
Development of a Portfolio Diet Score and Its Concurrent and Predictive Validity Assessed by a Food Frequency Questionnaire

 , and
, and 
Abstract
1. Introduction
2. Methods
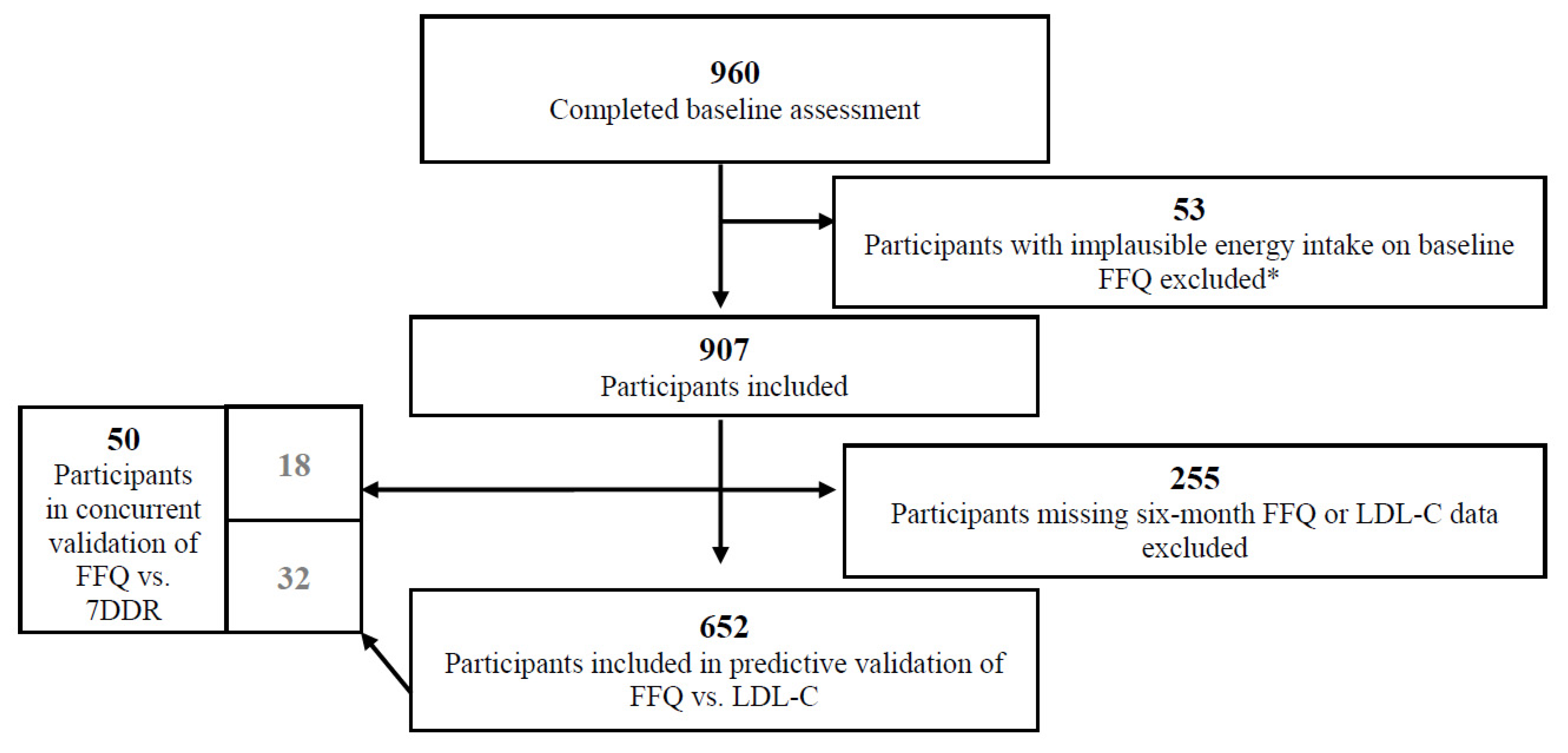
2.1. Study Population
2.2. Study Design
2.3. Nutrition Intervention
2.4. Dietary Assessment
2.4.1. Food Frequency Questionnaire
2.4.2. Diet Records
2.5. Development of the Portfolio Diet Score
2.5.1. Using Dietary Recommendations from the RCTs or Population-Specific Cut-Offs
2.5.2. Using a Nutrient or Food-Based Score
2.5.3. Choice of Quantiles
2.5.4. Weight of Each Diet Component
2.6. Calculating the PDS
2.7. Phytosterol Database
2.8. LDL-C Assessment
2.9. Covariate Assessment
2.10. Statistical Analysis
3. Results
3.1. Development of the PDS
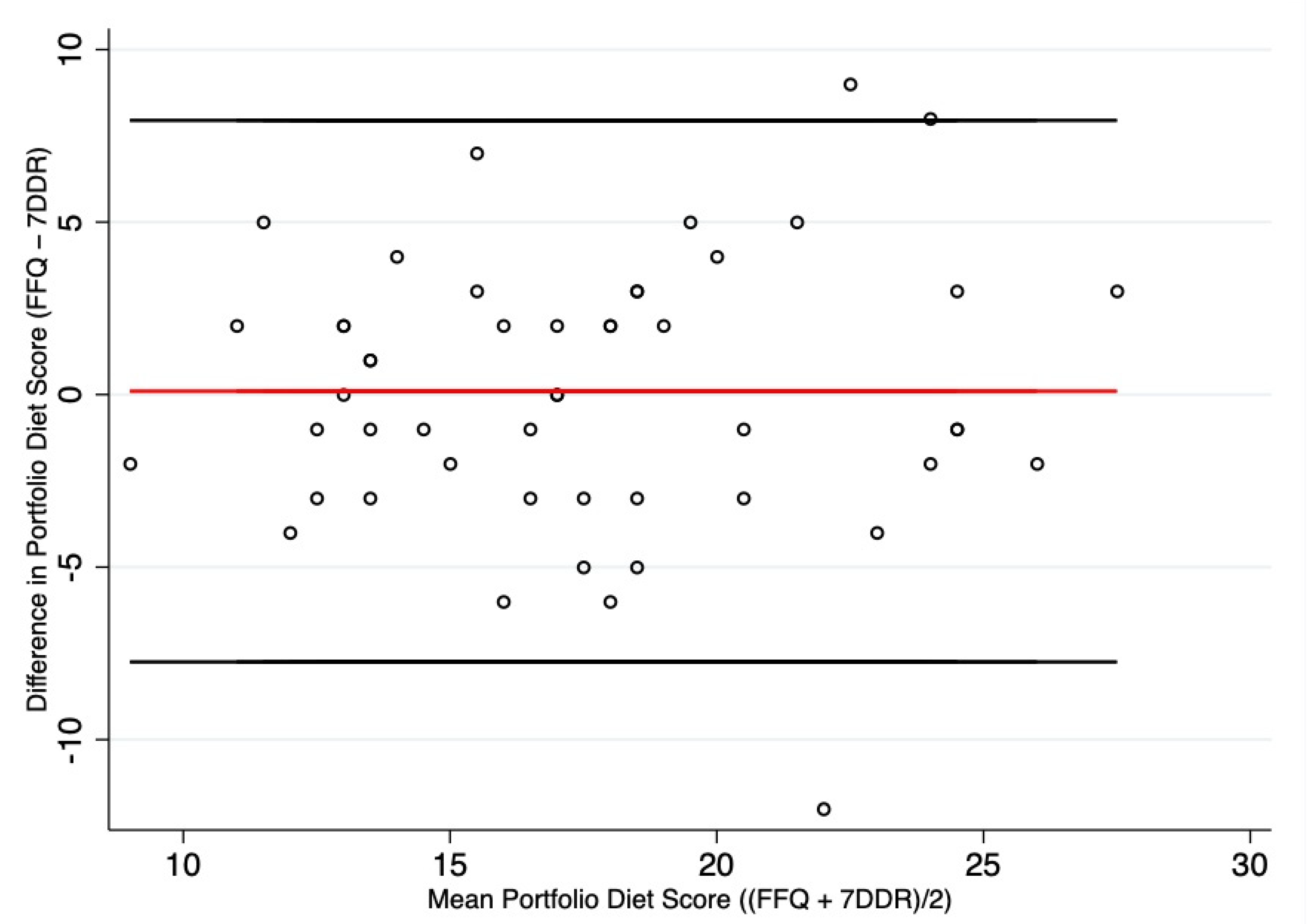
3.2. Validation of PDS by FFQ
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jenkins, D.J.; Kendall, C.W.; Faulkner, D.; Vidgen, E.; Trautwein, E.A.; Parker, T.L.; Marchie, A.; Koumbridis, G.; Lapsley, K.G.; Josse, R.G.; et al. A dietary portfolio approach to cholesterol reduction: Combined effects of plant sterols, vegetable proteins, and viscous fibers in hypercholesterolemia. Metabolism 2002, 51, 1596–1604. [Google Scholar] [CrossRef]
- Health Canada, Food Directorate Health Products and Food Branch. Plant Sterols and Blood Cholesterol Lowering. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/foodlabelling/health-claims/assessments/plant-sterols-blood-cholesterol-loweringnutrition-health-claims-food-labelling.html (accessed on 3 February 2021).
- Health Canada, Food Directorate Health Products and Food Branch. Oat Products and Blood Cholesterol Lowering. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-labelling/health-claims/assessments/products-blood-cholesterol-lowering-summary-assessment-health-claim-about-products-blood-cholesterol-lowering.html (accessed on 3 February 2021).
- Health Canada, Food Directorate Health Products and Food Branch, H.C. Summary of Health Canada’s Assessment of a Health Claim About Soy Protein and Cholesterol Lowering. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-labelling/health-claims/assessments/summary-assessment-health-claim-about-protein-cholesterol-lowering.html (accessed on 3 February 2021).
- Health Canada, Food Directorate Health Products and Food Branch. List of Dietary Fibres Reviewed and Accepted by Health Canada’s Food Directorate. Available online: https://www.canada.ca/en/healthcanada/services/publications/food-nutrition/list-reviewed-accepted-dietary-fibres.html (accessed on 3 February 2021).
