
Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size
2.2. Screening and Recruitment
2.3. Intervention/Treatment
2.4. Data Collection
2.5. Blood Sampling and Processing
2.6. Plasma Preparation
2.7. Biochemical Analysis
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. General Characteristics
3.3. Changes in Plasma Concentrations of Inflammatory and Anti-Inflammatory Biomarkers during the Study Period
3.3.1. Changes in Plasma Concentrations of IL6 and CRP
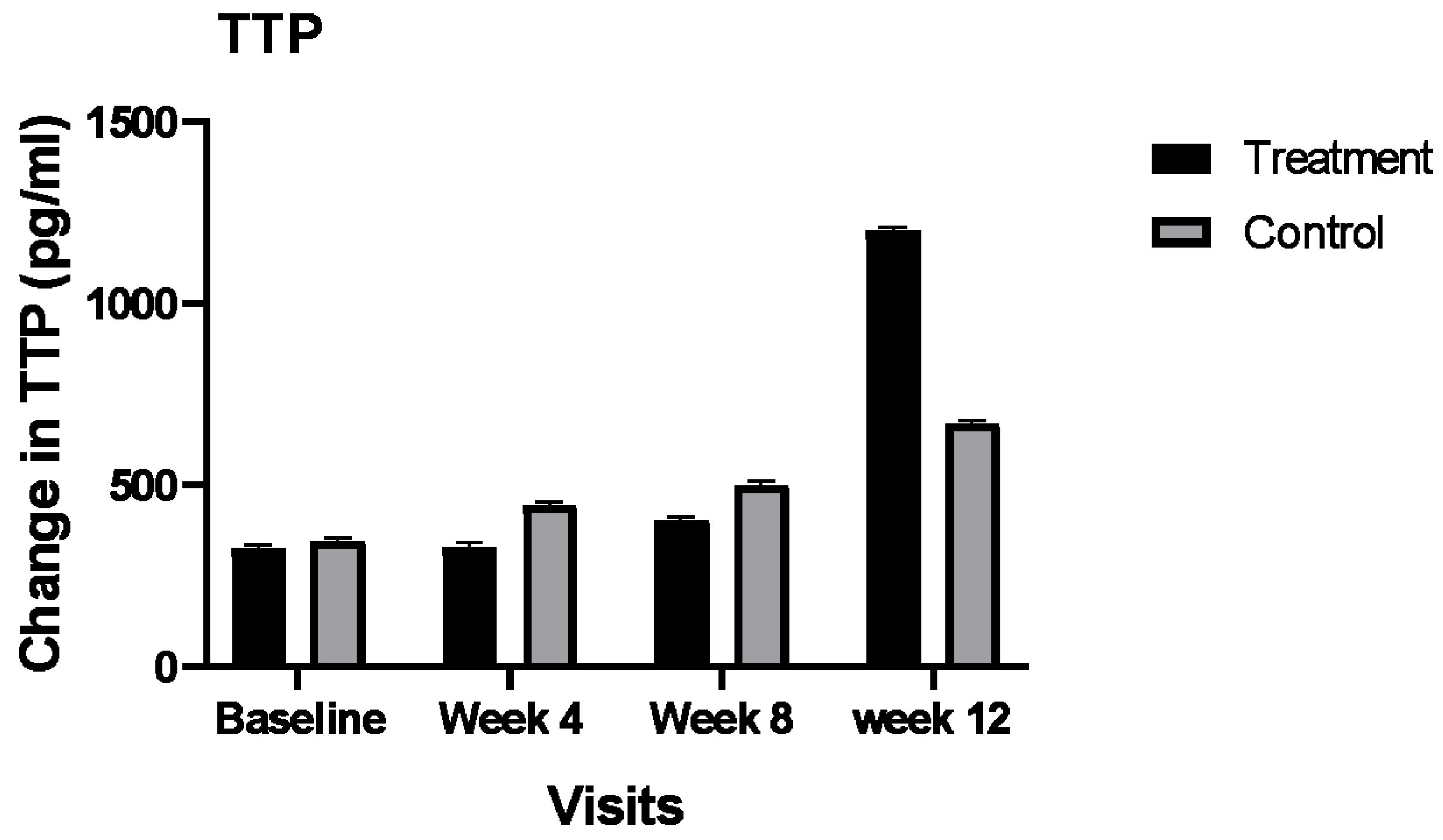
3.3.2. Changes in Plasma Concentrations of IL10 and TTP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singh, G.; Chawla, S. Amputation in Diabetic Patients. Med. J. Armed Forces India 2006, 62, 36–39. [Google Scholar] [CrossRef]
- Association for the Advancement of Wound Care (AAWC). How to Heal a Wound and Find a Wound Clinic. 2016. Available online: http://aawconline.org/ (accessed on 29 November 2016).
