
Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Test Nutritional Data and Polish Reference Method
2.2. Sample Size and Study Outcome
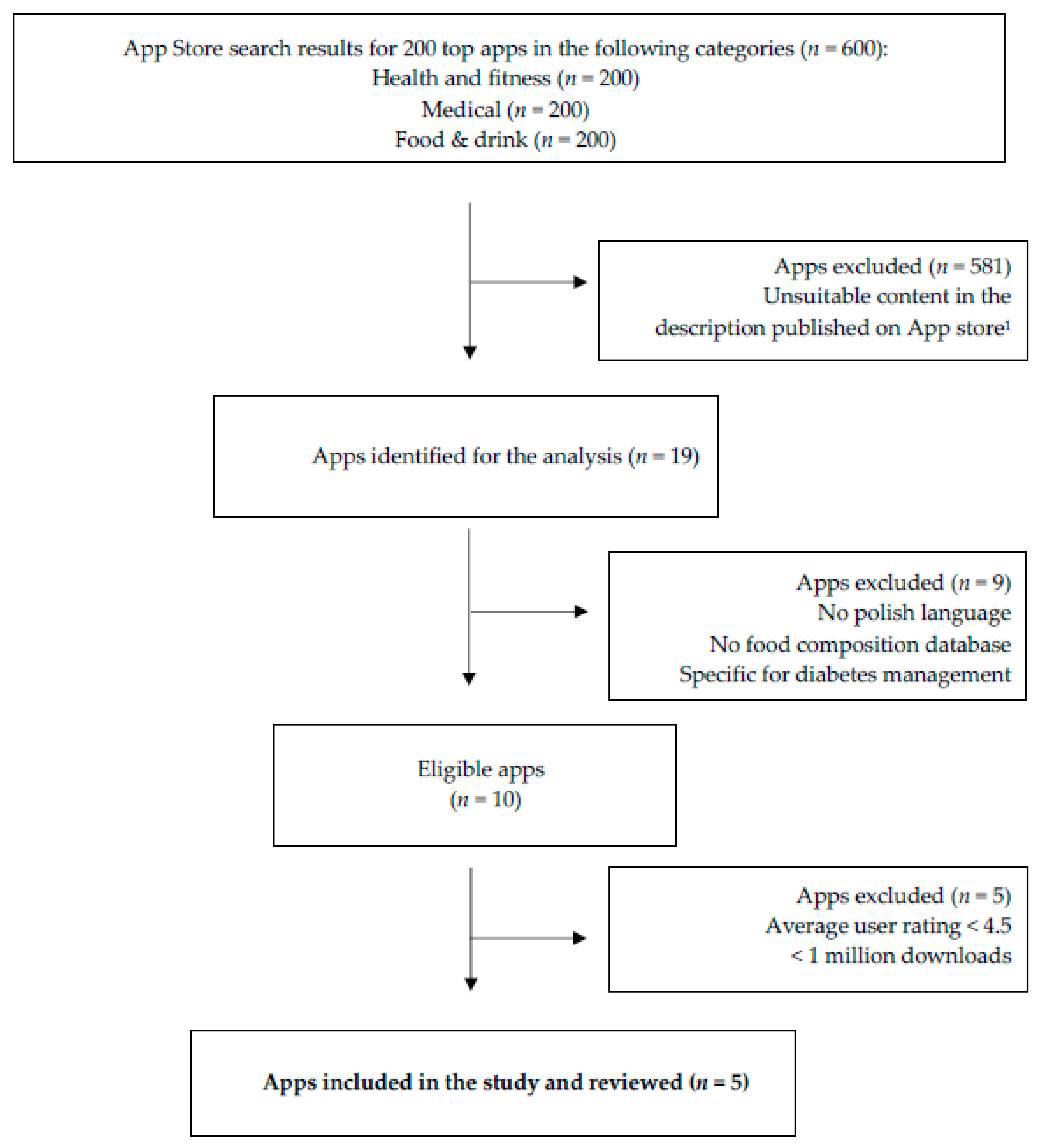
2.3. Identification and Selection of Mobile Apps
2.4. The Assessment of Nutritional and Technological Features of Mobile Apps
