
Sclerostin in Excessive Drinkers: Relationships with Liver Function and Body Composition

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Ethanol Consumption and Markers of Excessive Drinking
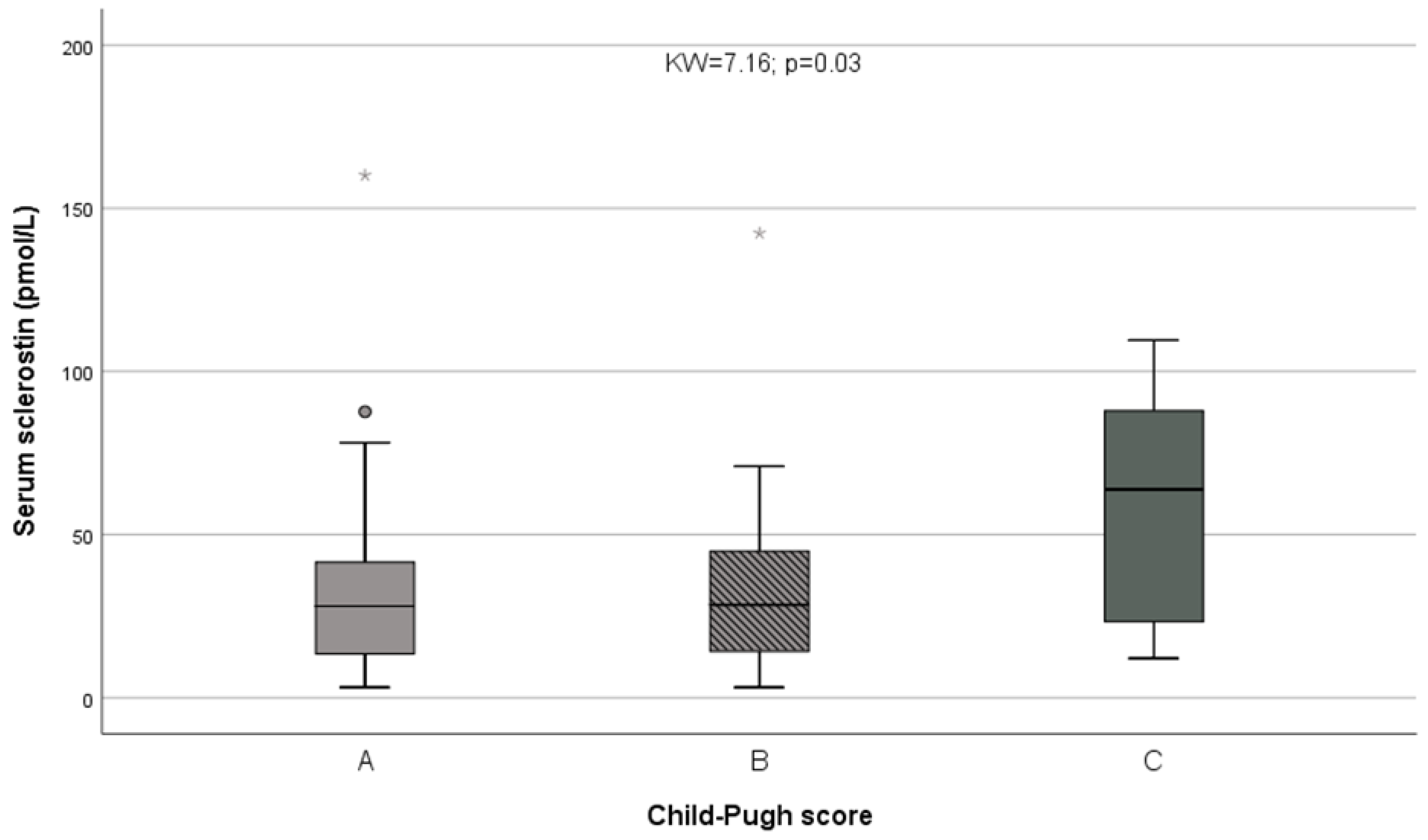
3.2. Liver Function
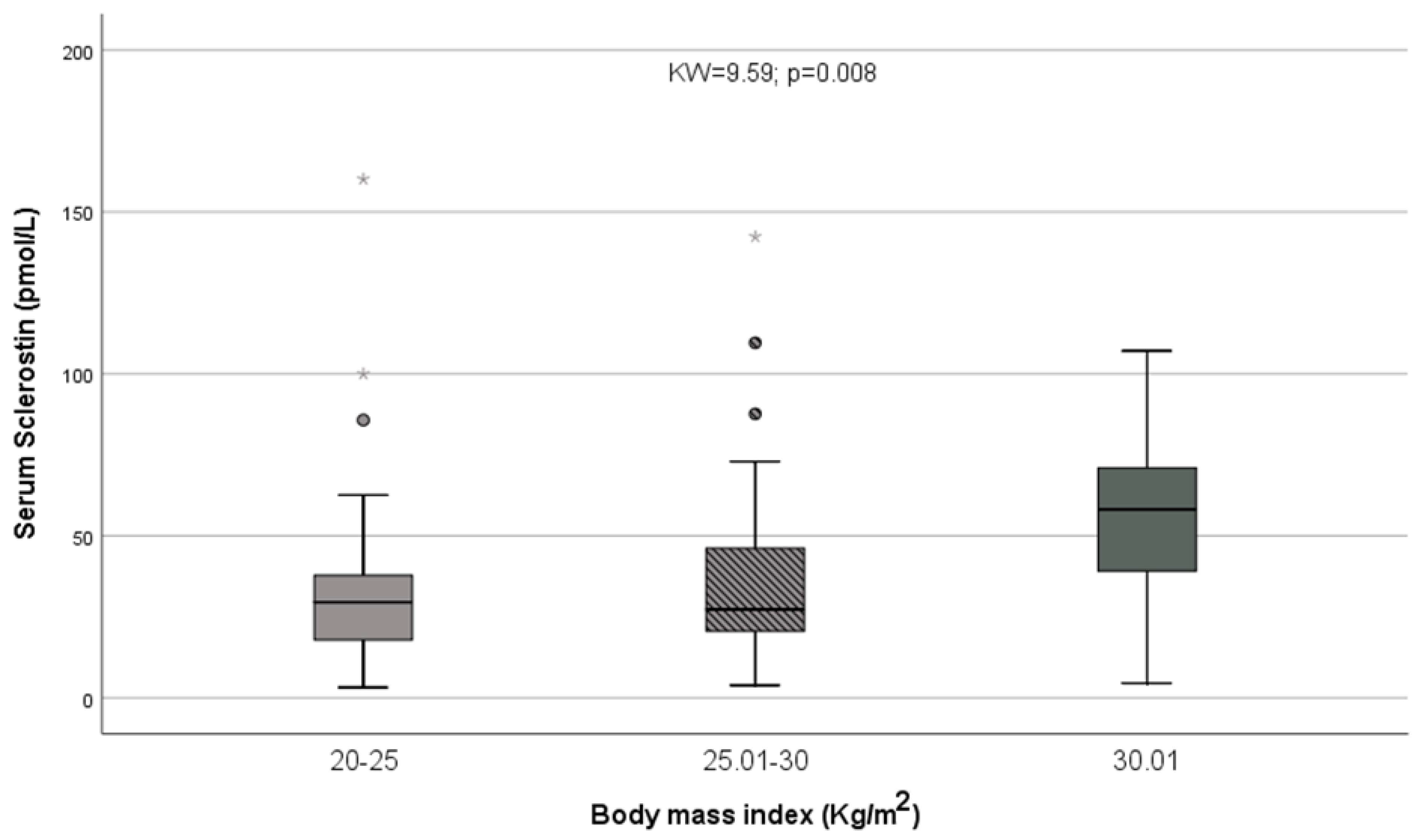
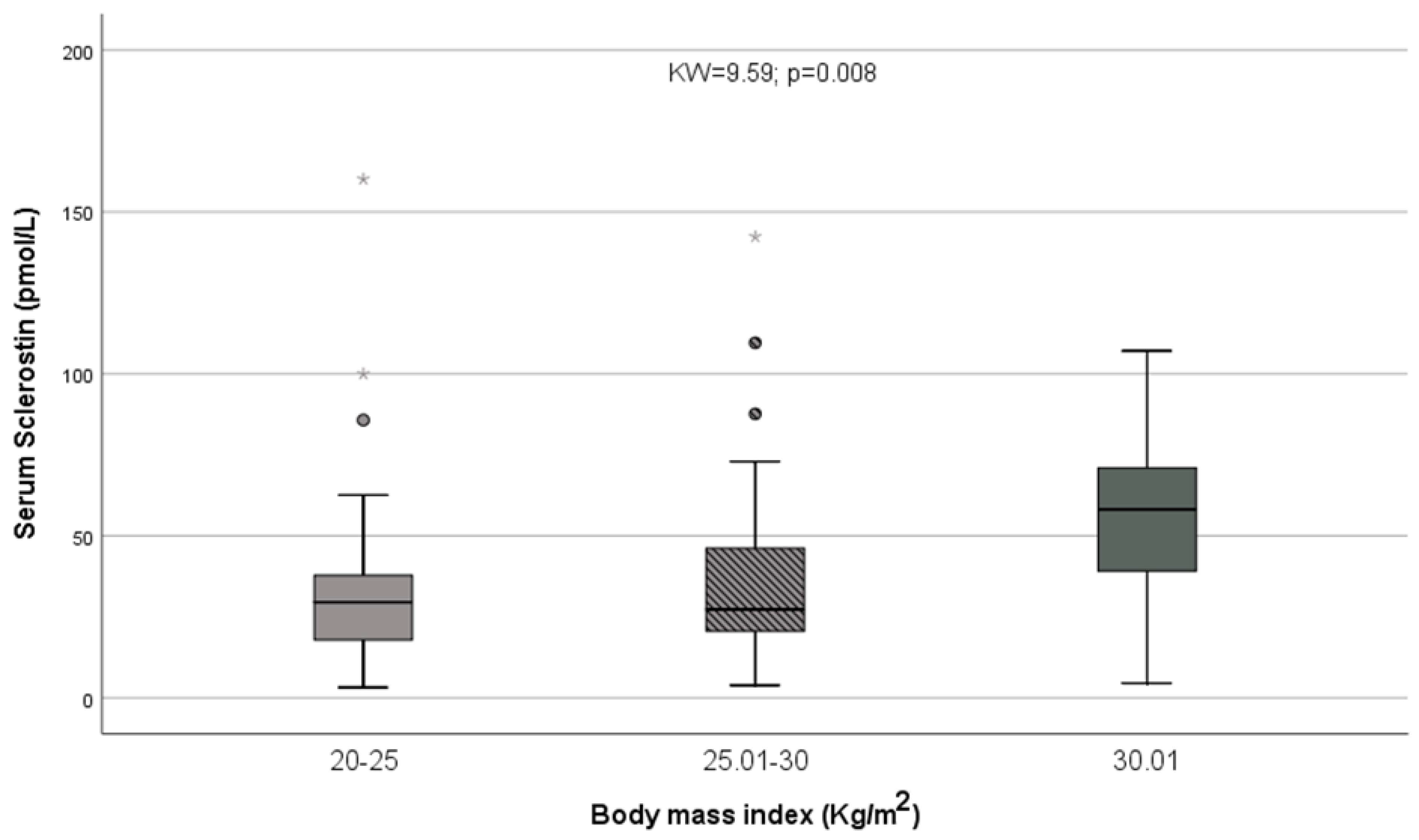
3.3. Body Composition/Nutritional Status
3.4. Relationships with Hypertension, Diabetes, Serum Lipids and Uric Acid
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, B.T.; Tamai, K.; He, X. Wnt/β-catenin signaling: Components, mechanisms, and diseases. Dev. Cell 2009, 17, 9–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, S.; Matsumoto, T. Sclerostin: From bench to bedside. J. Bone Miner. Metab. 2020, 39, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Fabre, S.; Funck-Brentano, T.; Cohen-Solal, M. Anti-sclerostin antibodies in osteoporosis and other bone diseases. J. Clin. Med. 2020, 9, 3439. [Google Scholar] [CrossRef] [PubMed]
- Wijenayaka, A.R.; Kogawa, M.; Lim, H.P.; Bonewald, L.F.; Findlay, D.E.M.; Atkins, G.J. Sclerostin stimulates osteocyte support of osteoclast activity by a RANKL-dependent pathway. PLoS ONE 2011, 6, e25900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitaura, H.; Marahleh, A.; Ohori, F.; Noguchi, T.; Shen, W.-R.; Qi, J.; Nara, Y.; Pramusita, A.; Kinjo, R.; Mizoguchi, I. Osteocyte-related cytokines regulate osteoclast formation and bone resorption. Int. J. Mol. Sci. 2020, 21, 5169. [Google Scholar] [CrossRef] [PubMed]
- Baek, K.; Hwang, H.R.; Park, H.-J.; Kwon, A.; Qadir, A.S.; Ko, S.-H.; Woo, K.M.; Ryoo, H.-M.; Kim, G.-S.; Baek, J.-H. TNF-α Upregulates sclerostin expression in obese mice fed a high-fat diet. J. Cell. Physiol. 2013, 229, 640–650. [Google Scholar] [CrossRef]
- Mödder, U.I.; Hoey, K.A.; Amin, S.; McCready, L.K.; Achenbach, S.J.; Riggs, B.L.; Melton, L.J., 3rd; Khosla, S. Relation of age, gender, and bone mass to circulating sclerostin levels in women and men. J. Bone Miner. Res. 2010, 26, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Arasu, A.; Cawthon, P.M.; Lui, L.-Y.; Do, T.P.; Arora, P.S.; Cauley, J.A.; Ensrud, K.E.; Cummings, S.R. Study of osteoporotic fractures research group. J. Clin. Endocrinol. Metab. 2012, 97, 2027–2032. [Google Scholar] [CrossRef] [Green Version]
