
Assessment of Maternal Macular Pigment Optical Density (MPOD) as a Potential Marker for Dietary Carotenoid Intake during Lactation in Humans

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Measurements
2.2.1. Macular Pigment Optical Density (MPOD) Measurement
2.2.2. Maternal Dietary Intake
2.2.3. Breastmilk
2.3. Statistical Analysis
3. Results
3.1. Cohort Description
3.2. Serial MPOD Measures
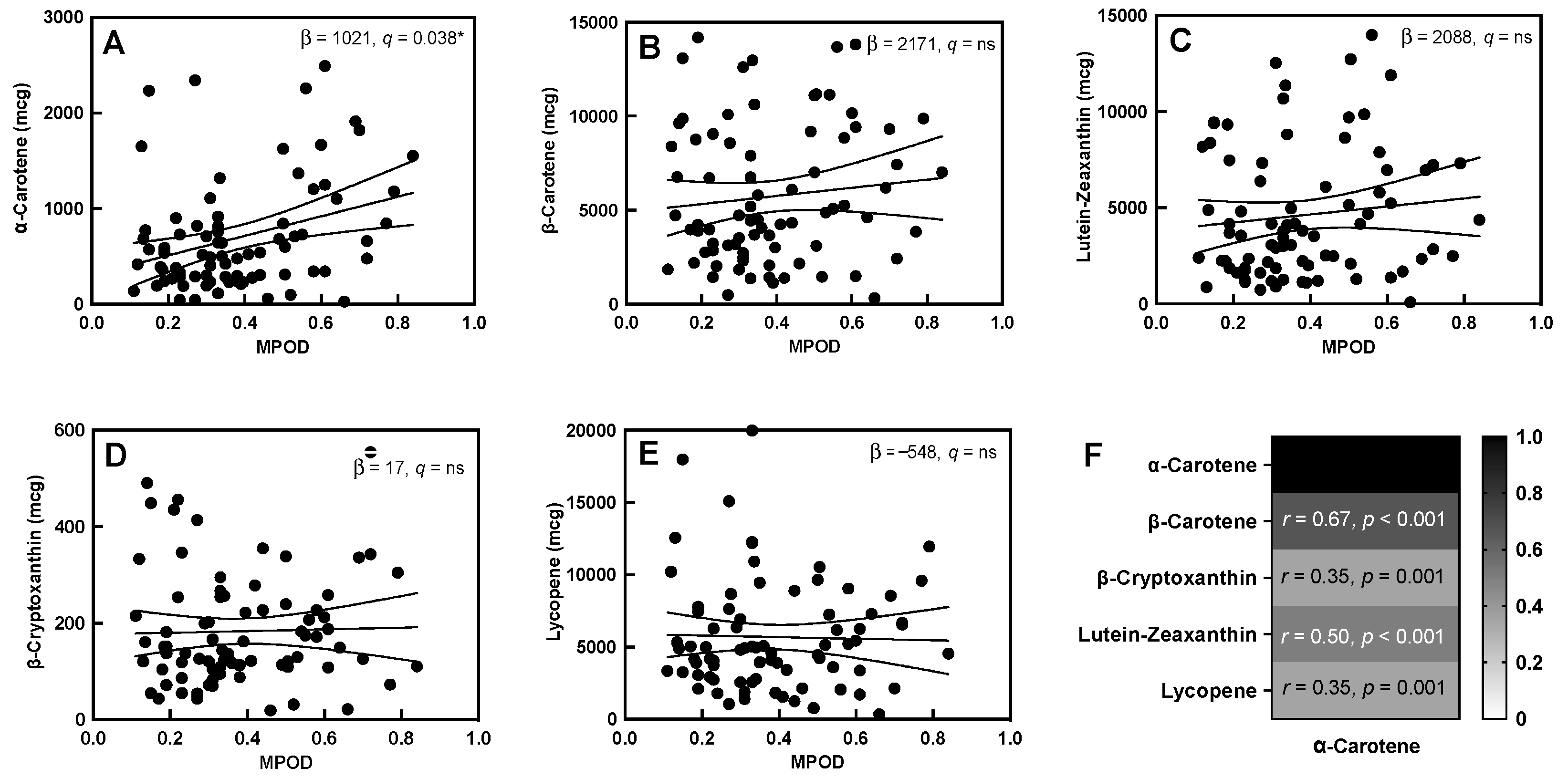
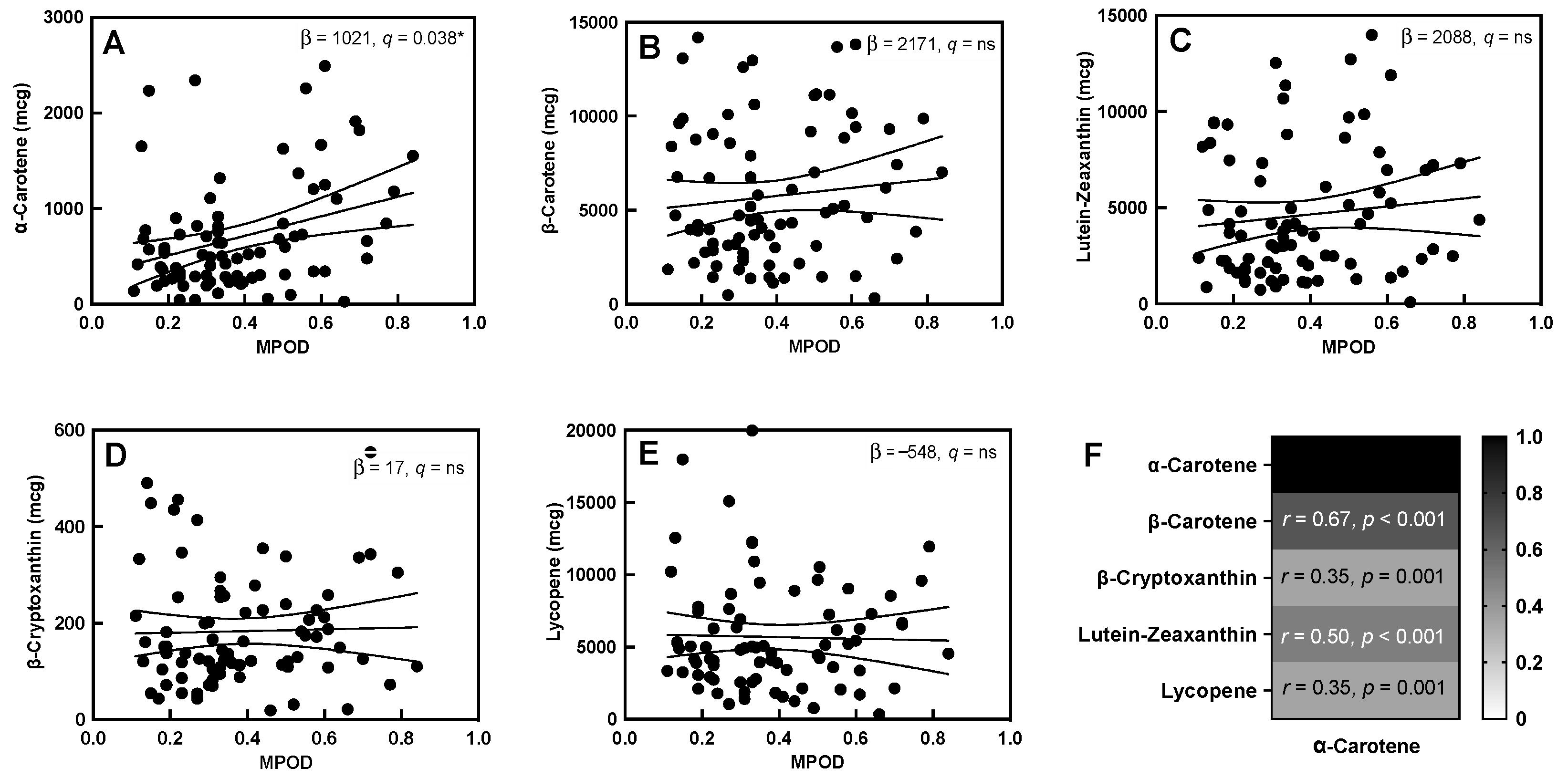
3.3. MPOD-Carotenoid Association
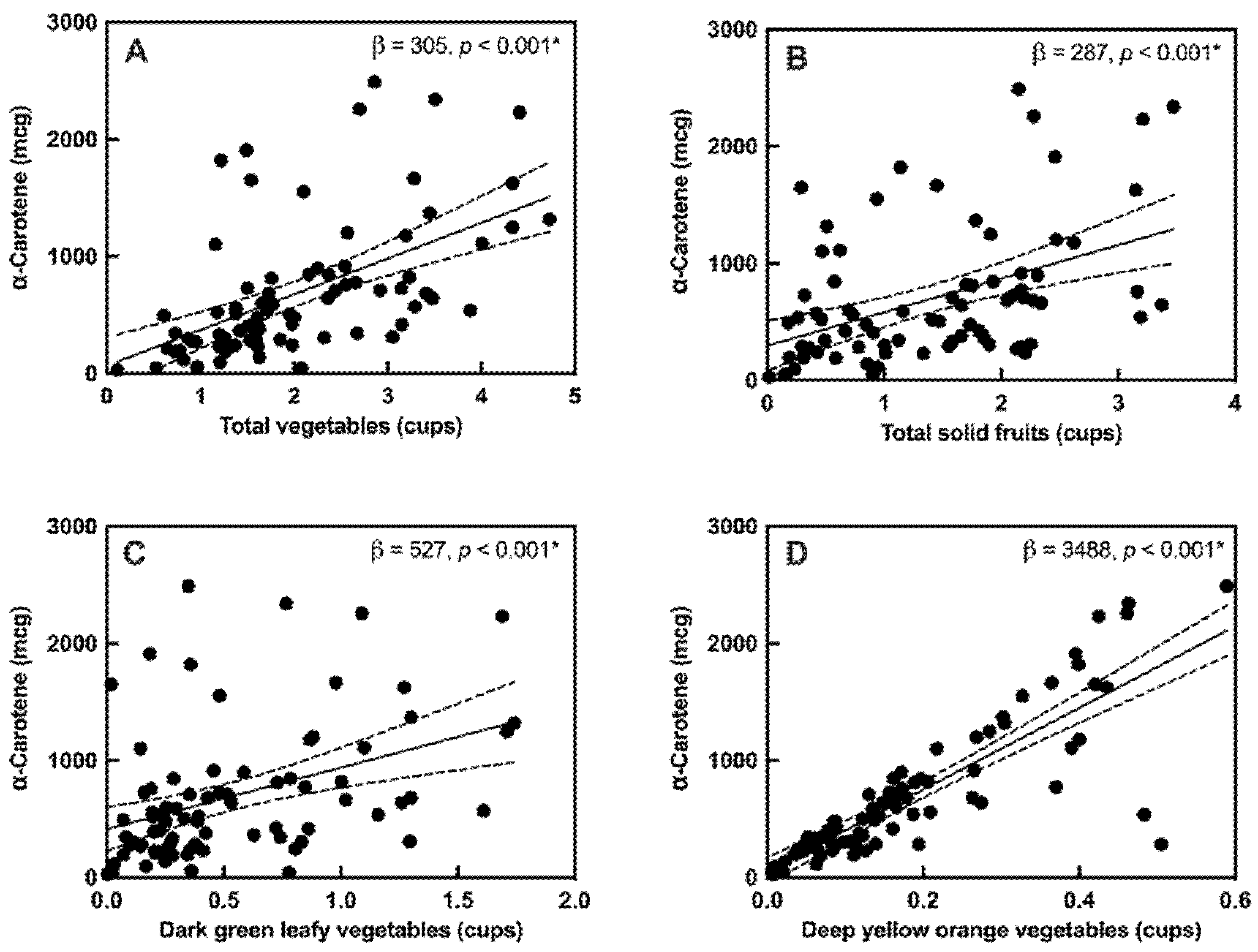
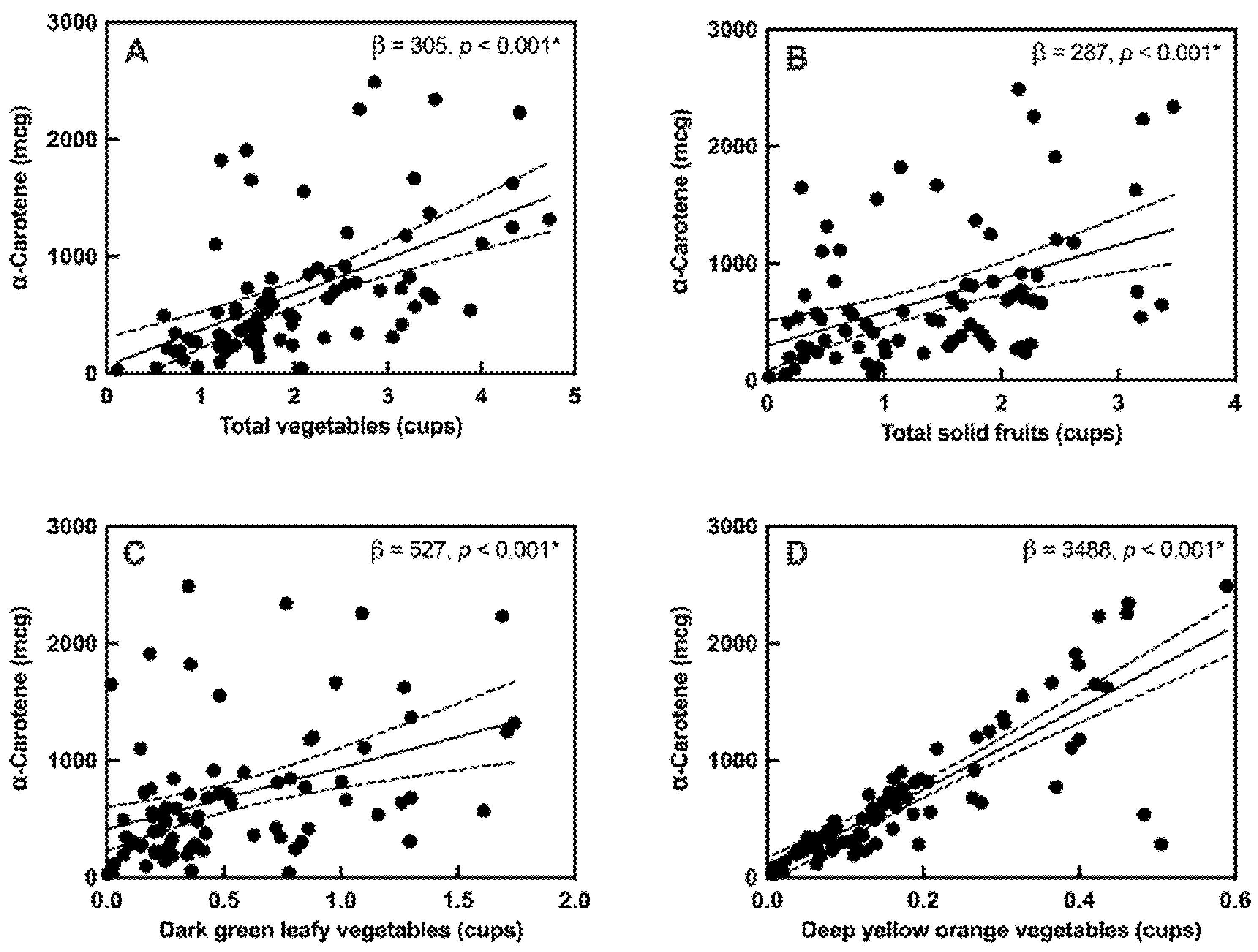
3.4. Material Diet-Breastmilk Association
3.5. MPOD-Breastmilk Association
4. Discussion
4.1. MPOD and α-Carotene Intake: Marker of Healthy Diet?
4.2. Lutein Isoforms
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [Green Version]
- Bravi, F.; Wiens, F.; Decarli, A.; Pont, A.D.; Agostoni, C.; Ferraroni, M. Impact of maternal nutrition on breast-milk composition: A systematic review. Am. J. Clin. Nutr. 2016, 104, 646–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Zhao, D.; Mao, X.; Xia, Y.; Baker, P.N.; Zhang, H. Maternal Dietary Patterns and Pregnancy Outcome. Nutrients 2016, 8, 351. [Google Scholar] [CrossRef] [PubMed]
- Dani, C.; Lori, I.; Favelli, F.; Frosini, S.; Messner, H.; Wanker, P.; De Marini, S.; Oretti, C.; Boldrini, A.; Massimiliano, C.; et al. Lutein and zeaxanthin supplementation in preterm infants to prevent retinopathy of prema-turity: A randomized controlled study. J. Matern. Fetal. Neonatal. Med. 2012, 25, 523–527. [Google Scholar] [CrossRef]
- Koletzko, B.; Godfrey, K.M.; Poston, L.; Szajewska, H.; Van Goudoever, J.B.; De Waard, M.; Brands, B.; Grivell, R.M.; Deussen, A.R.; Dodd, J.M.; et al. Nutrition during pregnancy, lactation and early childhood and its implications for maternal and long-term child health: The early nutrition project recommendations. Ann. Nutr. Metab. 2019, 74, 93–106. [Google Scholar] [CrossRef]