- U.S Food & Drug Administration. Qualified Health Claims: Letter of Enforcement Discretion—Nuts and Coronary Heart Disease. Available online: http://wayback.archive-it.org/7993/20171114183724/https://www.fda.gov/Food/IngredientsPackagingLabeling/LabelingNutrition/ucm072926.htm (accessed on 3 February 2021).
- U.S. Food & Drug Administration. Health Claims: Soy Protein and Risk of Coronary Heart Disease. Available online: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=101.82 (accessed on 3 February 2021).
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on the Substantiation of a Health Claim Related to oat Betaglucan and Lowering Blood Cholesterol and Reduced Risk of (Coronary) Heart Disease Pursuant to Article 14 of Regulation (EC) No 1924/2006. EFSA J. 2010, 8, 1885. Available online: www.efsa.europa.eu/efsajournal.htm (accessed on 3 February 2021).
- EFSA Panel on Dietetic Products, Nutrition and Allergies. Scientific Opinion on the Substantiation of a Health Claimrelated to 3 g/day Plant Sterols/Stanols and Lowering Blood LDL-Cholesterol and Reduced Risk of (Coronary) Heart Disease Pursuant to Article 19 of Regulation (EC) No 1924/2006. EFSA J. 2012, 10, 2693. Available online: https://www.efsa.europa.eu/en/publications (accessed on 3 February 2021). [CrossRef]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.A.; Kendall, C.W.C.; Marchie, A.; Faulkner, D.; Vidgen, E.; Lapsley, K.G.; Trautwein, E.A.; Parker, T.L.; Josse, R.G.; Leiter, L.A.; et al. The effect of combining plant sterols, soy protein, viscous fibers, and almonds in treating hypercholesterolemia. Metabolism 2003, 52, 1478–1483. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Marchie, A.; Faulkner, D.A.; Wong, J.M.W.; de Souza, R.; Emam, A.; Parker, T.L.; Vidgen, E.; Lapsley, K.G.; et al. Effects of a Dietary Portfolio of Cholesterol-Lowering Foods vs Lovastatin on Serum Lipids and C-Reactive Protein. JAMA 2003, 290, 502–510. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Faulkner, D.A.; Nguyen, T.; Kemp, T.; Marchie, A.; Wong, J.M.W.; de Souza, R.; Emam, A.; Vidgen, E.; et al. Assessment of the longer-term effects of a dietary portfolio of cholesterol-lowering foods in hypercholesterolemia. Am. J. Clin. Nutr. 2006, 83, 582–591. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Jones, P.; Lamarche, B.; Kendall, C.W.C.; Faulkner, D.; Cermakova, L.; Gigleux, I.; Ramprasath, V.; de Souza, R.; Ireland, C.; et al. Effect of a Dietary Portfolio of Cholesterol-Lowering Foods Given at 2 Levels of Intensity of Dietary Advice on Serum Lipids in Hyperlipidemia. JAMA 2011, 306, 831–839. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Chiavaroli, L.; Wong, J.M.; Kendall, C.; Lewis, G.F.; Vidgen, E.; Connelly, P.W.; Leiter, L.A.; Josse, R.G.; Lamarche, B. Adding monounsaturated fatty acids to a dietary portfolio of cholesterol-lowering foods in hypercholesterolemia. Can. Med. Assoc. J. 2010, 182, 1961–1967. [Google Scholar] [CrossRef]
- Chiavaroli, L.; Nishi, S.K.; Khan, T.A.; Braunstein, C.R.; Glenn, A.J.; Mejia, S.B.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Jenkins, D.J.; et al. Portfolio Dietary Pattern and Cardiovascular Disease: A Systematic Review and Meta-analysis of Controlled Trials. Prog. Cardiovasc. Dis. 2018, 61, 43–53. [Google Scholar] [CrossRef]
- Glenn, A.J.; Hernández-Alonso, P.; Kendall, C.W.; Martínez-González, M.Á.; Corella, D.; Fitó, M.; Martínez, J.; Alonso-Gómez, Á.M.; Wärnberg, J.; Vioque, J.; et al. Longitudinal changes in adherence to the portfolio and DASH dietary patterns and cardiometabolic risk factors in the PREDIMED-Plus study. Clin. Nutr. 2021, 40, 2825–2836. [Google Scholar] [CrossRef]
- Glenn, A.J.; Lo, K.; Jenkins, D.J.A.; Boucher, B.A.; Hanley, A.J.; Kendall, C.W.C.; Manson, J.E.; Vitolins, M.Z.; Snetselaar, L.G.; Liu, S.; et al. Relationship Between a Plant-Based Dietary Portfolio and Risk of Cardiovascular Disease: Findings from the Women’s Health Initiative Prospective Cohort Study. J. Am. Heart Assoc. 2021, e021515. [Google Scholar] [CrossRef]
- Kirkpatrick, S.I.; Vanderlee, L.; Raffoul, A.; Stapleton, J.; Csizmadi, I.; Boucher, B.; Massarelli, I.; Rondeau, I.; Robson, P.J. Self-Report Dietary Assessment Tools Used in Canadian Research: A Scoping Review. Adv. Nutr. 2017, 8, 276–289. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Boucher, B.; Ashbury, F.D.; Sloan, M.; Brown, P.; El-Sohemy, A.; Hanley, A.J.; Willett, W.; Paquette, M.; de Souza, R.J.; et al. Effect of Current Dietary Recommendations on Weight Loss and Cardiovascular Risk Factors. J. Am. Coll. Cardiol. 2017, 69, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. History of Canada’s Food Guides from 1942 to 2007. Available online: https://www.canada.ca/en/health-canada/services/canada-food-guide/about/history-food-guide.html (accessed on 12 April 2021).