- Calder, P.C.; Albers, R.; Antoine, J.-M.; Blum, S.; Bourdet-Sicard, R.; Ferns, G.A.; Folkerts, G.; Friedmann, P.S.; Frost, G.S.; Guarner, F.; et al. Inflammatory Disease Processes and Interactions with Nutrition. Br. J. Nutr. 2009, 101, S1–S45. [Google Scholar] [CrossRef] [PubMed]
- Brem, H.; Tomic-Canic, M. Cellular and Molecular Basis of Wound Healing in Diabetes. J. Clin. Investig. 2007, 117, 1219–1222. [Google Scholar] [CrossRef] [PubMed]
- Blakytny, R.; Jude, E.B. Altered Molecular Mechanisms of Diabetic Foot Ulcers. Int. J. Low. Extrem. Wounds 2009, 8, 95–104. [Google Scholar] [CrossRef]
- Poljsak, B.; Šuput, D.; Milisav, I. Achieving the Balance between ROS and Antioxidants: When to Use the Synthetic Antioxidants. Oxidative Med. Cell. Longev. 2013, 2013, e956792. [Google Scholar] [CrossRef]
- Svineng, G.; Ravuri, C.; Rikardsen, O.; Huseby, N.-E.; Winberg, J.-O. The Role of Reactive Oxygen Species in Integrin and Matrix Metalloproteinase Expression and Function. Connect. Tissue Res. 2008, 49, 197–202. [Google Scholar] [CrossRef]
- Falanga, V. Wound Healing and Its Impairment in the Diabetic Foot. Lancet 2005, 366, 1736–1743. [Google Scholar] [CrossRef]
- Patel, V.; Chivukula, I.V.; Roy, S.; Khanna, S.; He, G.; Ojha, N.; Mehrotra, A.; Dias, L.M.; Hunt, T.K.; Sen, C.K. Oxygen: From the Benefits of Inducing VEGF Expression to Managing the Risk of Hyperbaric Stress. Antioxid. Redox Signal. 2005, 7, 1377–1387. [Google Scholar] [CrossRef]
- Morey, M.; O’Gaora, P.; Pandit, A.; Hélary, C. Hyperglycemia Acts in Synergy with Hypoxia to Maintain the Pro-Inflammatory Phenotype of Macrophages. PLoS ONE 2019, 14, e0220577. [Google Scholar] [CrossRef]
- Teena, R.; Dhamodharan, U.; Ali, D.; Rajesh, K.; Ramkumar, K.M. Gene Expression Profiling of Multiple Histone Deacetylases (HDAC) and Its Correlation with NRF2-Mediated Redox Regulation in the Pathogenesis of Diabetic Foot Ulcers. Biomolecules 2020, 10, 1466. [Google Scholar] [CrossRef]
- Buscemi, S.; Batsis, J.A.; Parrinello, G.; Massenti, F.M.; Rosafio, G.; Sciascia, V.; Costa, F.; Pollina Addario, S.; Mendola, S.; Barile, A.M.; et al. Nutritional Predictors of Mortality after Discharge in Elderly Patients on a Medical Ward. Eur. J. Clin. Investig. 2016, 46, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, P.; Koçak, H.; Onbaşı, K.; Biçici, P.; Özmen, A.; Uyar, C.; Özatağ, D.M. The Role of Serum Procalcitonin, Interleukin-6, and Fibrinogen Levels in Differential Diagnosis of Diabetic Foot Ulcer Infection. J. Diabetes Res. 2018, 2018, 7104352. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.G.; Luckett-Chastain, L.R.; Calhoun, K.N.; Frempah, B.; Bastian, A.; Gallucci, R.M. Interleukin 6 Function in the Skin and Isolated Keratinocytes Is Modulated by Hyperglycemia. J. Immunol. Res. 2019, 2019, e5087847. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, C.; Rose, B.; Poschen, U.; Ziegler, D.; Friese, G.; Kempf, K.; Koenig, W.; Martin, S.; Herder, C. Immune Mediators in Patients With Acute Diabetic Foot Syndrome. Diabetes Care 2009, 32, 1491–1496. [Google Scholar] [CrossRef] [PubMed]
- Oyibo, S.O.; Jude, E.B.; Tarawneh, I.; Nguyen, H.C.; Harkless, L.B.; Boulton, A.J.M. A Comparison of Two Diabetic Foot Ulcer Classification Systems: The Wagner and the University of Texas Wound Classification Systems. Diabetes Care 2001, 24, 84–88. [Google Scholar] [CrossRef]
- Galkowska, H.; Wojewodzka, U.; Olszewski, W.L. Chemokines, Cytokines, and Growth Factors in Keratinocytes and Dermal Endothelial Cells in the Margin of Chronic Diabetic Foot Ulcers. Wound Repair Regen. 2006, 14, 558–565. [Google Scholar] [CrossRef]
- Kaur, P.; Choudhury, D. Modulation of Inflammatory Dynamics by Insulin to Promote Wound Recovery of Diabetic Ulcers. In Wound Healing; IntechOpen: London, UK, 2020. [Google Scholar] [CrossRef]
- Azevedo, F.F.; Carvalho, C.R.O.; Saad, M.J.A.; Lima, M.H.M.; Da Silva Cunha Breder, J. Insulin Topical Modulates Inflammatory Phase and the Angiogenesis of the Burns Wound Healing in Diabetic-Induced Rats. Diabetol. Metab. Syndr. 2015, 7, A259. [Google Scholar] [CrossRef]
- DeClue, C.E.; Shornick, L.P. The Cytokine Milieu of Diabetic Wounds. Diabetes Manag. 2015, 5, 525–537. [Google Scholar] [CrossRef]
- Barbosa, E.; Faintuch, J.; Machado Moreira, E.A.; Gonçalves da Silva, V.R.; Lopes Pereima, M.J.; Martins Fagundes, R.L.; Filho, D.W. Supplementation of Vitamin E, Vitamin C, and Zinc Attenuates Oxidative Stress in Burned Children: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. J. Burn Care Res. 2009, 30, 859–866. [Google Scholar] [CrossRef]
- Salgado, R.M.; Cruz-Castañeda, O.; Elizondo-Vázquez, F.; Pat, L.; De la Garza, A.; Cano-Colín, S.; Baena-Ocampo, L.; Krötzsch, E. Maltodextrin/Ascorbic Acid Stimulates Wound Closure by Increasing Collagen Turnover and TGF-Β1 Expression in Vitro and Changing the Stage of Inflammation from Chronic to Acute in Vivo. J. Tissue Viability 2017, 26, 131–137. [Google Scholar] [CrossRef]
