
Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania

 , , and
, , and
Abstract
:1. Introduction
Rationale for this Study
2. Materials and Methods
2.1. Development of the Draft FBDGs for Tanzania
2.2. The Development of Images to Accompany FBDG Messages—Artwork Process
2.3. Design and Setting
2.4. Study Population
2.5. Sample Size
Sampling Strategy
2.6. Training of Fieldworkers
2.7. Pilot Testing
2.8. Focus Group Discussions
2.9. Data Analysis
3. Results
3.1. Socio-Demographic Profile of Participants
3.2. General Understanding of the Proposed FBDG Messages and Images, and Recommendations for Improvement
“We need to use such foods so that we can put our body into a good health and our children to have strong minds and grow physically and mentally fit.”(Participant 2 ZG2)
“Yes, they will understand when they are exposed to education.”(Participant 6 ZG2)
“What I know is that in this message we are supposed to mobilize our children to eat food that will help build their health and also maintain their mental capability so as to manage well in their studies.”(Participant 1 ZG3)
3.3. Specific Understanding of the Proposed FBDG Messages and Images, and Recommendations for Improvement
- ○
- Image with children around a table depicting peanuts and vegetables;
- ○
- A child in school uniform being handed the suggested snacks by an elder or father;
- ○
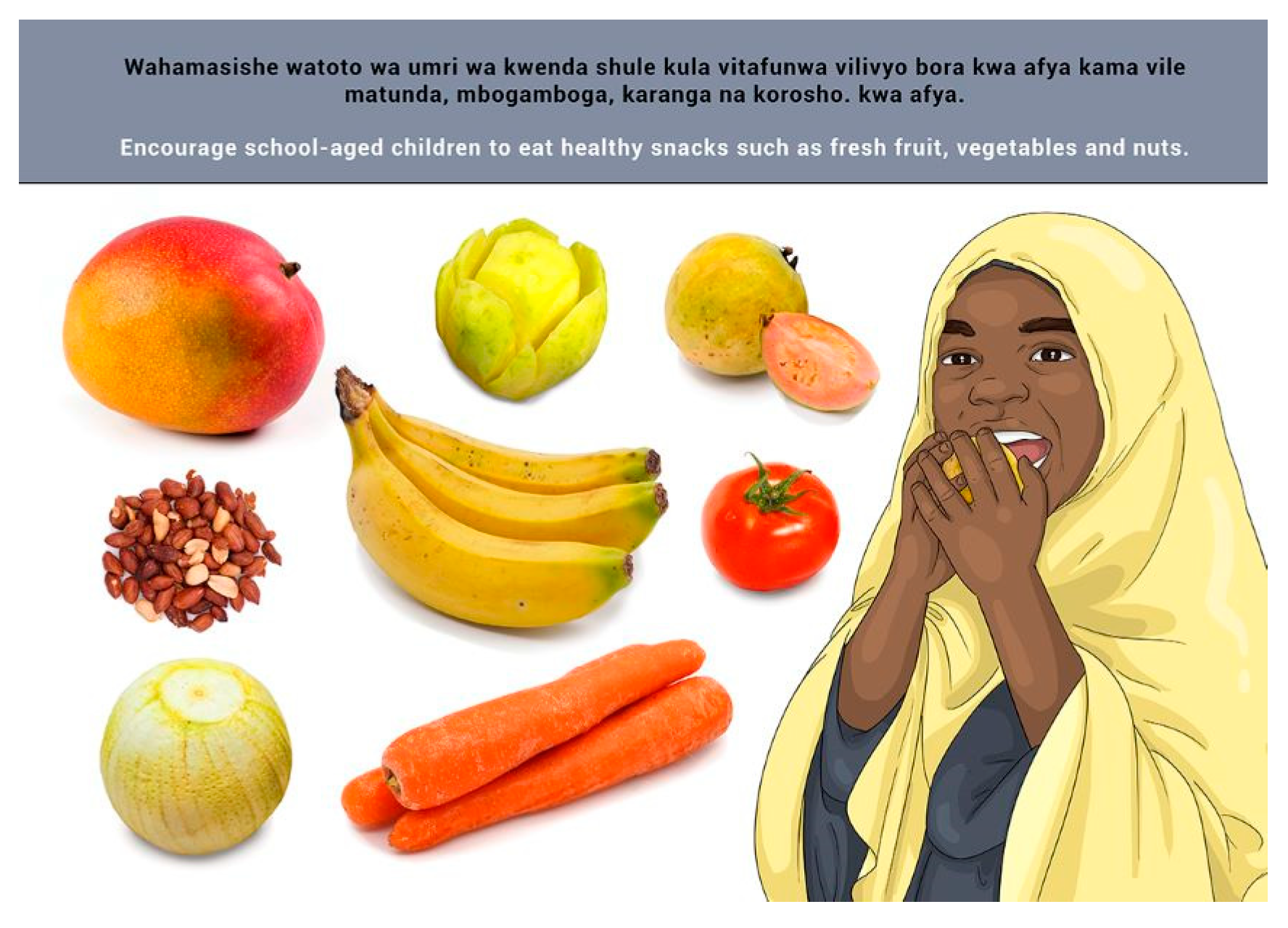
- A child standing next to the suggested snacks.
“The message should insist on lunch at school to avoid inequality at school which can create problems for the poor children.”(Participant 1 MD2)
“I would draw a picture showing all the children having lunch at school and not packed lunch which may create conflicts.”(Participant 3MI1)
- ○
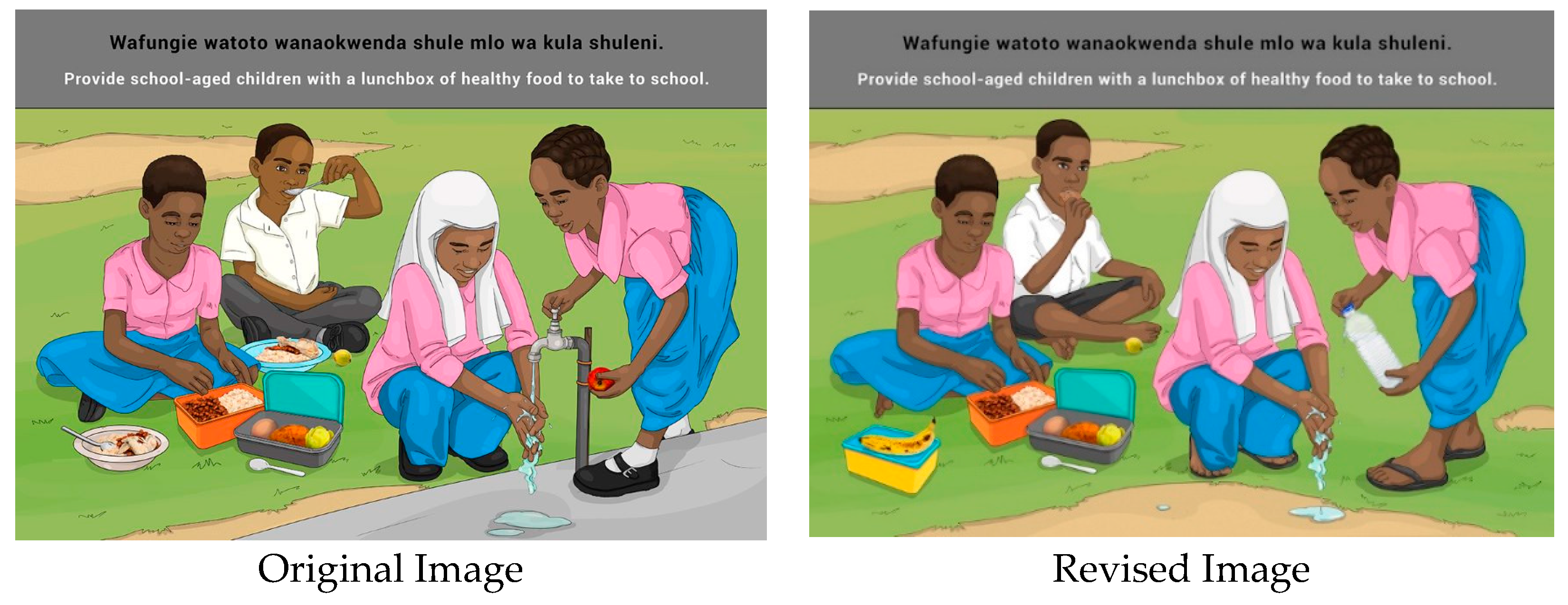
- A parent provides a child with a safe storage container containing food for school;
- ○
- A child washing hands with a lunchbox depicted in close proximity;
- ○
- Add a school building to the background;
- ○
- Add a tap for washing hands;
- ○
- Add a shared plate so that it represents a school feeding scheme.
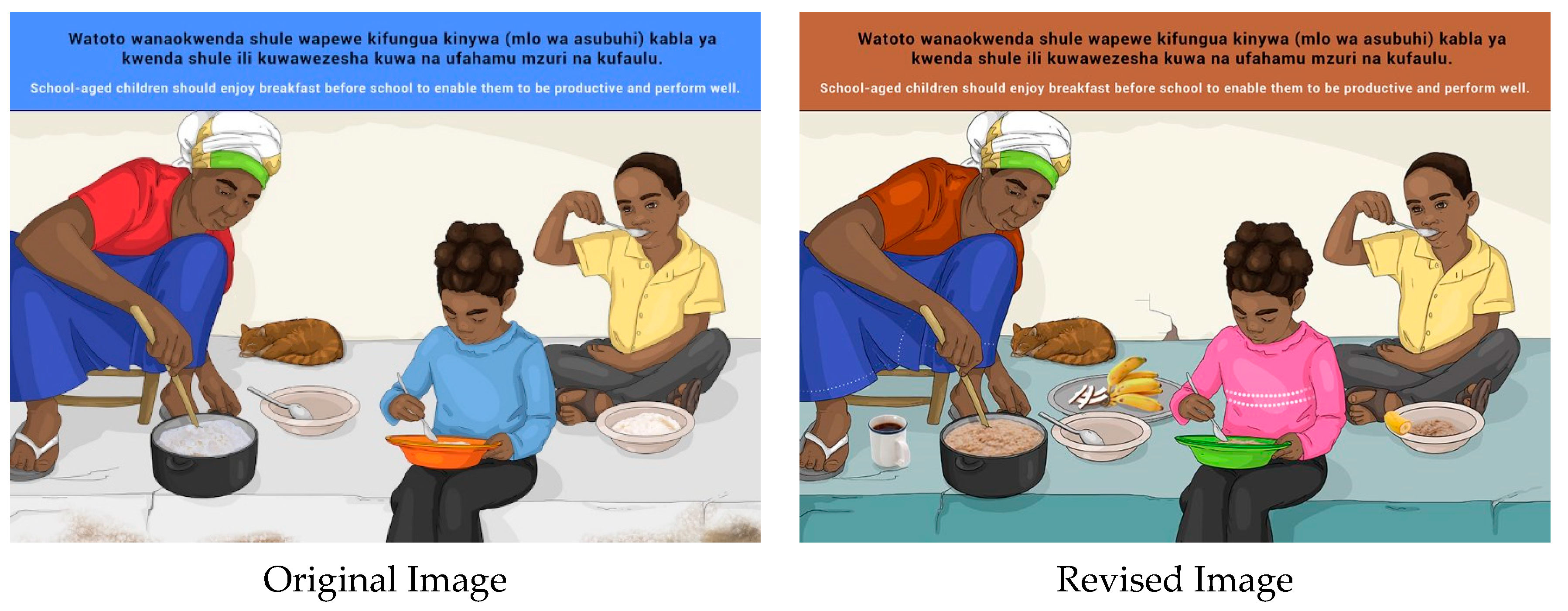
“It will not be understood because men do not work in the kitchen. The woman should be in the picture instead and more food should be included.”(Participant 6 MI1)
“The picture should show a clean house, with a clean kitchen, and the hair of the cook must be covered, and the other picture should show a house in a dirty environment and food covered with flies, for comparison.”(Participant 3 MI1)
3.4. Final Considerations
4. Discussion
Limitations
5. Conclusions and Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Joint FAO/WHO Consultation on Preparation and Use of Food-Based Dietary Guidelines (1995: Nicosia, Cyprus) & World Health Organization (1998). Preparation and Use of Food-Based Dietary Guidelines/Report of a Joint FAO/WHO Consultation. World Health Organization. Available online: http://apps.who.int/iris/bitstream/handle/10665/42051/WHO_TRS_880.pdf;jsessionid=BA4ECB9959ADB4E25ADE9A8BC7F9911D?sequence=1 (accessed on 22 June 2022).