2.5. Input of Nutritional Data into Mobile Apps
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of Study Participants and Selected Nutrition-Related Apps
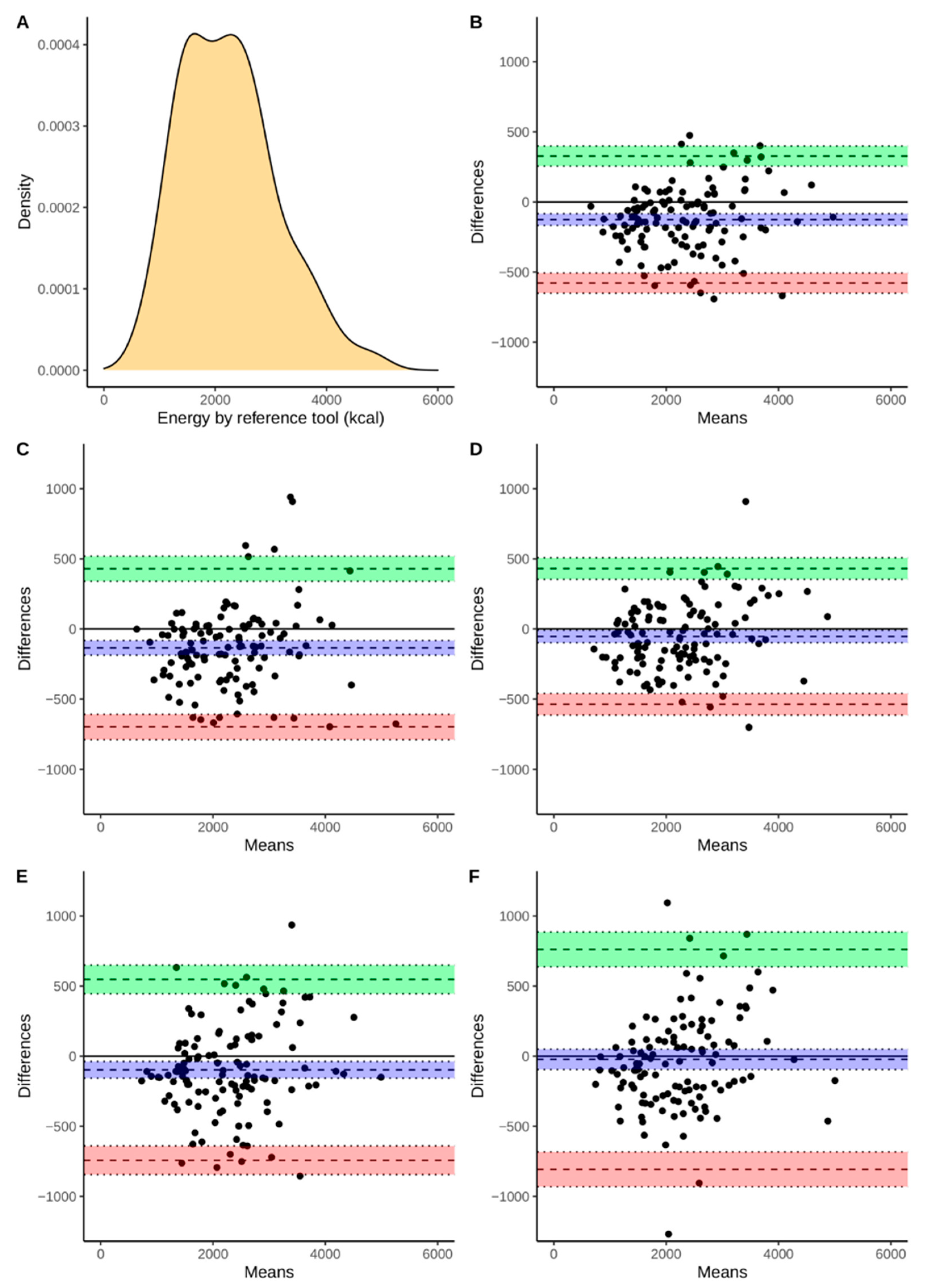
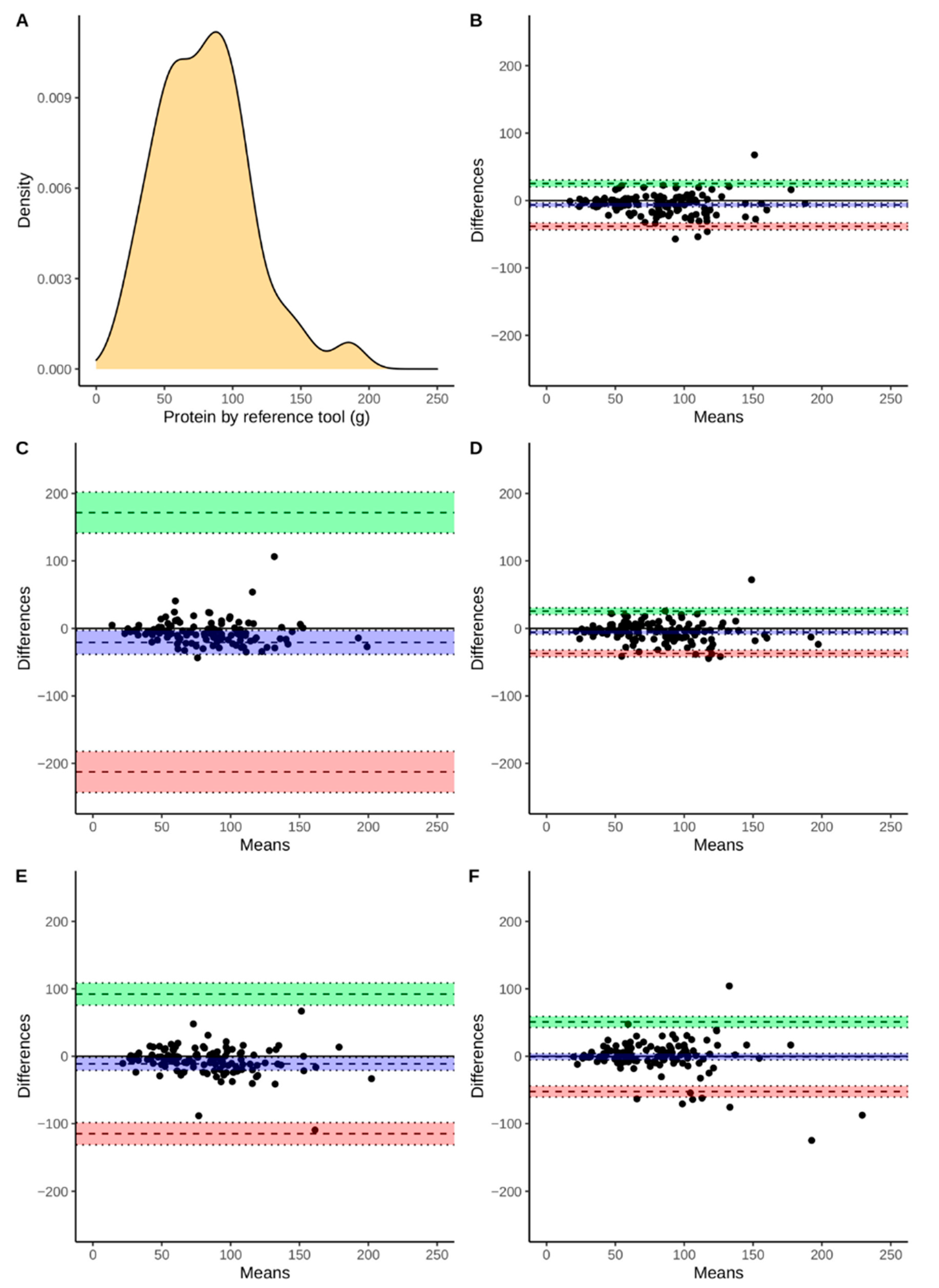
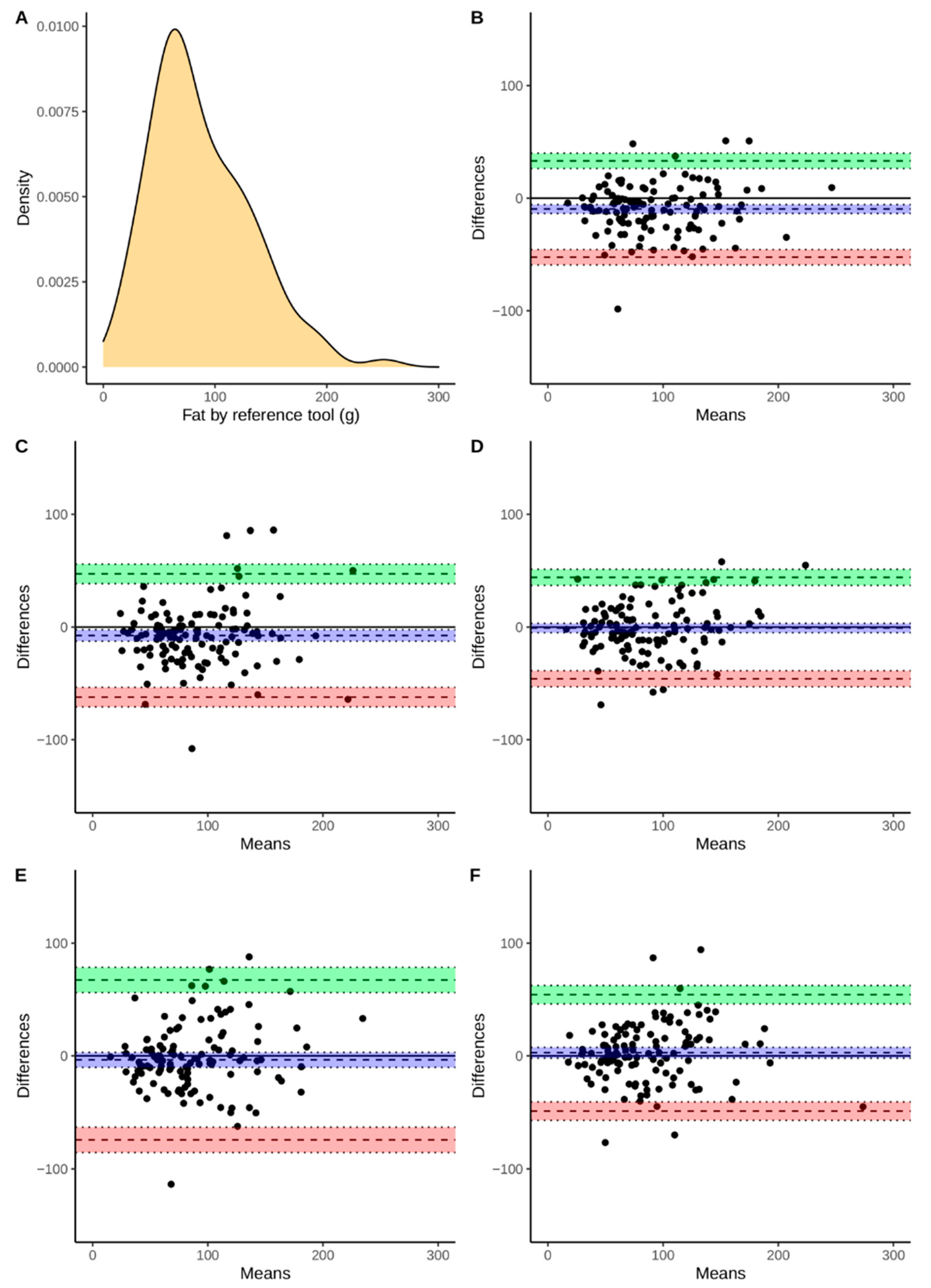
