
Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
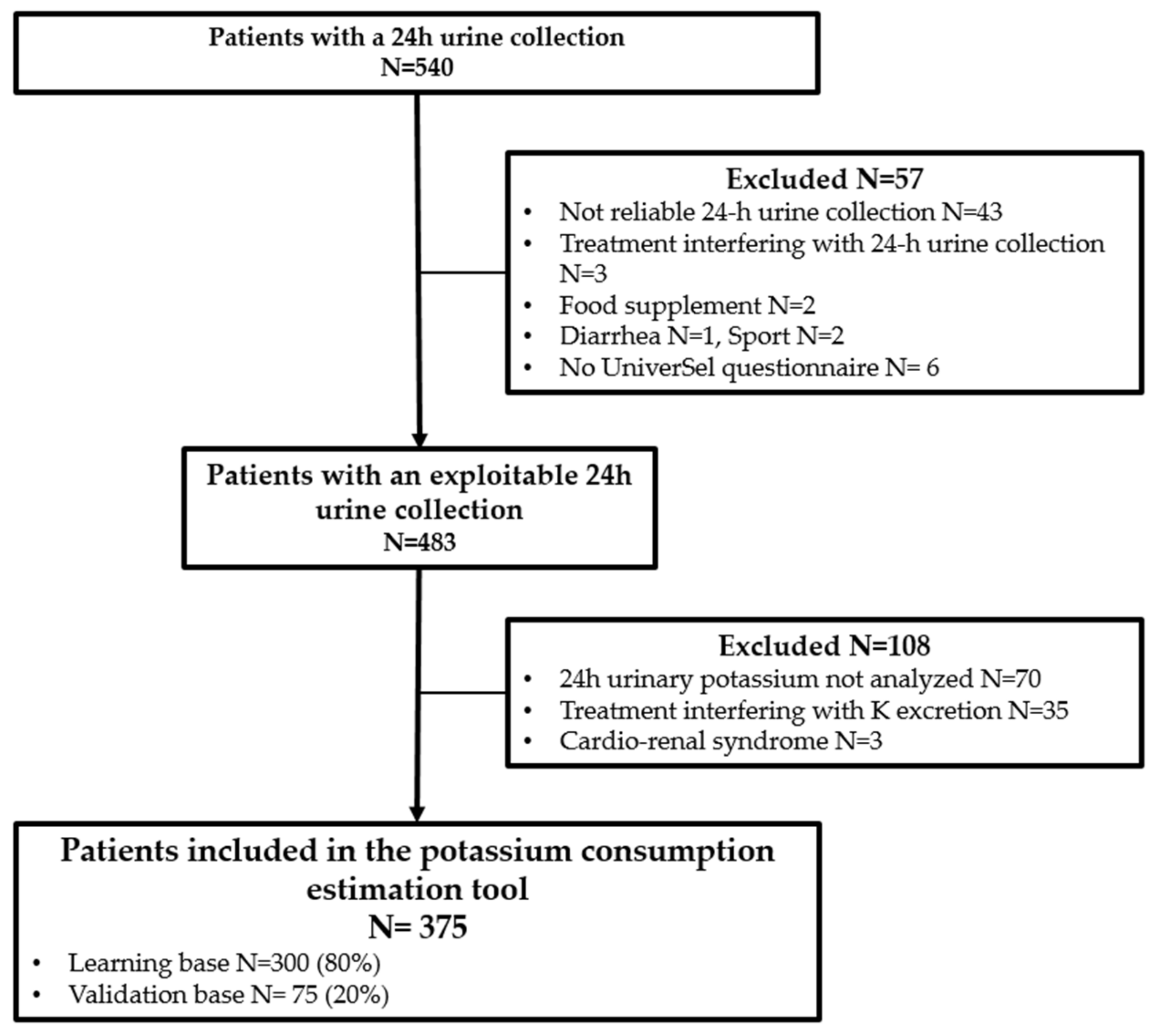
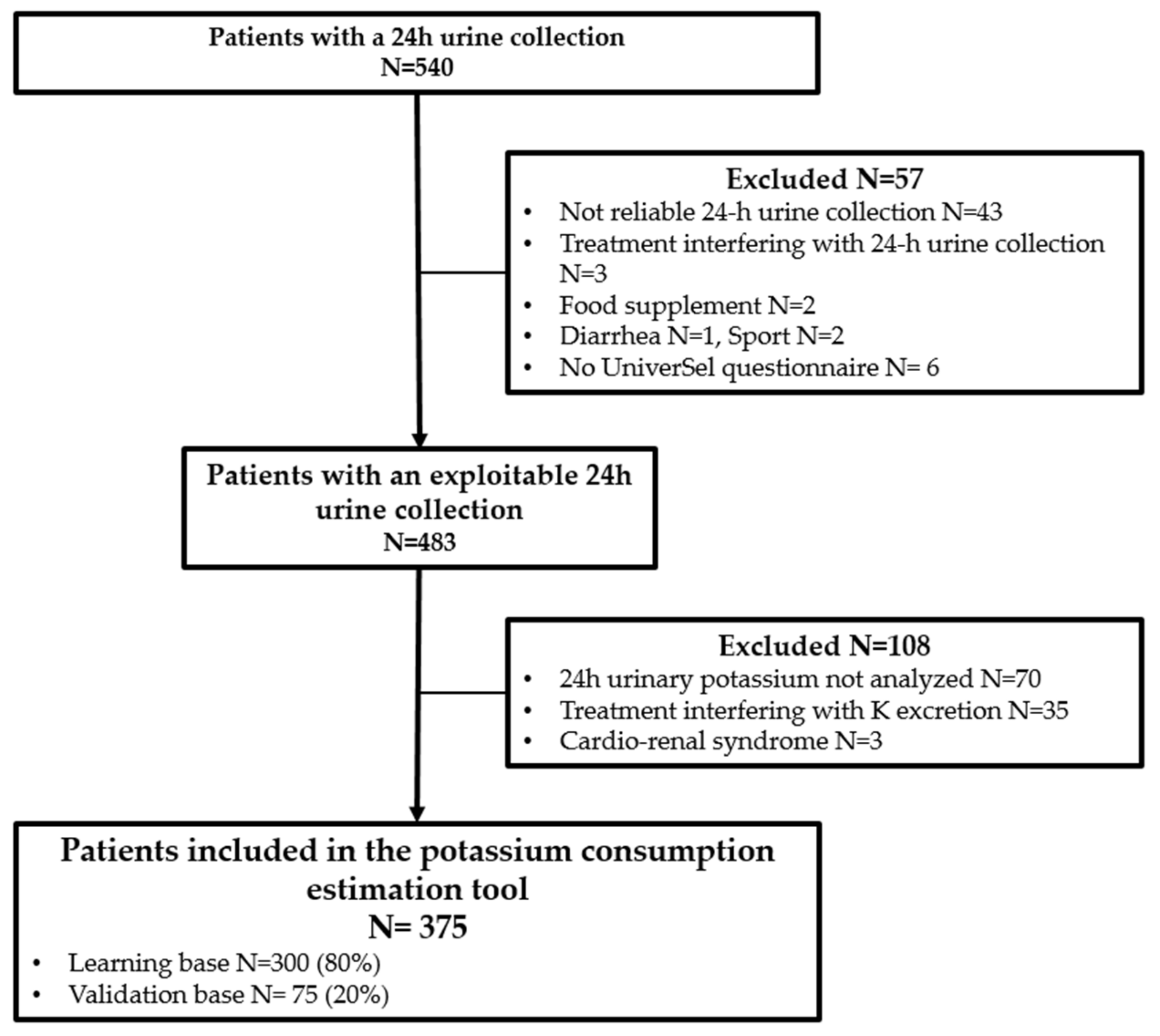
2.1. Patients and Data Pre-Processing
2.2. “UniverSel” Self-Questionnaire
2.3. Baseline Variables
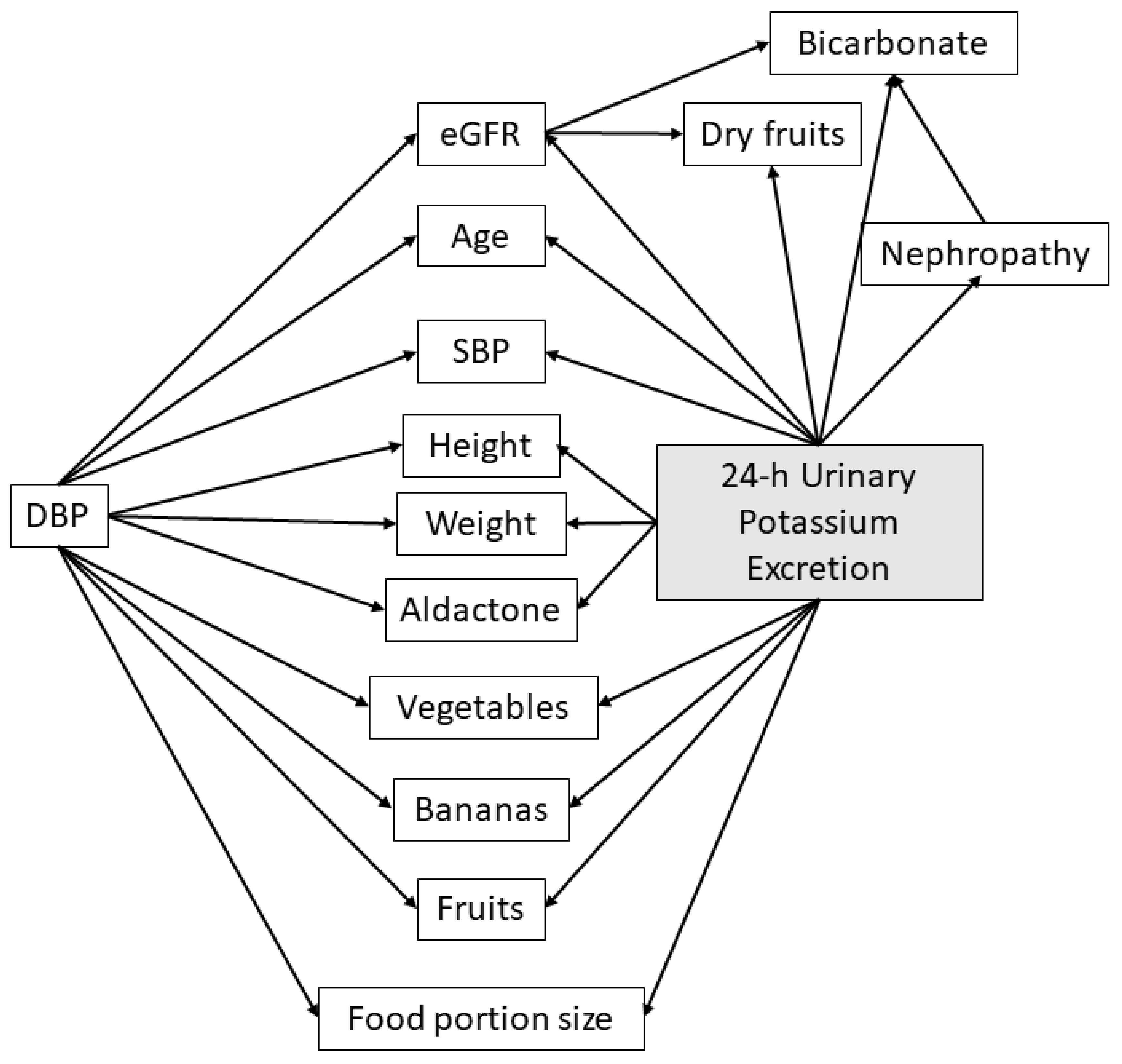
2.4. Development and Optimization of the Prediction Tool
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Variables Selected for the Development of the Clinical Prediction Tool and Internal Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of Increased Potassium Intake on Cardiovascular Risk Factors and Disease: Systematic Review and Meta-Analyses. BMJ 2013, 346, f1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mente, A.; O’Donnell, M.J.; Rangarajan, S.; McQueen, M.J.; Poirier, P.; Wielgosz, A.; Morrison, H.; Li, W.; Wang, X.; Di, C.; et al. Association of Urinary Sodium and Potassium Excretion with Blood Pressure. N. Engl. J. Med. 2014, 371, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Huang, X.; Liu, X.; Wang, L.; Chen, Z.; Ortega, D.; Chen, L.; Sun, J.; Hatsukami, T.S.; Yuan, C.; et al. Urinary Sodium and Potassium Excretion and Cerebrovascular Health: A Multimodal Imaging Study. Eur. J. Nutr. 2021, 60, 4555–4563. [Google Scholar] [CrossRef] [PubMed]
