
Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
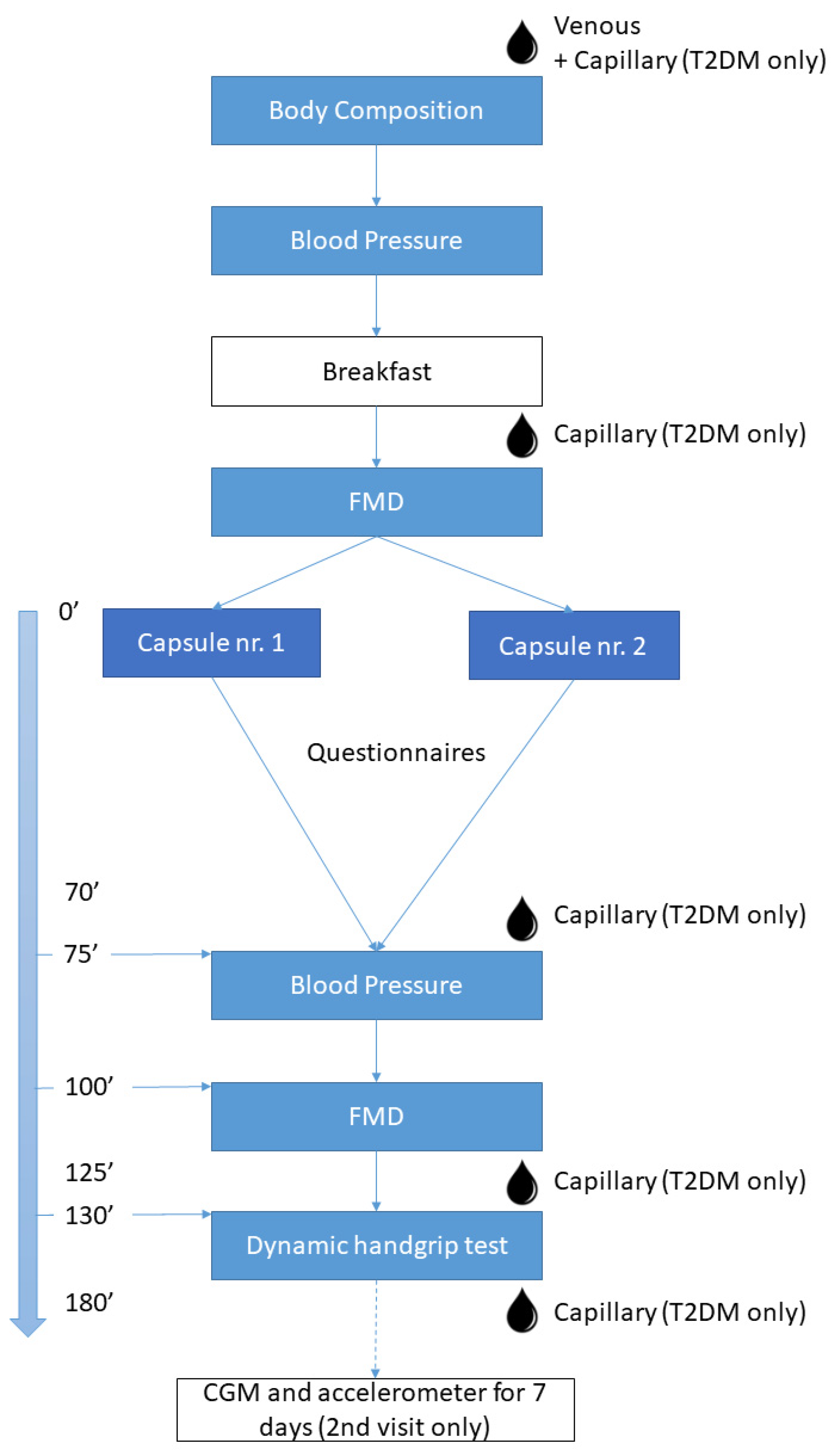
2.2. Trial Protocol
2.3. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
3.2. Results of Primary and Secondary Measurements
3.2.1. Macrovascular Reactivity: Flow-Mediated Dilation Test (FMD)—Primary Outcome
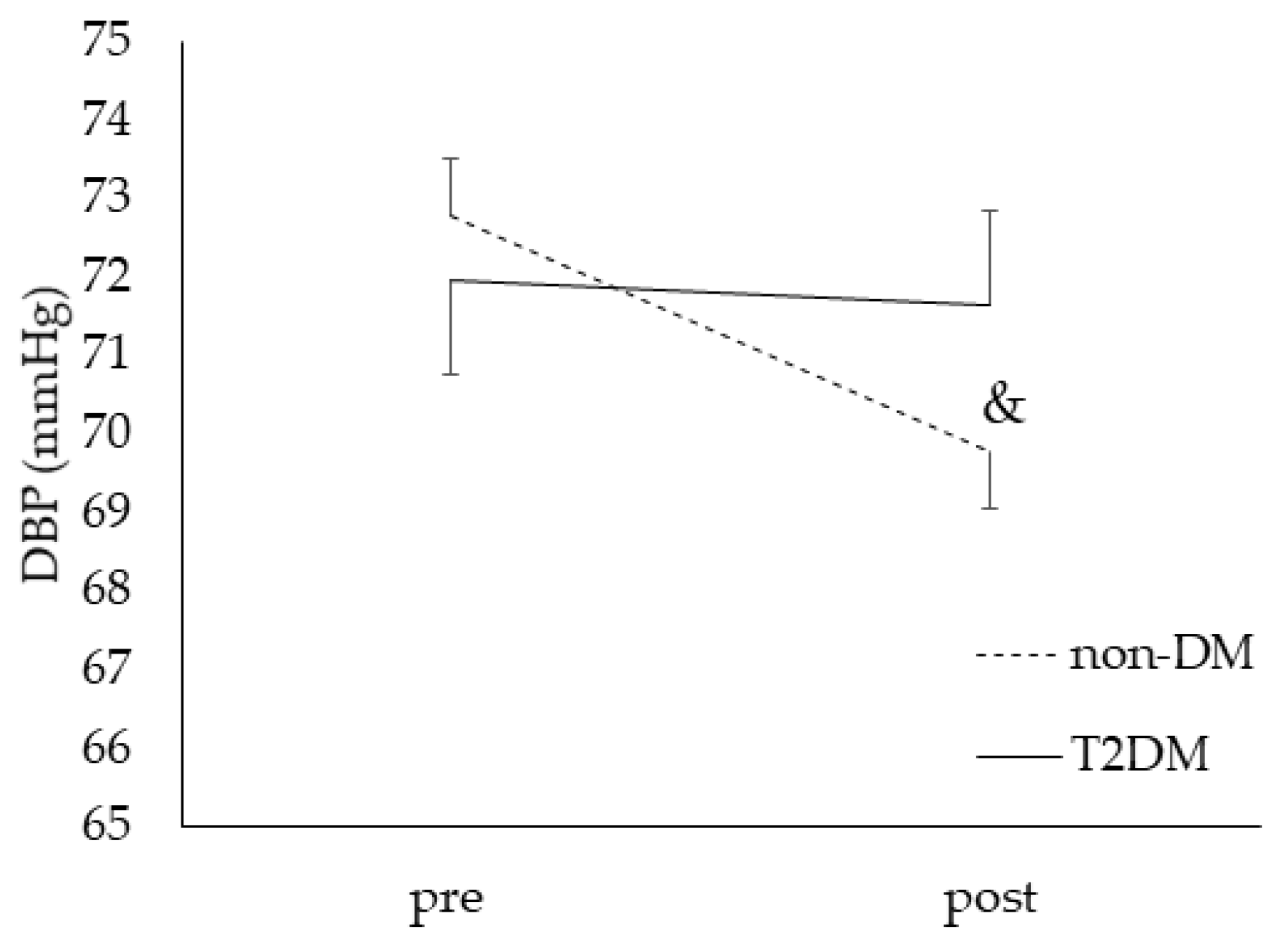
3.2.2. Blood Pressure Assessment—Secondary (Macrovascular) Outcome
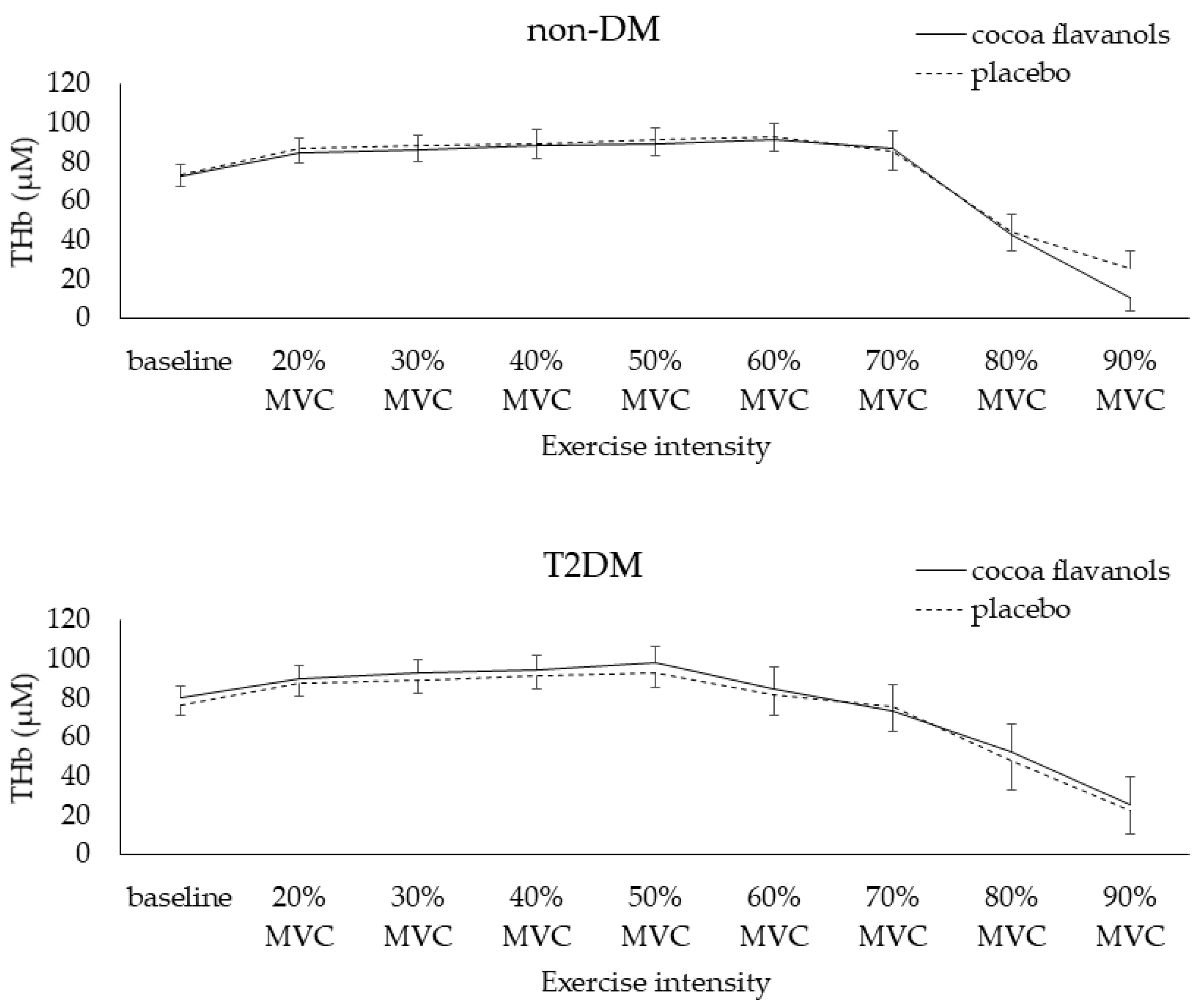
3.2.3. Microvascular Reactivity: Dynamic Handgrip Strength Test with Near-Infrared Spectroscopy—Secondary Outcome
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Koopmanschap, M. Coping with Type II diabetes: The patient’s perspective. Diabetologia 2002, 45, S21–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahia, L.R.; Araujo, D.V.; Schaan, B.D.; Dib, S.A.; Negrato, C.A.; Leão, M.P.; Ramos, A.J.S.; Forti, A.C.; Gomes, M.B.; Foss, M.C. The costs of type 2 diabetes mellitus outpatient care in the Brazilian public health system. Value Health 2011, 14, S137–S140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massi-Benedetti, M.; Board, C.-A. The cost of diabetes Type II in Europe: The CODE-2 Study. Diabetologia 2002, 45, S1–S4. [Google Scholar] [CrossRef] [Green Version]
- Tapas, A.R.; Sakarkar, D.; Kakde, R. Flavonoids as nutraceuticals: A review. Trop. J. Pharm. Res. 2008, 7, 1089–1099. [Google Scholar] [CrossRef]
- Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Rémésy, C. Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies. Am. J. Clin. Nutr. 2005, 81, 230S–242S. [Google Scholar] [CrossRef] [Green Version]
- Arts, I.C.; van de Putte, B.; Hollman, P.C. Catechin contents of foods commonly consumed in The Netherlands. 1. Fruits, vegetables, staple foods, and processed foods. J. Agric. Food Chem. 2000, 48, 1746–1751. [Google Scholar] [CrossRef] [PubMed]
- Ludovici, V.; Barthelmes, J.; Nägele, M.P.; Enseleit, F.; Ferri, C.; Flammer, A.J.; Ruschitzka, F.; Sudano, I. Cocoa, blood pressure, and vascular function. Front. Nutr. 2017, 4, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aprotosoaie, A.C.; Miron, A.; Trifan, A.; Luca, V.S.; Costache, I.I. The Cardiovascular Effects of Cocoa Polyphenols—An Overview. Diseases 2016, 4, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahn, S.E.; Cooper, M.E.; Del Prato, S. Pathophysiology and treatment of type 2 diabetes: Perspectives on the past, present, and future. Lancet 2014, 383, 1068–1083. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Schewe, T.; Steffen, Y.; Sies, H. How do dietary flavanols improve vascular function? A position paper. Arch. Biochem. Biophys. 2008, 476, 102–106. [Google Scholar] [CrossRef]
- Schroeter, H.; Heiss, C.; Balzer, J.; Kleinbongard, P.; Keen, C.L.; Hollenberg, N.K.; Sies, H.; Kwik-Uribe, C.; Schmitz, H.H.; Kelm, M. (-)-Epicatechin mediates beneficial effects of flavanol-rich cocoa on vascular function in humans. Proc. Natl. Acad. Sci. USA 2006, 103, 1024–1029. [Google Scholar] [CrossRef] [Green Version]