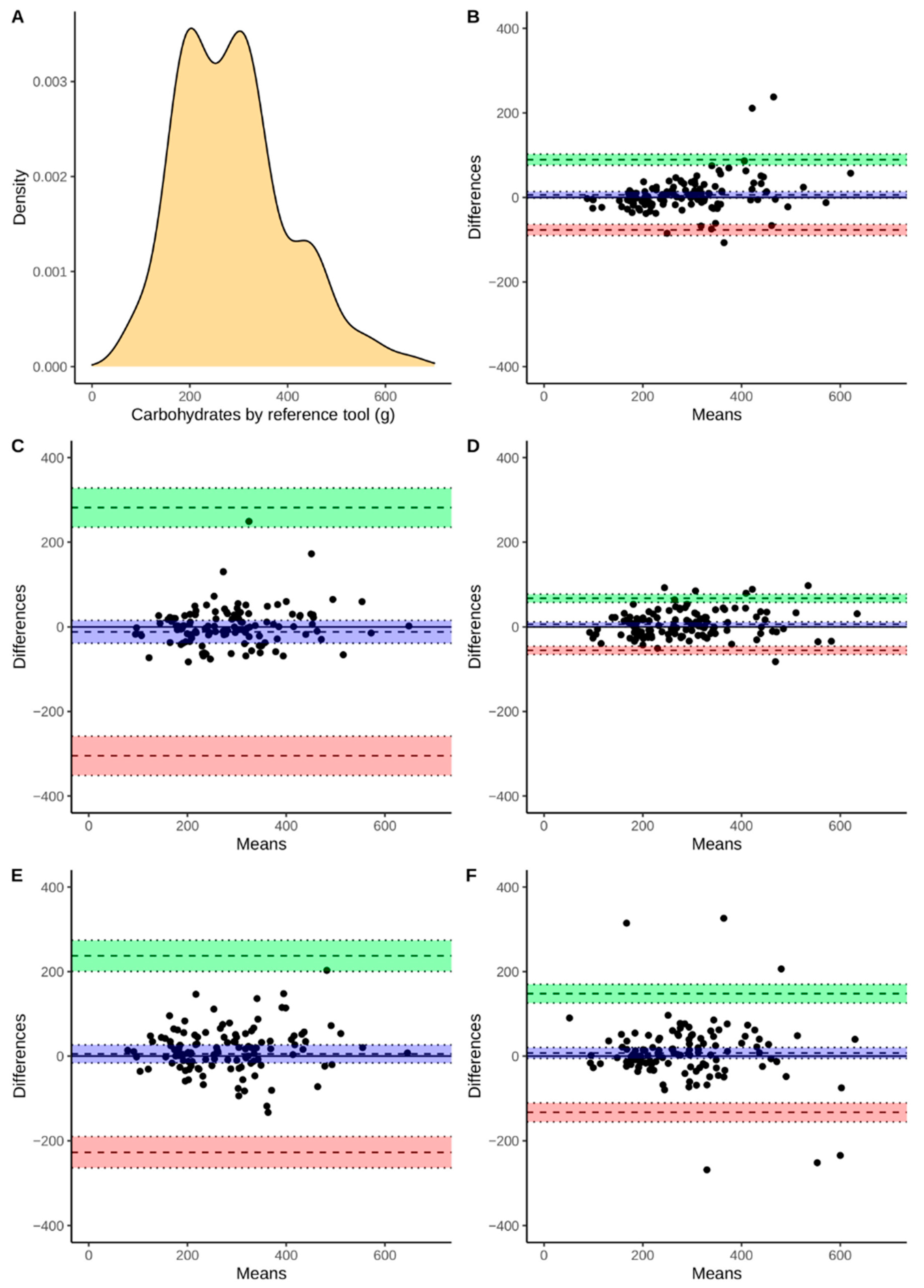
3.2. Comparison of Energy and Macronutrient Intake between Apps and Polish RM
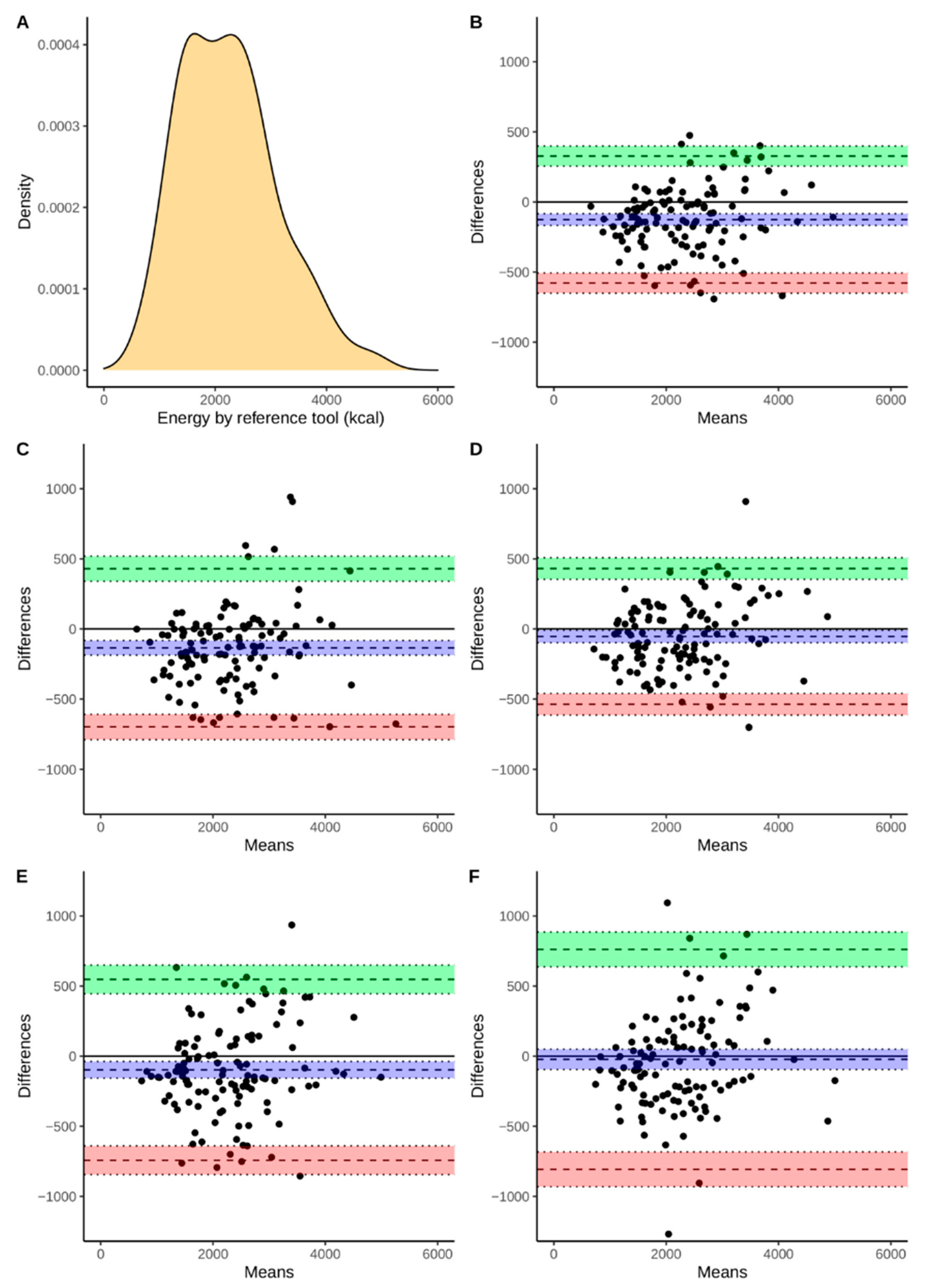
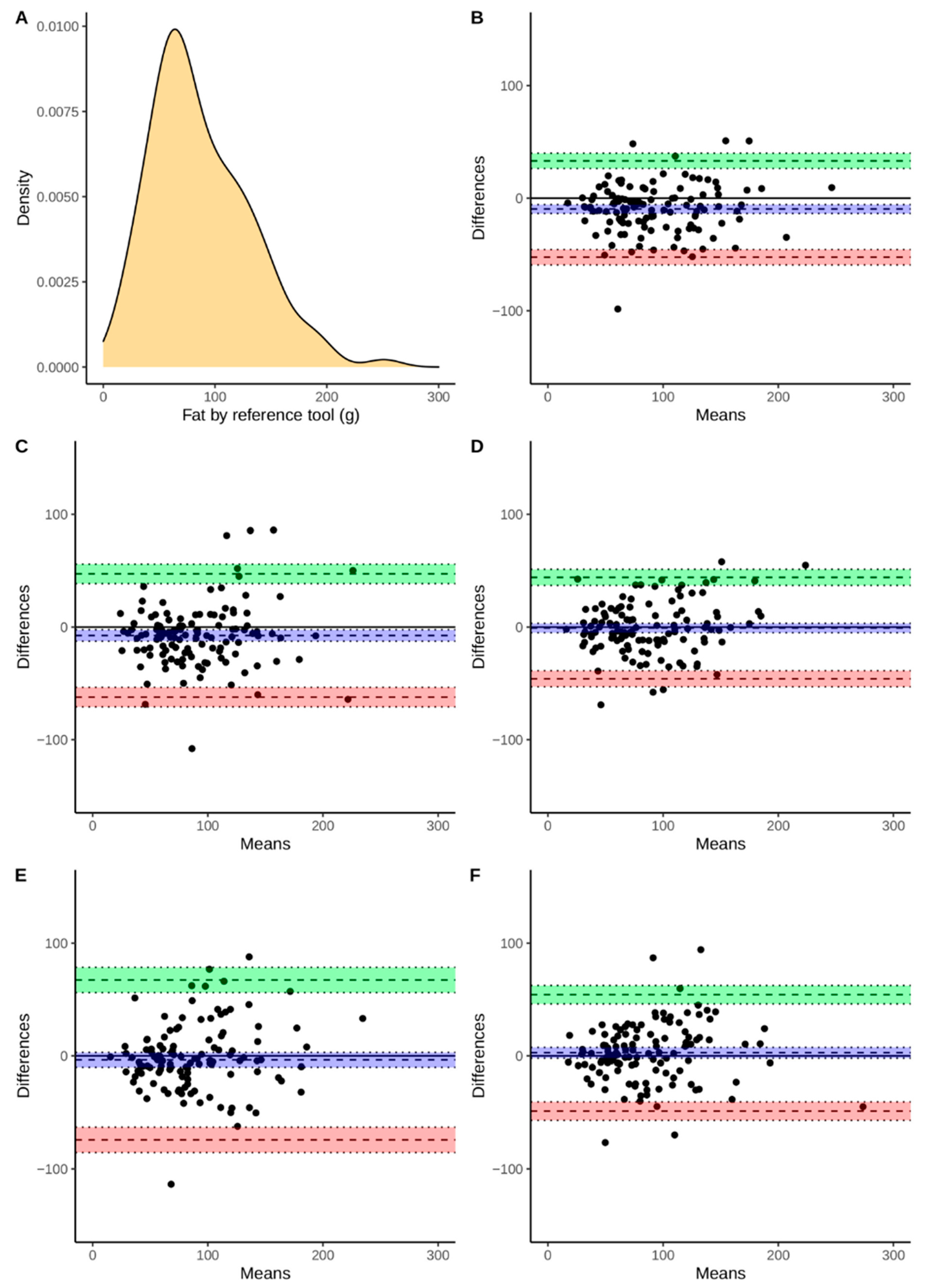
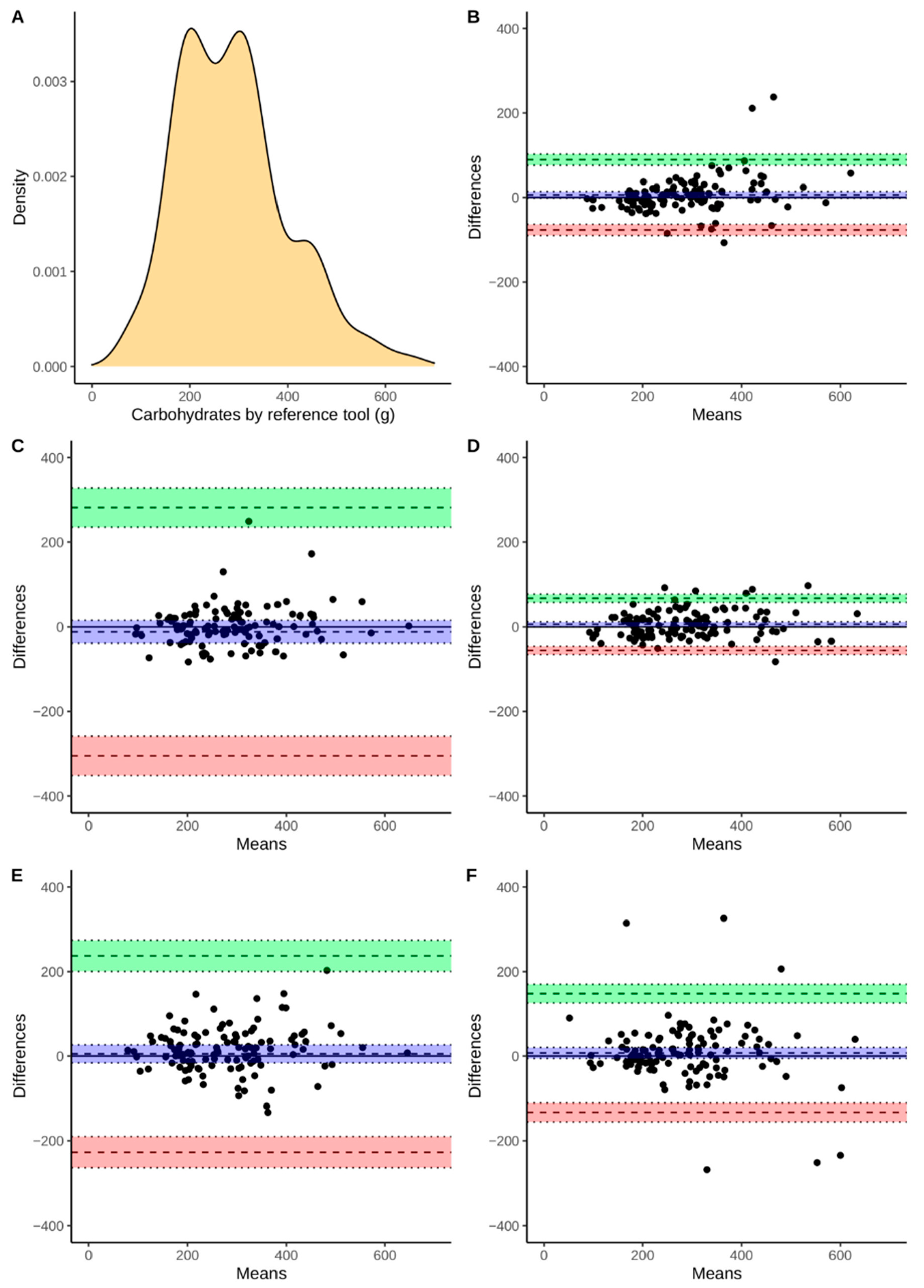
3.3. The Agreement between Selected Mobile Apps and RM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland. 2011. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 12 June 2021).
- Euro WHO. Available online: https://www.euro.who.int/en/health-topics/noncommunicable-diseases/ncd-background-information/noncommunicable-diseases-country-profiles-2014/ncd-country-profile-2014-poland (accessed on 12 June 2021).
- Prevention and Control of Noncommunicable Diseases: Guidelines for Primary Health Care in Low Resource Settings; Recommendations and Evidence; World Health Organization: Geneva, Switzerland, 2012.
