
Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials



 , ,
, , 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis and Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | Random Sequence Generation | Allocation Concealment | Selective Reporting | Other Sources of Bias | Blinding (Participants and Personnel) | Blinding (Outcome Assessment) | Incomplete Outcome Data | Overall Quality |
|---|---|---|---|---|---|---|---|---|
| Mangoni et al., 2003 [23] | L | H | H | H | H | H | L | Fair |
| Spoelstra-de Man et al., 2004 [33] | L | H | L | H | L | H | L | Good |
| Durga et al., 2005 [34] | L | H | H | H | L | H | L | Good |
| Klerk et al., 2005 [35] | L | H | H | H | L | H | L | Good |
| Olini et al., 2006 | L | H | H | H | H | H | L | Fair |
| Title et al., 2006 [24] | L | H | H | H | L | L | L | Good |
| Moens et al., 2007 [36] | L | H | H | H | L | H | L | Good |
| Bahmani et al., 2014 [37] | L | H | H | H | L | H | L | Good |
| Asemi et al., 2016 [38] | L | H | H | H | L | H | L | Good |
| Chen et al., 2016 [39] | L | H | H | H | H | H | L | Fair |
| Talari et al., 2016 [22] | L | H | H | H | L | H | L | Good |
| Bahmani et al., 2018 [35] | L | H | H | H | L | H | L | Good |
3. Results
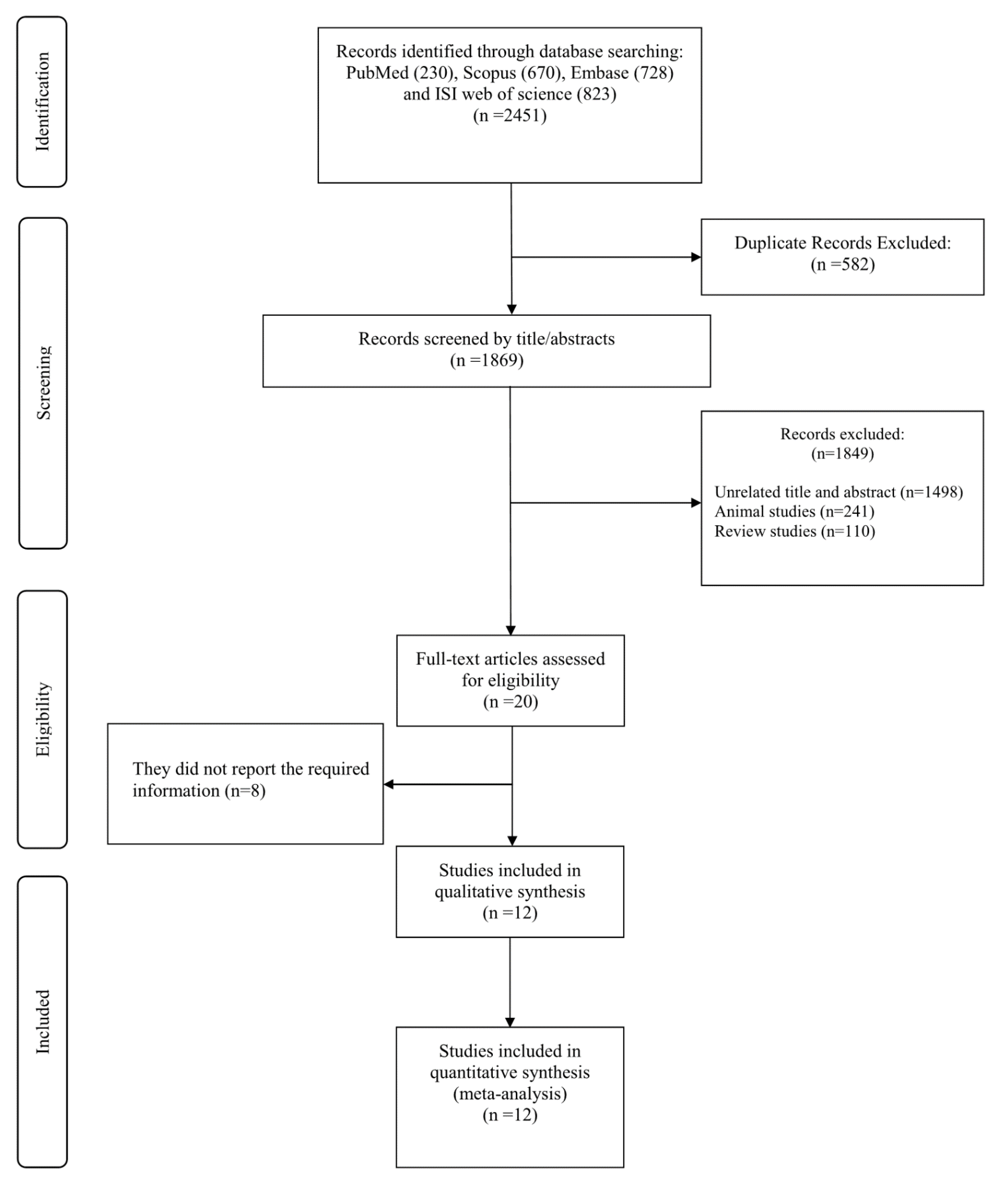
