
Effect of Different Types of Intermittent Fasting on Biochemical and Anthropometric Parameters among Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)—A Systematic Review

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
1.1. Pathophysiology: Multiple Hits Hypothesis
1.2. Intermittent Fasting
2. Materials and Methods
2.1. Types of Participants
2.2. Types of Interventions
2.3. Types of Comparisons
2.4. Types of Outcomes
2.5. Types of Studies
2.6. Search Strategy and Study Selection
3. Results
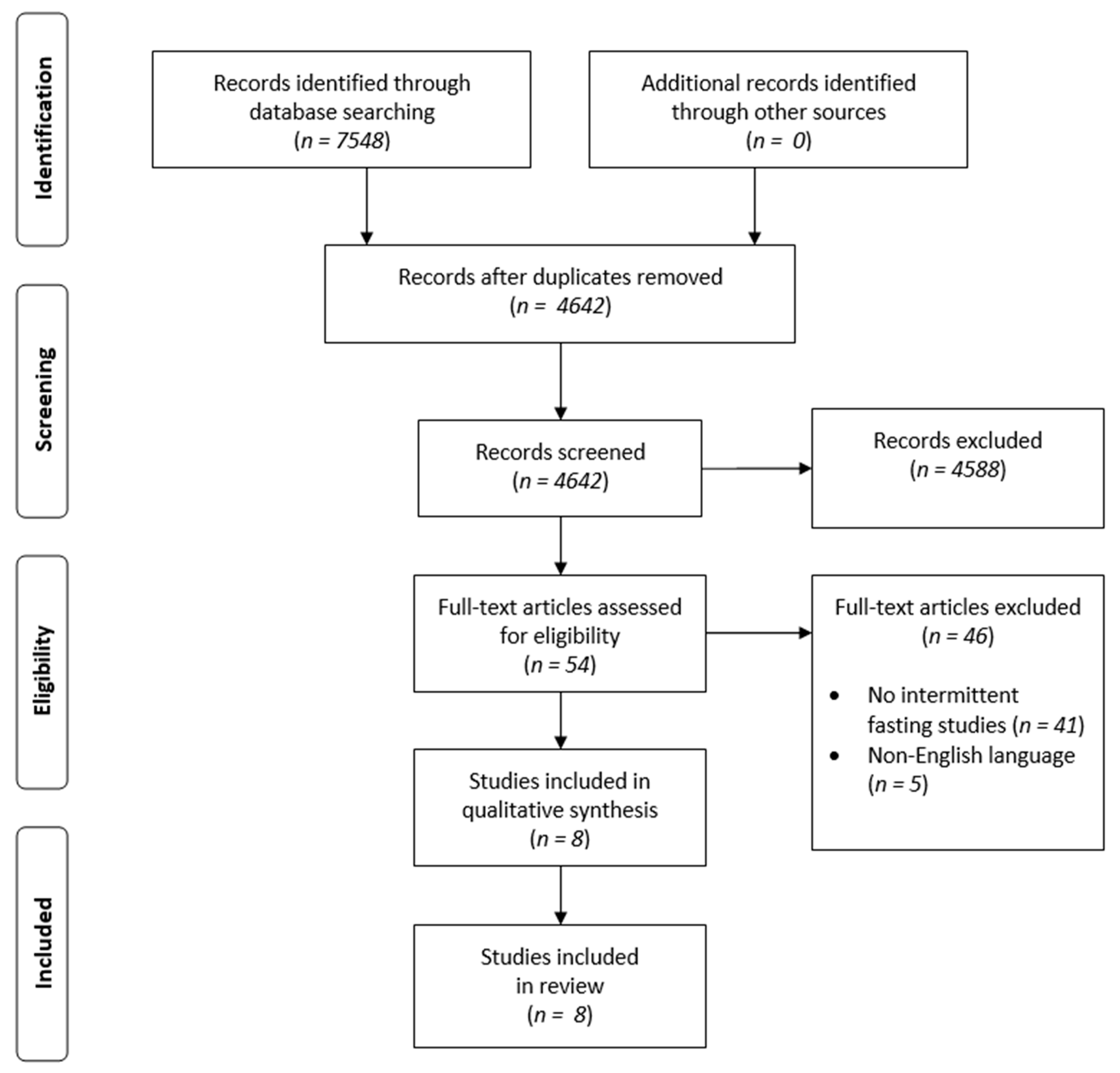
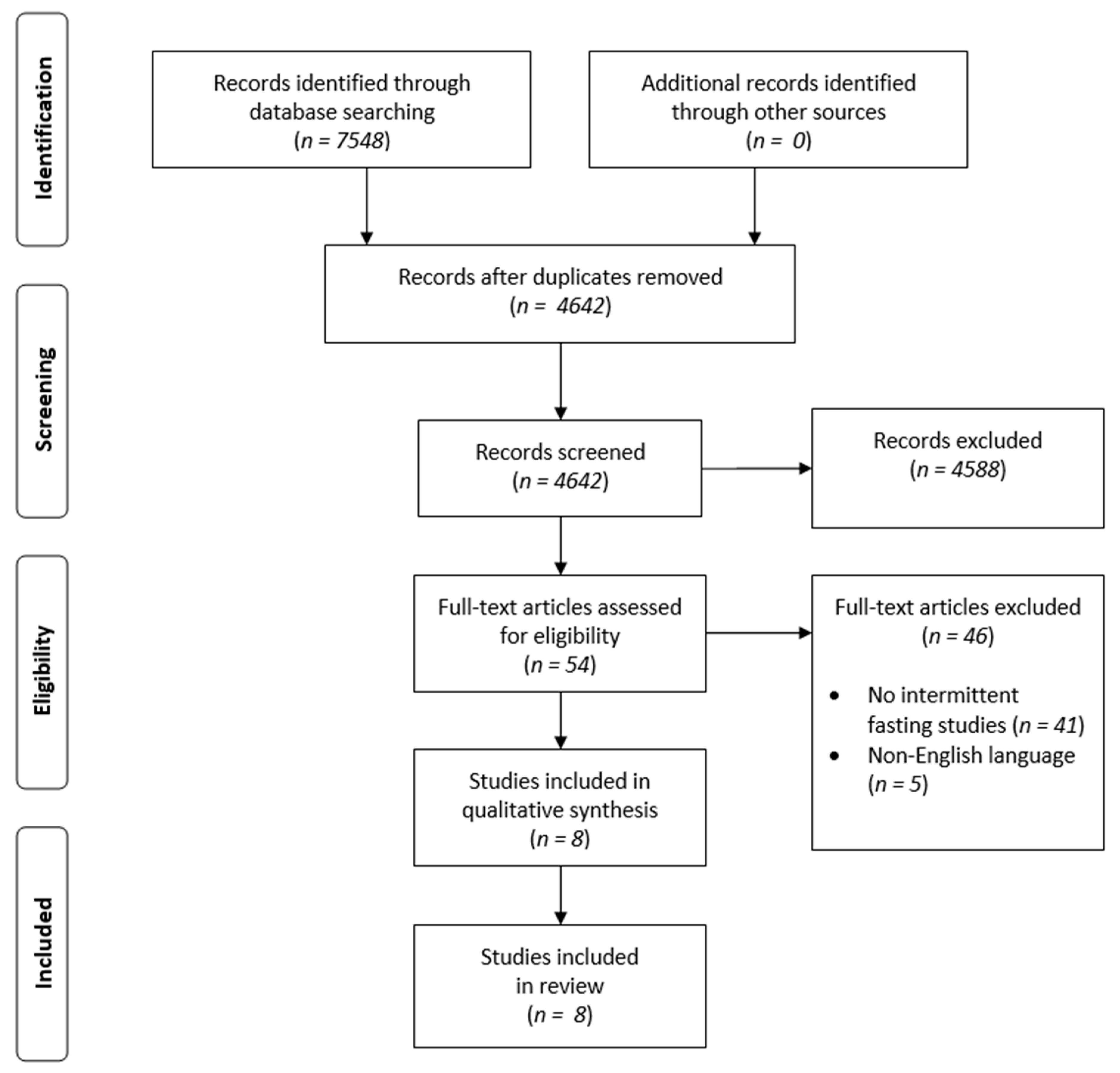
3.1. Study Selection
3.2. Participant Characteristics
3.3. Fasting Strategy and Duration
3.4. Time-Restricted Fasting (TRF)
3.5. Alternate-Day Modified Fasting (ADMF)
3.6. Modified Fasting Regimens (MFR)
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pavlides, M.; Cobbold, J. Non-Alcoholic Fatty Liver Disease. Medicine 2019, 47, 728–733. [Google Scholar] [CrossRef]
- Younossi, Z.M. Non-Alcoholic Fatty Liver Disease—A Global Public Health Perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, C.D.; Stengel, J.; Asike, M.I.; Torres, D.M.; Shaw, J.; Contreras, M.; Landt, C.L.; Harrison, S.A. Prevalence of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis among a Largely Middle-Aged Population Utilizing Ultrasound and Liver Biopsy: A Prospective Study. Gastroenterology 2011, 140, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Słomko, J.; Zalewska, M.; Niemiro, W.; Kujawski, S.; Słupski, M.; Januszko-Giergielewicz, B.; Zawadka-Kunikowska, M.; Newton, J.; Hodges, L.; Kubica, J.; et al. Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 1659. [Google Scholar] [CrossRef]
- Welsh, J.A.; Karpen, S.; Vos, M.B. Increasing Prevalence of Nonalcoholic Fatty Liver Disease Among United States Adolescents, 1988–1994 to 2007–2010. J. Pediatr. 2013, 162, 496–500. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Priyadarshi, R.N.; Anand, U. Non-Alcoholic Fatty Liver Disease: Growing Burden, Adverse Outcomes and Associations. J. Clin. Transl. Hepatol. 2020, 8, 76–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Vanni, E.; Bugianesi, E.; Kotronen, A.; De Minicis, S.; Yki-Järvinen, H.; Svegliati-Baroni, G. From the Metabolic Syndrome to NAFLD or Vice Versa? Dig. Liver Dis. 2010, 42, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Byrne, C.D.; Bonora, E.; Targher, G. Nonalcoholic Fatty Liver Disease and Risk of Incident Type 2 Diabetes: A Meta-Analysis. Diabetes Care 2018, 41, 372–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases: Hepatology, Vol. XX, No. X, 2017. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, D.; Andreou, E. Role of Diet on Non-Alcoholic Fatty Liver Disease: An Updated Narrative Review. World J. Hepatol 2015, 7, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The Multiple-Hit Pathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Targher, G.; Day, C.P.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef] [Green Version]
- Mahfood Haddad, T.; Hamdeh, S.; Kanmanthareddy, A.; Alla, V.M. Nonalcoholic Fatty Liver Disease and the Risk of Clinical Cardiovascular Events: A Systematic Review and Meta-Analysis. Diabetes Metab Syndr 2017, 11 (Suppl. 1), S209–S216. [Google Scholar] [CrossRef]
- Patterson, R.E.; Sears, D.D. Metabolic Effects of Intermittent Fasting. Annu. Rev. Nutr. 2017, 37, 371–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoddy, K.K.; Marlatt, K.L.; Çetinkaya, H.; Ravussin, E. Intermittent Fasting and Metabolic Health: From Religious Fast to Time-Restricted Feeding. Obesity 2020, 28, S29–S37. [Google Scholar] [CrossRef]
- Patterson, R.E.; Laughlin, G.A.; LaCroix, A.Z.; Hartman, S.J.; Natarajan, L.; Senger, C.M.; Martínez, M.E.; Villaseñor, A.; Sears, D.D.; Marinac, C.R.; et al. Intermittent Fasting and Human Metabolic Health. J. Acad. Nutr. Diet. 2015, 115, 1203–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, H.; Qin, Y.-L.; Shi, Z.-Y.; Chen, J.-H.; Zeng, M.-J.; Zhou, W.; Chen, R.-Q.; Chen, Z.-Y. Effects of Alternate-Day Fasting on Body Weight and Dyslipidaemia in Patients with Non-Alcoholic Fatty Liver Disease: A Randomised Controlled Trial. BMC Gastroenterol. 2019, 19, 219. [Google Scholar] [CrossRef]
- Aliasghari, F.; Izadi, A.; Gargari, B.P.; Ebrahimi, S. The Effects of Ramadan Fasting on Body Composition, Blood Pressure, Glucose Metabolism, and Markers of Inflammation in NAFLD Patients: An Observational Trial. J. Am. Coll. Nutr. 2017, 36, 640–645. [Google Scholar] [CrossRef]
- Rahimi, H.; Habibi, M.E.; Gharavinia, A.; Emami, M.; Baghaei, A.; Tavakol, N. Effect of Ramadan Fasting on Alanine Transferase (ALT) in Nonalcoholic Fatty Liver Disease (NAFLD). J. Nutr. Fast. Health 2017, 5, 107–112. [Google Scholar] [CrossRef]
- Arabi, S.M.; Nematy, M.; Hashemi, M.; Safarian, M. The Effect of Ramadan Fasting on Plasma Free Fatty Acids among Non-Alcoholic Fatty Liver Patients. J. Nutr. Fast. Health 2016, 4. [Google Scholar] [CrossRef]