- Food and Agriculture Organisation of the United Nations. Food-Based Dietary Guidelines. Background|Food-Based Dietary Guidelines|Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/background/en/ (accessed on 22 June 2022).
- Wingrove, K.; Lawrence, M.A.; McNaughton, S.A. Dietary patterns, foods and nutrients: A descriptive analysis of the systematic reviews conducted to inform the Australian Dietary Guidelines. Nutr. Res. Rev. 2020, 34, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organisation of the United Nations. Food Guides. Food-Based Dietary Guidelines. Food Guides|Food-Based Dietary Guidelines|Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/background/food-guide/en (accessed on 22 June 2022).
- Food and Agriculture Organisation of the United Nations. FAO’s Work in Dietary Guidelines. Food-Based Dietary Guidelines. FAO’s Work in Dietary Guidelines|Food-Based Dietary Guidelines|Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/nutrition/education/food-dietary-guidelines/background/fao-work-dietary-guidelines/en/ (accessed on 22 June 2022).
- Africa Facts. Facts about Tanzania. Facts About Tanzania|Africa Facts. Available online: https://africa-facts.org/ (accessed on 22 June 2022).
- Robinson, D.O.; Gaertner, M.; Papageorgiou, C. Tanzania: Growth acceleration and increased public spending with macroeconomic stability. Yes Afr. Can 2011, 21. Available online: https://openknowledge.worldbank.org/bitstream/handle/10986/2335/634310PUB0Yes0061512B09780821387450.pdf?sequence=1&i#page=37 (accessed on 22 June 2022).
- World Bank. United Republic of Tanzania Mainland Poverty Assessment. 2015. Microsoft Word-Tanzania Poverty Assessment_Final.docx. Available online: https://www.tralac.org/ (accessed on 22 June 2022).
- World Bank. Tanzania Mainland Poverty Assessment Report—Executive Summary. 2019. Tanzania-Mainland Poverty Assessment 2019: Executive Summary. Available online: https://www.worldbank.org/en/home (accessed on 22 June 2022).
- Mayén, A.L.; de Mestral, C.; Zamora, G.; Paccaud, F.; Marques-Vidal, P.; Bovet, P.; Stringhini, S. Interventions promoting healthy eating as a tool for reducing social inequalities in diet in low-and middle-income countries: A systematic review. Int. J. Equity Health 2016, 15, 1–10. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics (NBS) [Tanzania] and ICF Macro. Tanzania Demographic and Health Survey 2010. Dar es Salaam, Tanzania: NBS and ICF Macro. 2011. Tanzania Demographic and Health Survey 2010 [FR243]. Available online: https://dhsprogram.com/pubs/pdf/FR243/FR243%5B24June2011%5D.pdf (accessed on 22 June 2022).
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) [Tanzania Mainland]; Ministry of Health (MoH) [Zanzibar]; National Bureau of Statistics (NBS); Office of the Chief Government Statistician (OCGS); ICF. Tanzania Demographic and Health Survey and Malaria Indicator Survey (TDHS-MIS) 2015-16. Dar es Salaam, Tanzania, and Rockville, Maryland, USA: MoHCDGEC, MoH, NBS, OCGS, and ICF. 2016. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015–2016-Final Report [FR321]. Available online: https://dhsprogram.com/pubs/pdf/fr321/fr321.pdf (accessed on 22 June 2022).
- Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC); Ministry of Health (MoH); Tanzania Food and Nutrition Centre (TFNC); National Bureau of Statistics (NBS); Office of the Chief Government Statistician (OCGS); UNICEF. Tanzania National Nutrition Survey Using SMART Methodology (TNNS); MoHCDGEC: Mainland, Tanzania; MoH: Zanzibar, Tanzania; TFNC: Dar es Salaam, Tanzania; NBS: Dodoma, Tanzania; OCGS: Zanzibar, Tanzania; UNICEF: Dar es Salaam, Tanzania, 2018. [Google Scholar]
- Global Health Estimates 2020: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2019; Global Health Estimates: Leading Causes of Death; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/ (accessed on 22 June 2022).
- Mayige, M.; Kagaruki, G. Tanzania STEPS Survey Report; National Institute of Medical Research: Dar es Salaam, Tanzania, 2013. [Google Scholar]
- Zeba, A.N.; Delisle, H.F.; Renier, G. Dietary patterns and physical inactivity, two contributing factors to the double burden of malnutrition among adults in Burkina Faso, West Africa. J. Nutr. Sci. 2014, 3, e50. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef]
- Naicker, A.; Venter, C.S.; MacIntyre, U.E.; Ellis, S. Dietary quality and patterns and non-communicable disease risk of an Indian community in KwaZulu-Natal, South Africa. J. Health Popul. Nutr. 2015, 33, 1–9. [Google Scholar] [CrossRef]
- Maletnlema, T.N. A Tanzanian perspective on the nutrition transition and its implications for health. Public Health Nutr. 2002, 5, 163–168. [Google Scholar] [CrossRef]
- Research and Analysis Working Group, United Republic of Tanzania. Brief 4: An Analysis of Household Income and Expenditure in Tanzania. In Poverty and Human Development Report 2009; The Povert Eradication and Empowerment Division, Ministry of Finance and Economic Affairs: Dar es Salaam, Tanzania, 2009. [Google Scholar]
- World Bank. Action Plan for the Provision of Vitamins and Minerals to the Tanzanian Population through the Enrichment of Staple Foods; World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Beal, T.; Massiot, E.; Arsenault, J.E.; Smith, M.R.; Hijmans, R.J. Global trends in dietary micronutrient supplies and estimated prevalence of inadequate intakes. PLoS ONE 2017, 12, e0175554. [Google Scholar] [CrossRef]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottière, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Energy balance and obesity: What are the main drivers? Cancer Causes Control 2017, 28, 247–258. [Google Scholar] [CrossRef]
- Lachat, C.; Otchere, S.; Roberfroid, D.; Abdulai, A.; Seret, F.M.A.; Milesevic, J.; Xuereb, G.; Candeias, V.; Kolsteren, P. Diet and physical activity for the prevention of noncommunicable diseases in low-and middle-income countries: A systematic policy review. PLoS Med. 2013, 10, e1001465. [Google Scholar] [CrossRef]
- Delobelle, P.; Sanders, D.; Puoane, T.; Freudenberg, N. Reducing the role of the food, tobacco, and alcohol industries in noncommunicable disease risk in South Africa. Health Educ. Behav. 2016, 43, 70S–81S. [Google Scholar] [CrossRef] [PubMed]
- United States Department of State. 2018 Report on International Religious Freedom: Tanzania. 2019. Tanzania 2018 International Religious Freedom Report. Available online: https://www.state.gov/ (accessed on 22 June 2022).
- Du Plessis, L.M.; Daniels, L.C.; Koornhof, H.E.; Samuels, S.; Möller, I.; Röhrs, S. Overview of field-testing of the revised, draft Paediatric Food-Based Dietary Guidelines amongst mothers/caregivers of children aged 0–5 years in the Western Cape and Mpumalanga, South Africa. S. Afr. J. Clin. Nutr. 2021, 34, 123–131. [Google Scholar] [CrossRef]
- Hoddinott, J.; Maluccio, J.; Behrman, J.R.; Martorell, R.; Melgar, P.; Quisumbing, A.R.; Ramirez-Zea, M.; Stein, A.D.; Yount, K.M. The consequences of early childhood growth failure over the life course. In IFPRI Discussion Paper 01073; International Food Policy Research Institute: Washington, DC, USA, 2011. [Google Scholar]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Sargeant, J. Qualities of qualitative research: Part I. J. Grad. Med. Educ. 2011, 3, 449–452. [Google Scholar] [CrossRef]
- Skinner, D. Qualitative methodology: An introduction. In Epidemiology: A Research Manual for South Africa, 2nd ed.; Joubert, G., Ehrlich, R., Eds.; Oxford University Press: Cape Town, South Africa, 2007; pp. 318–327. [Google Scholar]
- Love, P.V. Developing and Assessing the Appropriateness of the Preliminary Food-Based Dietary Guidelines for South Africans. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2002. Available online: https://researchspace.ukzn.ac.za/xmlui/handle/10413/9422 (accessed on 22 June 2022).
