
Association among Premenstrual Syndrome, Dietary Patterns, and Adherence to Mediterranean Diet


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Diagnosis of Premenstrual Syndrome
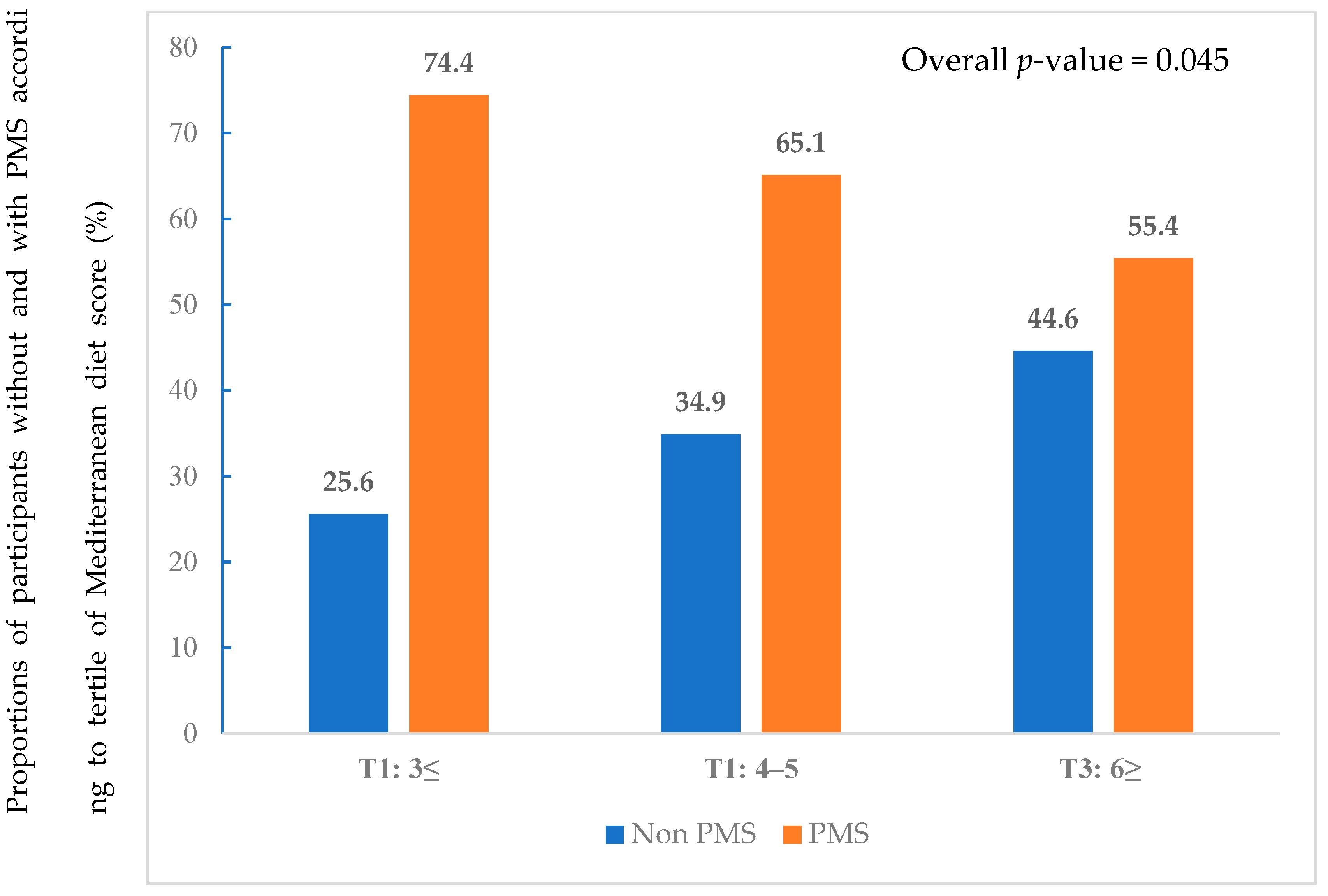
2.4. Assessment of Mediterranean Diet Adherence
2.5. Assessment of Nutritional Intake and Dietary Patterns
2.6. Statistical Analysis
3. Results
3.1. Baseline Participant Characteristics
3.2. Nutritional Status and Dietary Patterns
3.3. Association between Dietary Patterns and PMS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hofmeister, S.; Bodden, S. Premenstrual syndrome and premenstrual dysphoric disorder. Am. Fam. Physician 2016, 94, 236–240. [Google Scholar] [PubMed]
- Ryu, A.; Kim, T.H. Premenstrual syndrome: A mini review. Maturitas 2015, 82, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Halbreich, U.; Borenstein, J.; Pearlstein, T.; Kahn, L.S. The prevalence, impairment, impact, and burden of premenstrual dysphoric disorder (pms/pmdd). Psychoneuroendocrinology 2003, 28 (Suppl. 3), 1–23. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, Y.; van Heck, C.H.; Qiao, W. Stress reactivity and emotion in premenstrual syndrome. Neuropsychiatr. Dis. Treat. 2017, 13, 1597–1602. [Google Scholar] [CrossRef] [PubMed]
- MoradiFili, B.; Ghiasvand, R.; Pourmasoumi, M.; Feizi, A.; Shahdadian, F.; Shahshahan, Z. Dietary patterns are associated with premenstrual syndrome: Evidence from a case-control study. Public Health Nutr. 2020, 23, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Jahanfar, S.; Lye, M.S.; Krishnarajah, I.S. The heritability of premenstrual syndrome. Twin Res. Hum Genet. 2011, 14, 433–436. [Google Scholar] [CrossRef]
- Han, J.; Cha, Y.; Kim, S. Effect of psychosocial interventions on the severity of premenstrual syndrome: A meta-analysis. J. Psychosom. Obstet. Gynaecol. 2019, 40, 176–184. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R.; Hankinson, S.E.; Willett, W.C.; Johnson, S.R.; Manson, J.E. Adiposity and the development of premenstrual syndrome. J. Womens Health 2010, 19, 1955–1962. [Google Scholar] [CrossRef]