- Mulder, K.A.; Innis, S.M.; Rasmussen, B.F.; Wu, B.T.; Richardson, K.J.; Hasman, D. Plasma lutein concentrations are related to dietary intake, but unrelated to dietary saturated fat or cognition in young children. J. Nutr. Sci. 2014, 3, e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasano, H.; Obana, A.; Sharifzadeh, M.; Bernstein, P.S.; Okazaki, S.; Gohto, Y.; Seto, T.; Gellermann, W. Optical Detection of Macular Pigment Formation in Premature Infants. Transl. Vis. Sci. Technol. 2018, 7, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vohr, B.R.; Poggi Davis, E.; Wanke, C.A.; Krebs, N.F. Neurodevelopment: The Impact of Nutrition and Inflammation During Pre-conception and Pregnancy in Low-Resource Settings. Pediatrics 2017, 139 (Suppl. 1), S38–S49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Souza Mesquita, L.M.; Mennitti, L.V.; De Rosso, V.V.; Pisani, L.P. The role of vitamin A and its pro-vitamin carotenoids in fetal and neonatal programming: Gaps in knowledge and metabolic pathways. Nutr. Rev. 2021, 79, 76–87. [Google Scholar] [CrossRef]
- Zielińska, M.A.; Wesołowska, A.; Pawlus, B.; Hamułka, J. Health Effects of Carotenoids during Pregnancy and Lactation. Nutrients 2017, 9, 838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Bae, T.J.; Jung, B.M.; Yi, H.; Jung, J.A.; Chang, N. Association between lutein intake and lutein concentrations in human milk samples from lactating mothers in South Korea. Eur. J. Clin. Nutr. 2017, 71, 681. [Google Scholar] [CrossRef] [Green Version]