- Urano, T.; Shiraki, M.; Ouchi, Y.; Inoue, S. Association of circulating sclerostin levels with fat mass and metabolic disease—related markers in Japanese postmenopausal women. J. Clin. Endocrinol. Metab. 2012, 97, E1473–E1477. [Google Scholar] [CrossRef] [Green Version]
- Marzullo, P.; Mele, C.; Mai, S.; Nardone, A.; Scacchi, M.; Aimaretti, G. Obesity and bone loss at menopause: The role of sclerostin. Diagnostics 2021, 11, 1914. [Google Scholar] [CrossRef]
- Kim, S.P.; Frey, J.L.; Li, Z.; Kushwaha, P.; Zoch, M.L.; Tomlinson, R.E.; Da, H.; Aja, S.; Noh, H.L.; Kim, J.K.; et al. Sclerostin influences body composition by regulating catabolic and anabolic metabolism in adipocytes. Proc. Natl. Acad. Sci. USA 2017, 114, E11238–E11247. [Google Scholar] [CrossRef] [Green Version]
- Daniele, G.; Winnier, D.; Mari, A.; Bruder, J.; Fourcaudot, M.; Pengou, Z.; Tripathy, D.; Jenkinson, C.; Folli, F. Sclerostin and insulin resistance in prediabetes: Evidence of a cross talk between bone and glucose metabolism. Diabetes Care 2015, 38, 1509–1517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Martín, A.; Rozas-Moreno, P.; Reyes-Garcia, R.; Morales-Santana, S.; Fontana, B.G.; Garcia-Salcedo, J.; Muñoz-Torres, M. Circulating levels of sclerostin are increased in patients with type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 2012, 97, 234–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, Z.; Tong, D.; Ou, Y.; Zhang, H.; Zhang, Z.; Li, S.; Zhou, J.; Zhang, J.; Liao, E. Serum sclerostin levels were positively correlated with fat mass and bone mineral density in Central South Chinese postmenopausal women. Clin. Endocrinol. 2012, 76, 797–801. [Google Scholar] [CrossRef]
- Amrein, K.; Amrein, S.; Drexler, C.; Dimai, H.P.; Dobnig, H.; Pfeifer, K.; Tomaschitz, A.; Pieber, T.R.; Fahrleitner-Pammer, A. Sclerostin and its association with physical activity, age, gender, body composition, and bone mineral content in healthy adults. J. Clin. Endocrinol. Metab. 2012, 97, 148–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Wang, Y.; Li, Y.; Tang, M.; Wan, S.; Tian, H.; Chen, X. Decreased sclerostin secretion in humans and mice with nonalcoholic fatty liver disease. Front. Endocrinol. 2021, 12, 707505. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Anastasilakis, A.D.; Kountouras, J.; Makras, P.; Papatheodorou, A.; Kokkoris, P.; Sakellariou, G.T.; Terpos, E. Circulating sclerostin and Dickkopf-1 levels in patients with nonalcoholic fatty liver disease. J. Bone Miner. Metab. 2015, 34, 447–456. [Google Scholar] [CrossRef]