- Loke, W.M.; Hodgson, J.M.; Proudfoot, J.M.; McKinley, A.J.; Puddey, I.B.; Croft, K.D. Pure dietary flavonoids quercetin and (−)-epicatechin augment nitric oxide products and reduce endothelin-1 acutely in healthy men. Am. J. Clin. Nutr. 2008, 88, 1018–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Actis-Goretta, L.; Ottaviani, J.I.; Keen, C.L.; Fraga, C.G. Inhibition of angiotensin converting enzyme (ACE) activity by flavan-3-ols and procyanidins. FEBS Lett. 2003, 555, 597–600. [Google Scholar] [CrossRef] [Green Version]
- Oboh, G.; Ademosun, A.O.; Ademiluyi, A.O.; Omojokun, O.S.; Nwanna, E.E.; Longe, K.O. In vitro studies on the antioxidant property and inhibition of α-amylase, α-glucosidase, and angiotensin I-converting enzyme by polyphenol-rich extracts from cocoa (Theobroma cacao) bean. Pathol. Res. Int. 2014, 2014, 549287. [Google Scholar] [CrossRef]
- Actis-Goretta, L.; Ottaviani, J.I.; Fraga, C.G. Inhibition of angiotensin converting enzyme activity by flavanol-rich foods. J. Agric. Food Chem. 2006, 54, 229–234. [Google Scholar] [CrossRef]
- Persson, I.A.; Persson, K.; Hagg, S.; Andersson, R.G. Effects of cocoa extract and dark chocolate on angiotensin-converting enzyme and nitric oxide in human endothelial cells and healthy volunteers—A nutrigenomics perspective. J. Cardiovasc. Pharmacol. 2011, 57, 44–50. [Google Scholar] [CrossRef]
- Ebaditabar, M.; Djafarian, K.; Saeidifard, N.; Shab-Bidar, S. Effect of dark chocolate on flow-mediated dilatation: Systematic review, meta-analysis, and dose–response analysis of randomized controlled trials. Clin. Nutr. ESPEN 2020, 36, 17–27. [Google Scholar] [CrossRef]
- Grassi, D.; Desideri, G.; Necozione, S.; di Giosia, P.; Barnabei, R.; Allegaert, L.; Bernaert, H.; Ferri, C. Cocoa consumption dose-dependently improves flow-mediated dilation and arterial stiffness decreasing blood pressure in healthy individuals. J. Hypertens. 2015, 33, 294–303. [Google Scholar] [CrossRef]
- Heiss, C.; Finis, D.; Kleinbongard, P.; Hoffmann, A.; Rassaf, T.; Kelm, M.; Sies, H. Sustained increase in flow-mediated dilation after daily intake of high-flavanol cocoa drink over 1 week. J. Cardiovasc. Pharmacol. 2007, 49, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Ried, K.; Sullivan, T.R.; Fakler, P.; Frank, O.R.; Stocks, N.P. Effect of cocoa on blood pressure. Cochrane Database Syst. Rev. 2012, 8, CD008893. [Google Scholar]
- Jafarnejad, S.; Salek, M.; Clark, C.C. Cocoa consumption and blood pressure in middle-aged and elderly subjects: A meta-analysis. Curr. Hypertens. Rep. 2020, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Janszky, I.; Mukamal, K.; Ljung, R.; Ahnve, S.; Ahlbom, A.; Hallqvist, J. Chocolate consumption and mortality following a first acute myocardial infarction: The Stockholm Heart Epidemiology Program. J. Intern. Med. 2009, 266, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, N.K.; Fisher, N.D.; McCullough, M.L. Flavanols, the