- Farasati, N.; Siassi, F.; Koohdani, F.; Qorbani, M.; Abashzadeh, K.; Sotoudeh, G. Western dietary pattern is related to premenstrual syndrome: A case-control study. Br. J. Nutr. 2015, 114, 2016–2021. [Google Scholar] [CrossRef]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to mediterranean diet and health status: Meta-analysis. Bmj 2008, 337, a1344. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet quality as assessed by the healthy eating index, alternate healthy eating index, dietary approaches to stop hypertension score, and health outcomes: An updated systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2018, 118, 74–100.e111. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Jobin, J.; Bouillon, J. Assessment of leisure time exercise behavior by self-report: A concurrent validity study. Can. J. Public Health 1986, 77, 359–362. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice Bulletin. Premenstrual syndrome. Clinical management guidelines for obstetrician–gynecologists. Number 15. J. Obstet. Gynecol. 2001, 73, 183–191. [Google Scholar]
- Kim, T.-H.; Park, H.S.; Lee, H.-H.; Chung, S.-H. Premenstrual syndrome and dysmenorrhea in the career women at bucheon city. Korean J. Obstet. Gynecol. 2011, 54, 523–528. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Lee, H.; Yoon, Y.; Kim, H.M.; Chu, S.H.; Lee, J.W. Development and validation of a questionnaire to measure adherence to the mediterranean diet in korean adults. Nutrients 2020, 12, 1102. [Google Scholar] [CrossRef]
- Yun, S.H.; Shim, J.-S.; Kweon, S.; Oh, K. Development of a food frequency questionnaire for the korea national health and nutrition examination survey: Data from the fourth korea national health and nutrition examination survey (knhanes iv). Korean J. Nutr. 2013, 46, 186–196. [Google Scholar] [CrossRef]
- Korea Disease Control and Prevention Agency. Korea National Health & Nutritional Examination Survey Sixth (2013–2015), Guidbook for Data User (Korean). Available online: https://knhanes.cdc.go.kr/knhanes/eng/index.do (accessed on 20 November 2017).