- Azzam, E.; Ata, M.N.; Younan, D.N.; Salem, T.M.; Abdul-Aziz, A.A. DObesity: Relationship between vitamin D deficiency, obesity and sclerostin as a novel biomarker of bone metabolism. J. Clin. Transl. Endocrinol. 2019, 17, 100197. [Google Scholar] [CrossRef]
- Stanik, J.; Kratzsch, J.; Landgraf, K.; Vogel, M.; Thiery, J.; Kiess, W.; Körner, A. The bone markers sclerostin, osteoprotegerin, and bone-specific alkaline phosphatase are related to insulin resistance in children and adolescents, independent of their association with growth and obesity. Horm. Res. Paediatr. 2019, 91, 1–8. [Google Scholar] [CrossRef]
- Kirmani, S.; Amin, S.; McCready, L.K.; Atkinson, E.J.; Melton, L.J., 3rd; Müller, R.; Khosla, S. Sclerostin levels during growth in children. Osteoporos. Int. 2011, 23, 1123–1130. [Google Scholar] [CrossRef] [Green Version]
- Clarke, B.L.; Drake, M.T. Clinical utility of serum sclerostin measurements. BoneKEy Rep. 2013, 2, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mödder, U.I.; Clowes, J.; Hoey, K.; Peterson, J.M.; McCready, L.; Oursler, M.J.; Riggs, B.L.; Khosla, S. Regulation of circulating sclerostin levels by sex steroids in women and in men. J. Bone Miner. Res. 2010, 26, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Ardawi, M.-S.M.; Al-Kadi, H.; Rouzi, A.; Qari, M.H. Determinants of serum sclerostin in healthy pre- and postmenopausal women. J. Bone Miner. Res. 2011, 26, 2812–2822. [Google Scholar] [CrossRef] [PubMed]
- Von Maltzahn, J.; Chang, N.C.; Bentzinger, C.F.; Rudnicki, M.A. Wnt signaling in myogenesis. Trends Cell Biol. 2012, 22, 602–6099. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.; Schüler, S.C.; Hüttner, S.S.; von Eyss, B.; von Maltzahn, J. Adult stem cells at work: Regenerating skeletal muscle. Cell. Mol. Life Sci. 2019, 76, 2559–2570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pin, F.; Bonewald, L.F.; Bonetto, A. Role of myokines and osteokines in cancer cachexia. Exp. Biol. Med. 2021, 246, 2118–2127. [Google Scholar] [CrossRef]
- Hesse, E.; Schröder, S.; Brandt, D.; Pamperin, J.; Saito, H.; Taipaleenmäki, H. Sclerostin inhibition alleviates breast cancer–induced bone metastases and muscle weakness. JCI Insight 2019, 4, e125543. [Google Scholar] [CrossRef]
- Diamond, T.; Stiel, D.; Lunzer, M.; Wilkinson, M.; Posen, S. Ethanol reduces bone formation and may cause osteoporosis. Am. J. Med. 1989, 86, 282–288. [Google Scholar] [CrossRef]