- Gross, R.L. The Effect of Ascorbate on Wound Healing. Int. Ophthalmol. Clin. 2000, 40, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Musalmah, M.; Fairuz, A.H.; Gapor, M.T.; Wan Ngah, W.Z. Effect of Vitamin E on Plasma Malondialdehyde, Antioxidant Enzyme Levels and the Rates of Wound Closures during Wound Healing in Normal and Diabetic Rats. Asia Pac. J. Clin. Nutr. 2002, 11, S448–S451. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, E.M. Neural Regulation of Innate Immunity: A Coordinated Nonspecific Host Response to Pathogens. Nat. Rev. Immunol. 2006, 6, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Holley, A.K.; Bakthavatchalu, V.; Velez-Roman, J.M.; St Clair, D.K. Manganese Superoxide Dismutase: Guardian of the Powerhouse. Int. J. Mol. Sci. 2011, 12, 7114–7162. [Google Scholar] [CrossRef]
- Aschner, J.L.; Aschner, M. Nutritional Aspects of Manganese Homeostasis. Mol. Asp. Med. 2005, 26, 353–362. [Google Scholar] [CrossRef]
- Das, A.; Chen, G.-F.; Kim, H.W.; Youn, S.-W.; Varadarajan, S.; McKinney, R.D.; Finney, L.; Ushio-Fukai, M.; Fukai, T. Abstract 16637: Antioxidant-1, a Novel Cu-Dependent Transcription Factor for NADPH Oxidase P47phox, Promotes Wound Healing by Regulating Inflammation and Angiogenesis. Circulation 2014, 130, A16637. [Google Scholar] [CrossRef]
- Basiri, R.; Spicer, M.T.; Levenson, C.W.; Ormsbee, M.J.; Ledermann, T.; Arjmandi, B.H. Nutritional Supplementation Concurrent with Nutrition Education Accelerates the Wound Healing Process in Patients with Diabetic Foot Ulcers. Available online: https://pubmed.ncbi.nlm.nih.gov/32756299/ (accessed on 1 November 2020).
- Maier, H.M.; Ilich-Ernst, J.; Arjmandi, B.; Kim, J.-S.; Spicer, M. Deficiencies in Nutritional Intake in Patients with Diabetic Foot Ulcers. J. Nutr. Ther. 2016, 5, 85–92. [Google Scholar] [CrossRef]
- Nguyen, T.P.L.; Edwards, H.; Do, T.N.D.; Finlayson, K. Effectiveness of a Theory-Based Foot Care Education Program (3STEPFUN) in Improving Foot Self-Care Behaviours and Foot Risk Factors for Ulceration in People with Type 2 Diabetes. Diabetes Res. Clin. Pract. 2019, 152, 29–38. [Google Scholar] [CrossRef]
- Defeudis, G.; Khazrai, Y.M.; Di Rosa, C.; Secchi, C.; Montedoro, A.; Maurizi, A.R.; Palermo, A.; Pozzilli, P.; Manfrini, S. Conversation MapsTM, an Effective Tool for the Management of Males and Females with Type 2 Diabetes and Mildly Impaired Glycemic Control. Hormones 2018, 17, 113–117. [Google Scholar] [CrossRef]
- Cohen, J. A Power Primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Plasma and Serum Preparation-US. Available online: https://www.thermofisher.com/us/en/home/references/protocols/cell-and-tissue-analysis/elisa-protocol/elisa-sample-preparation-protocols/plasma-and-serum-preparation.html (accessed on 18 September 2019).