- Sherry, C.L.; Oliver, J.S.; Renzi-Hammond, L.; Marriage, B.J. Lutein Supplementation Increases Breast Milk and Plasma Lutein Concentrations in Lactating Women and Infant Plasma Concentrations but Does Not Affect Other Carotenoids. J. Nutr. 2014, 144, 1256–1263. [Google Scholar] [CrossRef] [Green Version]
- Zielinska, M.A.; Hamulka, J.; Wesolowska, A. Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients 2019, 11, 193. [Google Scholar] [CrossRef] [Green Version]
- Steinemann, N.; Grize, L.; Ziesemer, K.; Kauf, P.; Probst-Hensch, N.; Brombach, C. Relative validation of a food frequency questionnaire to estimate food intake in an adult population. Food Nutr. Res. 2017, 61, 1305193. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Aal, E.S.M.; Akhtar, H.; Zaheer, K.; Ali, R. Dietary sources of lutein and zeaxanthin carotenoids and their role in eye health. Nutrients 2013, 5, 1169–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, L.; Liu, R.; Du, J.H.; Liu, T.; Wu, S.S.; Liu, X.H. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients 2016, 8, 426. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Haslam, D.; Avendano, E.; Johnson, E.J. Lutein/zeaxanthin intake and visual outcomes in adults with healthy eyes: Qualitative gap analysis. Cogent Med. 2019, 6, 1683939. [Google Scholar] [CrossRef]
- Bernstein, P.S.; Delori, F.C.; Richer, S.; Van Kuijk, F.J.; Wenzel, A.J. The value of measurement of macular carotenoid pigment optical densities and distributions in age-related macular degeneration and other retinal disorders. Vis. Res. 2010, 50, 716–728. [Google Scholar] [CrossRef] [Green Version]
- Curran-Celentano, J.; Hammond, B.R., Jr.; Ciulla, T.A.; Cooper, D.A.; Pratt, L.M.; Danis, R.B. Relation between dietary intake, serum concentrations, and retinal concentrations of lutein and zeaxanthin in adults in a Midwest population. Am. J. Clin. Nutr. 2001, 74, 796–802. [Google Scholar] [CrossRef]