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and Validity of a Semiquantitative Food Frequency Questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Holmes, M.D.; Powell, I.J.; Campos, H.; Stampfer, M.J.; Giovannucci, E.L.; Willett, W.C. Validation of a food frequency questionnaire measurement of selected nutrients using biological markers in African-American men. Eur. J. Clin. Nutr. 2007, 61, 1328–1336. [Google Scholar] [CrossRef][Green Version]
- Fung, T.T.; Chiuve, S.E.; McCullough, M.L.; Rexrode, K.M.; Logroscino, G.; Hu, F.B. Adherence to a DASH-Style Diet and Risk of Coronary Heart Disease and Stroke in Women. Arch. Intern. Med. 2008, 168, 713–720. [Google Scholar] [CrossRef]
- Arvaniti, F.; Panagiotakos, D.B. Healthy Indexes in Public Health Practice and Research: A Review. Crit. Rev. Food Sci. Nutr. 2008, 48, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.E.; Cross, A.J.; Subar, A.F.; Krebs-Smith, S.M.; Park, Y.; Powell-Wiley, T.; Hollenbeck, A.; Reedy, J. Comparison of 4 established DASH diet indexes: Examining associations of index scores and colorectal cancer. Am. J. Clin. Nutr. 2013, 98, 794–803. [Google Scholar] [CrossRef]
- Anderson, T.J.; Grégoire, J.; Pearson, G.; Barry, A.; Couture, P.; Dawes, M.; Francis, G.A.; Genest, J.; Grover, S.; Gupta, M.; et al. 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can. J. Cardiol. 2016, 32, 1263–1282. [Google Scholar] [CrossRef]
- Sievenpiper, J.L.; Chan, C.B.; Dworatzek, P.D.; Freeze, C.; Williams, S.L. Nutrition Therapy. Can. J. Diabetes 2018, 42, S64–S79. [Google Scholar] [CrossRef]
- USDA; USDHHS. Dietary Guidelines for Americans, 2020–2025, 9th ed. Available online: https://www.dietaryguidelines.gov (accessed on 3 March 2021).
- Government of Canada. Canada’s Food Guide. Available online: https://food-guide.canada.ca/en/ (accessed on 12 April 2021).
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Mattei, J.; Fung, T.T.; Li, Y.; Pan, A.; Willett, W.C.; Rimm, E.B.; Hu, F.B. Changes in Diet Quality Scores and Risk of Cardiovascular Disease Among US Men and Women. Circulation 2015, 132, 2212–2219. [Google Scholar] [CrossRef] [PubMed]
- Galbete, C.; Kröger, J.; Jannasch, F.; Iqbal, K.; Schwingshackl, L.; Schwedhelm, C.; Weikert, C.; Boeing, H.; Schulze, M.B. Nordic diet, Mediterranean diet, and the risk of chronic diseases: The EPIC-Potsdam study. BMC Med. 2018, 16, 1–13. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Spiegelman, D.; Chiuve, S.; Manson, J.E.; Willett, W.; Rexrode, K.M.; Rimm, E.B.; Hu, F.B. Healthful and Unhealthful Plant-Based Diets and the Risk of Coronary Heart Disease in U.S. Adults. J. Am. Coll. Cardiol. 2017, 70, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Panagiotakos, D. The diagnostic accuracy of a composite index increases as the number of partitions of the components increases and when specific weights are assigned to each component. J. Appl. Stat. 2010, 37, 537–554. [Google Scholar] [CrossRef]
- D’Alessandro, A.; De Pergola, G. Mediterranean Diet and Cardiovascular Disease: A Critical Evaluation of A Priori Dietary Indexes. Nutrients 2015, 7, 7863–7888. [Google Scholar] [CrossRef]
- Ocké, M.C. Evaluation of methodologies for assessing the overall diet: Dietary quality scores and dietary pattern analysis. Proc. Nutr. Soc. 2013, 72, 191–199. [Google Scholar] [CrossRef]
- Mejia, S.B.; Messina, M.; Li, S.S.; Viguiliouk, E.; Chiavaroli, L.; Khan, T.A.; Srichaikul, K.; Mirrahimi, A.; Sievenpiper, J.L.; Kris-Etherton, P.; et al. A Meta-Analysis of 46 Studies Identified by the FDA Demonstrates that Soy Protein Decreases Circulating LDL and Total Cholesterol Concentrations in Adults. J. Nutr. 2019, 149, 968–981. [Google Scholar] [CrossRef]
- Ha, V.; Sievenpiper, J.L.; de Souza, R.; Jayalath, V.H.; Mirrahimi, A.; Agarwal, A.; Chiavaroli, L.; Mejia, S.B.; Sacks, F.M.; Di Buono, M.; et al. Effect of dietary pulse intake on established therapeutic lipid targets for cardiovascular risk reduction: A systematic review and meta-analysis of randomized controlled trials. Can. Med. Assoc. J. 2014, 186, E252–E262. [Google Scholar] [CrossRef]