- Arabi, S.M.; Zarifi, S.H.; Nematy, M.; Safarian, M. The Effect of Ramadan Fasting on Non-Alcoholic Fatty Liver Disease (NAFLD) Patients. J. Nutr. Fast. Health 2015, 3, 40–74. [Google Scholar] [CrossRef]
- Johari, M.I.; Yusoff, K.; Haron, J.; Nadarajan, C.; Ibrahim, K.N.; Wong, M.S.; Hafidz, M.I.A.; Chua, B.E.; Hamid, N.; Arifin, W.N.; et al. A Randomised Controlled Trial on the Effectiveness and Adherence of Modified Alternate-Day Calorie Restriction in Improving Activity of Non-Alcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 11232. [Google Scholar] [CrossRef]
- Holmer, M.; Lindqvist, C.; Petersson, S.; Moshtaghi-Svensson, J.; Tillander, V.; Brismar, T.B.; Hagström, H.; Stål, P. Treatment of NAFLD with Intermittent Calorie Restriction or Low-Carb High-Fat Diet—A Randomised Controlled Trial. JHEP Rep. 2021, 3, 100256. [Google Scholar] [CrossRef]
- Mari, A.; Khoury, T.; Baker, M.; Said Ahmad, H.; Abu Baker, F.; Mahamid, M. The Impact of Ramadan Fasting on Fatty Liver Disease Severity: A Retrospective Case Control Study from Israel. Isr. Med. Assoc. J. 2021, 23, 94–98. [Google Scholar] [PubMed]
- Kasper Ter Horst; Serlie, M. Fructose Consumption, Lipogenesis, and Non-Alcoholic Fatty Liver Disease. Nutrients 2017, 9, 981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with Diet, Physical Activity and Exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [Green Version]
- Perumpail, B.J.; Cholankeril, R.; Yoo, E.R.; Kim, D.; Ahmed, A. An Overview of Dietary Interventions and Strategies to Optimize the Management of Non-Alcoholic Fatty Liver Disease. Diseases 2017, 5, 23. [Google Scholar] [CrossRef]
- Mirizzi, A.; Franco, I.; Leone, C.M.; Bonfiglio, C.; Cozzolongo, R.; Notarnicola, M.; Giannuzzi, V.; Tutino, V.; De Nunzio, V.; Bruno, I.; et al. Effects of Some Food Components on Non-Alcoholic Fatty Liver Disease Severity: Results from a Cross-Sectional Study. Nutrients 2019, 11, 2744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quesada-Vázquez, S.; Aragonès, G.; Del Bas, J.M.; Escoté, X. Diet, Gut Microbiota and Non-Alcoholic Fatty Liver Disease: Three Parts of the Same Axis. Cells 2020, 9, 176. [Google Scholar] [CrossRef] [Green Version]
- Riazi, K.; Raman, M.; Taylor, L.; Swain, M.G.; Shaheen, A.A. Dietary Patterns and Components in Nonalcoholic Fatty Liver Disease (NAFLD): What Key Messages Can Health Care Providers Offer? Nutrients 2019, 11, 2878. [Google Scholar] [CrossRef] [Green Version]
