
Sarcopenia and Mortality in Older Hemodialysis Patients
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Primary Variables
- Clinical suspicion/case finding: Defined by the SARC-F Survey Score. SARC-F (Strength, Assistance walking, Rise from a chair, Climb stairs, and Falls) [24].
- Confirmation: muscle mass. Defined by appendicular skeletal muscle mass (ASM), measured by bioimpedance (BIA). A MALTRON® brand BioScantouch i8 BIA was used. The assessments were performed in the second session of the week between the first and second hour of HD, given that the device allows intrahaemodialytic measurements.
- Severity: physical condition. The severity of sarcopenia was defined by any of the following three variables: (1) gait speed (GS), measured as time needed to walk 4 m expressed in meters per second [27]; (2) the Timed-Up and Go test (TUG) [28]; (3) the Short Physical Performance Battery (SPPB) [29].

{kind=link}
{kind=link}
| Diagnostic Stages | Test | Males | Female |
|---|---|---|---|
| Finding | SARC-F [24] | ≥4 points | ≥4 points |
| Evaluation | Upper limbs: GSD [30] | <27 kg | <16 kg |
| Lower limbs: STS5 [31] | >15 s | >15 s | |
| Confirmation | AMS [32] | <20 kg | <15 kg |
| Severity | GS [32,33] | ≤0.8 m/s | ≤0.8 m/s |
| TUG [34] | ≥20 s | ≥20 s | |
| SPPB [35,36] | ≤8 points | ≤8 points |
2.2. Other Variables
2.3. Statistics
3. Results
3.1. Participants
3.2. Prevalence of Sarcopenia According to EWGSOP2
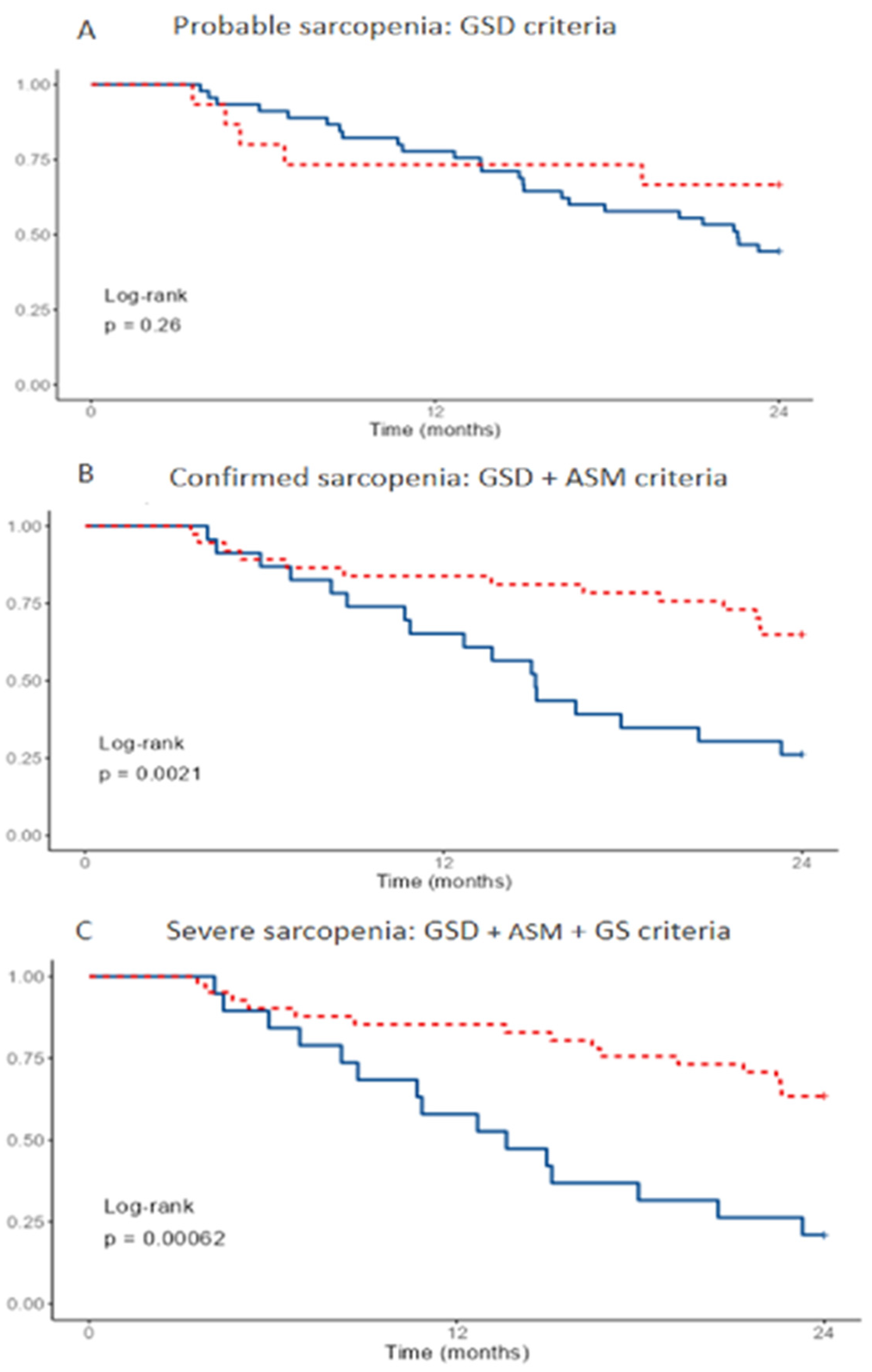
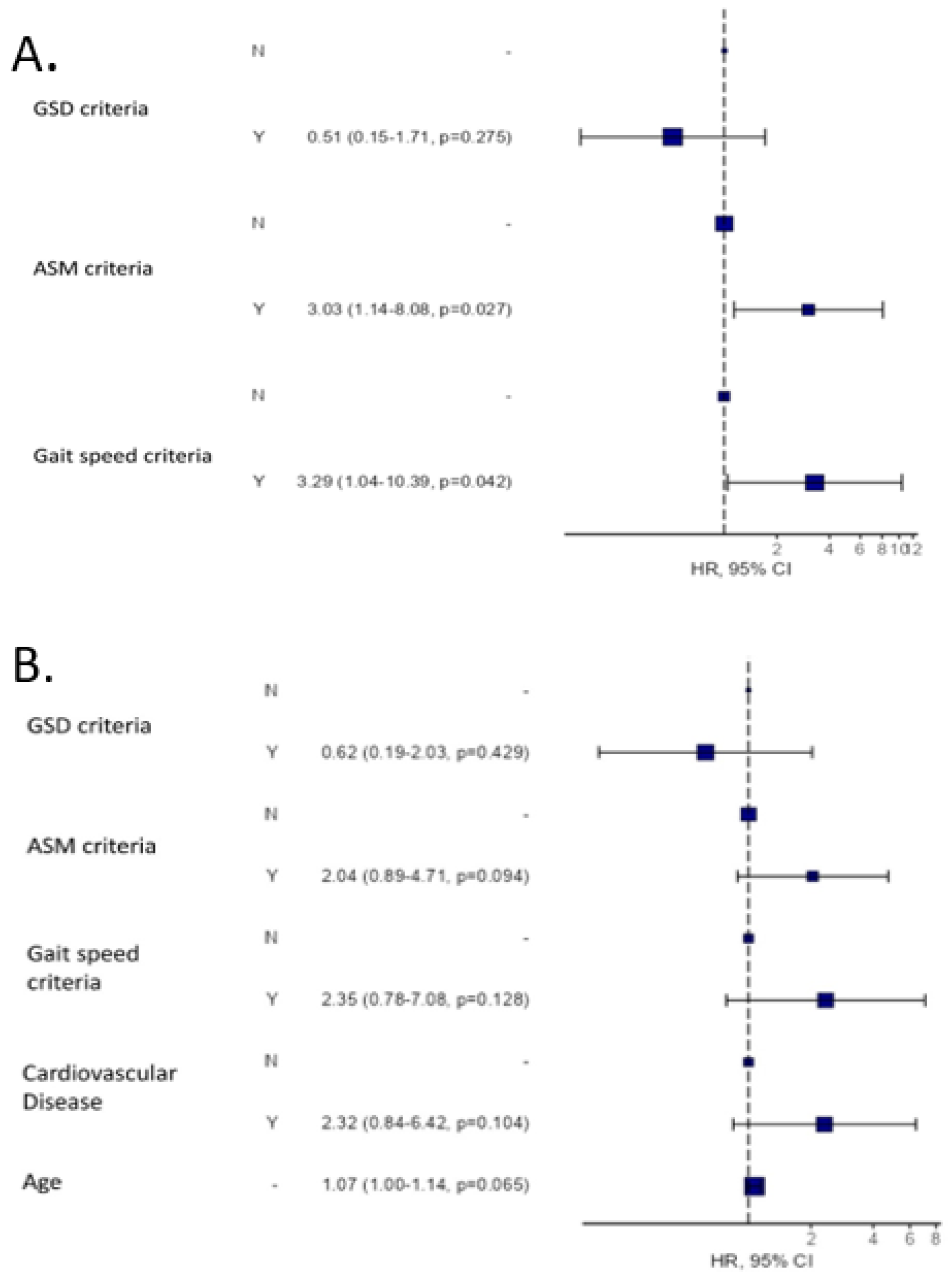
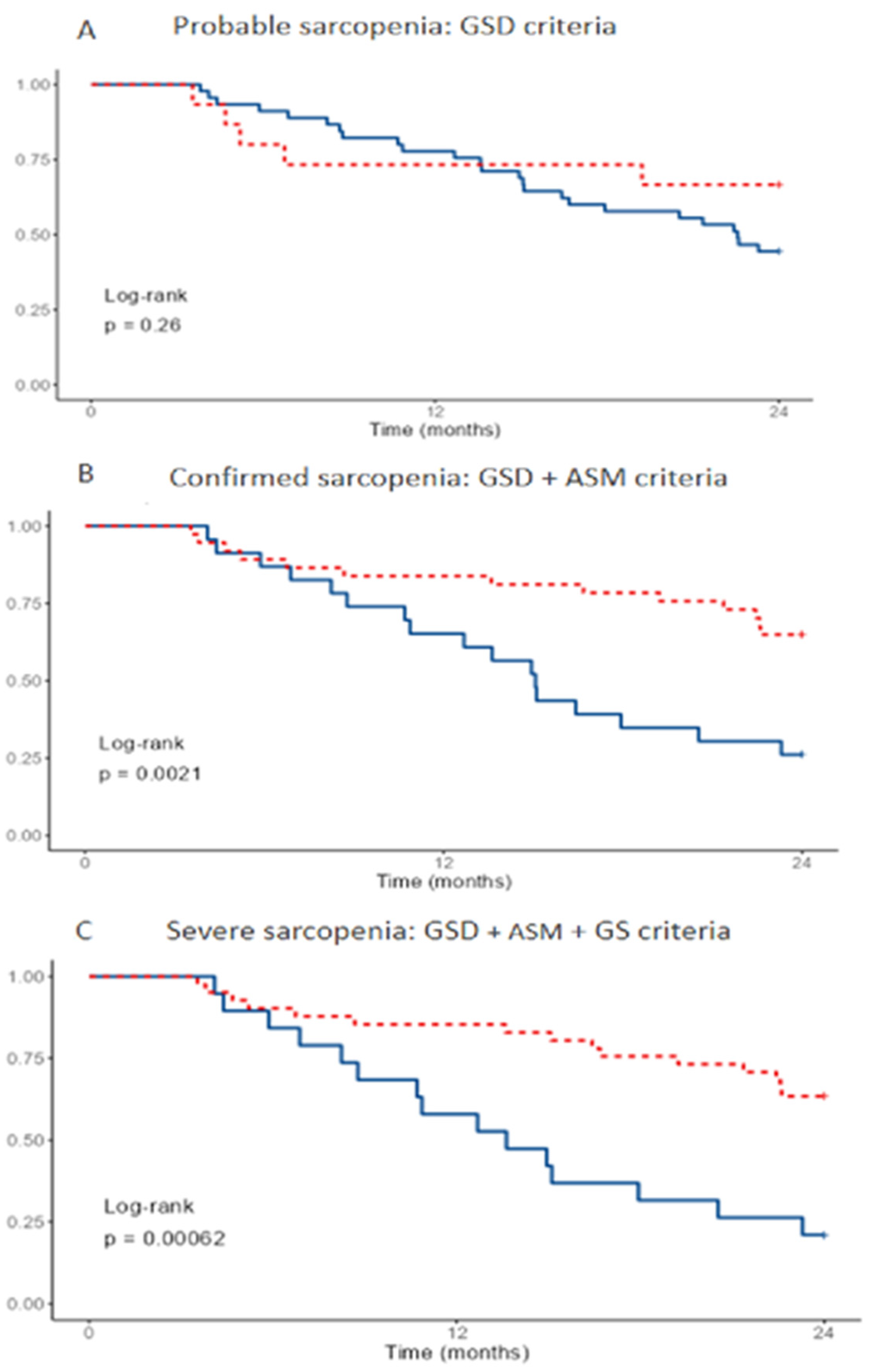
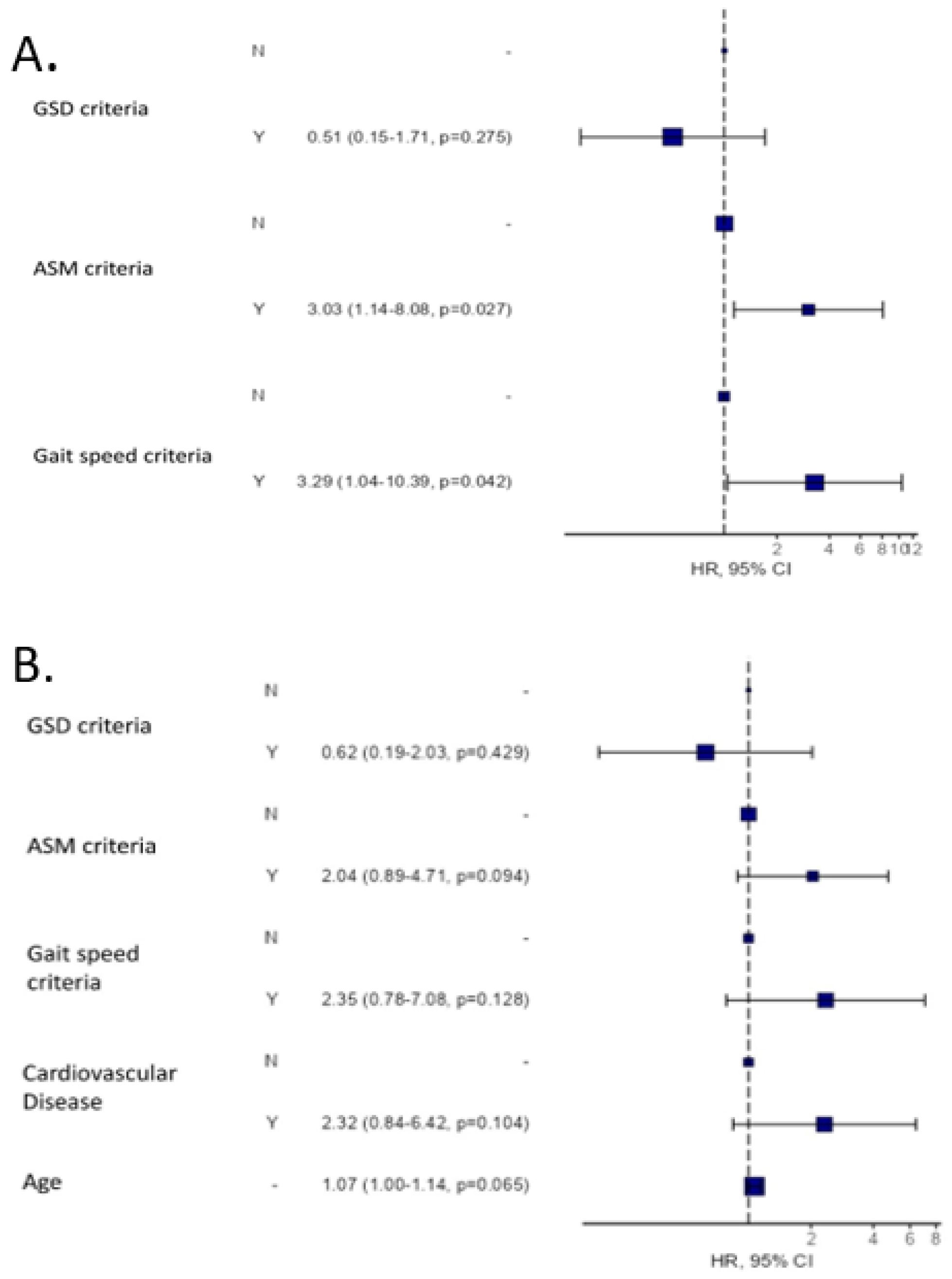
3.3. Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lang, T.; Streeper, T.; Cawthon, P.; Baldwin, K.; Taaffe, D.R.; Harris, T.B. Sarcopenia: Etiology, clinical consequences, intervention, and assessment. Osteoporos. Int. 2010, 21, 543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J.E. Sarcopenia in the elderly. Fam. Pract. 2012, 29, i44–i48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isoyama, N.; Qureshi, A.R.; Avesani, C.M.; Lindholm, B.; Bárány, P.; Heimbürger, O.; Cederholm, T.; Stenvinkel, P.; Carrero, J.J. Comparative Associations of Muscle Mass and Muscle Strength with Mortality in Dialysis Patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1720. [Google Scholar] [CrossRef]