- Dai, J.; Lin, D.; Zhang, J.; Habib, P.; Smith, P.; Murtha, J.; Fu, Z.; Yao, Z.; Qi, Y.; Keller, E.T. Chronic alcohol ingestion induces osteoclastogenesis and bone loss through IL-6 in mice. J. Clin. Investig. 2000, 106, 887–895. [Google Scholar] [CrossRef] [Green Version]
- Mendenhall, C.; Roselle, G.A.; Gartside, P.; Moritz, T. Relationship of protein calorie malnutrition to alcoholic liver disease: A reexamination of data from two veterans administration cooperative studies. Alcohol. Clin. Exp. Res. 1995, 19, 635–641. [Google Scholar] [CrossRef]
- Santolaria, F.; Pérez-Manzano, J.L.; Milena, A.; González-Reimers, E.; Gómez-Rodríguez, M.A.; Martínez-Riera, A.; Alemán-Valls, M.R.; de la Vega-Prieto, M.J. Nutritional assessment in alcoholic patients. Its relationship with alcoholic intake, feeding habits, organic complications and social problems. Drug Alcohol Depend. 2000, 59, 295–304. [Google Scholar] [CrossRef]
- Bjørkhaug, S.T.; Neupane, S.P.; Bramness, J.G.; Aanes, H.; Skar, V.; Medhus, A.W.; Valeur, J. Plasma cytokine levels in patients with chronic alcohol overconsumption: Relations to gut microbiota markers and clinical correlates. Alcohol 2019, 85, 35–40. [Google Scholar] [CrossRef] [PubMed]
- González-Reimers, E.; Martín-González, C.; De La Vega-Prieto, M.; González, R.P.; Fernández-Rodríguez, C.; López-Prieto, J.; Alvisa-Negrín, J.; Santolaria-Fernández, F. Serum sclerostin in alcoholics: A pilot study. Alcohol Alcohol. 2013, 48, 278–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, Y.; Kim, W.J.; Han, K.J.; Kil Lim, S.; Kim, S.H. Effect of liver dysfunction on circulating sclerostin. J. Bone Miner. Metab. 2013, 32, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Wakolbinger, R.; Muschitz, C.; Wallwitz, J.; Bodlaj, G.; Feichtinger, X.; Schanda, J.E.; Resch, H.; Baierl, A.; Pietschmann, P. Serum levels of sclerostin reflect altered bone microarchitecture in patients with hepatic cirrhosis. Wien. Klin. Wochenschr. 2020, 132, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Maurel, D.B.; Benaitreau, D.; Jaffré, C.; Toumi, H.; Portier, H.; Uzbekov, R.; Pichon, C.; Benhamou, C.L.; Lespessailles, E.; Pallu, S. Effect of the alcohol consumption on osteocyte cell processes: A molecular imaging study. J. Cell. Mol. Med. 2013, 18, 1680–1693. [Google Scholar] [CrossRef]