- Judge, C.; O’Donnell, M.J.; Hankey, G.J.; Rangarajan, S.; Chin, S.L.; Rao-Melacini, P.; Ferguson, J.; Smyth, A.; Xavier, D.; Lisheng, L.; et al. Urinary Sodium and Potassium, and Risk of Ischemic and Hemorrhagic Stroke (INTERSTROKE): A Case–Control Study. Am. J. Hypertens. 2021, 34, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily Potassium Intake and Sodium-to-Potassium Ratio in the Reduction of Blood Pressure: A Meta-Analysis of Randomized Controlled Trials. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef]
- Olde Engberink, R.H.G.; van den Born, B.-J.H.; Peters-Sengers, H.; Vogt, L. Long-Term Potassium Intake and Associated Renal and Cardiovascular Outcomes in the Clinical Setting. Clin. Nutr. 2020, 39, 3671–3676. [Google Scholar] [CrossRef]
- Davitte, J.; Laughlin, G.A.; Kritz-Silverstein, D.; McEvoy, L.K. Dietary Potassium Intake and 20-Year All-Cause Mortality in Older Adults: The Rancho Bernardo Study. J. Nutr. Gerontol. Geriatr. 2021, 40, 46–57. [Google Scholar] [CrossRef]
- Chang, H.-C.; Wu, C.-L.; Lee, Y.-H.; Gu, Y.-H.; Chen, Y.-T.; Tsai, Y.-W.; Chuang, S.-Y.; Guo, C.-Y.; Chen, C.-H.; Cheng, H.-M. Impact of Dietary Intake of Sodium and Potassium on Short-Term Blood Pressure Variability. J. Hypertens. 2021, 39, 1835–1843. [Google Scholar] [CrossRef]
- Allison, S.J. Urinary Sodium and Potassium Excretion: Association with Blood Pressure and Clinical Outcomes. Nat. Rev. Nephrol. 2014, 10, 541. [Google Scholar] [CrossRef]
- Filippini, T.; Naska, A.; Kasdagli, M.; Torres, D.; Lopes, C.; Carvalho, C.; Moreira, P.; Malavolti, M.; Orsini, N.; Whelton, P.K.; et al. Potassium Intake and Blood Pressure: A Dose-Response Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2020, 9, e015719. [Google Scholar] [CrossRef]
- Vinceti, M.; Filippini, T.; Crippa, A.; de Sesmaisons, A.; Wise, L.A.; Orsini, N. Meta-Analysis of Potassium Intake and the Risk of Stroke. J. Am. Heart Assoc. 2016, 5, e004210. [Google Scholar] [CrossRef] [PubMed]
- Palaka, E.; Grandy, S.; Darlington, O.; McEwan, P.; Doornewaard, A. Associations between Serum Potassium and Adverse Clinical Outcomes: A Systematic Literature Review. Int. J. Clin. Pract. 2020, 74, e13421. [Google Scholar] [CrossRef] [PubMed]