- Lamarca, F.; Carrero, J.J.; Rodrigues, J.C.D.; Bigogno, F.G.; Fetter, R.L.; Avesani, C.M. Prevalence of sarcopenia in elderly maintenance hemodialysis patients: The impact of different diagnostic criteria. J. Nutr. Health Aging 2014, 18, 710–717. [Google Scholar] [CrossRef]
- Kim, J.K.; Choi, S.R.; Choi, M.J.; Kim, S.G.; Lee, Y.K.; Noh, J.W.; Kim, H.J.; Song, Y.R. Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease. Clin. Nutr. 2014, 33, 64–68. [Google Scholar] [CrossRef]
- Sánchez-Tocino, M.L.; Miranda-Serrano, B.; Gracia-Iguacel, C.; De-Alba-Peñaranda, A.M.; Mas-Fontao, S.; López-González, A.; Villoria-González, S.; Pereira-García, M.; Ortíz, A.; González-Parra, E. Sarcopenia assessed by 4-step EWGSOP2 in elderly hemodialysis patients: Feasibility and limitations. PLoS ONE 2022, 17, e0261459. [Google Scholar] [CrossRef]
- Kittiskulnam, P.; Chertow, G.M.; Carrero, J.J.; Delgado, C.; Kaysen, G.A.; Johansen, K.L. Sarcopenia and its individual criteria are associated, in part, with mortality among patients on hemodialysis. Kidney Int. 2017, 92, 238–247. [Google Scholar] [CrossRef]
- Avin, K.G.; Chen, N.X.; Organ, J.M.; Zarse, C.; O’Neill, K.; Conway, R.G.; Konrad, R.J.; Bacallao, R.L.; Allen, M.R.; Moe, S.M. Skeletal Muscle Regeneration and Oxidative Stress Are Altered in Chronic Kidney Disease. PLoS ONE 2016, 11, e0159411. [Google Scholar] [CrossRef] [Green Version]
- Jo, H. Workshop on sarcopenia: Muscle atrophy in old age. J. Gerontol. 1995, 50, 1–161. [Google Scholar]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older AdultsEvidence for a Phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Jassal, S.V.; Chiu, E.; Hladunewich, M. Loss of independence in patients starting dialysis at 80 years of age or older. N. Engl. J. Med. 2009, 361, 1612–1613. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockwood, K. What would make a definition of frailty successful? Age Ageing 2005, 34, 432–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; Shepard, D.S.; Katzmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Am. Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Arango-Lopera, V.E.; Arroyo, P.; Gutiérrez-Robledo, L.M.; Perez-Zepeda, M.U.; Cesari, M. Mortality as an adverse outcome of sarcopenia. J. Nutr. Health Aging 2013, 17, 259–262. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Tosato, M.; Bernabei, R.; Onder, G. Sarcopenia and mortality among older nursing home residents. J. Am. Med. Dir. Assoc. 2012, 13, 121–126. [Google Scholar] [CrossRef]