- Maurel, D.B.; Pallu, S.; Jaffré, C.; Fazzalari, N.L.; Boisseau, N.; Uzbekov, R.; Benhamou, C.-L.; Rochefort, G.Y. Osteocyte apoptosis and lipid infiltration as mechanisms of alcohol-induced bone loss. Alcohol Alcohol. 2012, 47, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Child, C.G.; Turcotte, J.G. Surgery and portal hypertension. Major. Probl. Clin. Urg. 1964, 1, 1–85. [Google Scholar]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Smith, R.; Aulet, M.; Bensen, B.; Lichtman, S.; Wang, J.; Pierson, R.N. Appendicular skeletal muscle mass: Measurement by dual-photon absorptiometry. Am. J. Clin. Nutr. 1990, 52, 214–218. [Google Scholar] [CrossRef]
- Wyskida, K.; Franik, G.; Owczarek, A.J.; Choręza, P.; Kocełak, P.; Madej, P.; Chudek, J.; Olszanecka-Glinianowicz, M. Plasma sclerostin levels are associated with nutritional status and insulin resistance but not hormonal disturbances in women with polycystic ovary syndrome. Arch. Gynecol. Obstet. 2020, 302, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Ukita, M.; Yamaguchi, T.; Ohata, N.; Tamura, M. Sclerostin enhances adipocyte differentiation in 3T3-L1 cells. J. Cell. Biochem. 2015, 117, 1419–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.-H.V.; Schwartz, A.V.; Sigurdsson, S.; Hue, T.F.; Lang, T.F.; Harris, T.B.; Rosen, C.J.; Vittinghoff, E.; Eiriksdottir, G.; Hauksdottir, A.M.; et al. Circulating sclerostin associated with vertebral bone marrow fat in older men but not women. J. Clin. Endocrinol. Metab. 2014, 99, E2584–E2590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.S.; Mazur, C.M.; Wein, M.N. Sclerostin and osteocalcin: Candidate bone-produced hormones. Front. Endocrinol. 2021, 12, 584147. [Google Scholar] [CrossRef]
- González-Reimers, E.; López-Prieto, J.; Pelazas-González, R.; Alemán-Valls, M.; de la Vega-Prieto, M.J.; Jorge-Ripper, C.; Durán-Castellón, M.C.; Santolaria-Fernández, F. Serum sclerostin in hepatitis C virus infected patients. J. Bone Metab. 2014, 21, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, N.R.; Diemar, S.S.; Christensen, G.L.; Kimer, N.; Danielsen, K.V.; Møller, S. patients with cirrhosis have elevated bone turnover but normal hepatic production of osteoprotegerin. J. Clin. Endocrinol. Metab. 2021, 107, e980–e995. [Google Scholar] [CrossRef]
- Drake, M.T.; Khosla, S. Hormonal and systemic regulation of sclerostin. Bone 2016, 96, 8–17. [Google Scholar] [CrossRef] [Green Version]