- Micha, R.; Mannar, V.; Afshin, A.; Allemandi, L.; Baker, P.; Battersby, J.; Bhutta, Z.; Chen, K.; Corvalan, C.; Di Cesare, M.; et al. 2020 Global Nutrition Report: Action on Equity to End Malnutrition; Development Initiatives: Bristol, UK, 2020. [Google Scholar]
- Hoddinott, J.; Ahmed, A.; Karachiwalla, N.I.; Roy, S. Nutrition behaviour change communication causes sustained effects on IYCN knowledge in two cluster-randomized trials in Bangladesh. Matern. Child Nutr. 2018, 14, e12498. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Alvarez-Sanchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef]
- Dhandevi, P.E.M.; Jeewon, R. Fruit and Vegetable Intake: Benefits and Progress of Nutrition Education Interventions—Narrative Review Article. Iran. J. Public Health 2015, 44, 1309–1321. [Google Scholar]
- Mgongo, M.; Hashim, T.H.; Uriyo, J.G.; Damian, D.J.; Stray-Pedersen, B.; Msuya, S.E. Determinants of Exclusive Breastfeeding in Kilimanjaro Region, Tanzania. Sci. J. Public Health 2014, 2, 631–635. [Google Scholar] [CrossRef]
- Dukuzumuremyi, J.P.C.; Acheampong, K.; Abesig, J.; Luo, J. Knowledge, attitude, and practice of exclusive breastfeeding among mothers in East Africa: A systematic review. Int. Breastfeed. J. 2020, 15, 70. [Google Scholar] [CrossRef]
- Du Plessis, L.M.; Daniels, L.C.; Koornhof, H.E.; Solomon, Z.L.; Loftus, M.; Babajee, L.C.; Ronquest, C.; Kleingeld, B.; Greener, C.M.; Burn, K.J. Field-testing of the revised, draft South African Paediatric Food-Based Dietary Guidelines amongst mothers/caregivers of children aged 0–12 months in the Western Cape province, South Africa. S. Afr. J. Clin. Nutr. 2021, 34, 132–138. [Google Scholar] [CrossRef]
- Hoyland, A.; Dye, L.; Lawton, C.L. A systematic review of the effect of breakfast on the cognitive performance of children and adolescents. Nutr. Res. Rev. 2009, 22, 220–243. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization (FAO). Nutrition Guidelines and Standards for School Meals: A Report from 33 Low and Middle-Income Countries; FAO: Rome, Italy, 2019. [Google Scholar]