Kuna, cocoa consumption, and nitric oxide. J. Am. Soc. Hypertens. JASH 2009, 3, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Buijsse, B.; Feskens, E.J.; Kok, F.J.; Kromhout, D. Cocoa intake, blood pressure, and cardiovascular mortality: The Zutphen Elderly Study. Arch. Intern. Med. 2006, 166, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sansone, R.; Rodriguez-Mateos, A.; Heuel, J.; Falk, D.; Schuler, D.; Wagstaff, R.; Kuhnle, G.G.; Spencer, J.P.; Schroeter, H.; Merx, M.W. Cocoa flavanol intake improves endothelial function and Framingham Risk Score in healthy men and women: A randomised, controlled, double-masked trial: The Flaviola Health Study. Br. J. Nutr. 2015, 114, 1246–1255. [Google Scholar] [CrossRef]
- Jafari Azad, B.; Daneshzad, E.; Meysamie, A.P.; Koohdani, F. Chronic and acute effects of cocoa products intake on arterial stiffness and platelet count and function: A systematic review and dose-response Meta-analysis of randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 357–379. [Google Scholar] [CrossRef]
- Hooper, L.; Kay, C.; Abdelhamid, A.; Kroon, P.A.; Cohn, J.S.; Rimm, E.B.; Cassidy, A. Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: A systematic review and meta-analysis of randomized trials. Am. J. Clin. Nutr. 2012, 95, 740–751. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of a health claim related to cocoa flavanols and maintenance of normal endothelium-dependent vasodilation pursuant to Article 13(5) of Regulation (EC) No 1924/2006. EFSA J. 2012, 10, 2809. [Google Scholar] [CrossRef] [Green Version]
- Tanghe, A.; Heyman, E.; Wyngaert, K.V.; Van Ginckel, A.; Celie, B.; Rietzschel, E.; Calders, P.; Shadid, S. Evaluation of blood pressure lowering effects of cocoa flavanols in diabetes mellitus: A systematic review and meta-analysis. J. Funct. Foods 2021, 79, 104399. [Google Scholar] [CrossRef]
- Balzer, J.; Rassaf, T.; Heiss, C.; Kleinbongard, P.; Lauer, T.; Merx, M.; Heussen, N.; Gross, H.B.; Keen, C.L.; Schroeter, H.; et al. Sustained benefits in vascular function through flavanol-containing cocoa in medicated diabetic patients a double-masked, randomized, controlled trial. J. Am. Coll. Cardiol. 2008, 51, 2141–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basu, A.; Betts, N.M.; Leyva, M.J.; Fu, D.; Aston, C.E.; Lyons, T.J. Acute Cocoa Supplementation Increases Postprandial HDL Cholesterol and Insulin in Obese Adults with Type 2 Diabetes after Consumption of a High-Fat Breakfast. J. Nutr. 2015, 145, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Mellor, D.D.; Madden, L.A.; Smith, K.A.; Kilpatrick, E.S.; Atkin, S.L. High-polyphenol chocolate reduces endothelial dysfunction and oxidative stress during acute transient hyperglycaemia in Type 2 diabetes: A pilot randomized controlled trial. Diabet. Med. A J. Br. Diabet. Assoc. 2013, 30, 478–483. [Google Scholar] [CrossRef]
- Ferrannini, E.; Cushman, W.C. Diabetes and hypertension: The bad companions. Lancet 2012, 380, 601–610. [Google Scholar] [CrossRef]