- Jovanovski, E.; Yashpal, S.; Komishon, A.; Zurbau, A.; Mejia, S.B.; Ho, H.V.T.; Li, D.; Sievenpiper, J.; Duvnjak, L.; Vuksan, V. Effect of psyllium (Plantago ovata) fiber on LDL cholesterol and alternative lipid targets, non-HDL cholesterol and apolipoprotein B: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2018, 108, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.V.T.; Sievenpiper, J.L.; Zurbau, A.; Mejia, S.B.; Jovanovski, E.; Au-Yeung, F.; Jenkins, A.L.; Vuksan, V. The effect of oatβ-glucan on LDL-cholesterol, non-HDL-cholesterol and apoB for CVD risk reduction: A systematic review and meta-analysis of randomised-controlled trials. Br. J. Nutr. 2016, 116, 1369–1382. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.V.T.; Sievenpiper, J.L.; Zurbau, A.; Mejia, S.B.; Jovanovski, E.; Au-Yeung, F.; Jenkins, A.L.; Vuksan, V. Erratum: A systematic review and meta-analysis of randomized controlled trials of the effect of barley β-glucan on LDL-C, non-HDL-C and apoB for cardiovascular disease risk reductioni-iv. Eur. J. Clin. Nutr. 2016, 70, 1340. [Google Scholar] [CrossRef]
- Sabaté, J.; Oda, K.; Ros, E. Nut Consumption and Blood Lipid Levels. Arch. Intern. Med. 2010, 170, 821–827. [Google Scholar] [CrossRef]
- National Institute of Health and Welfare. FINELI—The National Food Composition Database. Available online: https://thl.fi/en/web/lifestyles-and-nutrition/nutrition/fineli-the-national-food-composition-database (accessed on 17 April 2021).
- Ras, R.T.; van der Schouw, Y.; Trautwein, E.A.; Sioen, I.; Dalmeijer, G.W.; Zock, P.; Beulens, J.W.J. Intake of phytosterols from natural sources and risk of cardiovascular disease in the European Prospective Investigation into Cancer and Nutrition-the Netherlands (EPIC-NL) population. Eur. J. Prev. Cardiol. 2015, 22, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- USDA. U.S. Department of Agriculture. Food Data Central. Food Composition Table. Available online: https://fdc.nal.usda.gov/ (accessed on 17 April 2021).
- Jiménez-Escrig, A.; Santos-Hidalgo, A.B.; Calixto, F.D.S. Common Sources and Estimated Intake of Plant Sterols in the Spanish Diet. J. Agric. Food Chem. 2006, 54, 3462–3471. [Google Scholar] [CrossRef]
- Klingberg, S.; Andersson, H.; Mulligan, A.; Bhaniani, A.; Welch, A.; Bingham, S.; Khaw, K.-T.; Ellegård, L.; Andersson, S. Food sources of plant sterols in the EPIC Norfolk population. Eur. J. Clin. Nutr. 2007, 62, 695–703. [Google Scholar] [CrossRef]
- Phillips, K.M.; Ruggio, A.D.M.; Ashraf-Khorassani, M. Phytosterol Composition of Nuts and Seeds Commonly Consumed in the United States. J. Agric. Food Chem. 2005, 53, 9436–9445. [Google Scholar] [CrossRef]
- Normen, L.E.; Johnsson, M. A phytosterol database: Fatty foods consumed in Sweden and the Netherlands. J. Food Comp. Anal. 2007, 20, 193–201. [Google Scholar] [CrossRef]
- Normen, L.B.; Johnsson, M. The phytosterol content of some cereal foods commonly consumed in Sweden and the Netherlands. J. Food Comp. Anal. 2002, 15, 693–704. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, Without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Piedmont, R.L. Inter-item Correlations. In Encyclopedia of Quality of Life and Well-Being Research; Springer International Publishing: Berlin/Heidelberg, Germany, 2014; pp. 3303–3304. [Google Scholar]
- Serra-Majem, L.; Andersen, L.F.; Henríque-Sánchez, P.; Doreste-Alonso, J.; Villegas, A.S.; Ortiz-Andrellucchi, A.; Negri, E.; La Vecchia, C. Evaluating the quality of dietary intake validation studies. Br. J. Nutr. 2009, 102, S3–S9. [Google Scholar] [CrossRef]
- Carroll, R.J.; Midthune, D.; Subar, A.F.; Shumakovich, M.; Freedman, L.S.; Thompson, F.E.; Kipnis, V. Taking Advantage of the Strengths of 2 Different Dietary Assessment Instruments to Improve Intake Estimates for Nutritional Epidemiology. Am. J. Epidemiol. 2012, 175, 340–347. [Google Scholar] [CrossRef]