- Meagher, K.A.; Thurnham, D.I.; Beatty, S.; Howard, A.N.; Connolly, E.; Cummins, W.; Nolan, J.M. Serum response to supplemental macular carotenoids in subjects with and without age-related macular degeneration. Br. J. Nutr. 2012, 110, 289–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, T.; Rasmussen, H.M.; Chen, C.-Y.O.; Johnson, E.J. Avocado consumption increases macular pigment density in older adults: A randomized, controlled trial. Nutrients 2017, 9, 919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, L.M.; Tharmarajah, S.; Jia, Y.; Semba, R.D.; Schaumberg, D.A.; Robinson, K.A. The Effect of Lutein/Zeaxanthin Intake on Human Macular Pigment Optical Density: A Systematic Review and Meta-Analysis. Adv. Nutr. Int. Rev. J. 2021, 12, 2244–2254. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T. Heterochromatic flicker photometry. Arch. Biochem. Biophys. 2004, 430, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Snodderly, D.; Handelman, G.J.; Adler, A.J. Distribution of individual macular pigment carotenoids in central retina of macaque and squirrel monkeys. Investig. Ophthalmol. Vis. Sci. 1991, 32, 268–279. [Google Scholar]
- Xu, X.; Zhao, X.; Berde, Y.; Low, Y.L.; Kuchan, M.J. Milk and Plasma Lutein and Zeaxanthin Concentrations in Chinese Breast-Feeding Mother–Infant Dyads with Healthy Maternal Fruit and Vegetable Intake. J. Am. Coll. Nutr. 2018, 38, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Renzi-Hammond, L.M.; Bovier, E.R.; Fletcher, L.M.; Miller, L.S.; Mewborn, C.M.; Lindbergh, C.A.; Baxter, J.H.; Hammond, B.R. Effects of a Lutein and Zeaxanthin Intervention on Cognitive Function: A Randomized, Double-Masked, Placebo-Controlled Trial of Younger Healthy Adults. Nutrients 2017, 9, 1246. [Google Scholar] [CrossRef] [Green Version]