- Simko, M.D.; Cowell, C.; Gilbride, J.A. Nutrition Assessment: A Comprehensive Guide for Planning Intervention, 2nd ed.; Aspen Publishers: Gaithersburg, MD, USA, 1995. [Google Scholar]
- Shriver, B.J.; Roman-Shriver, C.R.; Long, J.D. Technology-based methods of dietary assessment: Recent developments and considerations for clinical practice. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 548–551. [Google Scholar] [CrossRef]
- Cade, J.E. Measuring diet in the 21st century: Use of new technologies. Proc. Nutr. Soc. 2017, 76, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Samoggia, A.; Riedel, B. Assessment of nutrition-focused mobile apps’ influence on consumers’ healthy food behavior and nutrition knowledge. Food Res. Int. 2020, 128, 108766. [Google Scholar] [CrossRef] [PubMed]
- El-Gayar, O.; Timsina, P.; Nawar, N.; Eid, W. Mobile applications for diabetes self-management: Status and potential. J. Diabetes Sci. Technol. 2013, 7, 247–262. [Google Scholar] [CrossRef] [Green Version]
- Flores Mateo, G.; Granado-Font, E.; Ferré-Grau, C.; Montaña-Carreras, X. Mobile phone apps to promote weight loss and increase physical activity: A systematic review and meta-analysis. J. Med. Internet Res. 2015, 17, 253. [Google Scholar] [CrossRef] [Green Version]
- Pendergast, F.J.; Leech, R.M.; McNaughton, S.A. Novel online or mobile methods to assess eating patterns. Curr. Nutr. Rep. 2017, 6, 212–227. [Google Scholar] [CrossRef] [Green Version]
- Simpson, C.C.; Mazzeo, S.E. Calorie counting and fitness tracking technology: Associations with eating disorder symptomatology. Eat. Behav. 2017, 26, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C.A.; Fewell, L.; Brosof, L.C. MyFitnessPal calorie tracker usage in the eating disorders. Eat Behav. 2017, 27, 14–16. [Google Scholar] [CrossRef]
- Tosi, M.; Radice, D.; Carioni, G.; Vecchiati, T.; Fiori, F.; Parpinel, M.; Gnagnarella, P. Accuracy of applications to monitor food intake: Evaluation by comparison with 3-d food diary. Nutrition 2021, 84. [Google Scholar] [CrossRef] [PubMed]
- Williamson, C. The Different Uses of Food Composition Databases. EuroFIR 2006. Synthesis Report No 2. Available online: http://www.eurofir.org/wp-content/uploads/EuroFIR%20synthesis%20reports/Synthesis%20Report%202_The%20different%20uses%20of%20food%20composition%20databases.pdf (accessed on 7 June 2021).
- Elmadfa, I.; Meyer, A.L. Importance of food composition data to nutrition and public health. Eur. J. Clin. Nutr. 2010, 64, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Kunachowicz, H.; Nadolna, I.; Przygoda, B.; Iwanow, K. 3rd Edition Extended and Updated; National Food and Nutrition Institute: Warsaw, Poland, 2005. [Google Scholar]
- Carter, M.; Burley, V.; Nykjaer, C.; Cade, J. ‘My Meal Mate’ (MMM): Validation of the diet measures captured on a smartphone application to facilitate weight loss. Br. J. Nutr. 2013, 109, 539–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, F.; Tan, J. Automatic dietary assessment with mobile camera phones. Pervasive Mob. Comput. 2012, 8, 147–163. [Google Scholar] [CrossRef]
- Khazen, W.; Jeanne, J.F.; Demaretz, L.; Schäfer, F.; Fagherazzi, G. Rethinking the Use of Mobile Apps for Dietary Assessment in Medical Research. J. Med. Internet Res. 2020, 22, 15619. [Google Scholar] [CrossRef] [PubMed]
- Rhyner, D.; Loher, H.; Dehais, J.; Anthimopoulos, M.; Shevchik, S.; Botwey, R.H.; Duke, D.; Stettler, C.; Diem, P.; Mougiakakou, S. Carbohydrate Estimation by a Mobile Phone-Based System Versus Self-Estimations of Individuals with Type 1 Diabetes Mellitus: A Comparative Study. J. Med. Internet Res. 2016, 11, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pendergast, F.J.; Ridgers, N.D.; Worsley, A.; McNaughton, S.A. Evaluation of a smartphone food diary application using objectively measured energy expenditure. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 14. [Google Scholar] [CrossRef] [Green Version]
- Griffiths, C.; Harnack, L.; Pereira, M.A. Assessment of the accuracy of nutrient calculations of five popular nutrition tracking applications. Public Health Nutr. 2018, 21, 1495–1502. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, G.; Kim, J.; Lin, S.; Hua, J.; Seto, E. A focused review of smartphone diet-tracking apps: Usability, functionality, coherence with behavior change theory, and comparative validity of nutrient intake and energy estimates. JMIR mHealth uHealth 2019, 7, 1–16. [Google Scholar] [CrossRef]
- Chen, J.; Cade, J.E.; Allman-Farinelli, M. The most popular smartphone apps for weight loss: A quality assessment. JMIR mHealth uHealth 2015, 3, 104. [Google Scholar] [CrossRef]
- Rangan, A.M.; Connor, S.O.; Giannelli, V.; Yap, M.L.H.; Ming, L.; Hon, B.C.S.; Roy, R.; Chun, J.; Louie, Y.; Hebden, L.; et al. Electronic Dietary Intake Assessment (e-DIA): Comparison of a mobile phone digital entry app for dietary data collection with 24-hour dietary recalls. JMIR mHealth uHealth 2015, 3, 98. [Google Scholar] [CrossRef]
- Shinozaki, N.; Murakami, K. Evaluation of the Ability of Diet-Tracking Mobile Applications to Estimate Energy and Nutrient Intake in Japan. Nutrients 2020, 12, 3327. [Google Scholar] [CrossRef]
- Braz, V.N.; de Moraes Lopes, M.H.B. Evaluation of mobile applications related to nutrition. Public Health Nutr. 2019, 22, 1209–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szponar, L.; Wolnicka, K.; Rychlik, E. Album of Photographs of Food Products and Dishes; National Food and Nutrition Institute: Warsaw, Poland, 2011. [Google Scholar]
- Dietary Reference Intakes. Application in Dietary Planning; Institute of Medicine, National Academy Press: Washington, DC, USA, 2003.