- Rolland, Y.; Czerwinski, S.; Van Kan, G.A.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [Green Version]
- Clark, B.C.; Manini, T.M. Sarcopenia =/= dynapenia. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 829–834. [Google Scholar] [CrossRef]
- Sánchez-Tocino, M.L.; González-Parra, E.; Serrano, B.M.; Gracia-Iguacel, C.; María De-Alba-Peñaranda, A.; López-González, A.; Olegario, M.G.; Ortíz, A.; Mas-Fontao, S. Evaluation of the impact of an intradialytic exercise program on sarcopenia in very elderly hemodialysis patients. Clin. Kidney J. 2020, 0, sfac046. [Google Scholar]
- Hughes, V.A.; Frontera, W.R.; Wood, M.; Evans, W.J.; Dallal, G.E.; Roubenoff, R.; Fiatarone Singh, M.A. Longitudinal muscle strength changes in older adults: Influence of muscle mass, physical activity, and health. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, B209–B217. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Wan, C.S.; Ktoris, K.; Reijnierse, E.M.; Maier, A.B. Sarcopenia Is Associated with Mortality in Adults: A Systematic Review and Meta-Analysis. Gerontology 2021, 68, 361–376. [Google Scholar] [CrossRef]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia. Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Jamal, S.A.; Leiter, R.E.; Jassal, V.; Hamilton, C.J.; Bauer, D.C. Impaired muscle strength is associated with fractures in hemodialysis patients. Osteoporos. Int. 2006, 17, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Giannaki, C.D.; Sakkas, G.K.; Karatzaferi, C.; Hadjigeorgiou, G.M.; Lavdas, E.; Liakopoulos, V.; Tsianas, N.; Koukoulis, G.N.; Koutedakis, Y.; Stefanidis, I. Evidence of increased muscle atrophy and impaired quality of life parameters in patients with Uremic restless legs syndrome. PLoS ONE 2011, 6, e25180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abellan Van Kan, G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.P.; Gomes, I.B.; de Oliveira, C.S.; Ramos, I.R.; Rocha, M.D.M.; Forgiarini, L.A.; Camelier, F.W.R.; Camelier, A.A. Accuracy of the Timed Up and Go test for predicting sarcopenia in elderly hospitalized patients. Clinics 2015, 70, 369–372. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Leal, V.O.; Mafra, D.; Fouque, D.; Anjos, L.A. Use of handgrip strength in the assessment of the muscle function of chronic kidney disease patients on dialysis: A systematic review. Nephrol. Dial. Transplant. 