- Tanghe, A.; Celie, B.; Shadid, S.; Rietzschel, E.; Op‘t Roodt, J.; Reesink, K.D.; Heyman, E.; Calders, P. Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension: A Protocol for an Acute, Randomized, Double-Blinded, Placebo-Controlled Cross-Over Trial. Front. Cardiovasc. Med. 2021, 8, 152. [Google Scholar] [CrossRef]
- Association, A.D. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- T’Joen, V.; Phlypo, S.; Bekaert, S. Bimetra Biobank: A High Quality Biobank Facility to Stimulate Translational Biomedical Research. Open J. Bioresour. 2018, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Monnier, L.; Colette, C.; Wojtusciszyn, A.; Dejager, S.; Renard, E.; Molinari, N.; Owens, D.R. Toward defining the threshold between low and high glucose variability in diabetes. Diabetes Care 2017, 40, 832–838. [Google Scholar] [CrossRef] [Green Version]
- Grassi, B.; Pogliaghi, S.; Rampichini, S.; Quaresima, V.; Ferrari, M.; Marconi, C.; Cerretelli, P. Muscle oxygenation and pulmonary gas exchange kinetics during cycling exercise on-transitions in humans. J. Appl. Physiol. 2003, 95, 149–158. [Google Scholar] [CrossRef]
- Cook, N.R. Implications of Small Reductions in Diastolic Blood Pressure for Primary Prevention. Arch. Intern. Med. 1995, 155, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Stamler, R. Implications of the INTERSALT study. Hypertension 1991, 17, I16–I20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whelton, P.K.; He, J.; Appel, L.J.; Cutler, J.A.; Havas, S.; Kotchen, T.A.; Roccella, E.J.; Stout, R.; Vallbona, C.; Winston, M.C.; et al. Primary prevention of hypertension: Clinical and public health advisory from The National High Blood Pressure Education Program. JAMA 2002, 288, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Allgrove, J.; Davison, G. Dark chocolate/cocoa polyphenols and oxidative stress. In Polyphenols in Human Health and Disease; Elsevier: Amsterdam, The Netherlands, 2014; pp. 241–251. [Google Scholar]
- Martin, M.Á.; Ramos, S. Impact of cocoa flavanols on human health. Food Chem. Toxicol. 2021, 151, 112121. [Google Scholar] [CrossRef]
- Kerimi, A.; Williamson, G. The cardiovascular benefits of dark chocolate. Vasc. Pharmacol. 2015, 71, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Hermann, F.; Spieker, L.; Ruschitzka, F.; Sudano, I.; Hermann, M.; Binggeli, C.; Lüscher, T.; Riesen, W.; Noll, G.; Corti, R. Dark chocolate improves endothelial and platelet function. Heart 2006, 92, 119–120. [Google Scholar] [CrossRef] [Green Version]
- Heiss, C.; Kleinbongard, P.; Dejam, A.; Perre, S.; Schroeter, H.; Sies, H.; Kelm, M. Acute consumption of flavanol-rich cocoa and the reversal of endothelial dysfunction in smokers. J. Am. Coll. Cardiol. 2005, 46, 1276–1283. [Google Scholar] [CrossRef] [Green Version]
- Heiss, C.; Dejam, A.; Kleinbongard, P.; Schewe, T.; Sies, H.; Kelm, M. Vascular effects of cocoa rich in flavan-3-ols. JAMA 2003, 290, 1030–1031. [Google Scholar] [CrossRef]