- Allaf, M.; Elghazaly, H.; Mohamed, O.G.; Fareen, M.F.K.; Zaman, S.; Salmasi, A.-M.; Tsilidis, K.; Dehghan, A. Intermittent Fasting for the Prevention of Cardiovascular Disease. Cochrane Database Syst. Rev. 2021, 2021. [Google Scholar] [CrossRef]
- Różański, G.; Kujawski, S.; Newton, J.L.; Zalewski, P.; Słomko, J. Curcumin and Biochemical Parameters in Metabolic-Associated Fatty Liver Disease (MAFLD)—A Review. Nutrients 2021, 13, 2654. [Google Scholar] [CrossRef]
- Sadeghirad, B.; Motaghipisheh, S.; Kolahdooz, F.; Zahedi, M.J.; Haghdoost, A.A. Islamic Fasting and Weight Loss: A Systematic Review and Meta-Analysis. Public Health Nutr 2014, 17, 396–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvaresh, A.; Razavi, R.; Abbasi, B.; Yaghoobloo, K.; Hassanzadeh, A.; Mohammadifard, N.; Safavi, S.M.; Hadi, A.; Clark, C.C.T. Modified Alternate-Day Fasting vs. Calorie Restriction in the Treatment of Patients with Metabolic Syndrome: A Randomized Clinical Trial. Complement. Ther. Med. 2019, 47, 102187. [Google Scholar] [CrossRef] [PubMed]
- Razavi, R.; Parvaresh, A.; Abbasi, B.; Yaghoobloo, K.; Hassanzadeh, A.; Mohammadifard, N.; Clark, C.C.T.; Morteza Safavi, S. The Alternate-Day Fasting Diet Is a More Effective Approach than a Calorie Restriction Diet on Weight Loss and Hs-CRP Levels. Int. J. Vitam. Nutr Res. 2021, 91, 242–250. [Google Scholar] [CrossRef]
- Park, J.; Seo, Y.-G.; Paek, Y.-J.; Song, H.J.; Park, K.H.; Noh, H.-M. Effect of Alternate-Day Fasting on Obesity and Cardiometabolic Risk: A Systematic Review and Meta-Analysis. Metabolism 2020, 111, 154336. [Google Scholar] [CrossRef] [PubMed]
- Faris, M.A.-I.E.; Kacimi, S.; Al-Kurd, R.A.; Fararjeh, M.A.; Bustanji, Y.K.; Mohammad, M.K.; Salem, M.L. Intermittent Fasting during Ramadan Attenuates Proinflammatory Cytokines and Immune Cells in Healthy Subjects. Nutr. Res. 2012, 32, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Kord-Varkaneh, H.; Nazary-Vannani, A.; Mokhtari, Z.; Salehi-Sahlabadi, A.; Rahmani, J.; Clark, C.C.T.; Fatahi, S.; Zanghelini, F.; Hekmatdoost, A.; Okunade, K.; et al. The Influence of Fasting and Energy Restricting Diets on Blood Pressure in Humans: A Systematic Review and Meta-Analysis. High Blood Press. Cardiovasc. Prev 2020, 27, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Kang, J.; Kim, S.H.; Chung, H.S.; Kim, Y.J.; Yu, J.M.; Cho, S.T.; Oh, C.-M.; Kim, T. Beneficial Effects of Time-Restricted Eating on Metabolic Diseases: A Systemic Review and Meta-Analysis. Nutrients 2020, 12, 1267. [Google Scholar] [CrossRef]