- Murphy, S.P. Impact of new Dietary Reference Intakes on nutrient calculation programs. J. Food Compos. Anal. 2003, 16, 365–372. [Google Scholar] [CrossRef]
- Jarosz, M.; Rychlik, E.; Stoś, K.; Charzewska, J. Dietary Reference Values for the Polish Population and their Application; National Institute of Public Health: Warsaw, Poland, 2020. [Google Scholar]
- Fallaize, R.; Zenun Franco, R.; Pasang, J.; Hwang, F.; Lovegrove, J.A. Popular Nutrition-Related Mobile Apps: An Agreement Assessment against a UK Reference Method. JMIR Mhealth Uhealth 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smethers, A.D.; Rolls, B.J. Dietary Management of Obesity: Cornerstones of Healthy Eating Patterns. Med. Clin. N. Am. 2018, 102, 107–124. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Berkman, W.; Bardouh, M.; Ng, C.Y.; Allman-Farinelli, M. The use of a food logging app in the naturalistic setting fails to provide accurate measurements of nutrients and poses usability challenges. Nutrition 2018, 25, 208–216. [Google Scholar] [CrossRef]
- Maringer, M.; Wisse-Voorwinden, N.; Van’T Veer, P.; Geelen, A. Food identification by barcode scanning in the Netherlands: A quality assessment of labelled food product databases underlying popular nutrition applications. Public Health Nutr. 2019, 22, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Merchant, A.T.; Dehghan, M. Food composition database development for between country comparisons. Nutr. J. 2006, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Lieffers, J.; Bauman, A.; Hanning, R.; Allman-Farinelli, M. Designing Health Apps to Support Dietetic Professional Practice and Their Patients: Qualitative Results from an International Survey. JMIR Mhealth Uhealth 2017, 5, 40. [Google Scholar] [CrossRef]
- Nikolaou, C.K.; Lean, M.E. Mobile applications for obesity and weight management: Current market characteristics. Int. J. Obes. 2017, 41, 200–202. [Google Scholar] [CrossRef] [Green Version]
- Pagoto, S.; Schneider, K.; Jojic, M.; DeBiasse, M.; Mann, D. Evidence-based strategies in weight-loss mobile apps. Am. J. Prev. Med. 2013, 45, 576–582. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xue, H.; Huang, Y.; Huang, L.; Zhang, D. A Systematic Review of Application and Effectiveness of mHealth Interventions for Obesity and Diabetes Treatment and Self-Management. Adv. Nutr. 2017, 8, 449–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghelani, D.P.; Moran, L.J.; Johnson, C.; Mousa, A.; Naderpoor, N. Mobile Apps for Weight Management: A Review of the Latest Evidence to Inform Practice. Front. Endocrinol. 2020, 11, 412. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Subjects, n = 120 | Men, n = 60 | Women, n = 60 | |
|---|---|---|---|
| Age (years) | 41 (28.8–54) | 40 (29–53) | 44 (28–54) |
| BMI2 kg/m2 | 24.7 (22.4–27.7) | 25 (23–28) | 24 (22–28) |
| BMI < 18.5 kg/m2 | 1 (0.8%) | 0 (0%) | 1 (1.7%) |
| BMI ≥ 18.5 and <20 kg/m2 | 63 (52.5%) | 29 (48.3%) | 34 (56.7%) |
| BMI ≥ 20 and <25 kg/m2 | 40 (33.3%) | 24 (40%) | 16 (26.7%) |
| BMI ≥ 30 kg/m2 | 16 (13.3%) | 7 (11.7%) | 9 (15%) |
| Feature/App | FatSecret | YAZIO | Fitatu | MyFitnessPal | Dine4Fit |
|---|---|---|---|---|---|
| Dietary features | |||||
| The source of FCD 1 | USDA SR 2 Australian FCD 1 Crowd-sourced | USDA SR 2 BLS 3 Crowd-sourced | USDA SR 2 Polish FCD 1 Crowd-sourced | USDA SR 2 Crowd-sourced | Czech FCD 1 |
| Number of food items | 34,000 | No data | >1,600,000 | >300,000,000 | 934 |
| Barcode scanner | ✓ | ✓ | ✓ | ✓ | ✓ |
| Branded food products | ✓ | ✓ | ✓ | ✓ | ✓ |
| Serving size | ✓ | ✓ | ✓ | ✓ | ✓ |
| Favorite foods | ✓ | ✓ | ✓ | ✓ | ✓ |
| Uploading own data 4 | ✓ | ✓ | ✓ | ✓ | ✓ |
| Water consumption | ✓ 5 | ✓ | - | ✓ | ✓ |
| Food images | ✓ 5 | ✓ | ✓ | - | ✓ |
| Adding own dishes | ✓ 5 | ✓ | ✓ | ✓ | ✓ |
| Setting dietary goals | ✓ | ✓ | ✓ | ✓5 | ✓ |
| Users’ data | |||||
| Gender | ✓ | ✓ | ✓ | ✓ | ✓ |
| Weight | ✓ | ✓ | ✓ | ✓ | ✓ |
| Height | ✓ | ✓ | ✓ | ✓ | ✓ |
| Circumferences | - | - | ✓ | ✓ | - |
| Birth date | ✓ | ✓ | ✓ | ✓ | ✓ |
| Physical activity | |||||
| Type of physical activity | ✓ | ✓ | ✓ | ✓ | ✓ |
| Setting exercise goal | - | ✓ | ✓ | ✓ | - |
| Average activity level | ✓ | ✓ | - | ✓ | - |
| Other features | |||||
| Daily notes | - | ✓ | - | - | ✓ |
| Health status | - | - | - | - | - |
| Personal reminders | - | - | - | ✓ | ✓ |
| Community forums | ✓ | ✓ | - | ✓ | - |
| Keeping track of progress | - | ✓ | ✓ | ✓ | - |
| Feature/App | FatSecret | YAZIO | Fitatu | MyFitnessPal | Dine4Fit |
|---|---|---|---|---|---|
| Automated nutritional assessment | |||||
| Total energy intake | ✓ | ✓ | ✓ | ✓ | ✓ |
| Energy intake by meal | ✓ | ✓ | ✓ | ✓ | ✓ |