- Szulc, P.; Bertholon, C.; Borel, O.; Marchand, F.; Chapurlat, R. Lower fracture risk in older men with higher sclerostin concentration: A prospective analysis from the MINOS study. J. Bone Miner. Res. 2012, 28, 855–864. [Google Scholar] [CrossRef]
- Jean, G.; Chazot, C. Sclerostin in CKD-MBD: One more paradoxical bone protein? Nephrol. Dyal. Transplant. 2013, 28, 2932–2935. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.A.; Roh, E.; Hong, S.-H.; Lee, Y.-B.; Kim, N.H.; Yoo, H.J.; Seo, J.A.; Kim, N.H.; Kim, S.G.; Baik, S.H.; et al. Association of serum sclerostin levels with low skeletal muscle mass: The Korean Sarcopenic Obesity Study (KSOS). Bone 2019, 128, 115053. [Google Scholar] [CrossRef]
- Moriwaki, K.; Matsumoto, H.; Tanishima, S.; Tanimura, C.; Osaki, M.; Nagashima, H.; Hagino, H. Association of serum bone- and muscle-derived factors with age, sex, body composition, and physical function in community-dwelling middle-aged and elderly adults: A cross-sectional study. BMC Musculoskelet. Disord. 2019, 20, 276. [Google Scholar] [CrossRef] [PubMed]
- González-Reimers, E.; Romero-Acevedo, L.; Quintero-Platt, G.; Martín-González, C.; Cabrera-García, P.; Gómez-Rodríguez, M.A.; Espelosín-Ortega, E.; Santolaria-Fernández, F. Serum sclerostin and muscle strength in alcoholics. J. Musculoskelet Disord. Treat 2017, 3, 030. [Google Scholar] [CrossRef]
- Medeiros, M.C.; Rocha, N.; Bandeira, E.; Dantas, I.; Chaves, C.; Oliveira, M.; Bandeira, F. Serum sclerostin, body composition, and sarcopenia in hemodialysis patients with diabetes. Int. J. Nephrol. 2020, 2020, 4596920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novo-Rodríguez, C.; García-Fontana, B.; Castillo, J.D.D.L.-D.; Andújar-Vera, F.; Ávila-Rubio, V.; García-Fontana, C.; Morales-Santana, S.; Rozas-Moreno, P.; Muñoz-Torres, M. Circulating levels of sclerostin are associated with cardiovascular mortality. PLoS ONE 2018, 13, e0199504. [Google Scholar] [CrossRef]
- Catalano, A.; Bellone, F.; Morabito, N.; Corica, F. Sclerostin and vascular pathophysiology. Int. J. Mol. Sci. 2020, 21, 4779. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Cirrhotics (n = 54) | Non-Cirrhotics (n = 53) | T (Z); p * | Controls (n = 26) | |
|---|---|---|---|---|
| Age | 59.91 ± 10.40 | 58.09 ± 111.49 | T = 0.86; NS | 54.85 ± 7.71 |
| Daily ethanol (g) | 203 ± 110 200 (139–250) | 218 ± 180 200 (100–269) | Z = 0.18; NS | <10 g |
| Years of addiction | 32.56 ± 13.15 | 32.82 ± 13.13 | T = 0.11; NS | - |