- Faris, M.; Jahrami, H.; Abdelrahim, D.; Bragazzi, N.; BaHammam, A. The Effects of Ramadan Intermittent Fasting on Liver Function in Healthy Adults: A Systematic Review, Meta-Analysis, and Meta-Regression. Diabetes Res. Clin. Pract. 2021, 178, 108951. [Google Scholar] [CrossRef]
- Mirmiran, P.; Bahadoran, Z.; Gaeini, Z.; Moslehi, N.; Azizi, F. Effects of Ramadan Intermittent Fasting on Lipid and Lipoprotein Parameters: An Updated Meta-Analysis. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 906–915. [Google Scholar] [CrossRef]
- Faris, M.A.-I.; Jahrami, H.; BaHammam, A.; Kalaji, Z.; Madkour, M.; Hassanein, M. A Systematic Review, Meta-Analysis, and Meta-Regression of the Impact of Diurnal Intermittent Fasting during Ramadan on Glucometabolic Markers in Healthy Subjects. Diabetes Res. Clin. Pr. 2020, 165, 108226. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Hong, N.; Kim, K.; Cho, S.; Lee, M.; Lee, Y.; Lee, Y.; Kang, E.S.; Cha, B.-S.; Lee, B.-W. The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitale, R.; Kim, Y. The Effects of Intermittent Fasting on Glycemic Control and Body Composition in Adults with Obesity and Type 2 Diabetes: A Systematic Review. Metab. Syndr. Relat. Disord. 2020, 18, 450–461. [Google Scholar] [CrossRef]

{kind=link}
| Parameter | Defined Criteria for the Current Study |
|---|---|
| P (population) | Adult patients with MAFLD |
| I (intervention | Any type of intermittent fasting |
| C (comparison) | No special comparison criteria |
| O (outcomes) | Changes in biochemical parameters or anthropometric measurements * |
| S (study design) | Any type apart from case reports and reviews |
| n | Age (year) | BMI (kg/m2) | |
|---|---|---|---|
| Rahimi, 2017 [20] | 34 (25 men, 9 women) | 46.03 ± 11.72 | 29.46 ± 4.52 |
| Cai, 2019; ADMF group [18] | 95 (35 men, 60 women) | 35.50 ± 4.417 | 26.12 ± 2.21 |
| Cai, 2019; TRF group [18] | 95 (29 men, 66 women) | 33.56 ± 6.23 | 26.76 ± 1.59 |
| Arabi, 2016 [21] | 50 (33 men, 17 women) | 40.52 ± 10.90 | 31.38 ± 4.9 |
| Arabi, 2016 [22] | 50 (33 men, 17 women) | 40.52 ± 10.90 | 29.50 (men) 34.15 (women) |
| Aliasghari, 2017 [19] | 42 (25 men, 17 women) | 37.59 ± 7.06 | 30.09 ± 4.49 |
| Johari, 2019 [23] | 33 (24 men, 9 women) * | 45.33 ± 10.77 | 31.73 |
| Holmer, 2021 [24] | 25 (13 men, 12 women) | 57 ± 10 | 32.3 ± 2.7 |
| Mari, 2021 [25] | 74 (39 men, 35 women) | 51.8 ± 20.9 | 36.7 ± 7.1 |
| Study Design | Type of Intervention | Duration | n (Study Group) | n (Control Group) | Tested Parameters | |
|---|---|---|---|---|---|---|