2011, 26, 1354–1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, M.B.; Silva, L.F.; Dantas, M.A.S.; Matos, C.M.; Lopes, G.B.; Lopes, A.A. Sex-age-specific handgrip strength and mortality in an incident hemodialysis cohort: The risk explained by nutrition and comorbidities. Int. J. Artif. Organs 2018, 41, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Gracia-Iguacel, C.; González-Parra, E.; Pérez-Gómez, M.V.; Mahíllo, I.; Egido, J.; Ortiz, A.; Carrero, J.J. Prevalencia del síndrome de desgaste proteico-energético y su asociación con mortalidad en pacientes en hemodiálisis en un centro en españa. Nefrologia 2013, 33, 495–505. [Google Scholar]
- Rodríguez-Rejón, A.I.; Ruiz-López, M.D.; Artacho, R. Diagnosis and prevalence of sarcopenia in long-term care homes: EWGSOP2 versus EWGSOP1. Nutr. Hosp. 2019, 36, 1074–1080. [Google Scholar] [PubMed] [Green Version]
- Chamney, P.W.; Wabel, P.; Moissl, U.M.; Müller, M.J.; Bosy-Westphal, A.; Korth, O.; Fuller, N.J. A whole-body model to distinguish excess fluid from the hydration of major body tissues. Am. J. Clin. Nutr. 2007, 85, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Piccoli, A.; Nescolarde, L.D.; Rosell, J. Conventional and vectorial analysis of bioimpedance in clinical practice. Nefrologia 2002, 22, 228–238. [Google Scholar] [PubMed]
- Pereira, R.A.; Cordeiro, A.C.; Avesani, C.M.; Carrero, J.J.; Lindholm, B.; Amparo, F.C.; Amodeo, C.; Cuppari, L.; Kamimura, M.A. Sarcopenia in chronic kidney disease on conservative therapy: Prevalence and association with mortality. Nephrol. Dial. Transplant. 2015, 30, 1718–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onofriescu, M.; Siriopol, D.; Voroneanu, L.; Hogas, S.; Nistor, I.; Apetrii, M.; Florea, L.; Veisa, G.; Mititiuc, I.; Kanbay, M.; et al. Overhydration, Cardiac Function and Survival in Hemodialysis Patients. PLoS ONE 2015, 10, e0135691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yajima, T.; Arao, M.; Yajima, K.; Takahashi, H.; Yasuda, K. The associations of fat tissue and muscle mass indices with all-cause mortality in patients undergoing hemodialysis. PLoS ONE 2019, 14, e0211988. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Prado, R.; Peña-Esparragoza, J.K.; Santos-Sánchez-Rey, B.; Pereira, M.; Avello, A.; Gomá-Garcés, E.; González-Rivera, M.; González-Martin, G.; Gracia-Iguacel, C.; Mahillo, I.; et al. Ultrafiltration rate adjusted to body weight and mortality in hemodialysis patients. Nefrologia 2021, 41, 426–435. [Google Scholar] [CrossRef]