- Berry, N.M.; Davison, K.; Coates, A.M.; Buckley, J.D.; Howe, P.R. Impact of cocoa flavanol consumption on blood pressure responsiveness to exercise. Br. J. Nutr. 2010, 103, 1480–1484. [Google Scholar] [CrossRef]
- Faridi, Z.; Njike, V.Y.; Dutta, S.; Ali, A.; Katz, D.L. Acute dark chocolate and cocoa ingestion and endothelial function: A randomized controlled crossover trial. Am. J. Clin. Nutr. 2008, 88, 58–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; Alexopoulos, N.; Economou, E.; Andreadou, I.; Stefanadis, C. Effect of dark chocolate on arterial function in healthy individuals. Am. J. Hypertens. 2005, 18, 785–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westphal, S.; Luley, C. Flavanol-rich cocoa ameliorates lipemia-induced endothelial dysfunction. Heart Vessel. 2011, 26, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Rowe, J.W. Clinical consequences of age-related impairments in vascular compliance. Am. J. Cardiol. 1987, 60, G68–G71. [Google Scholar] [CrossRef]
- Cooper, K.A.; Campos-Giménez, E.; Jiménez Alvarez, D.; Rytz, A.; Nagy, K.; Williamson, G. Predictive relationship between polyphenol and nonfat cocoa solids content of chocolate. J. Agric. Food Chem. 2008, 56, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Schroeter, H.; Holt, R.R.; Orozco, T.J.; Schmitz, H.H.; Keen, C.L. Milk and absorption of dietary flavanols. Nature 2003, 426, 787–788. [Google Scholar] [CrossRef] [PubMed]
- Serafini, M.; Crozier, A. Nutrition—Milk and absorption of dietary flavanols—Reply. Nature 2003, 426, 788. [Google Scholar] [CrossRef]
- Serafini, M.; Bugianesi, R.; Maiani, G.; Valtuena, S.; De Santis, S.; Crozier, A. Plasma antioxidants from chocolate. Nature 2003, 424, 1013. [Google Scholar] [CrossRef]
- Schramm, D.D.; Karim, M.; Schrader, H.R.; Holt, R.R.; Kirkpatrick, N.J.; Polagruto, J.A.; Ensunsa, J.L.; Schmitz, H.H.; Keen, C.L. Food effects on the absorption and pharmacokinetics of cocoa flavanols. Life Sci. 2003, 73, 857–869. [Google Scholar] [CrossRef]
- Rodriguez-Mateos, A.; Oruna-Concha, M.J.; Kwik-Uribe, C.; Vidal, A.; Spencer, J.P. Influence of sugar type on the bioavailability of cocoa flavanols. Br. J. Nutr. 2012, 108, 2243–2250. [Google Scholar] [CrossRef] [Green Version]
- Monahan, K.D.; Feehan, R.P.; Kunselman, A.R.; Preston, A.G.; Miller, D.L.; Lott, M.E. Dose-dependent increases in flow-mediated dilation following acute cocoa ingestion in healthy older adults. J. Appl. Physiol. 2011, 111, 1568–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, D.; Necozione, S.; Lippi, C.; Croce, G.; Valeri, L.; Pasqualetti, P.; Desideri, G.; Blumberg, J.B.; Ferri, C. Cocoa reduces blood pressure and insulin resistance and improves endothelium-dependent vasodilation in hypertensives. Hypertension 2005, 46, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grassi, D.; Desideri, G.; Necozione, S.; Lippi, C.; Casale, R.; Properzi, G.; Blumberg, J.B.; Ferri, C. Blood pressure is reduced and insulin sensitivity increased in glucose-intolerant, hypertensive subjects after 15 days of consuming high-polyphenol dark chocolate. J. Nutr. 2008, 138, 1671–1676. [Google Scholar] [CrossRef]