| Mean corpuscular volume (fL) | 101.29 ± 10.55 | 101.04 ± 5.29 | T = 0.16; NS | 92.49 ± 4.31 |
| Serum GGT (U/L) | 374.67 ± 658.68 208.00 (54.00–396.50) | 229.90 ± 252.96 116.00 (59.50–345.00) | Z = 0.84; NS | 26.39 ± 10.77 |
| Prothrombin activity (%) | 66.31 ± 21.28 63.50 (50.75–83.75) | 89.79 ± 12.37 95.00 (84.00–100.00) | Z = 5.59; p < 0.001 | 97.50 ± 4.15 |
| Serum Albumin (g/dL) | 3.45 ± 0.78 | 3.75 ± 0.62 | T = 2.19: p = 0.031 | 4.56 ± 0.24 |
| Serum bilirubin (mg/dL) | 3.61 ± 4.28 2.30 (1.00–4.35) | 1.40 ± 1.88 1.00 (1.00–1.08) | Z = 5.45; p < 0.001 | 0.99 ± 0.11 |
| Serum sclerostin (pmol/L) | 41.19 ± 30.52 33.73 (16.32–59.95) | 31.48 ± 26.93 28.05 (12.90–40.30) | Z = 1.72; p = 0.086 | 29.14 ± 13.52 |
| Serum creatinine (mg/dL) | 1.02 ± 0.73 0.72 (0.62–0.95) | 0.81 ± 0.28 0.76 (0.61–0.95) | Z = 0.06; NS | 0.91 ± 0.11 |
| Serum cholesterol (mg/dL) | 124.36 ± 36.22 | 172.28 ± 49.53 | T = 5.58; p < 0.001 | 188.94 ± 40.01 |
| Serum triglycerides (mg/dL) | 92.06 ± 38.39 | 123.72 ± 59.98 | T = 3.17; p = 0.002 | 108.39 ± 46.19 |
| Serum uric acid (mg/dL) | 5.84 ± 2.54 | 5.17 ± 2.55 | T = 1.09; NS | 5.46 ± 0.76 |
| Glycated hemoglobin (%) | 5.93 ± 1.74 5.40 (4.98–6.15) | 5.46 ± 0.51 5.40 (5.08–5.63) | Z = 0.39; NS | 5.79 ± 0.64 |
| Total HIP BMD | 1.028 ± 0.163 | 1.012 ± 0.197 | T = 0.88; NS | 1.05 ± 0.14 |
| Pelvis BMD | 1.143 ± 0.122 | 1.105 ± 0.151 | T = 1.41; NS | - |
| Total BMD | 1.186 ± 0.106 | 1.186± 0.122 | T = 0.02; NS | - |
| L2-L4 BMD | 1.162 ± 0.165 | 1.143 ± 0.208 | T = 0.50; NS | 1.04 ± 0.06 |
| Total fat (g) | 22,733 ± 11,167 | 19,733 ± 9505 | T = 1.75; p = 0.084 | 21,329 ± 7059 |
| Trunk fat (g) | 13,398 ± 6155 | 11,682 ± 6252 | T = 1.71; p = 0.091 | 11,280 ± 4851 |
| Right leg fat (g) | 3334 ± 2022 | 2752 ± 1415 | T = 1.93; p = 0.057 | 3589 ± 1032 |
| Left leg fat (g) | 3295 ± 1970 | 2741 ± 1393 | T = 1.87; p = 0.064 | 3550 ± 1005 |
| Right arm fat (g) | 1054 ± 723 | 884 ± 473 | T = 1.61; NS | 1214 ± 510 |
| Left arm fat (g) | 1008 ± 652 | 938 ±486 | T = 0.82; NS | 1150 ± 472 |
| Gynoid fat (g) | 3753 ± 2045 | 3083 ± 1570 | T = 1.83; p = 0.070 | - |
| Android fat (g) | 2351 ± 1195 | 2095 ± 1176 | T = 1.07; NS | - |
| Total lean (g) | 50,513 ± 8286 | 48,753 ± 7271 | T = 1.48; NS | 54,933 ± 7100 |
| Trunk lean (g) | 26,279 ± 4839 | 24,536 ± 3612 | T = 2.29; p = 0.024 | 27,467 ± 3335 |
| Right arm lean (g) | 2661 ± 547 | 2763 ± 654 | T = 0.43; NS | 3323 ± 556 |
| Left arm lean (g) | 2657 ± 608 | 2774 ± 710 | T = 0.51; NS | 3163 ± 529 |