- Manzoni, P.; Stolfi, I.; Pedicino, R.; Vagnarelli, F.; Mosca, F.; Pugni, L.; Bollani, L.; Pozzi, M.; Gomez, K.; Tzialla, C.; et al. Human milk feeding prevents retinopathy of prematurity (ROP) in preterm VLBW neonates. Early Hum. Dev. 2013, 89 (Suppl. 1), S64–S68. [Google Scholar] [CrossRef]
- Henriksen, B.S.; Chan, G.; Hoffman, R.O.; Sharifzadeh, M.; Ermakov, I.V.; Gellermann, W.; Bernstein, P.S. Interrelationships between maternal carotenoid status and newborn infant macular pigment optical density and carotenoid status. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5568–5578. [Google Scholar] [CrossRef]
- Barnett, S.M.; Khan, N.A.; Walk, A.M.; Raine, L.B.; Moulton, C.; Cohen, N.J.; Kramer, A.F.; Hammond, B.R.; Renzi-Hammond, L.; Hillman, C.H. Macular pigment optical density is positively associated with academic performance among preadolescent children. Nutr. Neurosci. 2017, 21, 632–640. [Google Scholar] [CrossRef]
- Beatty, S.; Nolan, J.; Kavanagh, H.; Donovan, O.O. Macular pigment optical density and its relationship with serum and dietary levels of lutein and zeaxanthin. Arch. Biochem. Biophys. 2004, 430, 70–76. [Google Scholar] [CrossRef]
- Eggersdorfer, M.; Wyss, A. Carotenoids in human nutrition and health. Arch. Biochem. Biophys. 2018, 652, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R.; Ciulla, T.A.; Snodderly, D. Macular pigment density is reduced in obese subjects. Investig. Ophthalmol. Vis. Sci. 2002, 43, 47–50. [Google Scholar]
- Hammond, B.; Johnson, E.J.; Russell, R.M.; Krinsky, N.I.; Yeum, K.J.; Edwards, R.B.; Snodderly, D. Dietary modification of human macular pigment density. Investig. Ophthalmol. Vis. Sci. 1997, 38, 1795–1801. [Google Scholar]