- Smit, H.J. Theobromine and the pharmacology of cocoa. In Methylxanthines; Springer: Berlin/Heidelberg, Germany, 2011; pp. 201–234. [Google Scholar]
- Echeverri, D.; Montes, F.R.; Cabrera, M.; Galan, A.; Prieto, A. Caffeine’s Vascular Mechanisms of Action. Int. J. Vasc. Med. 2010, 2010, 834060. [Google Scholar] [CrossRef] [Green Version]
- Francis, S.H.; Sekhar, K.R.; Ke, H.; Corbin, J.D. Inhibition of cyclic nucleotide phosphodiesterases by methylxanthines and related compounds. In Methylxanthines; Springer: Berlin/Heidelberg, Germany, 2011; pp. 93–133. [Google Scholar]
- Franco, R.; Oñatibia-Astibia, A.; Martínez-Pinilla, E. Health benefits of methylxanthines in cacao and chocolate. Nutrients 2013, 5, 4159–4173. [Google Scholar] [CrossRef] [Green Version]
- Thijssen, D.H.; Black, M.A.; Pyke, K.E.; Padilla, J.; Atkinson, G.; Harris, R.A.; Parker, B.; Widlansky, M.E.; Tschakovsky, M.E.; Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H2–H12. [Google Scholar] [CrossRef] [Green Version]
- de Koning, E.J.; Rabelink, T.J. Endothelial function in the post-prandial state. Atheroscler. Suppl. 2002, 3, 11–16. [Google Scholar] [CrossRef]
- Association, A.D. Postprandial blood glucose. Diabetes Care 2001, 24, 775–778. [Google Scholar] [CrossRef] [Green Version]
- Tomiyama, H.; Yamashina, A. Non-invasive vascular function tests: Their pathophysiological background and clinical application. Circ. J. 2010, 74, 24–33. [Google Scholar] [CrossRef] [Green Version]
- Herrington, D.M.; Fan, L.; Drum, M.; Riley, W.A.; Pusser, B.E.; Crouse, J.R.; Burke, G.L.; McBurnie, M.A.; Morgan, T.M.; Espeland, M.A. Brachial flow-mediated vasodilator responses in population-based research: Methods, reproducibility and effects of age, gender and baseline diameter. J. Cardiovasc. Risk 2001, 8, 319–328. [Google Scholar] [CrossRef]
- Ren, Y.; Liu, Y.; Sun, X.Z.; Wang, B.Y.; Zhao, Y.; Liu, D.C.; Zhang, D.D.; Liu, X.J.; Zhang, R.Y.; Sun, H.H.; et al. Chocolate consumption and risk of cardiovascular diseases: A meta-analysis of prospective studies. Heart 2019, 105, 49–55. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-DM | T2DM | |
|---|---|---|
| N | 24 | 11 |
Sex (  / /  ) ) | 14/10 | 4/7 |
| Age (years) | 59. 5 ± 5.5 | 66.7 ± 6.1 * |
| Weight (kg) | 77.1 ± 14.1 | 77.6 ± 13.7 |
| BMI (kg·m−2) | 26.4 ± 4.5 | 26.2 ± 3.0 |
| Fat mass (%) | 31.9 ± 9.1 | 29.7 ± 5.6 |
| Waist-to-hip ratio | 0.91 ± 0.06 | 0.95 ± 0.11 * |
| Baseline SBP (mmHg) | 116.0 ± 10.9 | 125.1 ± 14.7 * |
| Baseline DBP (mmHg) | 73.5 ± 7.5 | 75.1 ± 8.2 |
| Baseline Mean arterial pressure (mmHg) | 87.7 ± 8.4 | 91.8 ± 10.1 |
| HbA1c (%) | 5.8 ± 0.3 | 6.9 ± 0.7 |
| Duration diabetes (years) | NA | 9.3 ± 5.5 |