- Erbil, N.; Yücesoy, H. Premenstrual syndrome prevalence in turkey: A systematic review and meta-analysis. Psychol. Health Med. 2021, 8, 1–11. [Google Scholar] [CrossRef]
- Dutta, A.; Sharma, A. Prevalence of premenstrual syndrome and premenstrual dysphoric disorder in india: A systematic review and meta-analysis. Health Promot. Perspect. 2021, 11, 161–170. [Google Scholar] [CrossRef]
- Dueñas, J.L.; Lete, I.; Bermejo, R.; Arbat, A.; Pérez-Campos, E.; Martínez-Salmeán, J.; Serrano, I.; Doval, J.L.; Coll, C. Prevalence of premenstrual syndrome and premenstrual dysphoric disorder in a representative cohort of spanish women of fertile age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 156, 72–77. [Google Scholar] [CrossRef]
- Ranjbaran, M.; Omani Samani, R.; Almasi-Hashiani, A.; Matourypour, P.; Moini, A. Prevalence of premenstrual syndrome in iran: A systematic review and meta-analysis. Int. J. Reprod. Biomed. 2017, 15, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Potter, J.; Bouyer, J.; Trussell, J.; Moreau, C. Premenstrual syndrome prevalence and fluctuation over time: Results from a french population-based survey. J. Womens Health 2009, 18, 31–39. [Google Scholar] [CrossRef] [PubMed]
- PARK, Y.-H.; JEONG, B.-S.; KIM, C.-Y.; Lee, C. Prevalence of premenstrual dysphoric disorder and occupational function in a nurse group. J. Korean Neuropsychiatr. Assoc. 2001, 40, 832–841. [Google Scholar]
- Kang, S.; Lee, Y. Menstruation and the variability of food intake in female college students. Korean J. Community Nutr. 2013, 18, 577–587. [Google Scholar] [CrossRef]
- Hashim, M.S.; Obaideen, A.A.; Jahrami, H.A.; Radwan, H.; Hamad, H.J.; Owais, A.A.; Alardah, L.G.; Qiblawi, S.; Al-Yateem, N.; Faris, M.A.E. Premenstrual syndrome is associated with dietary and lifestyle behaviors among university students: A cross-sectional study from sharjah, uae. Nutrients 2019, 11, 1939. [Google Scholar] [CrossRef]
- Gantenbein, K.V.; Kanaka-Gantenbein, C. Mediterranean diet as an antioxidant: The impact on metabolic health and overall wellbeing. Nutrients 2021, 13, 1951. [Google Scholar] [CrossRef]
- Onieva-Zafra, M.D.; Fernández-Martínez, E.; Abreu-Sánchez, A.; Iglesias-López, M.T.; García-Padilla, F.M.; Pedregal-González, M.; Parra-Fernández, M.L. Relationship between diet, menstrual pain and other menstrual characteristics among spanish students. Nutrients 2020, 12, 1759. [Google Scholar] [CrossRef]
- Kraemer, M.V.; Oliveira, R.C.; Gonzalez-Chica, D.A.; Proença, R.P. Sodium content on processed foods for snacks. Public Health Nutr. 2016, 19, 967–975. [Google Scholar] [CrossRef]
- Chidambaram, N.; Sethupathy, S.; Saravanan, N.; Mori, M.; Yamori, Y.; Garg, A.K.; Chockalingam, A. Relationship of sodium and magnesium intakes to hypertension proven by 24-hour urianalysis in a south indian population. J. Clin. Hypertens. 2014, 16, 581–586. [Google Scholar] [CrossRef]