- Kourlaba, G.; Panagiotakos, D. The Number of Index Components Affects the Diagnostic Accuracy of a Diet Quality Index: The Role of Intracorrelation and Intercorrelation Structure of the Components. Ann. Epidemiol. 2009, 19, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. The cost of dichotomising continuous variables. Br. Med. J. 2006, 332, 1080. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Rimm, E.; Smith-Warner, S.A.; Feskanich, D.; Stampfer, M.J.; Ascherio, A.; Sampson, L.; Willett, W.C. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am. J. Clin. Nutr. 1999, 69, 243–249. [Google Scholar] [CrossRef]
- Weinstein, S.J.; Vogt, T.M.; Gerrior, S.A. Healthy eating index scores are associated with blood nutrient concentrations in the third National Health and Nutrition Examination Survey. J. Am. Diet. Assoc. 2004, 104, 576–584. [Google Scholar] [CrossRef]
- Hann, C.S.; Rock, C.L.; King, I.; Drewnowski, A. Validation of the Healthy Eating Index with use of plasma biomarkers in a clinical sample of women. Am. J. Clin. Nutr. 2001, 74, 479–486. [Google Scholar] [CrossRef]
- Newby, P.K.; Hu, F.B.; Rimm, E.B.; Smith-Warner, S.A.; Feskanich, D.; Sampson, L.; Willett, W.C. Reproducibility and validity of the Diet Quality Index Revised as assessed by use of a food-frequency questionnaire. Am. J. Clin. Nutr. 2003, 78, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Satija, A. Plant-Based Diets and Risk of Type 2 Diabetes and Coronary Heart Disease; Harvard T.H. Chan School of Public Health: Boston, MA, USA, 2016. [Google Scholar]
- Beaton, G.H.; Milner, J.; Corey, P.; McGuire, V.; Cousins, M.; Stewart, E.; De Ramos, M.; Hewitt, D.; Grambsch, P.V.; Kassim, N.; et al. Sources of variance in 24-hour dietary recall data: Implications for nutrition study design and interpretation. Am. J. Clin. Nutr. 1979, 32, 2546–2559. [Google Scholar] [CrossRef]
- Khani, B.R.; Ye, W.; Terry, P.; Wolk, A. Reproducibility and Validity of Major Dietary Patterns among Swedish Women Assessed with a Food-Frequency Questionnaire. J. Nutr. 2004, 134, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Arciniega, A.A.; Mendez, M.A.; Baena-Diez, J.M.; Martori, M.-A.R.; Soler, C.; Marrugat, J.; Covas, M.-I.; Sanz, H.; Llopis, A.; Schroder, H. Concurrent and construct validity of Mediterranean diet scores as assessed by an FFQ. Public Health Nutr. 2011, 14, 2015–2021. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Van Roosbroeck, S.A.H.; Mackerras, D.; Fritschi, L.; De Klerk, N.H.; Musk, A.W. The reliability of ten-year dietary recall: Implications for cancer research. J. Nutr. 2003, 133, 2663–2668. [Google Scholar] [CrossRef]
- Feskanich, D.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.; Stampfer, M.J.; Litin, L.B.; Willett, W.C. Reproducibility and validity of food intake measurements from a semiquantitative food frequency questionnaire. J. Am. Diet. Assoc. 1993, 93, 790–796. [Google Scholar] [CrossRef]
- Willett, W.L.E. Reproducibility and valdiity of food frequency questionnaires. In Nutritional Epidemiology, 3th ed.; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Auclair, O.; Burgos, S.A. Protein consumption in Canadian habitual diets: Usual intake, inadequacy, and the contribution of animal- and plant-based foods to nutrient intakes. Appl. Physiol. Nutr. Metab. 2021, 46, 501–510. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Portfolio Diet Components | Food Items (Serving Sizes) in FFQ a |
|---|---|
| Plant protein, servings/day | Tofu, soybeans, or vegetable protein (3–4 oz); peas or lima beans (1/2 cup); lentils or beans, kidney, pinto, black-eyed, chickpeas, etc. (1/2 cup); soymilk (8 oz glass) |