- Kratochvill, F.; Gratz, N.; Qualls, J.E.; Van De Velde, L.-A.; Chi, H.; Kovarik, P.; Murray, P.J. Tristetraprolin Limits Inflammatory Cytokine Production in Tumor-Associated Macrophages in an MRNA Decay Independent Manner. Cancer Res. 2015, 75, 3054–3064. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Guo, J.; Zhang, Q.; Liu, D.; Wen, L.; Yang, Y.; Yang, L.; Liu, Z. The Expression of Tristetraprolin and Its Relationship with Urinary Proteins in Patients with Diabetic Nephropathy. PLoS ONE 2015, 10, e0141471. [Google Scholar] [CrossRef] [PubMed]
- Patial, S.; Curtis, A.D.; Lai, W.S.; Stumpo, D.J.; Hill, G.D.; Flake, G.P.; Mannie, M.D.; Blackshear, P.J. Enhanced Stability of Tristetraprolin MRNA Protects Mice against Immune-Mediated Inflammatory Pathologies. Proc. Natl. Acad. Sci. USA 2016, 113, 1865–1870. [Google Scholar] [CrossRef] [PubMed]
- Ross, E.A.; Smallie, T.; Ding, Q.; O’Neil, J.D.; Cunliffe, H.E.; Tang, T.; Rosner, D.R.; Klevernic, I.; Morrice, N.A.; Monaco, C.; et al. Dominant Suppression of Inflammation via Targeted Mutation of the MRNA Destabilizing Protein Tristetraprolin. J. Immunol. 2015, 195, 265–276. [Google Scholar] [CrossRef]
- Liang, J.; Lei, T.; Song, Y.; Yanes, N.; Qi, Y.; Fu, M. RNA-Destabilizing Factor Tristetraprolin Negatively Regulates NF-ΚB Signaling. J. Biol. Chem. 2009, 284, 29383–29390. [Google Scholar] [CrossRef]
- Afzali, H.; Jafari Kashi, A.H.; Momen-Heravi, M.; Razzaghi, R.; Amirani, E.; Bahmani, F.; Gilasi, H.R.; Asemi, Z. The Effects of Magnesium and Vitamin E Co-Supplementation on Wound Healing and Metabolic Status in Patients with Diabetic Foot Ulcer: A Randomized, Double-Blind, Placebo-Controlled Trial. Wound Repair Regen. 2019, 27, 277–284. [Google Scholar] [CrossRef]
- Tatti, P.; Barber, A.E. The Use of a Specialized Nutritional Supplement for Diabetic Foot Ulcers Reduces the Use of Antibiotics. J. Endocrinol. Metab. 2012, 2, 26–31. [Google Scholar] [CrossRef]
- Nettleton, J.A.; Steffen, L.M.; Mayer-Davis, E.J.; Jenny, N.S.; Jiang, R.; Herrington, D.M.; Jacobs, D.R. Dietary Patterns Are Associated with Biochemical Markers of Inflammation and Endothelial Activation in the Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Clin. Nutr. 2006, 83, 1369–1379. [Google Scholar] [CrossRef]
- Anderson, A.L.; Harris, T.B.; Tylavsky, F.A.; Perry, S.E.; Houston, D.K.; Lee, J.S.; Kanaya, A.M.; Sahyoun, N.R. Dietary Patterns, Insulin Sensitivity and Inflammation in Older Adults. Eur. J. Clin. Nutr. 2012, 66, 18–24. [Google Scholar] [CrossRef]
- Julia, C.; Meunier, N.; Touvier, M.; Ahluwalia, N.; Sapin, V.; Papet, I.; Cano, N.; Hercberg, S.; Galan, P.; Kesse-Guyot, E. Dietary Patterns and Risk of Elevated C-Reactive Protein Concentrations 12 Years Later. Br. J. Nutr. 2013, 110, 747–754. [Google Scholar] [CrossRef]
- Ahluwalia, N.; Andreeva, V.A.; Kesse-Guyot, E.; Hercberg, S. Dietary Patterns, Inflammation and the Metabolic Syndrome. Diabetes Metab. 2013, 39, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Maier, H.M. Nutritional Status and the Relationship of Dietary and Serum Advanced Glycation End-Products with Inflammation, Oxidative Stress and Healing of Diabetic Foot Ulcers. Ph.D. Thesis, The Florida State University, Tallahassee, FA, USA, 2016. [Google Scholar]