- Johnson, S. The multifaceted and widespread pathology of magnesium deficiency. Med. Hypotheses 2001, 56, 163–170. [Google Scholar] [CrossRef]
- Facchinetti, F.; Borella, P.; Sances, G.; Fioroni, L.; Nappi, R.E.; Genazzani, A.R. Oral magnesium successfully relieves premenstrual mood changes. Obstet. Gynecol. 1991, 78, 177–181. [Google Scholar] [PubMed]
- Song, Y.; Joung, H. A traditional korean dietary pattern and metabolic syndrome abnormalities. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 456–462. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, M.S.; Lee, M.S.; Park, Y.S.; Lee, H.J.; Kang, S.-a.; Lee, H.S.; Lee, K.-E.; Yang, H.J.; Kim, M.J. Korean diet: Characteristics and historical background. J. Ethn. Foods 2016, 3, 26–31. [Google Scholar] [CrossRef]
- Knüppel, A.; Shipley, M.J.; Llewellyn, C.H.; Brunner, E.J. Sugar intake from sweet food and beverages, common mental disorder and depression: Prospective findings from the whitehall ii study. Sci. Rep. 2017, 7, 6287. [Google Scholar] [CrossRef]
- Dye, L.; Blundell, J.E. Menstrual cycle and appetite control: Implications for weight regulation. Hum. Reprod. 1997, 12, 1142–1151. [Google Scholar] [CrossRef]
- Khayyatzadeh, S.S.; Bagherniya, M.; Fazeli, M.; Khorasanchi, Z.; Bidokhti, M.S.; Ahmadinejad, M.; Khoshmohabbat, S.; Arabpour, M.; Afkhamizadeh, M.; Ferns, G.A.; et al. A western dietary pattern is associated with elevated level of high sensitive c-reactive protein among adolescent girls. Eur. J. Clin. Investig. 2018, 48, e12897. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R.; Ronnenberg, A.G.; Houghton, S.C.; Nobles, C.; Zagarins, S.E.; Takashima-Uebelhoer, B.B.; Faraj, J.L.; Whitcomb, B.W. Association of inflammation markers with menstrual symptom severity and premenstrual syndrome in young women. Hum. Reprod. 2014, 29, 1987–1994. [Google Scholar] [CrossRef]
- Duvan, C.I.; Cumaoglu, A.; Turhan, N.O.; Karasu, C.; Kafali, H. Oxidant/antioxidant status in premenstrual syndrome. Arch. Gynecol. Obstet. 2011, 283, 299–304. [Google Scholar] [CrossRef]
- Resnicow, K.; Odom, E.; Wang, T.; Dudley, W.N.; Mitchell, D.; Vaughan, R.; Jackson, A.; Baranowski, T. Validation of three food frequency questionnaires and 24-hour recalls with serum carotenoid levels in a sample of african-american adults. Am. J. Epidemiol. 2000, 152, 1072–1080. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Non-PMS Group | PMS Group | p-Value |
|---|---|---|---|
| N | 91 (34.7%) | 171 (65.3%) | |
| Age (years) | 33.0 (26.0–37.0) | 31.0 (26.0–37.0) | 0.213 |
| BMI (kg/m2) | 21.1 (19.6–23.1) | 20.5 (19.1–22.9) | 0.460 |
| Education, N (%) | |||
| Undergraduate | 26 (28.6%) | 46 (26.9%) | 0.773 |
| Graduate | 65 (71.4%) | 125 (73.1%) | |
| Marital status, N (%) | |||