| Viscous fiber, servings/day | Cold breakfast cereal, Bran buds (1 cup); cooked oatmeal (1 cup); cooked oat bran (1 cup); oat bran added to food (1 tbsp); barley (1 cup); fresh apples or pears (1); applesauce (1/2 cup); oranges, tangerines, clementines (1); grapefruit (1/2); strawberries, raspberries or blackberries (1/2 cup); blueberries (1/2 cup); okra (1/2 cup); eggplant (1/2 cup); Metamucil supplement (2 tsp) b |
| Nuts, servings/day | Peanut butter (1 tbsp); almond butter (1 tbsp); peanuts (1 oz); almonds (1 oz); walnuts (1 oz); other nuts (1 oz) |
| Phytosterols, mg/day | Estimated from all plant foods |
| MUFAs c, servings/day | Avocado (1/2); olive oil, added to food or bread (1 tbsp); olive oil salad dressing (2 tbsp) |
| Saturated fat/cholesterol, servings/day | Whole milk (8 oz); cream (1 tbsp); ice cream (1/2 cup); other cheese (1 oz); cream cheese (1 oz); eggs with yolk (1); bacon (2 slices); poultry with skin (5 oz); beef/pork hot dogs (1); chicken/turkey hot dogs (1); salami, bologna or other processed meat (2 oz); lean hamburger (1 patty); regular hamburger (1 patty); mixed meals with red meat (1); pork (5 oz); beef/lamb (5 oz); beef liver (4 oz); chicken liver (1 oz); other organ meats (3 oz); butter (1 tsp); Salami, bologna or other processed meat sandwiches (1) |
| Characteristic, Mean (SD)/n (%) | Predictive Validation (n = 652) | Concurrent Validation (n = 50) | p-Value |
|---|---|---|---|
| Age, year | 45.2 (12.6) | 45.3 (11.5) | 0.96 |
| Sex, female | 493 (76) | 31 (62) | 0.03 |
| Current smoker | 45 (7) | 3 (7) | 0.07 |
| Exercise level | |||
| Low | 104 (16) | 7 (14) | 0.62 |
| Medium | 462 (71) | 34 (68) | |
| High | 86 (13) | 9 (18) | |
| Cholesterol-lowering medication use | 43 (7) | 2 (4) | 0.47 |
| Blood pressure lowering medication use | 64 (10) | 6 (12) | 0.62 |
| BMI | 32.1 (5.42) | 28.9 (4.57) | <0.001 |
| Family history of CVD | 288 (44) | 20 (40) | 0.58 |
| Total energy intake, kcal/d | 1995 (707) | 2056 (822) | 0.56 |
| Baseline LDL-C, mmol/L | 3.24 (0.80) | 3.25 (0.70) | 0.93 |
| Highest education completed | 0.54 | ||
| High school or less | 212 (33) | 14 (28) | |
| Undergraduate/college degree | 294 (45) | 25 (50) | |
| Graduate degree | 144 (22) | 11 (22) | |
| Ethnicity a | <0.001 | ||
| Caucasian | 416 (64) | 25 (50) | |
| Asian | 70 (11) | 3 (6) | |
| African & Caribbean | 49 (8) | 0 (0) | |
| Other | 58 (9) | 1 (2) | |
| Unknown | 59 (9) | 21 (42) | |
| Control group | 270 (41) | 27 (54) | 0.08 |
| PDS b, mean (SD), min–max | 18.1 (4.31) 7–30 | 17.6 (4.86) 8–29 | 0.43 |
| Plant protein, servings/day b | 0.41 (0.67) | 0.46 (0.56) | 0.61 |
| Viscous fiber, servings/day b | 1.38 (1.17) | 1.28 (1.35) | 0.56 |
| Nuts, servings/day b | 0.67 (0.86) | 0.90 (1.28) | 0.08 |
| Phytosterols, mg/day b | 337 (158) | 284 (171) | 0.02 |
| MUFAs, servings/day b | 0.65 (0.84) | 0.55 (0.64) | 0.41 |
| Saturated fat/cholesterol, servings/day b | 2.48 (1.82) | 2.89 (2.26) | 0.13 |
| Baseline | 6 Months | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Component | Q1 (1 Point) | Q2 (2 Points) | Q3 (3 Points) | Q4 (4 Points) | Q5 (5 Points) | Q1 (1 Point) | Q2 (2 Points) | Q3 (3 Points) | Q4 (4 Points) | Q5 (5 Points) |
| Plant protein, servings/day | 0.03 | 0.11 | 0.19 | 0.43 | 1.31 | 0.05 | 0.15 | 0.37 | 0.75 | 1.59 |
| Viscous fiber, servings/day | 0.25 | 0.66 | 1.08 | 1.59 | 3.24 | 0.51 | 1.17 | 1.74 | 2.60 | 4.77 |
| Nuts, servings/day | 0.03 | 0.14 | 0.38 | 0.81 | 1.96 | 0.05 | 0.17 | 0.39 | 0.72 | 1.94 |
| Phytosterols, mg/day | 164 | 240 | 310 | 389 | 587 | 182 | 274 | 354 | 443 | 690 |
| MUFAs, servings/day | 0.02 | 0.12 | 0.40 | 0.82 | 2.03 | 0.02 | 0.14 | 0.45 | 0.83 | 2.07 |
| Saturated fat/cholesterol a, servings/day | 5.50 | 3.05 | 2.16 | 1.42 | 0.62 | 4.29 | 2.47 | 1.71 | 1.16 | 0.52 |
| LDL-C (mmol/L) | Per 1-Unit Increase (β Coefficients (95%CI)) | p-Value | 5% Reduction in LDL-C (OR (95% CI)) | p-Value | Pearson Correlation Coefficient | p-Value |
|---|---|---|---|---|---|---|
| Model 1 * | −0.01 (−0.02, −0.002) | 0.02 | 1.05 (1.01–1.10) | 0.01 | −0.08 | 0.03 |
| FFQ | 7DDR | Pearson Correlation Coefficients | |||