- Saeed, F.; Arrigain, S.; Schold, J.D.; Nally, J.V.; Navaneethan, S.D. What are the Risk Factors for One-Year Mortality in Older Patients with Chronic Kidney Disease? An Analysis of the Cleveland Clinic CKD Registry. Nephron 2019, 141, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, Y.; Kanda, E.; Ishibashi, Y.; Yoshida, M. Sarcopenia and Frailty in PD: Impact on Mortality, Malnutrition, and Inflammation. Perit. Dial. Int. 2018, 38, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Kutner, N.G.; Zhang, R.; Huang, Y.; Painter, P. Gait Speed and Mortality, Hospitalization, and Functional Status Change Among Hemodialysis Patients: A US Renal Data System Special Study. Am. J. Kidney Dis. 2015, 66, 297–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, S.M.; Bear-Lehman, J.; Anderson, S.J. Declines in mobility and changes in performance in the instrumental activities of daily living among mildly disabled community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viccaro, L.J.; Perera, S.; Studenski, S.A. Is timed up and go better than gait speed in predicting health, function, and falls in older adults? J. Am. Geriatr. Soc. 2011, 59, 887–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bachettini, N.P.; Bielemann, R.M.; Barbosa-Silva, T.G.; Menezes, A.M.B.; Tomasi, E.; Gonzalez, M.C. Sarcopenia as a mortality predictor in community-dwelling older adults: A comparison of the diagnostic criteria of the European Working Group on Sarcopenia in Older People. Eur. J. Clin. Nutr. 2020, 74, 573–580. [Google Scholar] [CrossRef]
- Sobestiansky, S.; Michaelsson, K.; Cederholm, T. Sarcopenia prevalence and associations with mortality and hospitalisation by various sarcopenia definitions in 85–89 year old community-dwelling men: A report from the ULSAM study. BMC Geriatr. 2019, 19, 318. [Google Scholar] [CrossRef]
- Matos, C.M.; Silva, L.F.; Santana, L.D.; Santos, L.S.; Protásio, B.M.; Rocha, M.T.; Ferreira, V.L.; Azevedo, M.F.; Martins, M.T.S.; Lopes, G.B.; et al. Handgrip strength at baseline and mortality risk in a cohort of women and men on hemodialysis: A 4-year study. J. Ren. Nutr. 2014, 24, 157–162. [Google Scholar] [CrossRef]