- Bundy, D.A.P.; de Silva, N.; Horton, S.; Jamison, D.T.; Patton, G.C. Re-Imagining School Feeding: A High-Return Investment in Human Capital and Local Economies; License: Creative Commons Attribution CC BY 3.0 IGO; Re-Imagining School Feeding: A High-Return Investment in Human Capital and Local Economies|Save the Children’s Resource Centre; World Bank: Washington, DC, USA, 2018. [Google Scholar]
- Leme, A.C.B.; Hou, S.; Fisberg, R.M.; Fisberg, M.; Haines, J. Adherence to Food-Based Dietary Guidelines: A Systemic Review of High-Income and Low- and Middle-Income Countries. Nutrients 2021, 13, 1038. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Message Nr | E = English S = Kiswahili | Message Wording |
|---|---|---|
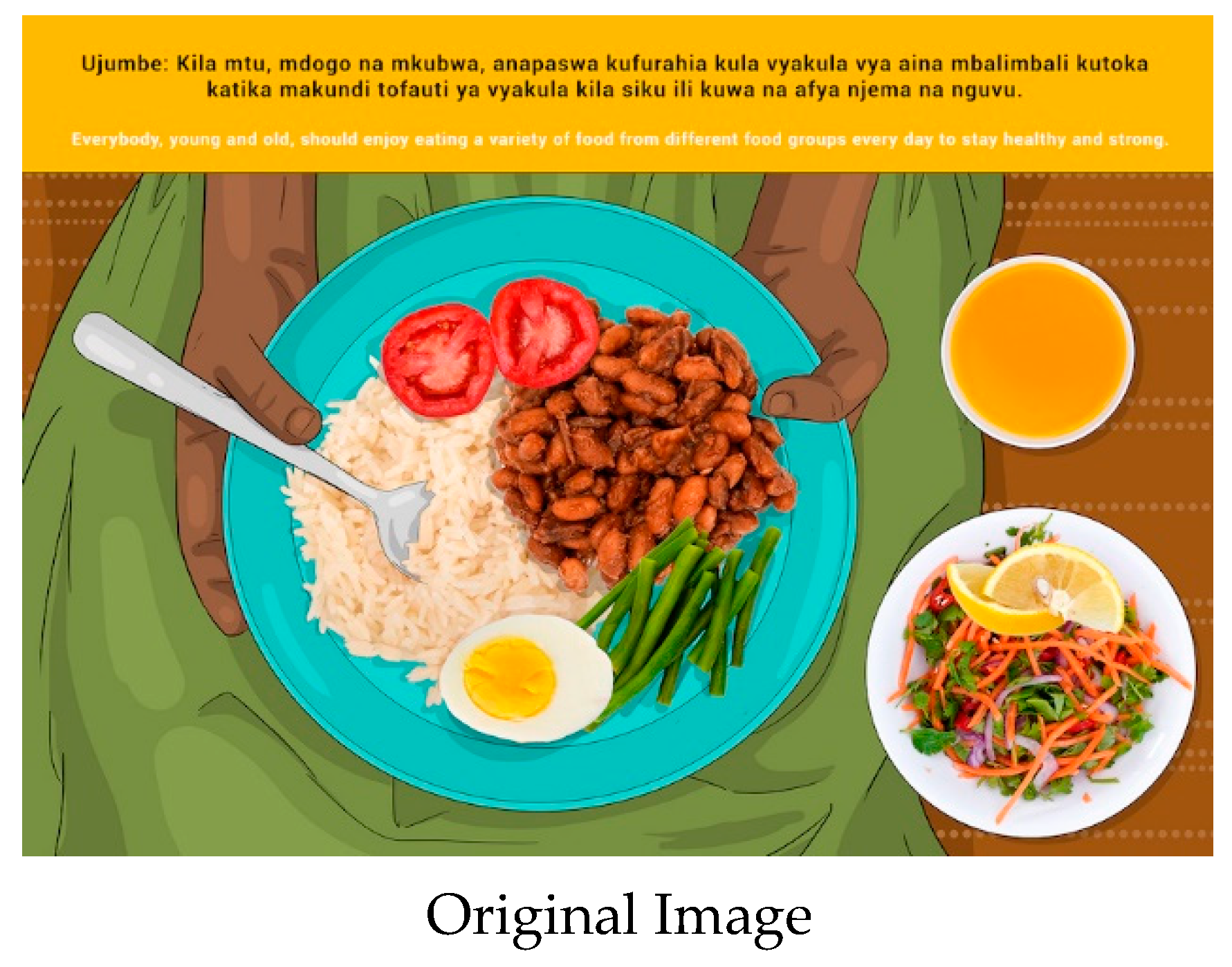
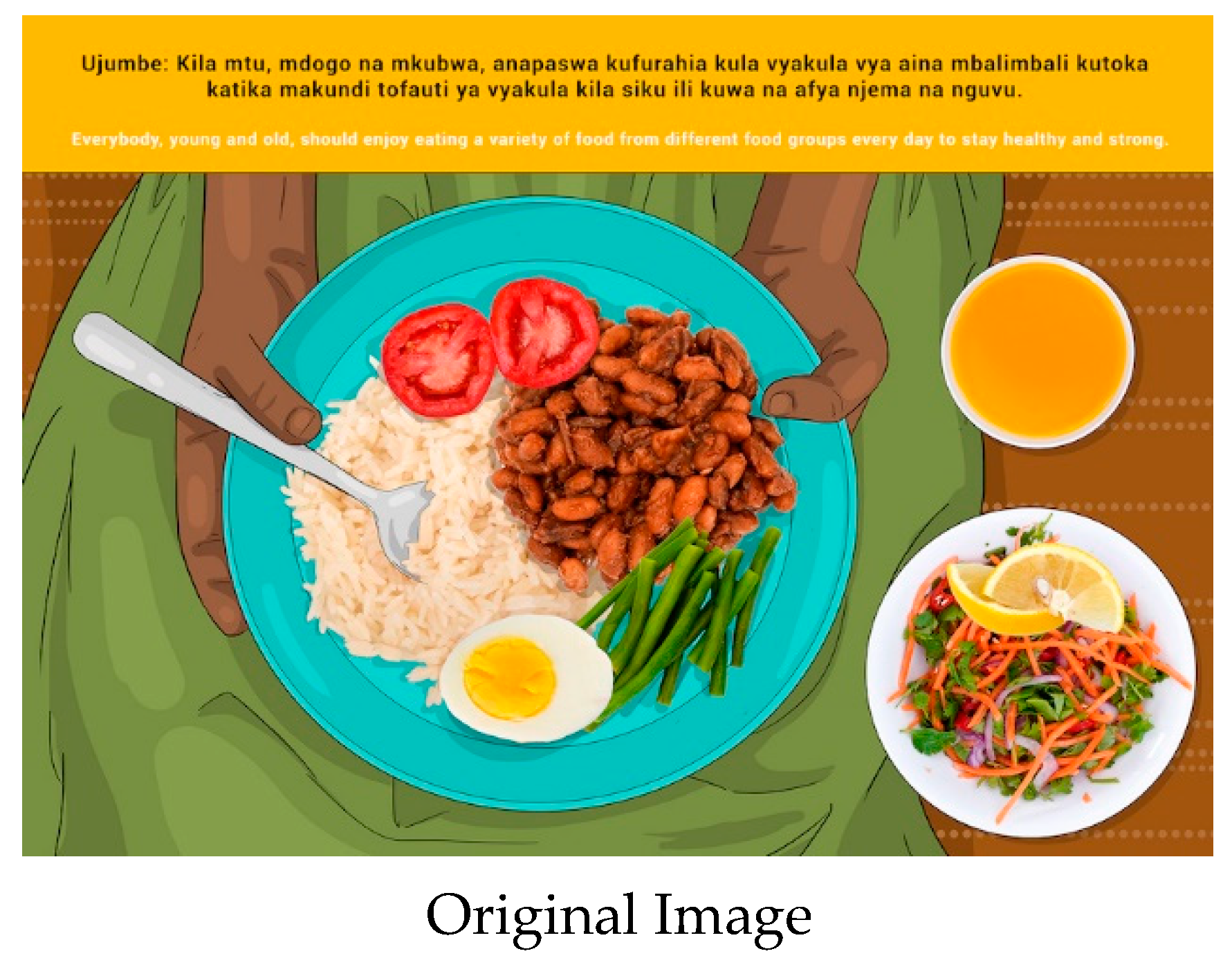
| 1 | E | Everybody, young and old, should enjoy eating a variety of foods from different food groups every day to stay healthy and strong. |
| 1 | S | Ujumbe: Kila mtu, mdogo na mkubwa, anapaswa kufurahia kula vyakula vya aina mbalimbali kutoka katika makundi tofauti ya vyakula kila siku ili kuwa na afya njema na nguvu. |
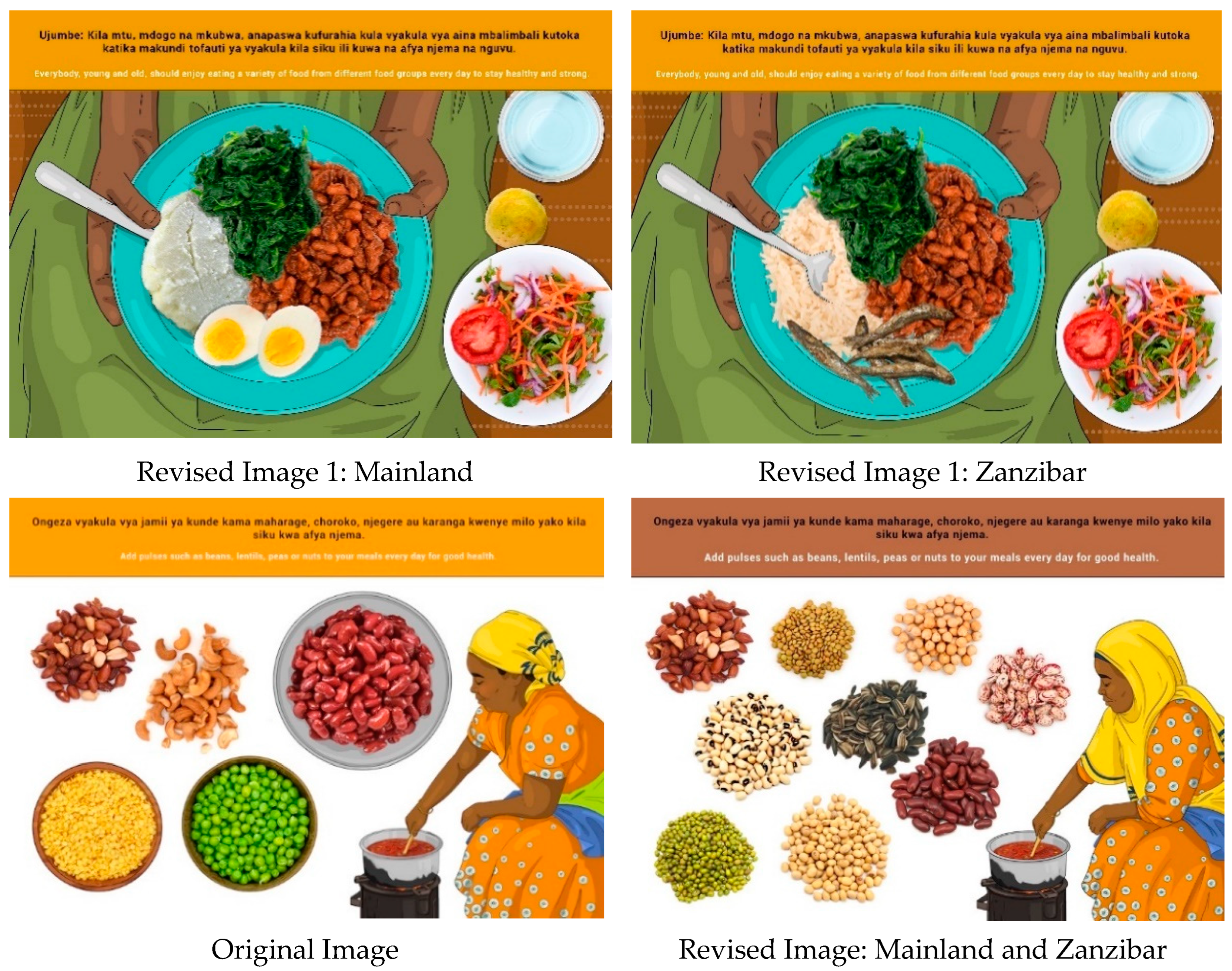
| 2 | E | Add pulses such as beans, lentils, peas or nuts to your meals every day for good health. |
| 2 | S | Ongeza vyakula vya jamii ya kunde kama maharage, choroko, njegere au karanga kwenye milo yako kila siku kwa afya njema. |
| 3 | E | Eat animal source foods, including seafood, meat, milk or eggs every day to stay strong. |
| 3 | S | Kula vyakula vya asili ya wanyama na baharini ikiwemo samaki, nyama, maziwa au mayai kila siku ili kuwa na mwili imara wenye nguvu. |
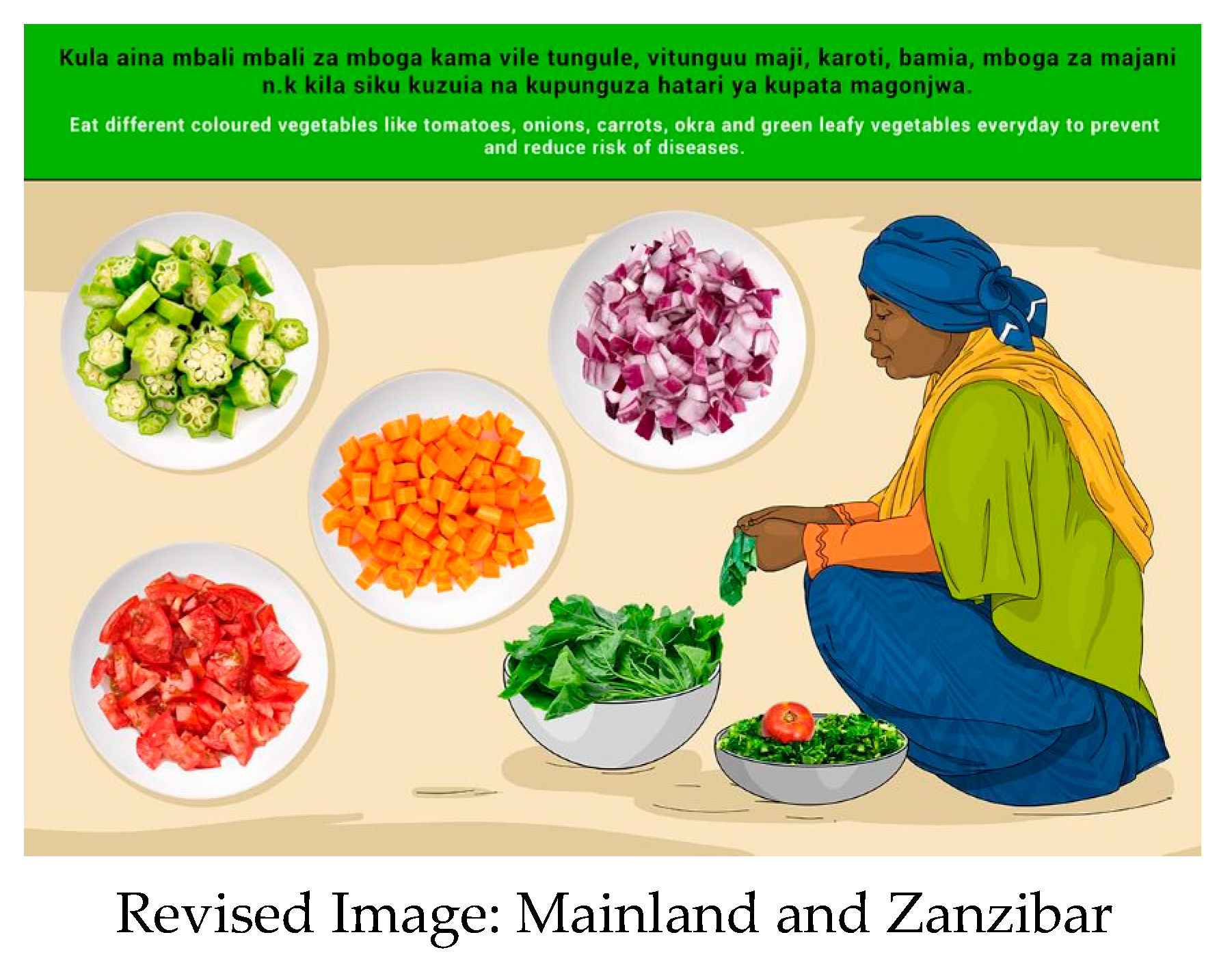
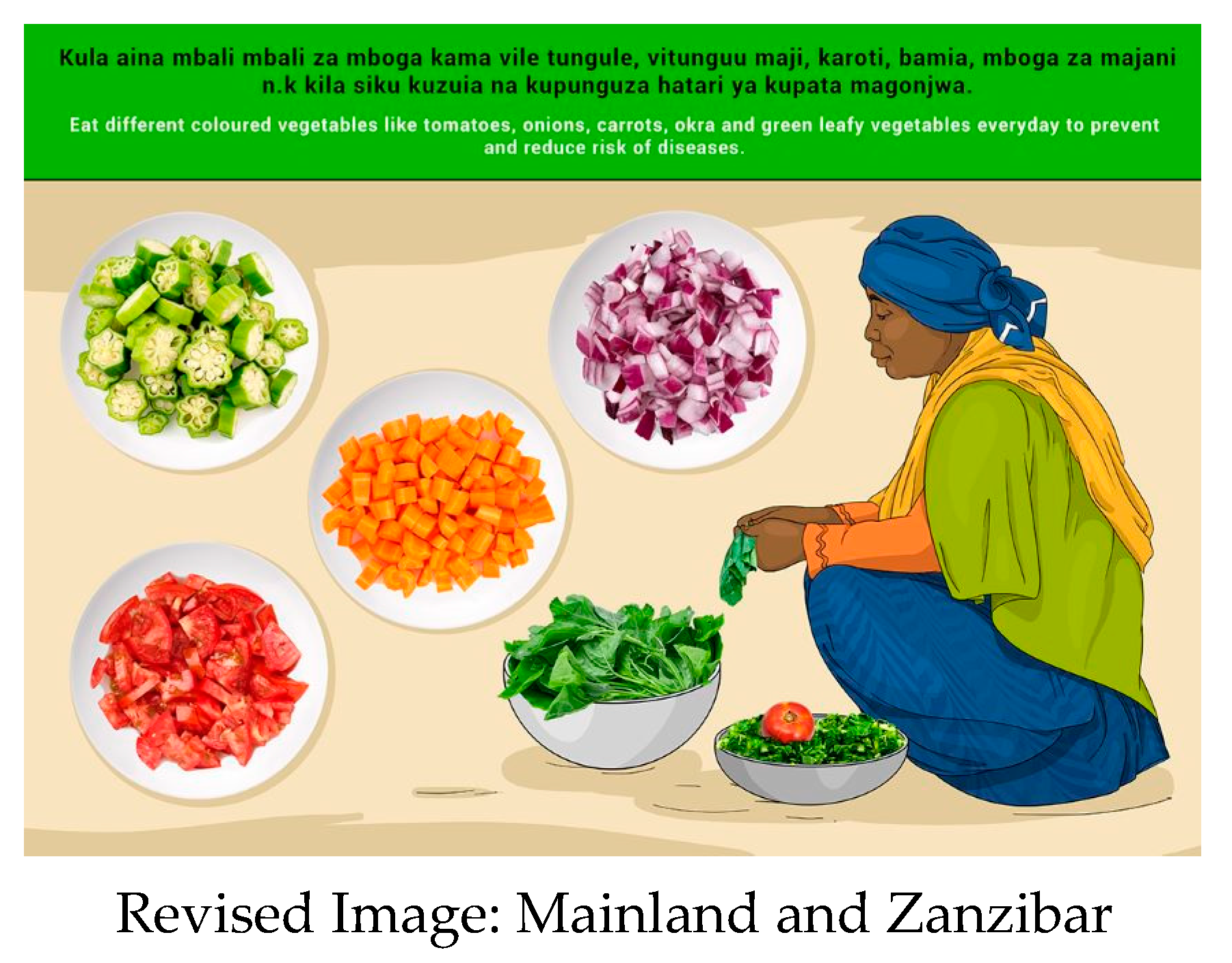
| 4 | E | MAINLAND: Eat different vegetables, at least three handfuls every day to prevent and reduce risk of diseases. |
| ZANZIBAR: Enjoy eating tomatoes, eggplant, onions, sweet pepper, carrot, okra and bitter tomatoes at least three handfuls every day to prevent and reduce risk of diseases. | ||