| Antihyperglycemic drugs (n): Metformin Sulfonylurea DPP4- inhibitors GLP-1- RA SGLT-2 Insulin | NA | 10 9 2 0 2 1 1 |
| Duration of hypertension (years) | 7.5 ± 5.5 | 9.0 ± 3.2 |
| Antihypertensive drugs (n)(%): ACEi ARB | 15 (62.5%) 11 4 | 4 (36.4%) 1 3 |
| Lipid-lowering drugs (n)(%): HMG-CoA reductase inhibitors Fibrates | 5 (20.8%) 4 1 | 7 (63.6%) * 7 0 |
| History of smoking (years) | 3.3 ± 6.7 | 8.8 ± 14.7 [0–40] |
| Non-DM | T2DM | |||
|---|---|---|---|---|
| CF | Placebo | CF | Placebo | |
| Glucose (mg/dL) | 97.0 ± 8.0 | 96.2 ± 9.1 | 127.7 ± 20.6 * | 127.4 ± 17.0 * |
| Insulin (mU/L) | 10.3 ± 6.6 | 9.8 ± 5.3 | 9.5 ± 6.1 | 9.5 ± 6.0 |
| HOMA a | 2.4 ± 1.6 | 2.4 ± 1.4 | 3.1 ± 2.1 | 3.0 ± 1.8 |
| Triglycerides (mg/dL) | 109.9 ± 38.4 | 106.9 ± 42.1 | 135.9 ± 72.2 | 112.1 ± 41.3 # |
| FFA (mmol/L) | 0.55 ± 0.16 | 0.54 ± 0.20 | 0.57 ± 0.16 | 0.55 ± 0.15 |
| HDL-cholesterol (mg/dL) | 57.8 ± 18.7 | 57.9 ± 14.8 | 52.6 ± 14.4 | 53.8 ± 17.3 |
| LDL-cholesterol (mg/dL) b | 126.2 ± 35.8 | 124.2 ± 36.4 | 89.7 ± 31.5 * | 92.6 ± 30.7 * |
| Total cholesterol (mg/dL) | 206.0 ± 47.5 | 203.5 ± 45.9 | 169.5 ± 39.5 * | 168.8 ± 41.3 * |
| Uric acid (mg/dL) | 4.7 ± 0.9 | 4.9 ± 1.3 | 5.1 ± 1.1 | 5.2 ± 1.0 |
| CRP (mg/dL) | 2.3 ± 3.4 | 2.8 ± 4.6 | 1.8 ± 1.0 | 1.5 ± 0.6 |
| Vitamin C (mg/dL) | 0.7 ± 0.3 | 0.7 ± 0.4 | 0.5 ± 0.3 * | 0.6 ± 0.3 |
| Vitamin A (µg/dL) c Vitamin E (mg/dL) c | 67.5 ± 13.1 1.3 ± 0.3 | 74.4 ± 15.2 1.2 ± 0.3 | ||
| Haptoglobin (g/L) c | 1.0 ± 0.4 | 1.2 ± 0.6 | ||
| Non-DM | T2DM | |
|---|---|---|
| Accelerometry: | ||
| Wearing time (min/day) | 874.9 ± 16.5 | 842.2 ± 50.9 |
| Valid days (days/week) | 6.8 ± 0.5 | 6.6 ± 0.9 |
| Step counts (n/day) | 7521.1 ± 2690.3 | 6593.8 ± 2279.1 |
| Moderate (min/week) | 316.6 ± 219.5 | 186.4 ± 145.2 |
| Vigorous (min/week) | 6.3 ± 14.2 | 6.5 ± 17.4 |
| Very vigorous (min/week) | 0.8 ± 3.5 | 1.3 ± 4.2 |
| MVPA (min/week) | 323.7 ± 225.9 | 194.2 ± 149.3 |
| Continuous Glucose Monitoring System: | ||
| Glycemic excursions: % time in range (70–180 mg/dL) % time in hypoglycemic range <70 mg/dL % time in hyperglycemic range >180 mg/dL >250 mg/dL | 97.1 ± 3.4 1.1 ± 1.8 1.8 ± 3.0 0.2 ± 0.4 | 83.9 ± 14.0 * 0.7 ± 2.2 * 15.4 ± 14.1 * 1.4 ± 1.8 * |
| Glycemic variability: Coefficient of variation (%) a MAGE (mg/dL) | 17.4 ± 6.8 45.1 ± 21.1 | 22.9 ± 7.0 * 79.4 ± 23.7 * |
| Data sufficiency (%) | 99.9 ± 0.4 | 99.9 ± 0.1 |
| Non-DM | T2DM | |||
|---|---|---|---|---|
| CF | Placebo | CF | Placebo | |
| Macrovascular reactivity: | ||||
| FMD-test: diameter of brachial artery (BAD) | ||||
| Baseline BAD (mm) | ||||
| Before capsule Post capsule | 3.8 ± 0.1 3.9 ± 0.1 | 3.8 ± 0.1 3.8 ± 0.1 | 3.9 ± 0.2 4.1 ± 0.2 | 4.1 ± 0.2 4.1 ± 0.3 |
| Peak BAD (mm) | ||||
| Pre intake Post intake | 4.0 ± 0.1 4.1 ± 0.2 | 3.9 ± 0.1 4.1 ± 0.1 | 4.2 ± 0.2 4.3 ± 0.2 | 4.2 ± 0.2 4.3 ± 0.2 |
| Difference BAD (µm) (peak–baseline) | ||||
| Pre intake Post intake | 158.0 ± 25.7 189.0 ± 32.9 & | 161.3 ± 25.5 244.4 ± 35.8 & | 260.5 ± 91.0 132.7 ± 29.7 | 165.6 ± 56.1 171.7 ± 30.4 |