- Landi, F.; Cruz-Jentoft, A.J.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia and mortality risk in frail older persons aged 80 years and older: Results from ilSIRENTE study. Age Ageing 2013, 42, 203–209. [Google Scholar] [CrossRef] [Green Version]
- Azzolino, D.; Saporiti, E.; Proietti, M.; Cesari, M. Nutritional Considerations in Frail Older Patients with COVID-19. J. Nutr. Health Aging 2020, 24, 696–698. [Google Scholar] [CrossRef]
| All (n = 60) | Male (n = 41) | Female (n = 19) | * p Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 81.85 ± 5.58 | 81.31 ± 5.72 | 83 ± 5.22 | 0.27 |
| Dialysis vintage (months) | 36 (21–67) | 42 (21–62) | 36 (21–80) | 0.78 |
| Comorbidities | ||||
| Diabetes | 24/60 (40%) | 18/41 (44%) | 6/19 (32%) | 0.365 |
| Cardiovascular disease | 40/60 (67%) | 32/41 (78%) | 8/19 (42%) | 0.006 |
| Malignancy | 21/60 (35%) | 17/41 (41%) | 4/19 (21%) | 0.123 |
| Analytical data | ||||
| Albumin (g/dL) | 3.66 ± 0.47 | 3.69 ± 0.41 | 3.59 ± 0.60 | 0.43 |
| Hemoglobin (g/dL) | 11.26 ± 1.13 | 11.40 ± 1.02 | 11.26 ± 1.13 | 0.63 |
| C Reactive Protein (mg/L) | 0.74 (0.33–1.62) | 0.82 (0.39–1.65) | 0.74 (0.26–1.50) | 0.82 |
| 25OH Vitamin D3 (ng/mL) | 21.51 ± 13.13 | 21.14 ± 12.95 | 22.31 ± 13.81 | 0.75 |
| Kt/Vurea | 1.80 ± 0.38 | 1.70 ± 0.372 | 2.01 ± 0.30 | 0.002 |
| Anthropometric data | ||||
| Body mass index (kg/m2) | 25.20 ± 3.64 | 25.73 ± 3.40 | 24.08 ± 3.95 | 0.10 |
| Mid-Upper Arm Circumference (cm) | 25.69 ± 3.11 | 26.62 ± 2.66 | 25.69 ± 3.11 | 0.26 |
| Waist Perimeter (cm) | 92.78 ± 10.41 | 97 ± 7.58 | 83.87 ± 10.07 | <0.001 |
| Hip Perimeter (cm) | 100.57 ± 7.23 | 101.61 ± 6.92 | 98.39 ± 7.56 | 0.121 |
| Waist hip index | 0.92 ± 0.08 | 0.95 ± 0.69 | 0.85 ± 0.06 | <0.001 |
| Tricipital Fold (mm) | 11.89 ± 4.32 | 10.86 ± 3.83 | 14.08 ± 4.60 | 0.008 |
| Abdominal Fold (mm) | 18.38 ± 6.35 | 19.79 ± 6.98 | 15.76 ± 4,39 | 0.054 |
| Subscapular Fold (mm) | 15.39 ± 7.09 | 16.42 ± 6.69 | 13.22 ± 7.61 | 0.115 |
| Body composition | ||||
| Muscle Mass (kg) | 19.27 ± 3.82 | 20.98 ± 3.22 | 15.57 ± 1.87 | <0.001 |
| Fast Mass (kg) | 22.91 ± 5.07 | 22.91 ± 5.07 | 22 ± 7.40 | 0.581 |
| Total Body Water (L) | 32.41 ± 6.52 | 35.52 ± 5.17 | 25.69 ± 3.15 | <0.001 |
| Overhydration (L) | 1. 10 ± 1.41 | 1.26 ± 1.61 | 0.75 ± 1.21 | 0.233 |
| Individual Criterion | Value for Criterion | Consistent with Sarcopenia, n (%) | Diagnostic Algorithm | Consistent with Sarcopenia, n (%) |