- Nolan, J.M.; Stack, J.; O’Connell, E.; Beatty, S. The relationships between macular pigment optical density and its constituent carotenoids in diet and serum. Investig. Ophthalmol. Vis. Sci. 2007, 48, 571–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ochoa Becerra, M.; Mojica Contreras, L.; Hsieh Lo, M.; Mateos Díaz, J.; Castillo Herrera, G. Lutein as a functional food ingredient: Stability and bioavailability. J. Funct. Foods 2020, 66, 103771. [Google Scholar] [CrossRef]
- Tanprasertsuk, J.; Li, B.; Bernstein, P.S.; Vishwanathan, R.; Johnson, M.A.; Poon, L.; Johnson, E.J. Relationship between Concentrations of Lutein and StARD3 among Pediatric and Geriatric Human Brain Tissue. PLoS ONE 2016, 11, e0155488. [Google Scholar]
- Osborne, M.; Porto, K.; Patel, K.; Soviravong, S.; White, R.; Barrow, K.; Luthra, N.; Hammond, B.R.; Stringham, J.; Tracy, Q. Investigating macular pigment optical density in pregnant mothers during prenatal and postnatal stages. In Proceedings of the 38th Annual Convention of the Behavioral Sciences, Psi Chi International Honor Society, Athens, GA, USA, 10 April 2015. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics, median (inter-quartile range, IQR) | |
| Age (years) | 33 (30–36) |
| Body mass index (BMI) (kg/m2) | 27 (25–30) |
| Time of MPOD measurements postpartum (days) | 30 (22–59) |
| Time of FFQ collection postpartum (days) | 35 (23–60) |
| Time of breastmilk sample collection (days) | 108 (99–119) |
| Ethnicity, number (%) | |
| Hispanic or Latino | 6 (7.5%) |
| Not Hispanic or Latino | 65 (87.5%) |
| Not reported | 4 (5.0%) |
| Race, number (%) | |
| White | 56 (70.0%) |
| Black or African American | 11 (13.8%) |
| Asian | 6 (7.5%) |
| More than one race | 2 (2.5%) |
| Not reported | 5 (6.2%) |