| 4 | S | MAINLAND: Kula mboga za majani angalau viganja vitatu kila siku kuzuia na kupunguza hatari ya kupata magonjwa. |
| ZANZIBAR: Pendelea kula tungule, bilinganyi, vitunguu maji, pilipili boga, karoti, bamia, na nyanya chungu angalau viganga vitatu kila siku kuzuia na kupunguza hatari ya kupata magonjwa. | ||
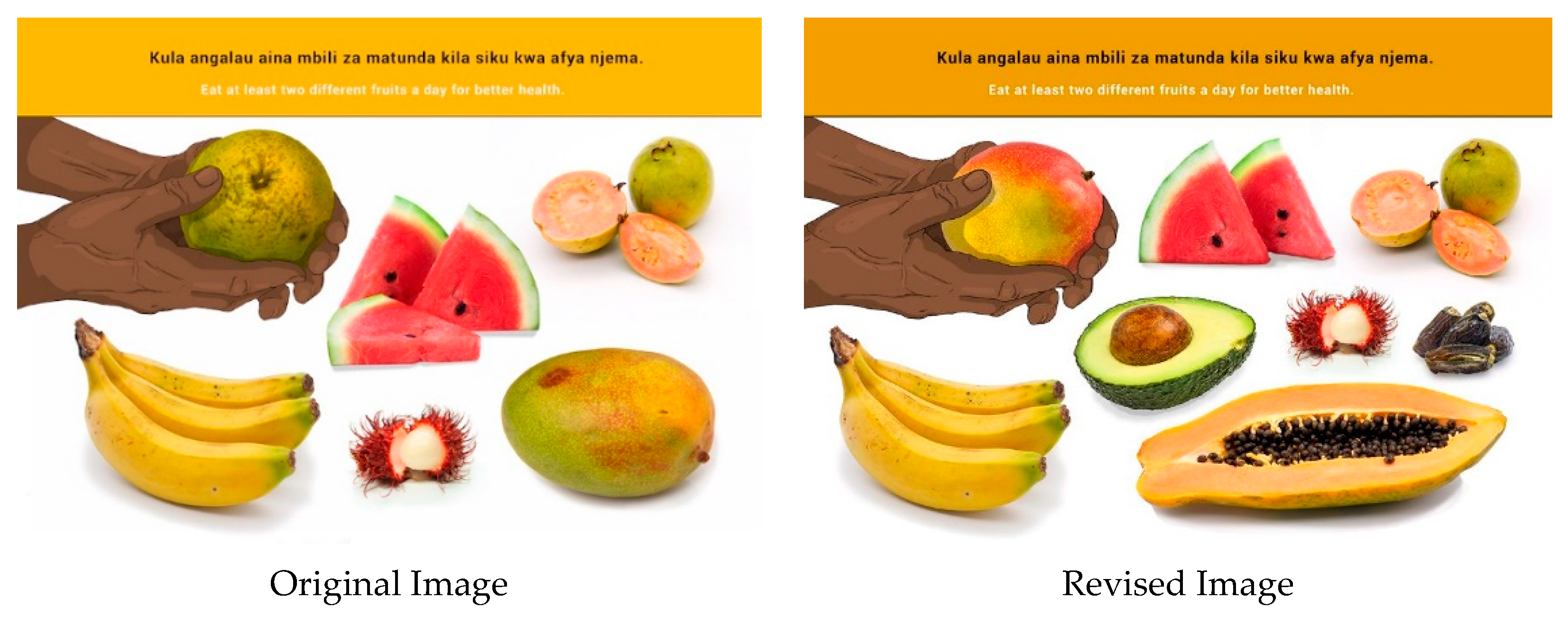
| 5 | E | Eat at least two types of fruits every day for better health. |
| 5 | S | Kula angalau aina mbili za matunda kila siku kwa afya njema. |
| 6 | E | Eat staples such as cereals, starchy roots, tubers or plantains every day for a strong and active body. |
| 6 | S | Kula chakula kikuu kama vile nafaka, vyakula vya mizizi (viazi, mihogo, nk) au ndizi za kupika kila siku kuwa na mwili imara na wenye nguvu. |
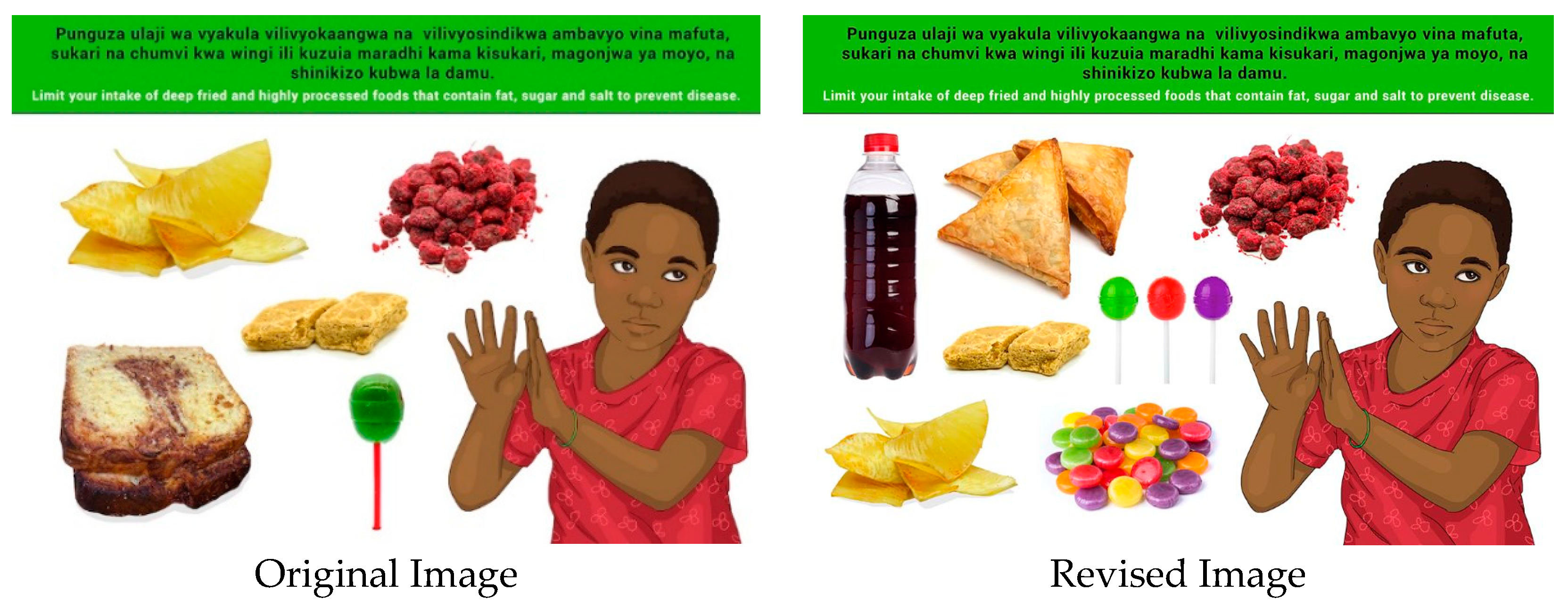
| 7 | E | Limit your intake of deep fried and highly processed foods that contain fat, sugar and salt to prevent disease such as high blood pressure, diabetes and heart diseases. |
| 7 | S | Punguza ulaji wa vyakula vilivyokaangwa na vilivyosindikwa ambavyo vina mafuta, sukari na chumvi kwa wingi ili kuzuia maradhi kama kisukari, magonjwa ya moyo, na shinikizo kubwa la damu. |
| 8 | E | Statement: The first thousand days of a child’s life starts in pregnancy and continues until two years of age. This is a very important time to ensure a child grows well on food, love and care and becomes a productive adult. |
| 8 | S | Tamko: Siku elfu moja za mwanzo wa maisha ya mtoto huanzia wakati mama amepata ujauzito na kuendelea mpaka mtoto anapotimiza umri wa miaka miwili. Muda huu ni wa muhimu kuhakikisha mtoto anapewa chakula vizuri, kwa upendo na kujaliwa ili aweze kukua vizuri na kuwa mtu mzima mwenye nguvu na afya. |
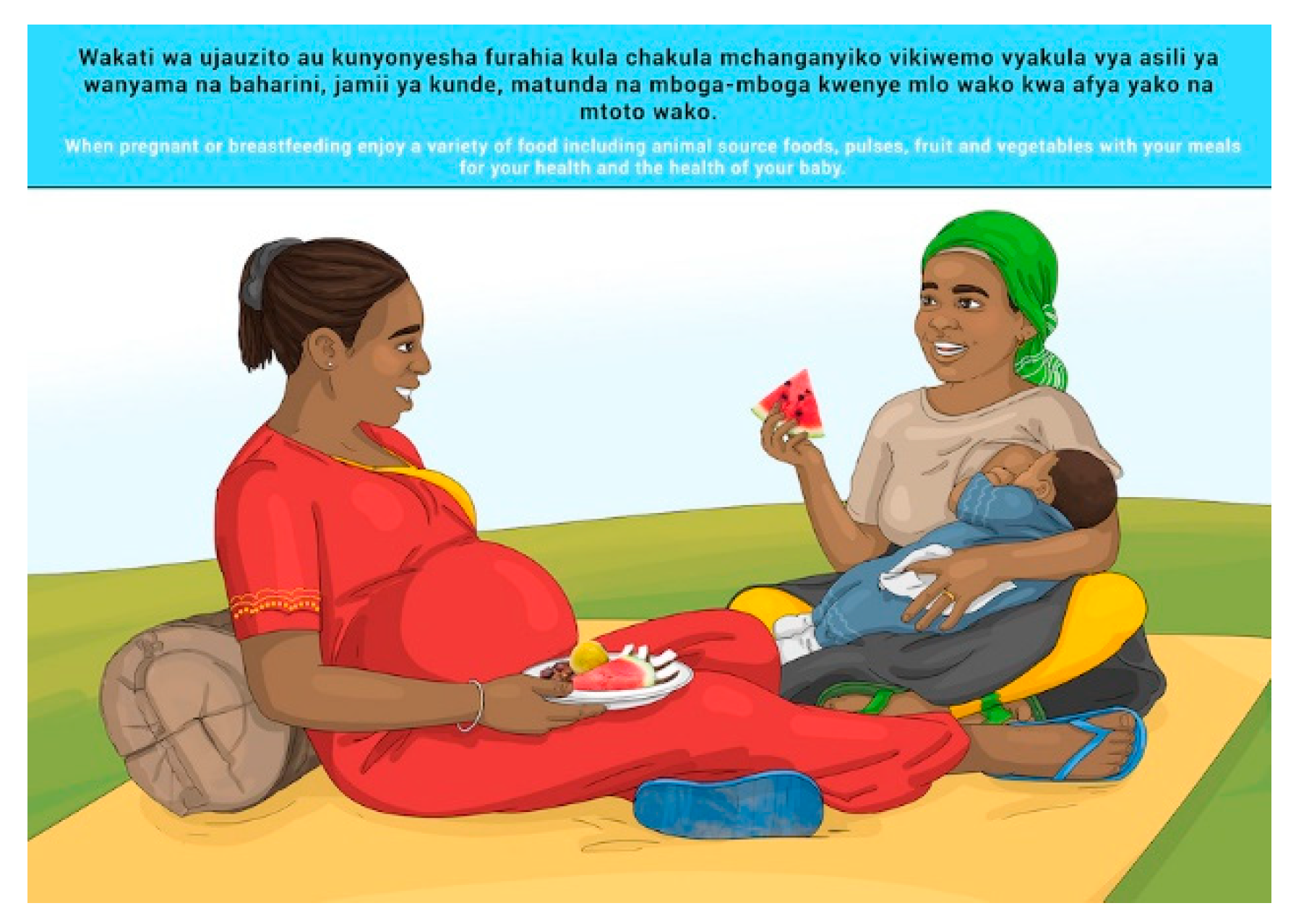
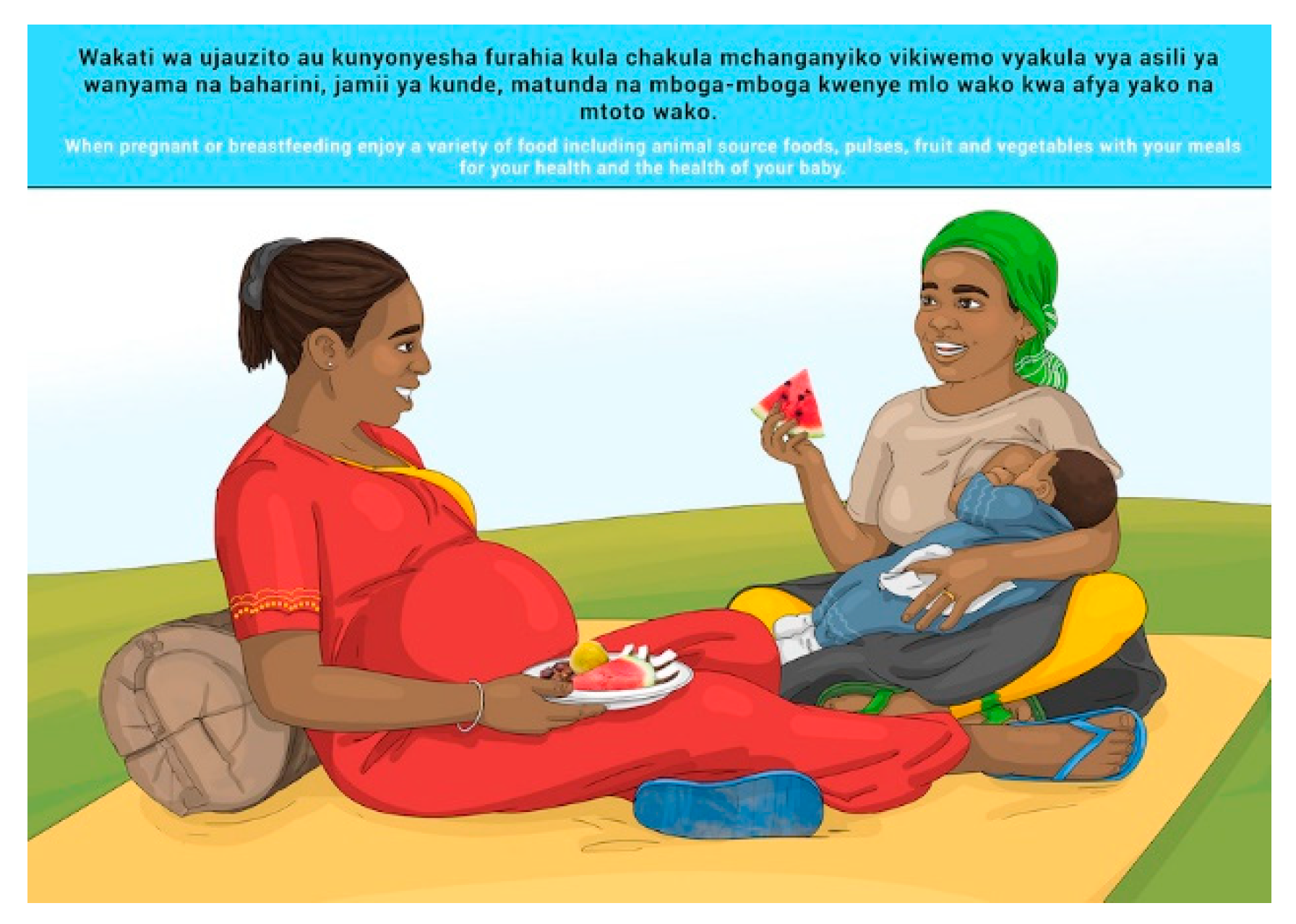
| 8 | E | When pregnant or breastfeeding enjoy a variety of food including animal source foods, pulses, fruit and vegetables with your meals for your health and the health of your baby. |