| Single | 63 (69.2%) | 123 (71.9%) | 0.647 |
| Married | 28 (30.8%) | 48 (28.1%) | |
| Smoking status, N (%) | |||
| Never smoker | 78 (85.7%) | 126 (73.7%) | 0.046 |
| Former smoker | 8 (8.8%) | 19 (11.1%) | |
| Current smoker | 5 (5.5%) | 26 (15.2%) | |
| Alcohol drinking status, N (%) | |||
| Never drinker | 31 (34.1%) | 23 (13.5%) | <0.001 |
| Current drinker | 60 (65.9%) | 148 (86.5%) | |
| Physical activity, N (%) | |||
| Active | 22 (24.2%) | 55 (32.2%) | 0.389 |
| Moderately active | 28 (30.8%) | 45 (26.3%) | |
| Insufficiently active/sedentary | 41 (45.1%) | 71 (41.5%) | |
| Underlying conditions, N (%) | |||
| Hypertension | 3 (3.3%) | 1 (0.6%) | 0.122 |
| Diabetes mellitus | 0 (0.0%) | 3 (1.8%) | 0.554 |
| Characteristics | Non-PMS Group | PMS Group | p-Value |
|---|---|---|---|
| Age of Menarche (years) | 14.0 (13.0–15.0) | 13.0 (12.0–13.0) | 0.227 |
| Menstrual Length (days) | 28.0 (28.0–30.0) | 29.0 (28.0–30.0) | 0.275 |
| Duration of flow (days) | 5.0 (5.0–7.0) | 6.0 (5.0–6.0) | 0.771 |
| Menstrual regularity, N (%) | |||
| Regular | 61 (67.0%) | 124 (72.5%) | 0.354 |
| Irregular | 30 (33.0%) | 47 (27.5%) | |
| Amount of flow, N (%) | |||
| Mild | 10 (11.0%) | 18 (10.5%) | 0.993 |
| Moderate | 72 (79.1%) | 136 (79.5%) | |
| Heavy | 9 (9.9%) | 17 (9.9%) | |
| Dysmenorrhea, N (%) | |||
| Present | 73 (80.2%) | 163 (95.3%) | <0.001 |
| None | 18 (19.3%) | 8 (4.7%) |
| Variables | Non-PMS Group | PMS Group | p-Value |
|---|---|---|---|
| N | 91 | 171 | |
| Total calorie | 1667.6 ± 931.2 | 1950.6 ± 1121.5 | 0.041 |
| Carbohydrate (g/day) | 255.7 ± 128.3 | 295.7 ± 168.8 | 0.049 |
| Protein (g/day) | 45.9 ± 4.8 | 43.5 ± 3.3 | 0.112 |
| Fat (g/day) | 45.5 ± 34.3 | 55.1 ± 39.2 | 0.050 |
| Fiber (g/day) | 10.7 ± 1.1 | 13.3 ± 1.0 | 0.036 |
| Saturated fatty acids (%) | 1.93 ± 0.2 | 1.90 ± 2.0 | 0.584 |
| Polyunsaturated fatty acids (%) | 5.36 ± 2.90 | 5.35 ± 1.95 | 0.961 |
| Monounsaturated fatty acids | 5.34 ± 1.90 | 5.50 ± 2.20 | 0.539 |
| Omega-3 fatty acids | 0.30 ± 0.31 | 0.29 ± 0.20 | 0.692 |
| Omega-6 fatty acids | 0.01 ± 0.02 | 0.01 ± 0.01 | 0.783 |
| Omega-6/Omega-3 | 0.08 ± 0.19 | 0.06 ± 0.11 | 0.268 |
| Vitamin A | 298.6 ± 236.4 | 386.2 ± 304.2 | 0.011 |
| Vitamin C | 93.4 ± 83.5 | 115.2 ± 121.1 | 0.088 |
| Vitamin D | 3.2 ± 5.0 | 4.2 ± 11.5 | 0.473 |
| Vitamin E | 13.4 ± 10.7 | 15.9 ± 11.5 | 0.098 |
| Vitamin K | 116.1 ± 121.0 | 166.2 ± 177.9 | 0.008 |
| Riboflavin | 1.3 ± 0.9 | 1.5 ± 1.0 | 0.250 |
| Niacin | 9.8 ± 7.3 | 11.5 ± 7.2 | 0.075 |
| Vitamin B6 | 1.7 ± 3.8 | 1.5 ± 1.0 | 0.660 |
| Ca | 375.2 ± 280.0 | 460.3 ± 307.9 | 0.029 |
| Na | 2327.4 ± 2287.3 | 2783.7 ± 2068.3 | 0.103 |
| K | 2216.4 ± 1547.6 | 2584.9 ± 1665.6 | 0.082 |
| Zinc | 8.6 ± 7.7 | 9.7 ± 5.8 | 0.222 |
| Variables | Non-PMS Group | PMS Group | p-Value |
|---|---|---|---|
| N | 91 | 171 | |
| Rice | 2.31 ± 1.67 | 2.43 ± 1.73 | 0.598 |