| Highest Degree Earned, number (%) | |
| High school diploma or equivalency (GED) | 7 (8.7%) |
| Associate degree (junior college) | 7 (8.7%) |
| Bachelor’s degree | 31 (38.7%) |
| Master’s degree | 21 (26.3%) |
| Doctorate professional | 11 (13.8%) |
| Other | 3 (3.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Hassan, A.; Vyas, R.; Zhang, Y.; Sisitsky, M.; Gagoski, B.; Litt, J.S.; Larsen, R.J.; Kuchan, M.J.; Lasekan, J.B.; Sutton, B.P.; et al. Assessment of Maternal Macular Pigment Optical Density (MPOD) as a Potential Marker for Dietary Carotenoid Intake during Lactation in Humans. Nutrients 2022, 14, 182. https://doi.org/10.3390/nu14010182
Al-Hassan A, Vyas R, Zhang Y, Sisitsky M, Gagoski B, Litt JS, Larsen RJ, Kuchan MJ, Lasekan JB, Sutton BP, et al. Assessment of Maternal Macular Pigment Optical Density (MPOD) as a Potential Marker for Dietary Carotenoid Intake during Lactation in Humans. Nutrients. 2022; 14(1):182. https://doi.org/10.3390/nu14010182
Chicago/Turabian StyleAl-Hassan, Ateka, Rutvi Vyas, Yue Zhang, Michaela Sisitsky, Borjan Gagoski, Jonathan S. Litt, Ryan J. Larsen, Matthew J. Kuchan, John B. Lasekan, Brad P. Sutton, and et al. 2022. "Assessment of Maternal Macular Pigment Optical Density (MPOD) as a Potential Marker for Dietary Carotenoid Intake during Lactation in Humans" Nutrients 14, no. 1: 182. https://doi.org/10.3390/nu14010182
APA StyleAl-Hassan, A., Vyas, R., Zhang, Y., Sisitsky, M., Gagoski, B., Litt, J. S., Larsen, R. J., Kuchan, M. J., Lasekan, J. B., Sutton, B. P., Grant, P. E., Ou, Y., & Morton, S. U. (2022). Assessment of Maternal Macular Pigment Optical Density (MPOD) as a Potential Marker for Dietary Carotenoid Intake during Lactation in Humans. Nutrients, 14(1), 182. https://doi.org/10.3390/nu14010182