- Clase, C.M.; Carrero, J.-J.; Ellison, D.H.; Grams, M.E.; Hemmelgarn, B.R.; Jardine, M.J.; Kovesdy, C.P.; Kline, G.A.; Lindner, G.; Obrador, G.T.; et al. Potassium Homeostasis and Management of Dyskalemia in Kidney Diseases: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2020, 97, 42–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fauvel, J.-P.; Gueyffier, F.; Thijs, L.; Ducher, M. Combined Effect of Renal Function and Serum Potassium Level in Sudden Cardiac Death in Aging Hypertensive Subjects. Hypertens. Res. 2018, 41, 469–474. [Google Scholar] [CrossRef]
- Xi, L.; Hao, Y.-C.; Liu, J.; Wang, W.; Wang, M.; Li, G.-Q.; Qi, Y.; Zhao, F.; Xie, W.-X.; Li, Y.; et al. Associations between Serum Potassium and Sodium Levels and Risk of Hypertension: A Community-Based Cohort Study. J. Geriatr. Cardiol. 2015, 12, 119–126. [Google Scholar] [CrossRef]
- Organisation Mondiale de la Santé Directives: Sur L’apport En Potassium Chez L’adulte et Chez L’enfant. Available online: https://apps.who.int/iris/bitstream/handle/10665/85225/WHO_NMH_NHD_13.1_fre.pdf (accessed on 9 June 2022).
- KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease—Volume 3. Issue 1. Available online: https://www.kidney-international.org/ (accessed on 9 June 2022).
- Ikizler, T.A.; Jerrilynn, D.B.; Laura, D.B.; Katrina, L.C.; Carrero, J.-J.; Chan, W.; Fouque, D.; Allon, N.F.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. Kdoqi Kdoqi Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76 (Suppl. 1), S1–S107. [Google Scholar] [CrossRef]
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and Stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Polonia, J.; Martins, L.; Pinto, F.; Nazare, J. Estimation of 24-Hour Sodium, Potassium and Albumin Excretion from Spot Urine Samples in a National Representative Survey of Hypertension (PHYSA). J. Am. Soc. Hypertens. 2014, 8, e83. [Google Scholar] [CrossRef]
- Jędrusik, P.; Symonides, B.; Gaciong, Z. Estimating 24-Hour Urinary Sodium, Potassium, and Creatinine Excretion in Hypertensive Patients: Can We Replace 24-Hour Urine Collection with Spot Urine Measurements? Pol. Arch. Intern. Med. 2019, 129, 505–516. [Google Scholar] [CrossRef] [Green Version]
- Molina, M.d.C.B.; Pereira, T.S.S.; Porto, A.S.; Silva, R.P.; Santana, N.M.T.; Cade, N.V.; Mill, J.G. Validation of Single Measurement of 12-Hour Urine Excretion for Estimation of Sodium and Potassium Intake. A Longitudinal Study. Sao Paulo Med. J. 2018, 136, 150–156. [Google Scholar] [CrossRef] [Green Version]
- Ginos, B.N.R.; Engberink, R.H.G.O. Estimation of Sodium and Potassium Intake: Current Limitations and Future Perspectives. Nutrients 2020, 12, 3275. [Google Scholar] [CrossRef] [PubMed]
- Kusuma, J.D.; Yang, H.-L.; Yang, Y.-L.; Chen, Z.-F.; Shiao, S.-Y.P.K. Validating Accuracy of a Mobile Application against Food Frequency Questionnaire on Key Nutrients with Modern Diets for MHealth Era. Nutrients 2022, 14, 537. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.N.; de Moura Souza, A.; Pereira, R.A.; Sichieri, R. Contribution of Foods Consumed Away from Home to Energy Intake in Brazilian Urban Areas: The 2008–9 Nationwide Dietary Survey. Br. J. Nutr. 2013, 109, 1276–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, K.; Mullan, J.; Mansfield, K. An Integrative Review of the Methodology and Findings Regarding Dietary Adherence in End Stage Kidney Disease. BMC Nephrol. 2017, 18, 318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkpatrick, S.I.; Raffoul, A.; Lee, K.M.; Jones, A.C. Top Dietary Sources of Energy, Sodium, Sugars, and Saturated Fats among Canadians: Insights from the 2015 Canadian Community Health Survey. Appl. Physiol. Nutr. Metab. 2019, 44, 650–658. [Google Scholar] [CrossRef]
- Ducher, M.; Mounier-Véhier, C.; Lantelme, P.; Vaisse, B.; Baguet, J.-P.; Fauvel, J.-P. Reliability of a Bayesian Network to Predict an Elevated Aldosterone-to-Renin Ratio. Arch. Cardiovasc. Dis. 2015, 108, 293–299. [Google Scholar] [CrossRef]