|---|---|---|---|---|
| Find | ||||
| SARC-F (points) | 2.6 ± 2.3 | 18 (30%) | ||
| Assess: Probable sarcopenia | ||||
| GSD (Kg) | 19.2 ± 6.6 | 45 (75%) | GSD | 45 (75%) |
| STS5 (s) | 20.3 ± 6.3 | 53 (88%) | STS-5 | 53 (88%) |
| GSD and/or STS-5 | 58 (97%) | |||
| Confirm: Sarcopenia confirmed | ||||
| ASM (kg) | 19.3 ± 3.8 | 24 (40%) | GSD + ASM | 23 (38%) |
| STS-5 + ASM | 22 (37%) | |||
| GSD and/or STS-5 + ASM | 24 (40%) | |||
| Severity: Severe sarcopenia | ||||
| GS (m/s) | 0.69 ± 0.27 | 42 (70%) | GSD + ASM + GS | 19 (32%) |
| STS-5 + ASM + GS | 19 (32%) | |||
| GSD and/or STS-5 + ASM + GS | 19 (32%) | |||
| TUG (s) | 19.1 ± 12.1 | 22 (37%) | GSD + ASM + TUG | 11 (18%) |
| STS-5 + ASM + TUG | 11 (18%) | |||
| GSD and/or STS5 +ASM + TUG | 11 (18%) | |||
| SPPB (points) | 6.2 ± 2.9 | 45 (75%) | GSD + ASM + SPPB | 21 (35%) |
| STS-5 + ASM + SPPB | 21 (35%) | |||
| GSD and/or STS-5 + ASM + SPPB | 21 (35%) | |||
| GSD and/or STS-5 + ASM + GS and/or TUG and/or SPPB | 22 (37%) | |||
| Alive, n = 30 | Deceased, n = 30 | p Value | |
|---|---|---|---|
| Demographic data | |||
| Age (years) | 79.9 ± 4.9 | 83.8 ± 5.6 | 0.005 |
| Dialysis vintage (months) | 47.9 ± 42.3 | 51.6 ± 39.1 | 0.728 |
| Comorbidities | |||
| Diabetes | 11.0 (36.7%) | 13.0 (43.3%) | 0.598 |
| Cardiovascular disease | 15.0 (50.0%) | 25.0 (83.3%) | 0.006 |
| Malignancy | 9.0 (30.0%) | 12.0 (40.0%) | 0.417 |
| Analytical data | |||
| Albumin (g/dL) | 3.7 ± 0.4 | 3.6 ± 0.5 | 0.233 |
| Hemoglobin (g/dL) | 11.5 ± 1.0 | 11.2 ± 1.1 | 0.225 |
| C Reactive Protein (mg/L) | 0.7 ± 0.7 | 2.5 ± 3.7 | 0.013 |
| 25OH Vitamin D3 (ng/mL) | 19.3 ± 10.2 | 23.8 ± 15.4 | 0.194 |
| Kt/Vurea | 1.8 ± 0.4 | 1.8 ± 0.3 | 0.533 |
| Anthropometric data | |||
| Body mass index (kg/m2) | 25.5 ± 4.3 | 24.9 ± 2.9 | 0.518 |
| Mid-Upper Arm Circumference (cm) | 26.7 ± 3.2 | 25.9 ± 2.4 | 0.338 |
| Waist Perimeter (cm) | 92.2 ± 11.2 | 93.4 ± 9.7 | 0.689 |
| Hip Perimeter (cm) | 100.1 ± 8.3 | 101.1 ± 6.1 | 0.607 |
| Waist hip index | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.828 |
| Tricipital Fold (mm) | 1.2 ± 0.5 | 1.2 ± 0.4 | 0.637 |
| Abdominal Fold (mm) | 18.9 ± 7.1 | 17.7 ± 5.3 | 0.558 |
| Subscapular Fold (mm) | 15.6 ± 7.9 | 15.1 ± 6.2 | 0.788 |
| Body composition | |||
| Muscle Mass (kg) | 20.0 ± 4.5 | 18.6 ± 2.9 | 0.150 |
| Fast Mass (kg) | 22.9 ± 7.1 | 22.3 ± 4.4 | 0–703 |
| Total Body Water (L) | 33.0 ± 7.4 | 31.8 ± 5.5 | 0.488 |