| FMD (%) [((peak BAD–baseline BAD))/baseline BAD) x 100] | ||||
| Pre intake Post intake | 4.3 ± 0.8 4.8 ± 0.8 | 4.6 ± 0.9 6.7 ± 1.0 | 7.4 ± 2.9 3.3 ± 0.8 | 4.0 ± 1.2 4.6 ± 1.0 |
| Blood pressure (BP) and heart rate | ||||
| SBP (mmHg) Pre intake Post intake | 114.1 ± 2.6 110.4 ± 2.3 | 114.4 ± 2.4 110.3 ± 2.1 | 122.3 ± 3.7 119.6 ± 3.1 | 123.5 ± 4.5 121.8 ± 3.5 |
| DBP (mmHg) Pre intake Post intake | 71.7 ± 1.7 69.2 ± 1.6 & | 72.4 ± 1.6 68.8 ± 1.4 & | 73.4 ± 1.9 73.2 ± 1.6 | 74.0 ± 2.6 73.7 ± 1.8 |
| Mean arterial pressure [DBP + (1/3 x Pule pressure)] | ||||
| Pre intake Post intake | 85.8 ± 1.9 82.9 ± 1.7 | 86.4 ± 1.8 82.6 ± 1.6 | 89.7 ± 2.5 88.6 ± 2.0 | 90.5 ± 3.2 89.7 ± 2.3 |
| Pulse pressure (mmHg) (SBP–DBP) | ||||
| Pre intake Post intake | 42.4 ± 1.3 41.3 ± 1.1 | 41.9 ± 1.2 41.5 ± 1.1 | 48.9 ± 2.2 46.4 ± 1.9 | 49.4 ± 2.3 48.1 ± 2.2 |
| Heart rate (bpm) Pre intake Post intake | 62.1 ± 1.6 66.4 ± 1.7 | 64.5 ± 1.6 67.3 ± 1.7 | 65.0 ± 3.5 70.5 ± 3.6 | 63.6 ± 2.7 67.5 ± 2.9 |
| Non-DM | T2DM | |||||||
|---|---|---|---|---|---|---|---|---|
| Without AHD | With AHD | Without AHD | With AHD | |||||
| CF | Placebo | CF | Placebo | CF | Placebo | CF | Placebo | |
| Microvascular reactivity: Muscle vasoreactivity to exercise | ||||||||
| THb (µM) Baseline | 63.1 ± 5.7 | 66.9 ± 7.8 | 77.4 ± 9.4 | 77.9 ± 9.3 | 81.3 ± 6.8 | 76.7 ± 6.2 | 79.2 ± 11.5 | 75.3 ± 9.9 |
| Maximal | 83.9 ± 7.7 | 90.9 ± 10.5 | 101.5 ± 12.4 | 102.3 ± 11.5 | 102.4 ± 8.7 | 93.6 ± 8.1 | 101.8 ± 16.3 | 100.7 ± 13.7 |
| Difference (maximal–baseline) | ||||||||
| 20.8 ± 2.5 | 24.0 ± 4.2 # | 24.1 ± 4.2 | 24.5 ± 3.1 | 21.1 ± 2.2 | 17.0 ± 2.5 | 22.6 ± 6.3 | 25.5 ± 3.9 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanghe, A.; Heyman, E.; Lespagnol, E.; Stautemas, J.; Celie, B.; Op ‘t Roodt, J.; Rietzschel, E.; Dias Soares, D.; Hermans, N.; Tuenter, E.; et al. Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension. Nutrients 2022, 14, 2692. https://doi.org/10.3390/nu14132692
Tanghe A, Heyman E, Lespagnol E, Stautemas J, Celie B, Op ‘t Roodt J, Rietzschel E, Dias Soares D, Hermans N, Tuenter E, et al. Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension. Nutrients. 2022; 14(13):2692. https://doi.org/10.3390/nu14132692
Chicago/Turabian StyleTanghe, Anouk, Elsa Heyman, Elodie Lespagnol, Jan Stautemas, Bert Celie, Jos Op ‘t Roodt, Ernst Rietzschel, Danusa Dias Soares, Nina Hermans, Emmy Tuenter, and et al. 2022. "Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension" Nutrients 14, no. 13: 2692. https://doi.org/10.3390/nu14132692
APA StyleTanghe, A., Heyman, E., Lespagnol, E., Stautemas, J., Celie, B., Op ‘t Roodt, J., Rietzschel, E., Dias Soares, D., Hermans, N., Tuenter, E., Shadid, S., & Calders, P. (2022). Acute Effects of Cocoa Flavanols on Blood Pressure and Peripheral Vascular Reactivity in Type 2 Diabetes Mellitus and Essential Hypertension. Nutrients, 14(13), 2692. https://doi.org/10.3390/nu14132692