| Mixed grain rice | 5.19 ± 5.88 | 5.04 ± 5.67 | 0.84 |
| Noodles/dumplings | 0.50 ± 0.49 | 0.58 ± 0.58 | 0.27 |
| Breads/rice cakes | 0.42 ± 0.48 | 0.51 ± 0.49 | 0.166 |
| Soup/stew | 0.36 ± 0.56 | 0.40 ± 0.41 | 0.492 |
| Soybeans | 0.67 ± 0.98 | 0.75 ± 1.08 | 0.56 |
| Eggs | 1.91 ± 1.89 | 1.90 ± 1.74 | 0.953 |
| Red meat | 0.48 ± 0.66 | 0.47 ± 0.44 | 0.833 |
| White meat | 0.23 ± 0.17 | 0.32 ± 0.46 | 0.024 |
| Fish/seafood | 0.38 ± 0.68 | 0.37 ± 0.61 | 0.957 |
| Vegetables | 0.59 ± 0.70 | 0.64 ± 0.74 | 0.623 |
| Fermented foods | 0.83 ± 1.65 | 0.96 ± 1.37 | 0.53 |
| Kimchi | 2.64 ± 3.00 | 2.92 ± 3.22 | 0.492 |
| Seaweed | 0.69 ± 1.37 | 0.66 ± 1.16 | 0.876 |
| Potatoes | 0.34 ± 0.64 | 0.35 ± 0.66 | 0.986 |
| Milk/dairy products | 1.37 ± 1.55 | 1.72 ± 1.97 | 0.11 |
| Fruits | 0.51 ± 0.53 | 0.57 ± 0.60 | 0.401 |
| Beverages | 1.80 ± 1.65 | 2.03 ± 1.72 | 0.289 |
| Snacks | 1.05 ± 1.49 | 1.52 ± 2.07 | 0.033 |
| Nuts | 0.19 ± 0.51 | 0.34 ± 1.35 | 0.171 |
| Alcoholic beverages | 0.25 ± 0.45 | 0.44 ± 0.86 | 0.022 |
| Traditional Diet Pattern | Meat and Alcohol Pattern | Bread and Snack Pattern | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Model 1 | ||||||
| T1 | 1.00 (Ref) | 1.00 (Ref) | 1.00 (Ref) | |||
| T2 | 1.07 | 0.831 | 1.75 | 0.076 | 1.91 | 0.039 |
| (0.57–2.00) | (0.94–3.26) | (1.03–3.53) | ||||
| T3 | 0.91 | 0.905 | 1.82 | 0.060 | 2.63 | 0.003 |
| (0.49–1.68) | (0.97–3.40) | (1.39–5.00) | ||||
| Model 2 | ||||||
| T1 | 1.00 (Ref) | 1.00 (Ref) | 1.00 (Ref) | |||
| T2 | 1.11 | 0.751 | 1.80 | 0.068 | 1.87 | 0.048 |
| (0.59–2.09) | (0.96–3.36) | (1.01–3.48) | ||||
| T3 | 1.03 | 0.927 | 1.86 | 0.053 | 2.61 | 0.003 |
| (0.54–1.98) | (0.99–3.49) | (1.37–4.97) | ||||
| Model 3 | ||||||
| T1 | 1.00 (Ref) | 1.00 (Ref) | 1.00 (Ref) | |||
| T2 | 1.17 | 0.635 | 1.53 | 0.205 | 1.88 | 0.056 |
| (0.61–2.29) | (0.79–2.95) | (0.98–3.58) | ||||
| T3 | 1.13 | 0.735 | 1.60 | 0.160 | 2.59 | 0.006 |
| (0.56–2.30) | (0.83–2.09) | (1.32–5.06) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.-J.; Sung, D.-I.; Lee, J.-W. Association among Premenstrual Syndrome, Dietary Patterns, and Adherence to Mediterranean Diet. Nutrients 2022, 14, 2460. https://doi.org/10.3390/nu14122460
Kwon Y-J, Sung D-I, Lee J-W. Association among Premenstrual Syndrome, Dietary Patterns, and Adherence to Mediterranean Diet. Nutrients. 2022; 14(12):2460. https://doi.org/10.3390/nu14122460
Chicago/Turabian StyleKwon, Yu-Jin, Da-In Sung, and Ji-Won Lee. 2022. "Association among Premenstrual Syndrome, Dietary Patterns, and Adherence to Mediterranean Diet" Nutrients 14, no. 12: 2460. https://doi.org/10.3390/nu14122460
APA StyleKwon, Y.-J., Sung, D.-I., & Lee, J.-W. (2022). Association among Premenstrual Syndrome, Dietary Patterns, and Adherence to Mediterranean Diet. Nutrients, 14(12), 2460. https://doi.org/10.3390/nu14122460