- Vouillarmet, J.; Maucort-Boulch, D.; Michon, P.; Thivolet, C. Advanced Glycation End Products Assessed by Skin Autofluorescence: A New Marker of Diabetic Foot Ulceration. Diabetes Technol. 2013, 15, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Maurizi, A.R.; Menduni, M.; Del Toro, R.; Kyanvash, S.; Maggi, D.; Guglielmi, C.; Pantano, A.L.; Defeudis, G.; Fioriti, E.; Manfrini, S.; et al. A Pilot Study of D-Chiro-Inositol plus Folic Acid in Overweight Patients with Type 1 Diabetes. Acta Diabetol. 2017, 54, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Baldassarre, M.P.A.; Di Tomo, P.; Centorame, G.; Pandolfi, A.; Di Pietro, N.; Consoli, A.; Formoso, G. Myoinositol Reduces Inflammation and Oxidative Stress in Human Endothelial Cells Exposed In Vivo to Chronic Hyperglycemia. Nutrients 2021, 13, 2210. [Google Scholar] [CrossRef] [PubMed]
- Basiri, R.; Spicer, M.; Munoz, J.; Arjmandi, B. Nutritional Intervention Improves the Dietary Intake of Essential Micronutrients in Patients with Diabetic Foot Ulcers. Curr. Dev. Nutr. 2020, 4, 8. [Google Scholar] [CrossRef]
- Wheeler, M.L.; Dunbar, S.A.; Jaacks, L.M.; Karmally, W.; Mayer-Davis, E.J.; Wylie-Rosett, J.; Yancy, W.S. Macronutrients, Food Groups, and Eating Patterns in the Management of Diabetes: A Systematic Review of the Literature, 2010. Diabetes Care 2012, 35, 434–445. [Google Scholar] [CrossRef]
- Collins, R.; Burrows, T.; Donnelly, H.; Tehan, P.E. Macronutrient and Micronutrient Intake of Individuals with Diabetic Foot Ulceration: A Short Report. J. Hum. Nutr. Diet. 2021. epub ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Nutrient | RDA for Nutrient | Total from Two Supplements/Day | % of RDA Provided; Men vs. Women if RDA Varied |
|---|---|---|---|
| Vitamin C | 60 | 204 | 304% |
| Vitamin A | 3000 IU | 2500 IU | 83% |
| Vitamin E | 33.3 IU | 66 IU | 200% |
| * Manganese Men/Women | 2.3/1.8 mg | 0.8 mg | 35%/44% |
| Copper | 0.9 mg | 0.8 mg | 88% |
| Zinc Men/Women | 11/8 mg | 6 mg | 54%/75% |
| Protein Men/Women | 56 g/46 g | 28 g | 50%/61% |
| Groups | Treatment (n = 15) | Control (n = 14) | p-Value |
|---|---|---|---|
| Men/women | 8/7 | 11/3 | 0.08 |
| Age (year) Means ± SD | 52.9 ± 9.74 | 53.8 ± 12.8 | 0.84 |
| Ethnicity African American/white | 4/11 | 3/11 | 0.75 |
| BMI 1 (kg/m2) Means ± SD | 33.5 ± 7.98 | 34.1 ± 6.04 | 0.84 |
| Diabetes Duration (year) Means ± SD | 14.40 ± 8.03 | 11.7 ± 6.17 | 0.32 |
| Estimated wound age (m) Means ± SD | 10.97 ± 15.09 | 10.58 ± 18.27 | 0.95 |
| HbA1c 2 Means ± SD | 7.95 ± 2.06 | 8.40 ± 2.16 | 0.57 |
| Smoking (yes/no) | 3/12 | 3/11 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basiri, R.; Spicer, M.; Levenson, C.; Ledermann, T.; Akhavan, N.; Arjmandi, B. Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers. Nutrients 2022, 14, 2393. https://doi.org/10.3390/nu14122393
Basiri R, Spicer M, Levenson C, Ledermann T, Akhavan N, Arjmandi B. Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers. Nutrients. 2022; 14(12):2393. https://doi.org/10.3390/nu14122393
Chicago/Turabian StyleBasiri, Raedeh, Maria Spicer, Cathy Levenson, Thomas Ledermann, Neda Akhavan, and Bahram Arjmandi. 2022. "Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers" Nutrients 14, no. 12: 2393. https://doi.org/10.3390/nu14122393
APA StyleBasiri, R., Spicer, M., Levenson, C., Ledermann, T., Akhavan, N., & Arjmandi, B. (2022). Improving Dietary Intake of Essential Nutrients Can Ameliorate Inflammation in Patients with Diabetic Foot Ulcers. Nutrients, 14(12), 2393. https://doi.org/10.3390/nu14122393