Asthma symptom score | −0.44 | −0.34 | −0.27r | 0.31 | 0.44 | 0.25 | 0.24 | ||||||||||||||||||
| [14] | 10 | Respiratory diseases | Respiratory disease score | 0.70 | 0.6 | |||||||||||||||||||||||
| [19] | <75 | NPC | NPC status | −0.32 | −0.43 | −0.35 | −0.27 | −0.4 | −0.24 | |||||||||||||||||||
| [8] | N/A | Poor testicular function | Hb, Hct, TG, HDL-c, TC/HDL-c, uric acid | −0.23 | −0.23 | −0.21 ~ −0.47 | 0.31 | 0.28 | 0.27 | 0.37 | 0.27 | |||||||||||||||||
| [20] | 18–65 | All-cause and cause-specific mortality | All cause death risk | NA | NA | NA | NA | NA | NA | NA | NA | |||||||||||||||||
| [17] | 20–45 | Anemia | Hb, Hct, RBC, WBC, CRP | 0.3 | 0.2~ 0.5 | 0.4 ~ 0.5 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | |||||||||||||||||||
| [16] | 20–45 | Abnormal liver function | ALT, AST, γ-GT, ALP, LDH, albumin, total bilirubin | −0.24 | −0.3 | −0.31 | −0.3 | 0.47 | 0.46 | 0.22 | ||||||||||||||||||
| [13] | 20–64 | Hyperlipidemia & MetS | RBC aggregation, Hepcidin, %TS, sCD163 | −0.25 ~ −0.29 | −0.22 | −0.21r ~ 0.38n | −0.3 | 0.28 | −0.34 | |||||||||||||||||||
| [7] | 20–64 | Hypogonadism | Total testosterone, insulin, %TS, RBC aggregation | −0.25 | −0.31n | 0.26 | 0.35 | 0.24 | −0.28 | 0.24 | ||||||||||||||||||
| [21] | 20–64 | MetS | AST, RBC | −0.2 ~ −0.29 | −0.24 | −0.21 | 0.38 | −0.24 | 0.25 | −0.41 | 0.26 | |||||||||||||||||
| [3] | 20–65 | Central obesity & MetS | Hepcidin, ferritin, ALT, HDL-c | 0.23 | −0.24 | 0.41 | 0.29 chicken & pork | 0.22 | 0.34 | −0.28 | 0.28 | |||||||||||||||||
| [5] | ≧19 | Hyperuricemia in women | Uric acid | −0.24 ~ −0.4 | −0.24 | −0.29 | −0.29 | −0.33 | 0.21 | |||||||||||||||||||
| [5] | ≧19 | Hyperuricemia in men | Uric acid | −0.2 ~ −0.33 | −0.22 | −0.31 | −0.38 | 0.23 | −0.24 lean meat | 0.34 | 0.22 | 0.30 | ||||||||||||||||
| [4] | ≧19 | Morbid obesity | BMI | −0.36 | −0.16 | −0.2 oat | −0.35 | −0.16 | −0.28 | 0.24 red meat | 0.42 | 0.17 | ||||||||||||||||
| [10] | ≧40 | Dyslipidemia in males; anemia in both gender | CRP, N/L ratio | −0.2 | −0.4 ~ −0.5 | −0.3 | −0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | |||||||||||||||
| [11] | ≧40 | Weight status & others | WHR, TG, LDL-c, TC/HDL-c, BUN, creatinine | −0.23 | −0.24 | −0.22 | −0.23 | 0.25 ~ 0.32 | 0.31 | 0.21 | 0.32 | 0.31 | 0.38 | |||||||||||||||
| [9] | ≥40 | MetS | WC, TG, HDL-c, SBP, DBP, FBG | −0.2 | 0.2 ~ 0.3 | 0.2 ~ 0.3 | −0.2 ~ −0.3 | 0.2 ~ 0.3 | 0.3 ~ 0.4 | 0.2 ~ 0.3 | 0.3 | 0.3 ~ 0.4 | 0.4 | |||||||||||||||
| [18] | ≧53 | Frailty | Frailty score | −0.21 | −0.4 | −0.27 ~ −0.35 | −0.46 | −0.41 | −0.23 | −0.33 | ||||||||||||||||||