|---|---|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | Unadjusted, r (95% CI) | Energy-Adjusted, r (95% CI) | Energy-Adjusted and Deattenuated, r (95% CI) | |
| PDS, points | 17.6 (8–29) | 17.0 (9–28) | 0.66 (0.47, 0.80) | 0.65 (0.45, 0.79) | 0.69 (0.48, 0.85) |
| Plant protein, servings/day | 0.19 (0.00–2.85) | 0.17 (0.00–2.77) | 0.25 (−0.03, 0.49) | 0.25 (−0.04, 0.49) | 0.26 (−0.04, 0.52) |
| Viscous fiber, servings/day | 0.88 (0.05–6.93) | 0.53 (0.00–2.23) | 0.42 (0.15, 0.62) | 0.40 (0.14, 0.61) | 0.44 (0.15, 0.67) |
| Nuts, servings/day | 0.50 (0.00–6.72) | 0.37 (0.00–5.36) | 0.40 (0.14, 0.61) | 0.31 (0.04, 0.54) | 0.33 (0.04, 0.58) |
| Phytosterols, mg/day | 234 (68–964) | 316 (108–780) | 0.40 (0.13, 0.61) | 0.59 (0.38, 0.75) | 0.64 (0.41, 0.80) |
| MUFAs, servings/day | 0.44 (0.00–3.29) | 0.29 (0.00–2.10) | 0.30 (0.02, 0.53) | 0.26 (−0.02, 0.50) | 0.28 (−0.02, 0.55) |
| Saturated fat/cholesterol, servings/day | 2.25 (0.08–10.9) | 3.37 (0.08–7.44) | 0.37 (0.10, 0.59) | 0.37 (0.10, 0.59) | 0.41 (0.11, 0.65) |
| FFQ | 7DDR | Pearson Correlation Coefficients | |||
|---|---|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | Unadjusted, r (95% CI) | Energy-Adjusted, r (95% CI) | Energy-Adjusted and Deattenuated, r (95% CI) | |
| Energy, kcal/day | 2049 (744–4690) | 2114 (1171–3729) | 0.31 (0.04, 0.54) | -- | 0.34 (0.04, 0.58) |
| Carbohydrate, g/day | 233 (80–656) | 270 (100–417) | 0.31 (0.03, 0.54) | 0.59 (0.37, 0.75) | 0.64 (0.40, 0.81) |
| Total protein, g/day | 83 (26–178) | 94 (54–180) | 0.23 (−0.05, 0.48) | 0.38 (0.11, 0.59) | 0.41 (0.12, 0.65) |
| Total fat, g/day | 70 (18–187) | 79 (37–143) | 0.42 (0.15, 0.62) | 0.53 (0.29, 0.70) | 0.57 (0.31, 0.76) |
| Spearman Correlation Coefficients | |||||
|---|---|---|---|---|---|
| Unadjusted, r (95% CI) | Energy-Adjusted, r (95% CI) | Energy-Adjusted and Deattenuated, r (95% CI) | Same Quantile a, n (%) | Opposite Quantile b, n (%) | |
| PDS | 0.69 (0.51, 0.81) | 0.65 (0.45, 0.79) | 0.67 (0.47, 0.83) | 24 (48) | 0 (0) |
| Plant protein | 0.35 (0.07, 0.57) | 0.36 (0.09, 0.58) | 0.38 (0.10, 0.62) | 19 (38) | 1 (2) |
| Viscous fiber | 0.44 (0.18, 0.64) | 0.39 (0.13, 0.60) | 0.42 (0.14, 0.64) | 18 (36) | 2 (4) |
| Nuts | 0.58 (0.36, 0.74) | 0.49 (0.25, 0.68) | 0.53 (0.27, 0.73) | 17 (34) | 0 (0) |
| Phytosterols | 0.43 (0.18, 0.64) | 0.51 (0.27, 0.69) | 0.54 (0.29, 0.73) | 12 (24) | 0 (0) |
| MUFAs | 0.57 (0.35, 0.73) | 0.50 (0.25, 0.68) | 0.54 (0.27, 0.74) | 18 (36) | 1 (2) |
| Saturated fat/cholesterol | 0.31 (0.04, 0.54) | 0.34 (0.07, 0.57) | 0.36 (0.07, 0.71) | 13 (26) | 0 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glenn, A.J.; Boucher, B.A.; Kavcic, C.C.; Khan, T.A.; Paquette, M.; Kendall, C.W.C.; Hanley, A.J.; Jenkins, D.J.A.; Sievenpiper, J.L. Development of a Portfolio Diet Score and Its Concurrent and Predictive Validity Assessed by a Food Frequency Questionnaire. Nutrients 2021, 13, 2850. https://doi.org/10.3390/nu13082850
Glenn AJ, Boucher BA, Kavcic CC, Khan TA, Paquette M, Kendall CWC, Hanley AJ, Jenkins DJA, Sievenpiper JL. Development of a Portfolio Diet Score and Its Concurrent and Predictive Validity Assessed by a Food Frequency Questionnaire. Nutrients. 2021; 13(8):2850. https://doi.org/10.3390/nu13082850
Chicago/Turabian StyleGlenn, Andrea J., Beatrice A. Boucher, Chloe C. Kavcic, Tauseef A. Khan, Melanie Paquette, Cyril W. C. Kendall, Anthony J. Hanley, David J. A. Jenkins, and John L. Sievenpiper. 2021. "Development of a Portfolio Diet Score and Its Concurrent and Predictive Validity Assessed by a Food Frequency Questionnaire" Nutrients 13, no. 8: 2850. https://doi.org/10.3390/nu13082850
APA StyleGlenn, A. J., Boucher, B. A., Kavcic, C. C., Khan, T. A., Paquette, M., Kendall, C. W. C., Hanley, A. J., Jenkins, D. J. A., & Sievenpiper, J. L. (2021). Development of a Portfolio Diet Score and Its Concurrent and Predictive Validity Assessed by a Food Frequency Questionnaire. Nutrients, 13(8), 2850. https://doi.org/10.3390/nu13082850