- Ducher, M.; Kalbacher, E.; Combarnous, F.; Finaz de Vilaine, J.; McGregor, B.; Fouque, D.; Fauvel, J.P. Comparison of a Bayesian Network with a Logistic Regression Model to Forecast IgA Nephropathy. Biomed. Res. Int. 2013, 2013, 686150. [Google Scholar] [CrossRef] [Green Version]
- Siga, M.M.; Ducher, M.; Florens, N.; Roth, H.; Mahloul, N.; Fouque, D.; Fauvel, J.-P. Prediction of All-Cause Mortality in Haemodialysis Patients Using a Bayesian Network. Nephrol. Dial. Transplant. 2020, 35, 1420–1425. [Google Scholar] [CrossRef]
- Sansot, C.; Kalbacher, E.; Lemoine, S.; Bourguignon, L.; Fauvel, J.-P.; Ducher, M. A Bayesian Model to Describe Factors Influencing Trough Levels of Vancomycin in Hemodialysis Patients. Nephron 2015, 131, 131–137. [Google Scholar] [CrossRef]
- Robard, M.C.; Coquillaud, B. Evaluation de la Consommation de sel en Pratique Médicale: Mise au Point d’un Auto-Questionnaire; S.C.D. de l’Université de Limoges: Limoges, France, 2011. [Google Scholar]
- Jallet, C. Evaluation de la Consommation de sel en Pratique Médicale: Validation d’un Auto-Questionnaire. Ph.D. Thesis, Universite de Limoges, Limoges, France, 2012. [Google Scholar]
- UniverSel-Potassium Questionnaire. Available online: https://webquest.fr/?m=118423_universel---potassium-questionnaire (accessed on 9 June 2022).
- Levey, A.S.; Inker, L.A.; Coresh, J. GFR Estimation: From Physiology to Public Health. Am. J. Kidney Dis. 2014, 63, 820–834. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604. [Google Scholar] [CrossRef] [PubMed]
- BiostTGV. Available online: https://biostatgv.sentiweb.fr/? (accessed on 9 June 2022).
- Agence de la Biomédecine Rapport 2019 du Registre REIN. Available online: https://www.agence-biomedecine.fr/IMG/pdf/rapport_rein_2019_2021-10-14.pdf (accessed on 9 June 2022).

{kind=link}
{kind=link}
| 24-h Potassium Urinary Excretion | Mean | SD | Distribution (%) |
| Less than 50 mmol/day | 38.6 | 8.8 | 34.93 |
| 50 to 69.9 mmol/day | 58.8 | 5.6 | 32.53 |
| More than 70 mmol/day | 89.5 | 18.5 | 32.53 |
| Patient characteristics | Mean | SD | Distribution (%) |
| Gender | |||
| M | 66.9 | ||
| F | 33.1 | ||
| Age (years) | 64 | 15 | |
| Weight (kg) | 78.8 | 15.9 | |
| Height (m) | 1.68 | 0.09 | |
| Nephropathy | |||
| Hypertension | 32.0 | ||
| Diabetes | 18.7 | ||
| Tubulo interstitial | 16.8 | ||
| Glomerular | 12.5 | ||
| Autosomal Dominant Polycystic | 5.3 | ||
| Other | 14.7 | ||
| CKD stage | |||
| I (≥90 mL/min/1.73 m²) | 8.8 | ||
| II (60–89 mL/min/1.73 m²) | 26.1 | ||
| IIIa (45–59 mL/min/1.73 m²) | 22.9 | ||
| IIIb (30–44 mL/min/1.73 m²) | 24.5 | ||
| IV (15–29 mL/min/1.73 m²) | 15.2 | ||
| V (<15 mL/min/1.73 m²) | 2.4 | ||
| SBP (mmHg) | 133.5 | 16.4 | |
| DBP (mmHg) | 75.1 | 11.7 | |
| Number of antihypertensive drugs | |||
| 0 | 16 | ||
| 1 | 22.1 | ||
| 2 | 26.1 | ||
| 3 or more | 35.7 | ||
| Diuretics (Yes) | 37.3 | ||
| Oedema (Yes) | 8.7 | ||
| Diabetes (Yes) | 26.7 | ||
| Heart failure | 9.1 | ||
| Ethnic origin | |||
| African | 10.4 | ||
| Caucasian | 87.7 | ||
| Asian | 1.9 | ||
| Month of inclusion | |||
| January | 8 | ||
| February | 7.5 | ||