| [15] | ≧65 | Frailty | Frailty score | −0.33 | −0.48 | −0.2 ~ −0.23 | −0.34 | −0.27 | −0.39 | −0.21 | ||||||||||||||||||
| [6] | ≧65 | MCI in men | MMSE score | 0.47 | 0.20 ~ 0.21 | 0.29oat ~ 0.33 | 0.46 | 0.24 | 0.24 | |||||||||||||||||||
| [6] | ≧65 | MCI in women | MMSE score | 0.23 | 0.52 | 0.26 | 0.33 | 0.28 | 0.34 | 0.20 | 0.3 | |||||||||||||||||
| N = 6538 | ||||||
|---|---|---|---|---|---|---|
| Food Groups (Servings) b | Mean | 25th Percentile | Median | 75th Percentile | Taiwanese Food Guide | Health TEA Recommendation |
| Total carbohydrate-rich food | 12.5 | 7.9 | 11.4 | 15.9 | 12.0 | 12.0 |
| Cereals and roots | 7.8 | 4.2 | 7.0 | 10.3 | >11 | |
| Carbohydrate-rich convenience foods | 2.0 | 0.0 | 0.3 | 3.1 | ||
| Pastries and cookies | 1.0 | 0.0 | 0.0 | 1.2 | ||
| Soup and miscellaneous foods | 0.1 | 0.0 | 0.0 | 0.0 | ||
| Simple sugar | 1.7 | 0.1 | 0.7 | 2.4 | <1 | |
| Total protein-rich food | 7.7 | 4.0 | 6.5 | 10.1 | 5.0 | 6.0 |
| Soy bean and products | 1.1 | 0.0 | 0.1 | 1.5 | 2.0 | |
| Fish and seafood | 1.3 | 0.0 | 0.4 | 1.8 | 2.0 | |
| Eggs | 0.8 | 0.0 | 0.5 | 1.1 | 1.0 | |
| Livestock and Poultry | 4.1 | 1.2 | 3.1 | 5.7 | 1.0 | |
| Protein from staple foods | 0.4 | 0.0 | 0.1 | 0.5 | ||
| Dairy products | 0.5 | 0.0 | 0.0 | 0.7 | 1.5 | 0.5 |
| Vegetables | 2.4 | 0.9 | 1.9 | 3.3 | 3.0 | 3.0 |
| Fruits | 1.5 | 0.0 | 1.0 | 2.2 | 2.0 | 2.0 |
| Oil | 5.3 | 2.4 | 4.3 | 7.1 | 5.0 | 5.0 |
| Cooking oil | 4.8 | 2.1 | 3.9 | 6.5 | 4.0 | 4.0 |
| Nuts | 0.5 | 0.0 | 0.0 | 0.0 | 1.0 | 1.0 |
| n = 5549 | ||||||
| Sugar-free tea (times/day) | 0.43 | 0 | 0.08 | 0.71 | 1 | |
| n = 5548 | ||||||
| Sugar-free coffee (times/day) | 0.26 | 0 | 0 | 0.29 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, W.-H.; Wu, S.-Y.; Yeh, N.-H.; Hung, S.-Y. Healthy Taiwanese Eating Approach (TEA) toward Total Wellbeing and Healthy Longevity. Nutrients 2022, 14, 2774. https://doi.org/10.3390/nu14132774
Pan W-H, Wu S-Y, Yeh N-H, Hung S-Y. Healthy Taiwanese Eating Approach (TEA) toward Total Wellbeing and Healthy Longevity. Nutrients. 2022; 14(13):2774. https://doi.org/10.3390/nu14132774
Chicago/Turabian StylePan, Wen-Harn, Szu-Yun Wu, Nai-Hua Yeh, and Shu-Yi Hung. 2022. "Healthy Taiwanese Eating Approach (TEA) toward Total Wellbeing and Healthy Longevity" Nutrients 14, no. 13: 2774. https://doi.org/10.3390/nu14132774
APA StylePan, W.-H., Wu, S.-Y., Yeh, N.-H., & Hung, S.-Y. (2022). Healthy Taiwanese Eating Approach (TEA) toward Total Wellbeing and Healthy Longevity. Nutrients, 14(13), 2774. https://doi.org/10.3390/nu14132774