| Right leg lean (g) | 7639 ± 1690 | 7378 ± 1449 | T = 1.17; NS | 8661 ± 1097 |
| Left leg lean (g) | 7557 ± 1693 | 7351 ± 1374 | T = 1.00; NS | 8363 ± 1268 |
| Gynoid lean (g) | 6470 ± 1494 | 6245 ± 1670 | T = 0.71; NS | - |
| Android lean (g) | 4343 ± 1086 | 3723 ± 927 | T = 3.06; p = 0.003 | - |
| BMI (kg/m2) | 26.70 ± 4.91 | 25.95 ± 4.45 | T = 0.76; NS | 26.22 ± 2.58 |
| Handgrip strength (kg) | 15.40 ± 10.88 | 27.93 ± 46.99 | Z = 1.35; NS | 40.21 ± 9.18 |
| Serum Sclerostin | ||
|---|---|---|
| All Patients (n = 107) | Cirrhotics (n = 54) | |
| Lean mass at upper of lower limbs ASM * | ρ = −0.03; NS | ρ = −0.01; NS |
| Upper limbs ASM | ρ = −0.20; p = 0.055 | ρ = −0.23; NS |
| Lower limbs ASM | ρ = 0.01; NS | ρ = 0.04; NS |
| Handgrip strength | ρ = −0.14; NS | ρ = −0.28; p = 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martín González, C.; Fernández Rodríguez, C.M.; Abreu González, P.; García Rodríguez, A.; Alvisa Negrín, J.C.; Cabañas Perales, E.; González Navarrete, L.; Vera Delgado, V.E.; Ortega Toledo, P.; González Reimers, E. Sclerostin in Excessive Drinkers: Relationships with Liver Function and Body Composition. Nutrients 2022, 14, 2574. https://doi.org/10.3390/nu14132574
Martín González C, Fernández Rodríguez CM, Abreu González P, García Rodríguez A, Alvisa Negrín JC, Cabañas Perales E, González Navarrete L, Vera Delgado VE, Ortega Toledo P, González Reimers E. Sclerostin in Excessive Drinkers: Relationships with Liver Function and Body Composition. Nutrients. 2022; 14(13):2574. https://doi.org/10.3390/nu14132574
Chicago/Turabian StyleMartín González, Candelaria, Camino María Fernández Rodríguez, Pedro Abreu González, Alen García Rodríguez, Julio César Alvisa Negrín, Elisa Cabañas Perales, Lourdes González Navarrete, Víctor Eugenio Vera Delgado, Paula Ortega Toledo, and Emilio González Reimers. 2022. "Sclerostin in Excessive Drinkers: Relationships with Liver Function and Body Composition" Nutrients 14, no. 13: 2574. https://doi.org/10.3390/nu14132574
APA StyleMartín González, C., Fernández Rodríguez, C. M., Abreu González, P., García Rodríguez, A., Alvisa Negrín, J. C., Cabañas Perales, E., González Navarrete, L., Vera Delgado, V. E., Ortega Toledo, P., & González Reimers, E. (2022). Sclerostin in Excessive Drinkers: Relationships with Liver Function and Body Composition. Nutrients, 14(13), 2574. https://doi.org/10.3390/nu14132574