| 8 | S | Wakati wa ujauzito au kunyonyesha furahia kula chakula mchanganyiko vikiwemo vyakula vya asili ya wanyama na baharini, jamii ya kunde, matunda na mboga-mboga kwenye mlo wako kwa afya yako na mtoto wako. |
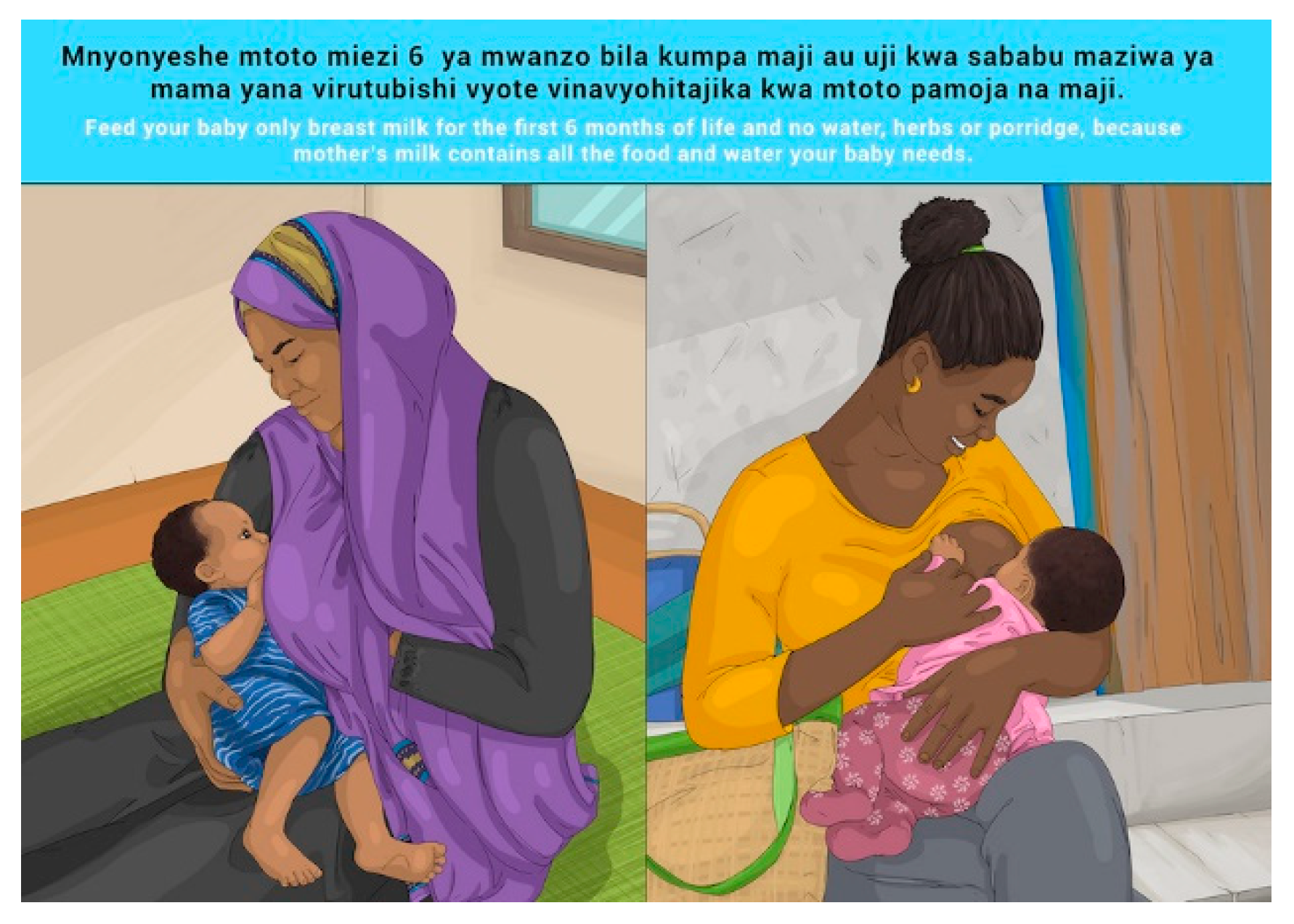
| 9 | E | Feed your baby only breast milk for the first 6 months of life and no water, herbs or porridge, because mother’s milk contains all the food and water your baby needs. |
| 9 | S | Mnyonyeshe mtoto miezi 6 ya mwanzo bila kumpa maji au uji kwa sababu maziwa ya mama yana virutubishi vyote vinavyohitajika kwa mtoto pamoja na maji. |
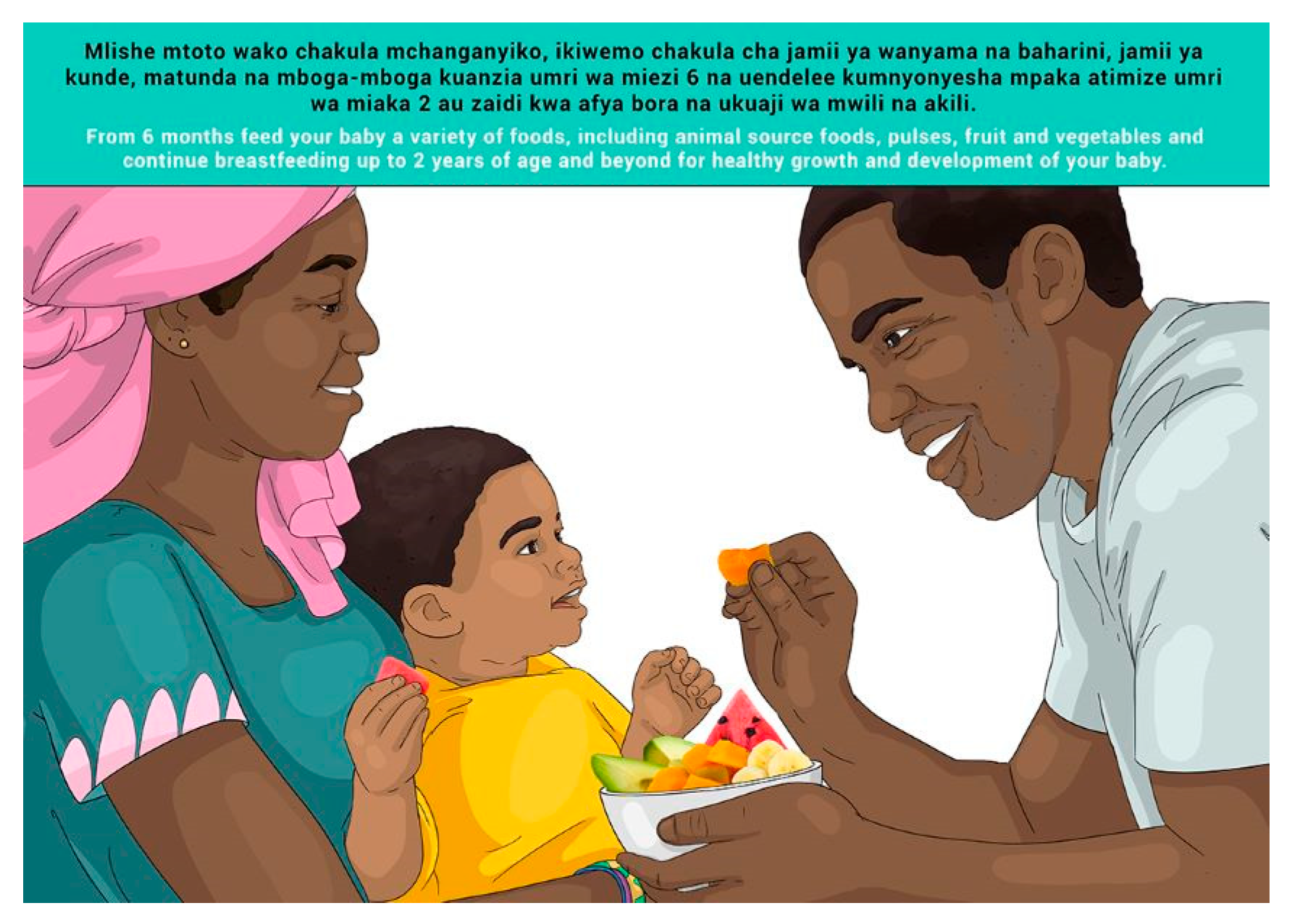
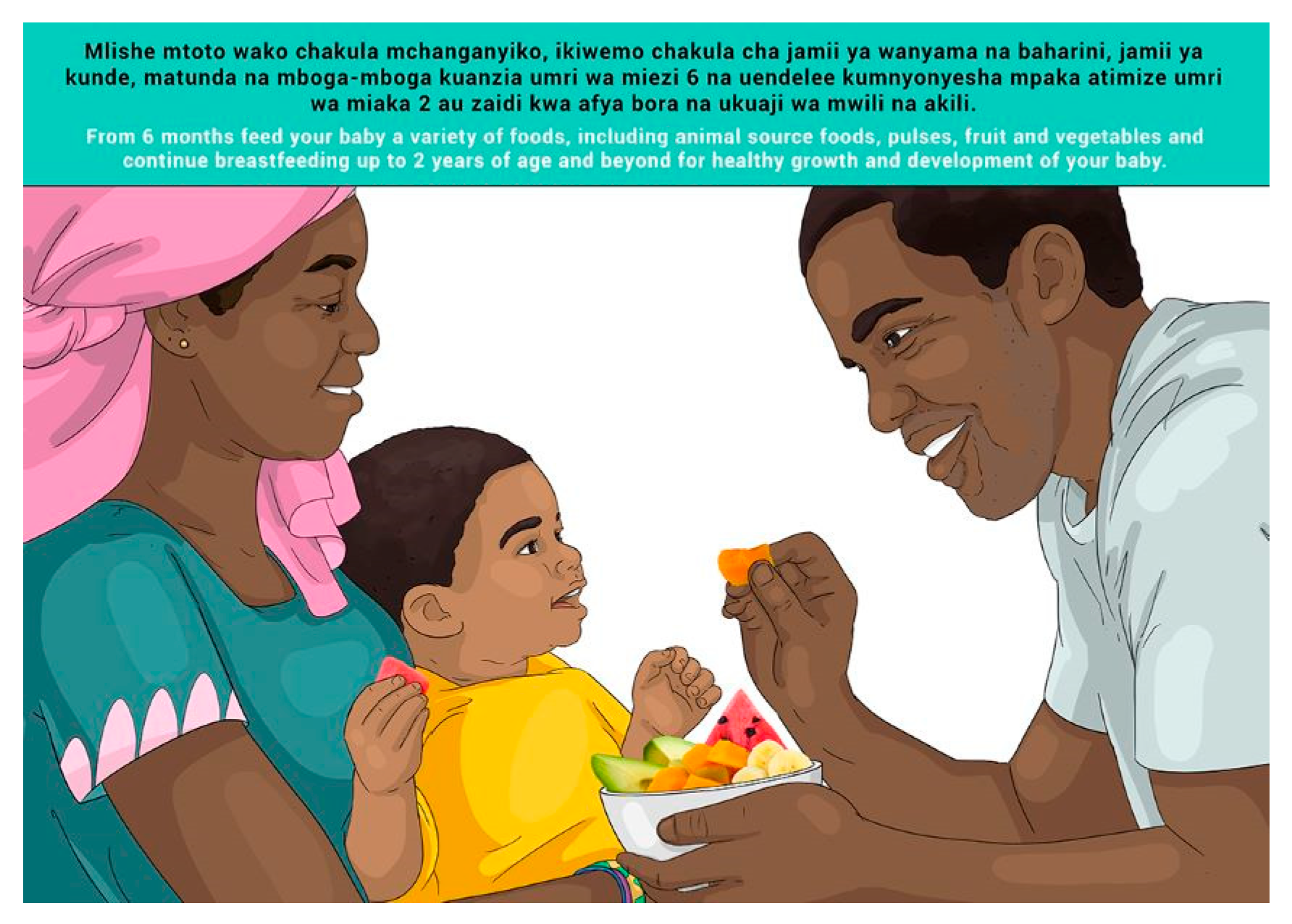
| 10 | E | From 6 months feed your baby a variety of foods, including animal source foods, pulses, fruit and vegetables and continue breastfeeding up to 2 years of age and beyond for healthy growth and development of your baby. |
| 10 | S | Mlishe mtoto wako chakula mchanganyiko, ikiwemo chakula cha jamii ya wanyama na baharini, jamii ya kunde, matunda na mboga-mboga kuanzia umri wa miezi 6 na uendelee kumnyonyesha mpaka atimize umri wa miaka 2 au zaidi kwa afya bora na ukuaji wa mwili na akili. |
| 11a | E | Encourage school-aged children to eat healthy snacks such as fresh fruit, vegetables and nuts. |
| 11a | S | Wahamasishe watoto wa umri wa kwenda shule kula vitafunwa (asusa) vilivyo bora kwa afya kama vile matunda, mbogamboga, karanga na korosho. |
| 11b | E | School-aged children should enjoy breakfast before school to enable them to be productive and perform well. |
| 11b | S | Watoto wanaokwenda shule wapewe kifungua kinywa (mlo wa asubuhi) kabla ya kwenda shule ili kuwawezesha kuwa na ufahamu mzuri na kufaulu. |
| 11c | Provide school-aged children with a lunchbox to take to school. | |
| 11c | Wafungie watoto wanaokwenda shule mlo wa kula shuleni. | |
| 12 | E | Keep your food, home environment and water safe and clean to prevent diseases. |
| 12 | S | Weka chakula, mazingira ya nyumbani na maji katika hali ya usafi na usalama ili kuzuia magonjwa. |