| Rahimi, 2017 [20] | Prospective observational cross-sectional study | Ramadan | 4 weeks | 34 | 26 | Body weight, BMI, ALT |
| Cai, 2019 [18] | RCT | ADMF | 12 weeks | 95 | 79 | Body weight, BMI, WC, Fat mass, Lean mass, FBG, TG, TC, LDL, HDL |
| TRF | 95 | 79 | ||||
| Arabi, 2016 [21] | Cross-sectional study | Ramadan | 27.3 ± 5 days (25–30) | 50 | - | BMI, Palmitic acid, Oleic acid, Elaidic acid |
| Arabi, 2016 [22] | Prospective observational cross-sectional study | Ramadan | 27.3 ± 5 days (25–30) | 50 | - | BMI, WC, Fat mass, Free fatty mass, SBP, DBP, ALT, AST, FBG, Insulin, TG, HDL, LDL |
| Aliasghari, 2017 [19] | Observational trial | Ramadan | 4 weeks | 42 | 41 | Body weight, BMI, WC, Waist:Hip ratio, Fat mass, FBG, Insulin, HOMA-IR, IL-6, hs-CRP |
| Johari, 2019 [23] | RCT | ADMF | 8 weeks | 33 * | 10 | Body weight, BMI, ALT, AST, FBG, TG, TC, LDL, HDL |
| Holmer, 2021 [24] | RCT | MFR | 12 weeks | 25 | 24 | Body weight, BMI, Waist:hip ratio, SBP, DBP, ALT, AST, HOMA-IR, HbA1c, TG, TC, LDL-C, HDL-C |
| Mari, 2021 [25] | Retrospective, case-control study | Ramadan | 4 weeks | 74 | 81 | BMI, ALT, AST, Insulin, HOMA-IR, hs-CRP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Różański, G.; Pheby, D.; Newton, J.L.; Murovska, M.; Zalewski, P.; Słomko, J. Effect of Different Types of Intermittent Fasting on Biochemical and Anthropometric Parameters among Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)—A Systematic Review. Nutrients 2022, 14, 91. https://doi.org/10.3390/nu14010091
Różański G, Pheby D, Newton JL, Murovska M, Zalewski P, Słomko J. Effect of Different Types of Intermittent Fasting on Biochemical and Anthropometric Parameters among Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)—A Systematic Review. Nutrients. 2022; 14(1):91. https://doi.org/10.3390/nu14010091
Chicago/Turabian StyleRóżański, Gracjan, Derek Pheby, Julia L. Newton, Modra Murovska, Paweł Zalewski, and Joanna Słomko. 2022. "Effect of Different Types of Intermittent Fasting on Biochemical and Anthropometric Parameters among Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)—A Systematic Review" Nutrients 14, no. 1: 91. https://doi.org/10.3390/nu14010091
APA StyleRóżański, G., Pheby, D., Newton, J. L., Murovska, M., Zalewski, P., & Słomko, J. (2022). Effect of Different Types of Intermittent Fasting on Biochemical and Anthropometric Parameters among Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)—A Systematic Review. Nutrients, 14(1), 91. https://doi.org/10.3390/nu14010091