| Macronutrient intake | ✓ | ✓ | ✓ | ✓ | ✓ |
| Micronutrient intake | ✓ 1 | ✓ | ✓ | ✓ 2 | ✓ 3 |
| Vitamins intake | - | ✓ | ✓ | ✓ 4 | - |
| Recommended water consumption | - | ✓ | ✓ 5 | - | ✓ |
| Diet plan | ✓ 5 | ✓ | ✓ 5 | - | - |
| Shopping list | - | - | ✓ 5 | - | - |
| CVS file with nutrition data | - | - | ✓ 5 | ✓5 | - |
| Other features | |||||
| Weight changes | ✓ | ✓ | ✓ | ✓ | ✓ |
| BMI 1 calculation | - | - | - | - | ✓ |
| Energy expenditure | ✓ | ✓ | ✓ 5 | ✓ | ✓ |
| Private social media | ✓ | ✓ | - | ✓ | - |
| Sharing with professionals | ✓ | - | - | - | - |
| Variables | Median (IQR) 1 | p-Value 3 | |
|---|---|---|---|
| RM 2 | Energy (kcal) | 2193 (1504–2767) | - |
| Protein (g) | 80 (55–100) | - | |
| Fat (g) | 76 (55–117) | - | |
| Carbohydrates (g) | 281 (198–339) | - | |
| FatSecret | Energy (kcal) | 2292 (1695–2865) | <0.001 |
| Protein (g) | 89 (57–108) | <0.001 | |
| Fat (g) | 89 (66–130) | <0.001 | |
| Carbohydrates (g) | 271 (208–335) | 0.972 | |
| YAZIO | Energy (kcal) | 2320 (1703–2825) | <0.001 |
| Protein (g) | 88 (56–110) | <0.001 | |
| Fat (g) | 92 (66–117) | <0.001 | |
| Carbohydrates (g) | 278 (208–356) | 1.0 | |
| Fitatu | Energy (kcal) | 2310 (1638–2798) | 0.059 |
| Protein (g) | 84 (57–108) | <0.001 | |
| Fat (g) | 81 (58–117) | 1.0 | |
| Carbohydrates (g) | 264 (202–338) | 0.587 | |
| MyFitnessPal | Energy (kcal) | 2328 (1640–2812) | 0.003 |
| Protein (g) | 86 (56–112) | <0.001 | |
| Fat (g) | 88 (59–107) | 0.753 | |
| Carbohydrates (g) | 263 (197–340) | 0.018 | |
| Dine4Fit | Energy (kcal) | 2221 (1658–2744) | 0.549 |
| Protein (g) | 81 (52–98) | 1.0 | |
| Fat (g) | 80 (55–108) | 1.0 | |
| Carbohydrates (g) | 260 (202–335) | 0.578 |
| FatSecret | YAZIO | Fitatu | MyFitnessPal | Dine4Fit | |
|---|---|---|---|---|---|
| Variables | |||||
| Energy | 0.96 | 0.95 | 0.96 | 0.92 | 0.86 |
| Protein | 0.90 | 0.83 | 0.90 | 0.86 | 0.82 |
| Fat | 0.86 | 0.81 | 0.86 | 0.74 | 0.80 |
| Carbohydrates | 0.95 | 0.85 | 0.95 | 0.86 | 0.85 |
| FatSecret | YAZIO | Fitatu | MyFitnessPal | Dine4Fit | ||
|---|---|---|---|---|---|---|
| Energy (kcal) | −126 | −135 | −53 | −97 | −23 | |
| (−167 to −84) | (−187 to −83) | (−98 to −9) | (−157 to −38) | (−95 to 50) | ||
| 327 | 429 | 431 | 548 | 762 | ||
| (256 to 399) | (340 to 519) | (354 to 507) | (446 to 649) | (638 to 886) | ||
| −579 | −699 | −538 | −742 | −807 | ||
| (−650 to −507) | (−788 to −610) | (−614 to −461) | (−844 to −640) | (−931 to −683) | ||
| Protein (g) | −7 | −21 | −6 | −11 | −0.7 | |
| (−9 to −4) | (−38 to −3) | (−9 to −3) | (−21 to −2) | (−5 to 4) | ||
| 25 | 172 | 26 | 92 | 51 | ||
| (20 to 30) | (141 to 202) | (21 to 31) | (76 to 109) | (43 to 59) | ||
| −38 | −213 | −37 | −115 | −52 | ||
| (−43 to −33) | (−243 to −182) | (−42 to −32) | (−131 to −99) | (−60 to −44) | ||
| Fat (g) | −10 | −7 | −0.9 | −4 | 3 | |
| (−14 to −6) | (−13 to −2) | (−5 to 3) | (−10 to 3) | (−2 to 7) | ||
| 33 | 47 | 44 | 67 | 54 | ||
| (26 to 40) | (39 to 56) | (37 to 51) | (56 to 78) | (46 to 62) | ||
| −52 | −62 | −46 | −74 | −49 | ||
| (−59 to −46) | (−71 to −54) | (−53 to −39) | (−85 to −63) | (−57 to −41) | ||
| Carbohydrates (g) | 6 | −12 | 6 | 5 | 7 | |
| (−1 to 14) | (−39 to 15) | (0.4 to 12) | (−16 to 27) | (−6 to 20) | ||
| 282 | 68 | 237 | 148 | |||
| 89 | (235 to 328) | (58 to 77) | (201 to 274) | (126 to 170) | ||
| (76 to 102) | ||||||
| −305 | −56 | −227 | −133 | |||
| −77 | (−351 to −258) | (−65 to −46) | (−264 to −190) | (−155 to −111) | ||
| (−90 to −64) | ||||||
| FatSecret | YAZIO | Fitatu | MyFitnessPal | Dine4Fit | |
|---|---|---|---|---|---|
| Energy | 73 (60.8%) | 67 (55.8%) | 77 (64.2%) | 58 (48.3%) | 60 (50%) |
| Protein | 58 (48.3%) | 41 (34.2%) | 52 (43.3%) | 40 (33.3%) | 49 (40.8%) |
| Fat | 40 (33.3%) | 39 (32.5%) | 36 (30%) | 35 (29.2%) | 31 (25.8%) |
| Carbohydrates | 81 (67.5%) | 61 (50.8%) | 72 (60%) | 53 (44.2%) | 61 (50.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bzikowska-Jura, A.; Sobieraj, P.; Raciborski, F. Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study. Nutrients 2021, 13, 2868. https://doi.org/10.3390/nu13082868
Bzikowska-Jura A, Sobieraj P, Raciborski F. Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study. Nutrients. 2021; 13(8):2868. https://doi.org/10.3390/nu13082868
Chicago/Turabian StyleBzikowska-Jura, Agnieszka, Piotr Sobieraj, and Filip Raciborski. 2021. "Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study" Nutrients 13, no. 8: 2868. https://doi.org/10.3390/nu13082868
APA StyleBzikowska-Jura, A., Sobieraj, P., & Raciborski, F. (2021). Low Comparability of Nutrition-Related Mobile Apps against the Polish Reference Method—A Validity Study. Nutrients, 13(8), 2868. https://doi.org/10.3390/nu13082868