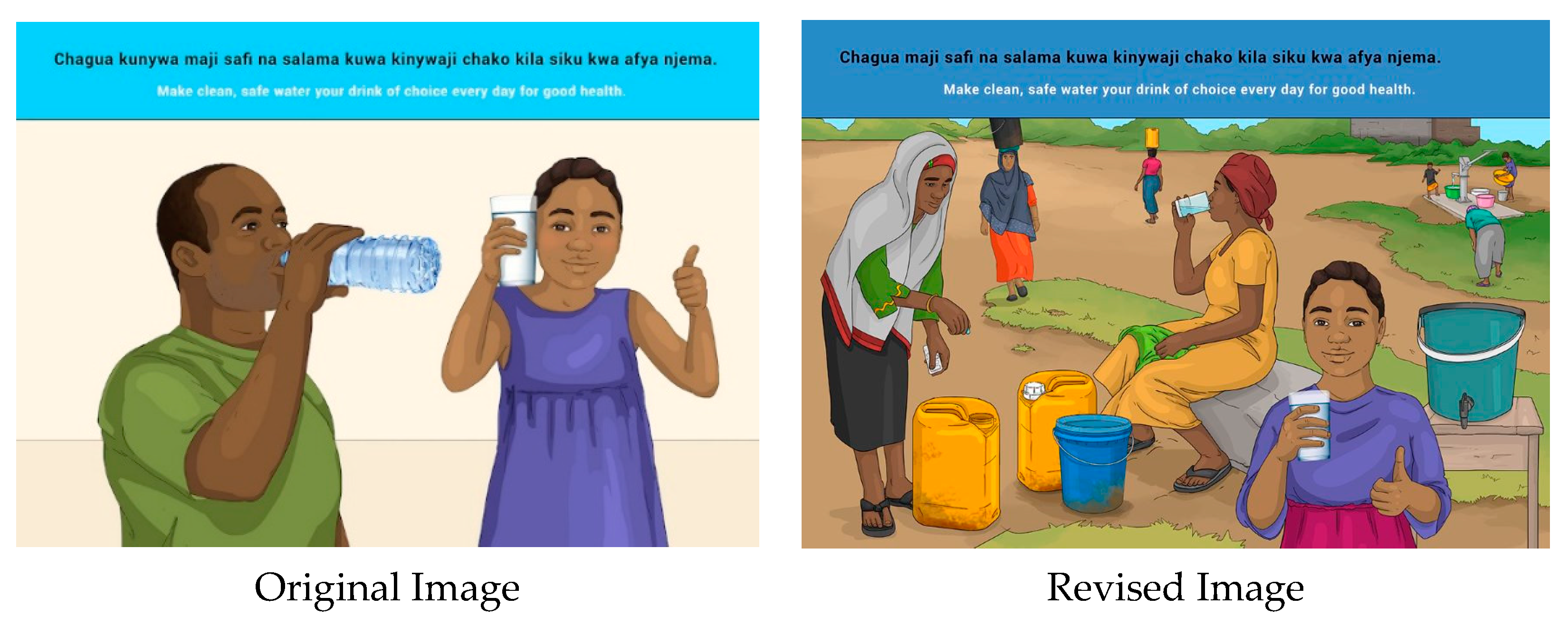
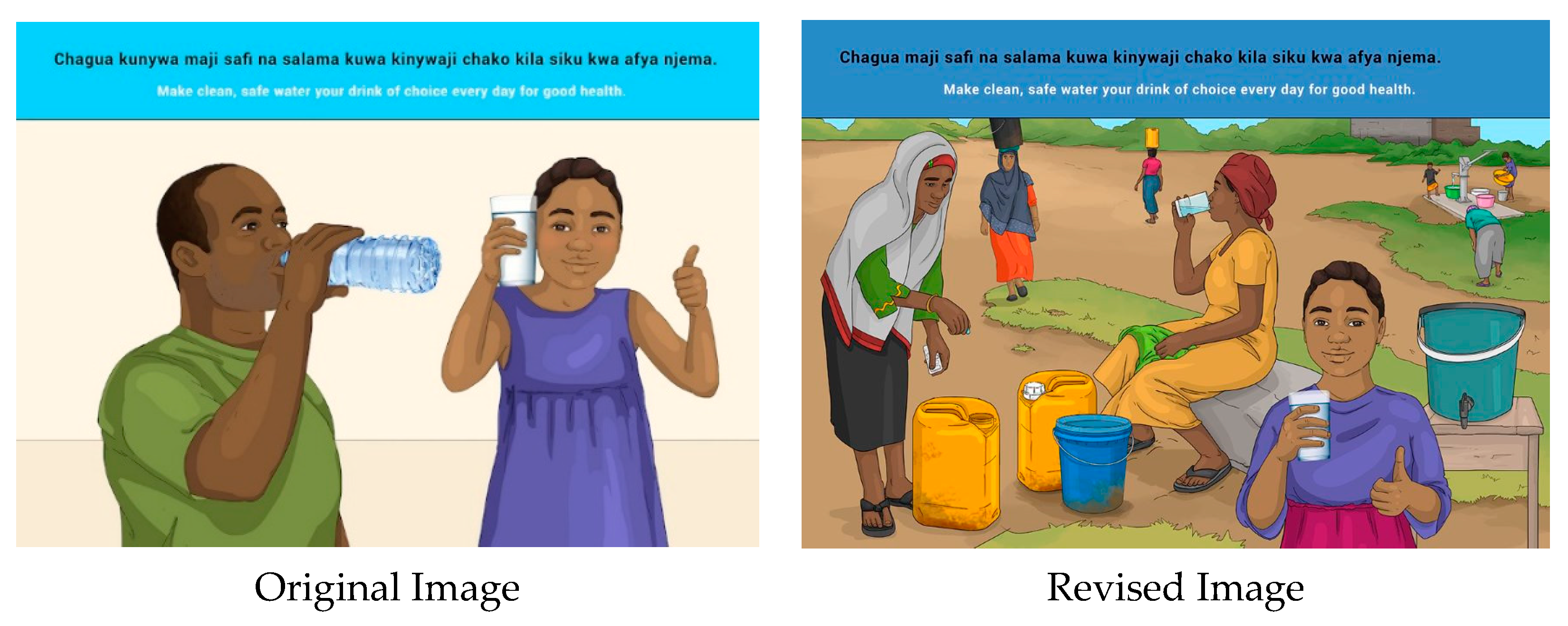
| 13 | E | Make clean, safe water your drink of choice every day for good health. |
| 13 | S | Chagua kunywa maji safi na salama kuwa kinywaji chako kila siku kwa afya njema. |
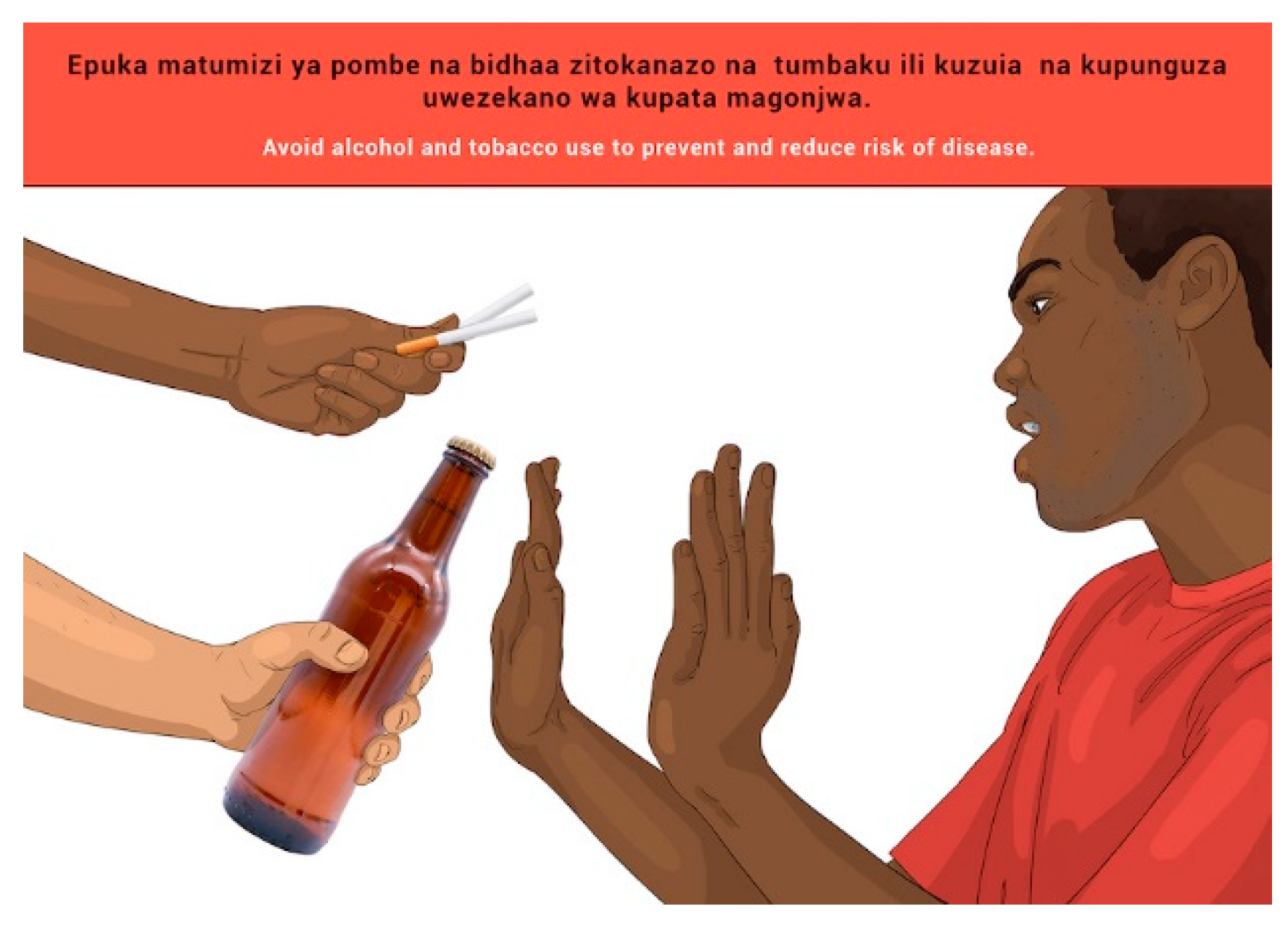
| 14 | E | Avoid drinking alcohol and tobacco use to prevent and reduce risk of diseases. |
| 14 | S | Epuka matumizi ya pombe na bidhaa zitokanazo na tumbaku ili kuzuia na kupunguza uwezekano wa kupata magonjwa. |
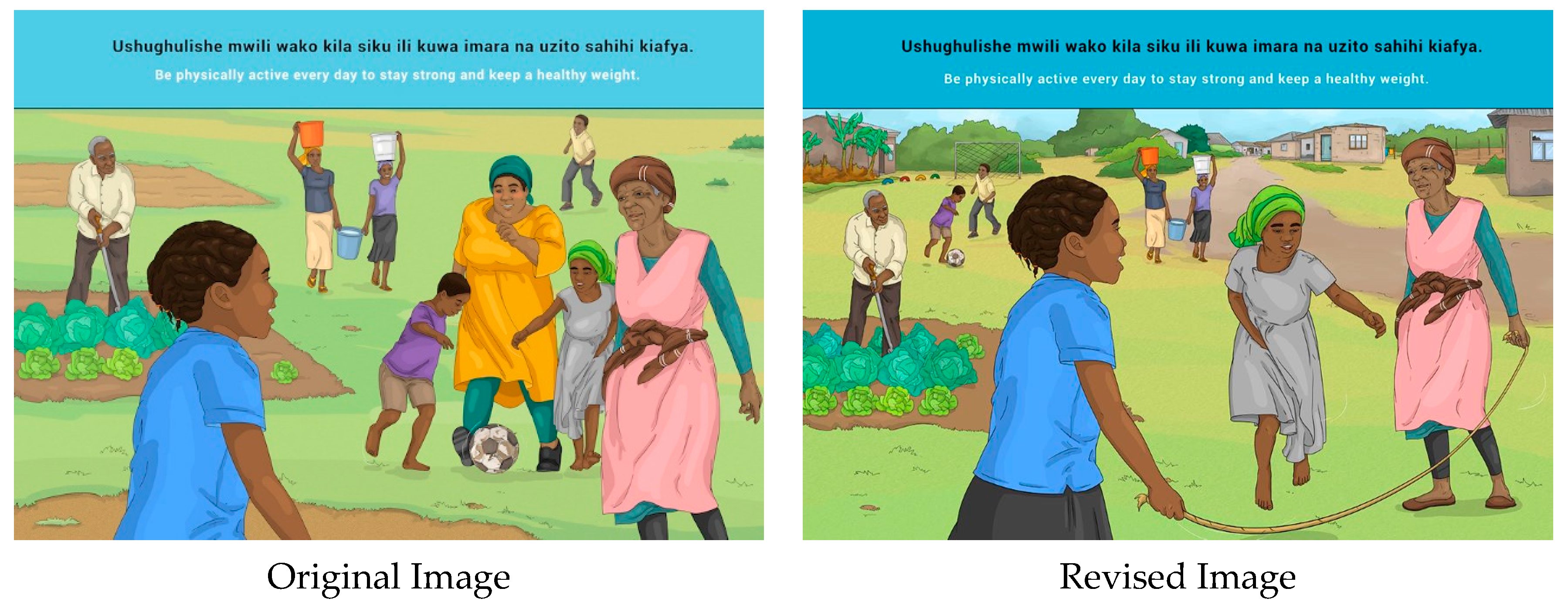
| 15 | E | Be physically active every day to stay strong and keep a healthy weight. |
| 15 | S | Ushughulishe mwili wako kila siku ili kuwa imara na uzito sahihi kiafya. |
| Variable | n (%) α | |
|---|---|---|
| District/region | Dar es Salaam | 96 (29.6) |
| Mwanza | 98 (30.5) | |
| Iringa | 72 (22.2) | |
| Kusini (Zanzibar) | 58 (17.9) | |
| Age | * Average age in years (Mean ± SD) | 35.01 ± 11.62 |
| Women with children | Yes | 277 (85.5) |
| No | 47 (14.5) | |
| Number of children | * Average number of children (mean ± SD) | 3.22 ± 2.30 |
| Ages of children | * Average age of children in years (mean ± SD) | 13.93 ± 10.48 |
| Mother/caregiver of children under 5 years of age | Yes | 174 (53.7) |
| No | 150 (46.3) | |
| Home Language | Kiswahili | 322 (99.4) |
| * missing data | 2 (0.6) | |
| Education status | None | 15 (4.6) |
| Primary school/Grade 1–7 | 196 (60.5) | |
| Secondary school/Grade 8–10 (Form i–iv) | 107 (33.0) | |
| Secondary school/Grade 11–12 (Form v–vi) | 2 (0.6) | |
| Diploma | 2 (0.6) | |
| Tertiary education (college, university) | 0 (0.0) | |
| * missing data | 2 (0.85) | |
| Employment status | Employed | 193 (59.6) |
| Unemployed | 76 (23.5) | |
| Unemployed, not looking for work | 55 (17.0) | |
| Role relating to food in the household | Provide or contribute money for food | 248 (76.5) |
| Decide what food should be bought or used in the house | 240 (74.1) | |
| Purchase food | 252 (77.8) | |