| Overhydration (L) | 0.9 ± 1.6 | 1.2 ± 1.4 | 0.584 |
| Sarcopenia | Alive, n = 30 | Deceased, n = 30 | p Value | |
|---|---|---|---|---|
| Find | ||||
| SARC-F (points) | YES, n = 20 | 10/20 (50%) | 10/20 (50%) | 1.000 |
| NO, n = 40 | 20/40 (50%) | 20/40 (50%) | ||
| Assess | ||||
| GSD (Kg) | YES, n = 15 | 10/15 (66%) | 5/15 (33%) | 0.136 |
| NO, n = 45 | 20/45 (44%) | 25/45 (56%) | ||
| STS5 (s) | YES, n = 53 | 25/53 (47%) | 28/53 (53%) | 0.227 |
| NO, n = 7 | 5/7 (71.5%) | 2/7 (28.5%) | ||
| Confirm | ||||
| ASM (kg) | YES, n = 24 | 7/24 (29%) | 17/24 (71%) | 0.008 |
| NO, n = 36 | 23/36 (64%) | 13/36 (36%) | ||
| Severity | ||||
| GS (m/s) | YES, n = 42 | 15/42 (36%) | 27/42 (64%) | >0.001 |
| NO, n = 18 | 15/18 (83%) | 3/18 (17%) | ||
| TUG (s) | YES, n = 22 | 5/22 (23%) | 17/22 (77%) | 0.001 |
| NO, n = 38 | 25/38 (66%) | 13/38 (33%) | ||
| SPPB (points) | YES, n = 45 | 19/45 (42%) | 26/45 (58%) | 0.036 |
| NO, n = 15 | 11/15 (73%) | 4/15 (27%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Tocino, M.L.; Miranda-Serrano, B.; López-González, A.; Villoria-González, S.; Pereira-García, M.; Gracia-Iguacel, C.; González-Ibarguren, I.; Ortíz-Arduan, A.; Mas-Fontao, S.; González-Parra, E. Sarcopenia and Mortality in Older Hemodialysis Patients. Nutrients 2022, 14, 2354. https://doi.org/10.3390/nu14112354
Sánchez-Tocino ML, Miranda-Serrano B, López-González A, Villoria-González S, Pereira-García M, Gracia-Iguacel C, González-Ibarguren I, Ortíz-Arduan A, Mas-Fontao S, González-Parra E. Sarcopenia and Mortality in Older Hemodialysis Patients. Nutrients. 2022; 14(11):2354. https://doi.org/10.3390/nu14112354
Chicago/Turabian StyleSánchez-Tocino, M. Luz, Blanca Miranda-Serrano, Antonio López-González, Silvia Villoria-González, Mónica Pereira-García, Carolina Gracia-Iguacel, Isabel González-Ibarguren, Alberto Ortíz-Arduan, Sebastian Mas-Fontao, and Emilio González-Parra. 2022. "Sarcopenia and Mortality in Older Hemodialysis Patients" Nutrients 14, no. 11: 2354. https://doi.org/10.3390/nu14112354
APA StyleSánchez-Tocino, M. L., Miranda-Serrano, B., López-González, A., Villoria-González, S., Pereira-García, M., Gracia-Iguacel, C., González-Ibarguren, I., Ortíz-Arduan, A., Mas-Fontao, S., & González-Parra, E. (2022). Sarcopenia and Mortality in Older Hemodialysis Patients. Nutrients, 14(11), 2354. https://doi.org/10.3390/nu14112354