| March | 12.3 | ||
| April | 3.5 | ||
| May | 10.9 | ||
| June | 18.4 | ||
| July | 9.3 | ||
| August | 3.7 | ||
| September | 7.7 | ||
| October | 6.4 | ||
| November | 8 | ||
| December | 4.3 | ||
| Biology | Mean | SD | |
| eGFR (ml/min/1.73 m²) | 52.4 | 23.9 | |
| Kalemia (mmol/L) | 4.4 | 0.5 | |
| Bicarbonates (mmol/L) | 25.5 | 2.9 | |
| Creatinemia (µmol/L) | 140.5 | 69.9 | |
| 24-h diuresis (L/day) | 1.9 | 0.6 | |
| 24-h kaliuresis (mmol/day) | 61.7 | 24.3 | |
| 24-h creatinuria (mmol/day) | 12.0 | 4.3 |
| Variables | Percentage Variance of Beliefs | |
|---|---|---|
| Variables included in the optimized Bayesian network | ||
| 1 | Weight | 4.91 |
| 2 | Height | 4.66 |
| 3 | Age | 4.02 |
| 4 | Food portion size | 3.18 |
| 5 | eGFR | 2.8 |
| 6 | Nephropathy | 2.39 |
| 7 | Fruits | 1.9 |
| 8 | Spironolactone | 1.37 |
| 9 | Diastolic blood pressure | 1.37 |
| 10 | Vegetables | 0.94 |
| 11 | Bicarbonate | 0.74 |
| 12 | Systolic blood pressure | 0.74 |
| 13 | Dry Fruits | 0.74 |
| 14 | Bananas | 0.64 |
| Variables not included in the optimized Bayesian network | ||
| 15 | Gender | 0.49 |
| 16 | Oedema | 0.49 |
| 17 | Mushrooms | 0.43 |
| 18 | Kalemia | 0.32 |
| 19 | Heart Failure | 0.31 |
| 20 | Nephrotic syndrome | 0.27 |
| 21 | Chocolate | 0.25 |
| 22 | Thiazides | 0.23 |
| 23 | Furosemide | 0.22 |
| 24 | Renin angiotensine sytem blockers | 0.15 |
| 25 | Dry vegetables | 0.07 |
| Estimated 24-h Kaliuresis | ||||
|---|---|---|---|---|
| Less Than 50 mmol/day | From 50 to 69.9 mmol/day | More Than 70 mmol/day | ||
| Observed 24-h Kaliuresis | Less than 50 mmol/day | 85 (70%) | 20 | 17 |
| From 50 to 69.9 mmol/day | 17 | 96 (73%) | 18 | |
| More than 70 mmol/day | 16 | 10 | 96 (79%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granal, M.; Slimani, L.; Florens, N.; Sens, F.; Pelletier, C.; Pszczolinski, R.; Casiez, C.; Kalbacher, E.; Jolivot, A.; Dubourg, L.; et al. Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study. Nutrients 2022, 14, 2419. https://doi.org/10.3390/nu14122419
Granal M, Slimani L, Florens N, Sens F, Pelletier C, Pszczolinski R, Casiez C, Kalbacher E, Jolivot A, Dubourg L, et al. Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study. Nutrients. 2022; 14(12):2419. https://doi.org/10.3390/nu14122419
Chicago/Turabian StyleGranal, Maelys, Lydia Slimani, Nans Florens, Florence Sens, Caroline Pelletier, Romain Pszczolinski, Catherine Casiez, Emilie Kalbacher, Anne Jolivot, Laurence Dubourg, and et al. 2022. "Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study" Nutrients 14, no. 12: 2419. https://doi.org/10.3390/nu14122419
APA StyleGranal, M., Slimani, L., Florens, N., Sens, F., Pelletier, C., Pszczolinski, R., Casiez, C., Kalbacher, E., Jolivot, A., Dubourg, L., Lemoine, S., Pasian, C., Ducher, M., & Fauvel, J. P. (2022). Prediction Tool to Estimate Potassium Diet in Chronic Kidney Disease Patients Developed Using a Machine Learning Tool: The UniverSel Study. Nutrients, 14(12), 2419. https://doi.org/10.3390/nu14122419