| Prepare food | 302 (93.2) | |
| Grow food for use in household | 212 (65.4) | |
| Grow food and sell produce for money | 158 (48.8) | |
| Other | 17 (5.2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© FAO, 2022. Licensee MDPI, Basel, Switzerland. This article is an open access publication distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/). The views expressed in this publication are those of the author(s) and do not necessarily reflect the views or policies of the Food and Agriculture Organization of the United Nations.
Share and Cite
Du Plessis, L.M.; Job, N.; Coetzee, A.; Fischer, S.; Chikoko, M.P.; Adam, M.; Love, P.; on behalf of the Food-Based Dietary Guideline (FBDG) Technical Working Group (TWG) Led by Tanzania Food and Nutrition Centre (TFNC). Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania. Nutrients 2022, 14, 2705. https://doi.org/10.3390/nu14132705
Du Plessis LM, Job N, Coetzee A, Fischer S, Chikoko MP, Adam M, Love P, on behalf of the Food-Based Dietary Guideline (FBDG) Technical Working Group (TWG) Led by Tanzania Food and Nutrition Centre (TFNC). Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania. Nutrients. 2022; 14(13):2705. https://doi.org/10.3390/nu14132705
Chicago/Turabian StyleDu Plessis, Lisanne M., Nophiwe Job, Angela Coetzee, Shân Fischer, Mercy P. Chikoko, Maya Adam, Penelope Love, and on behalf of the Food-Based Dietary Guideline (FBDG) Technical Working Group (TWG) Led by Tanzania Food and Nutrition Centre (TFNC). 2022. "Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania" Nutrients 14, no. 13: 2705. https://doi.org/10.3390/nu14132705
APA StyleDu Plessis, L. M., Job, N., Coetzee, A., Fischer, S., Chikoko, M. P., Adam, M., Love, P., & on behalf of the Food-Based Dietary Guideline (FBDG) Technical Working Group (TWG) Led by Tanzania Food and Nutrition Centre (TFNC). (2022). Development and Field-Testing of Proposed Food-Based Dietary Guideline Messages and Images amongst Consumers in Tanzania. Nutrients, 14(13), 2705. https://doi.org/10.3390/nu14132705