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Quality Assessment
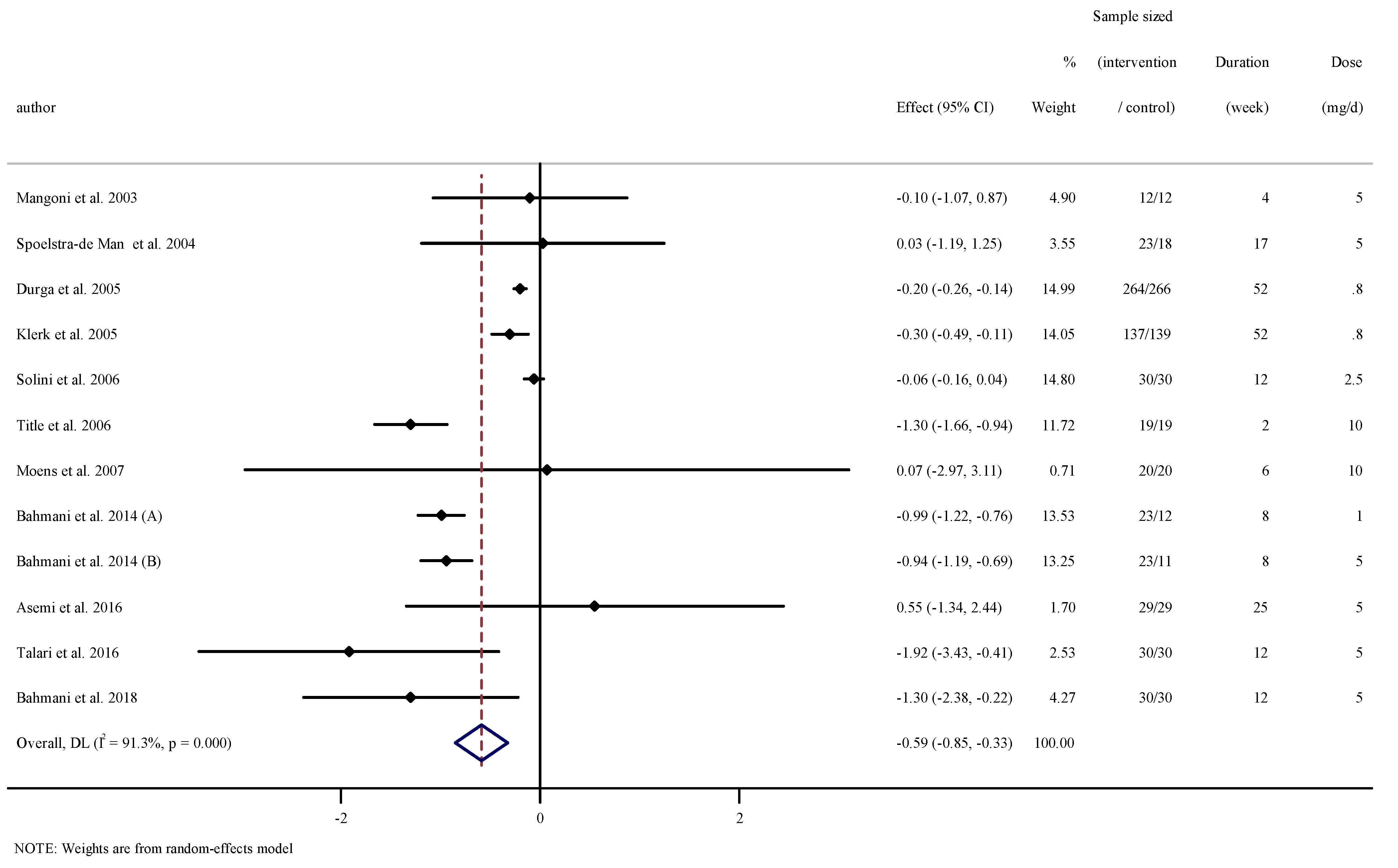
3.4. The Effect of Folic Acid Supplementation on Serum Concentrations of CRP
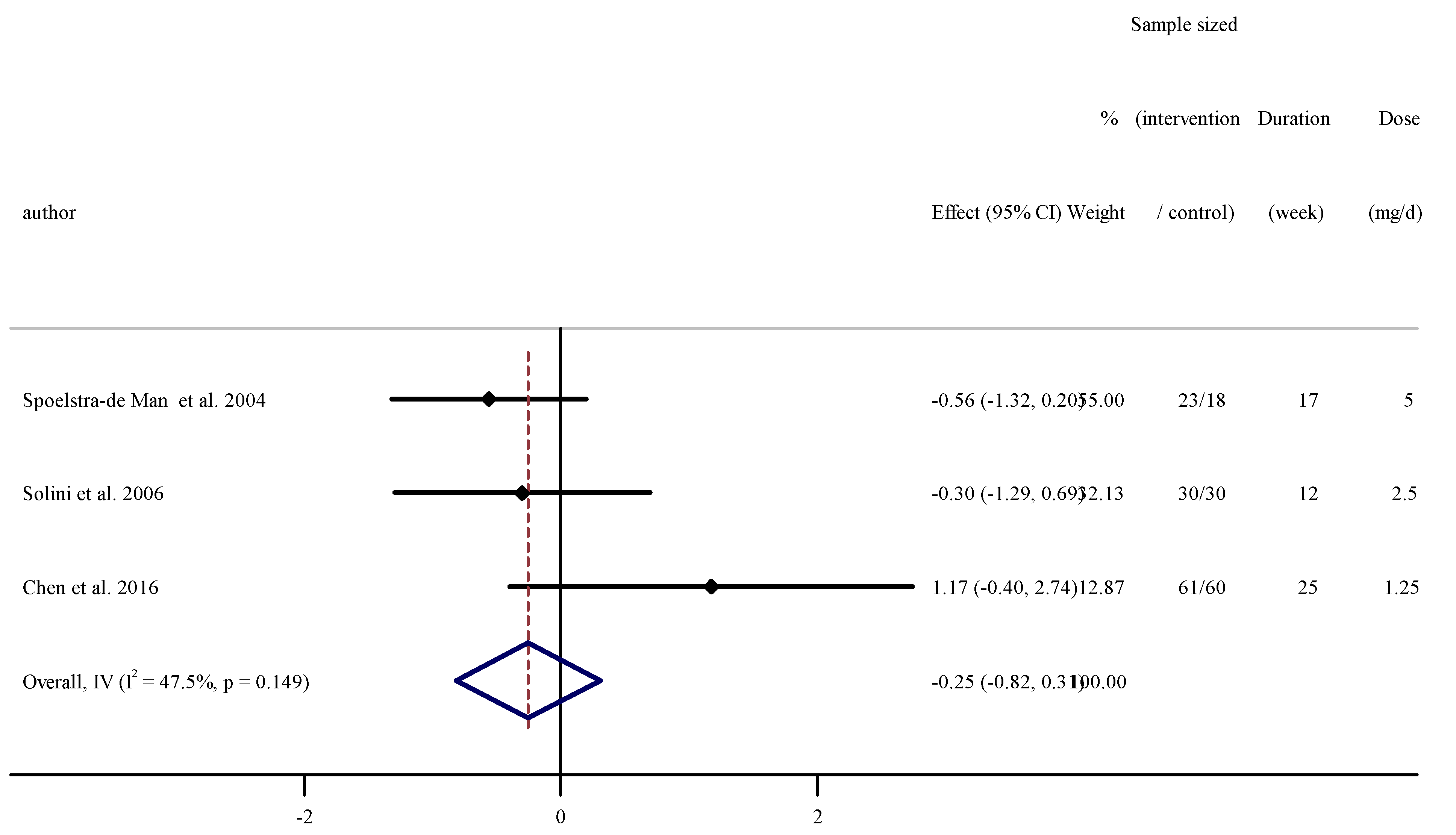
3.5. The Effect of Folic Acid Supplementation on Serum Concentrations of IL-6
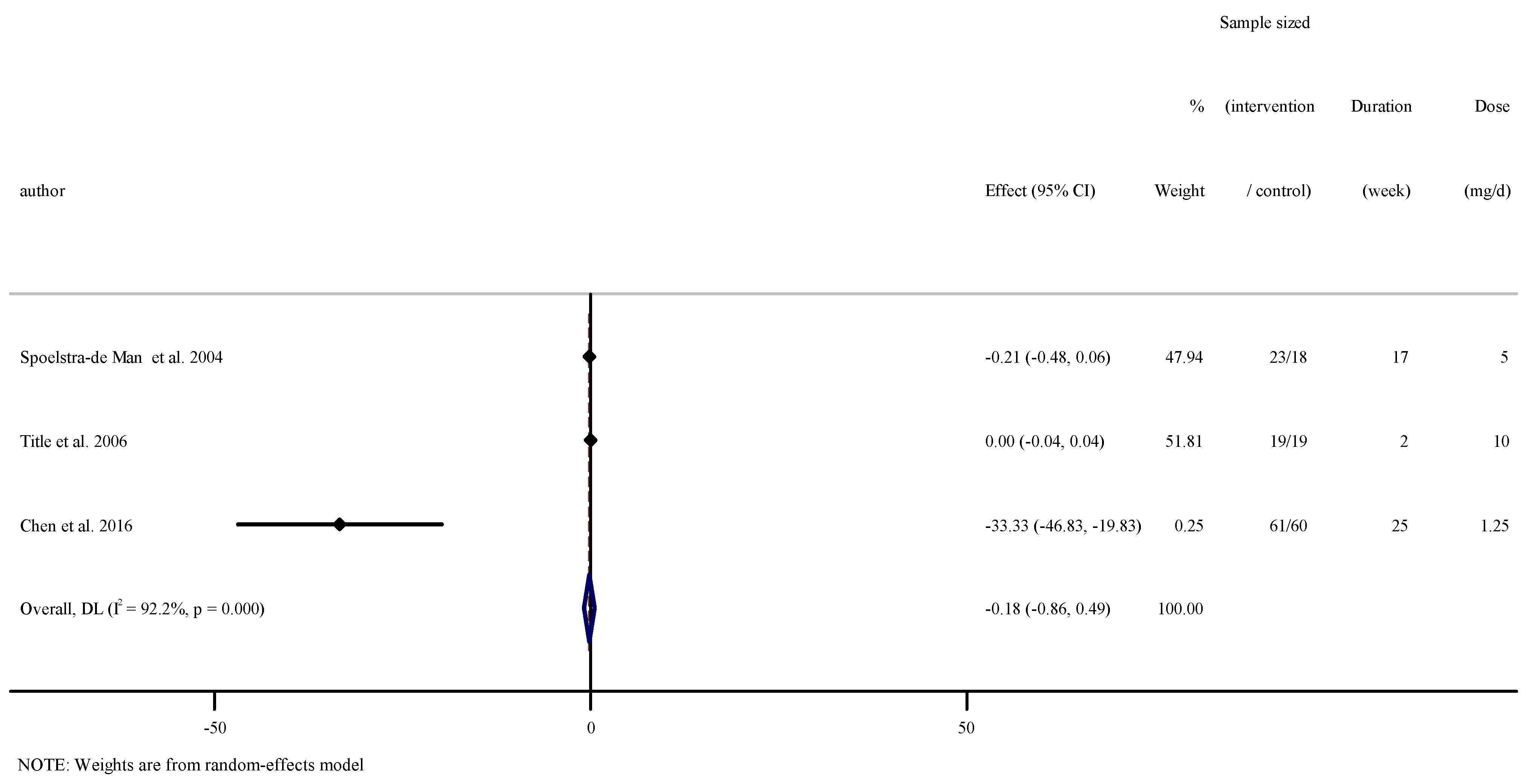
3.6. The Effect of Folic Acid Supplementation on Serum Concentrations of TNF-α
3.7. Sensitivity Analysis
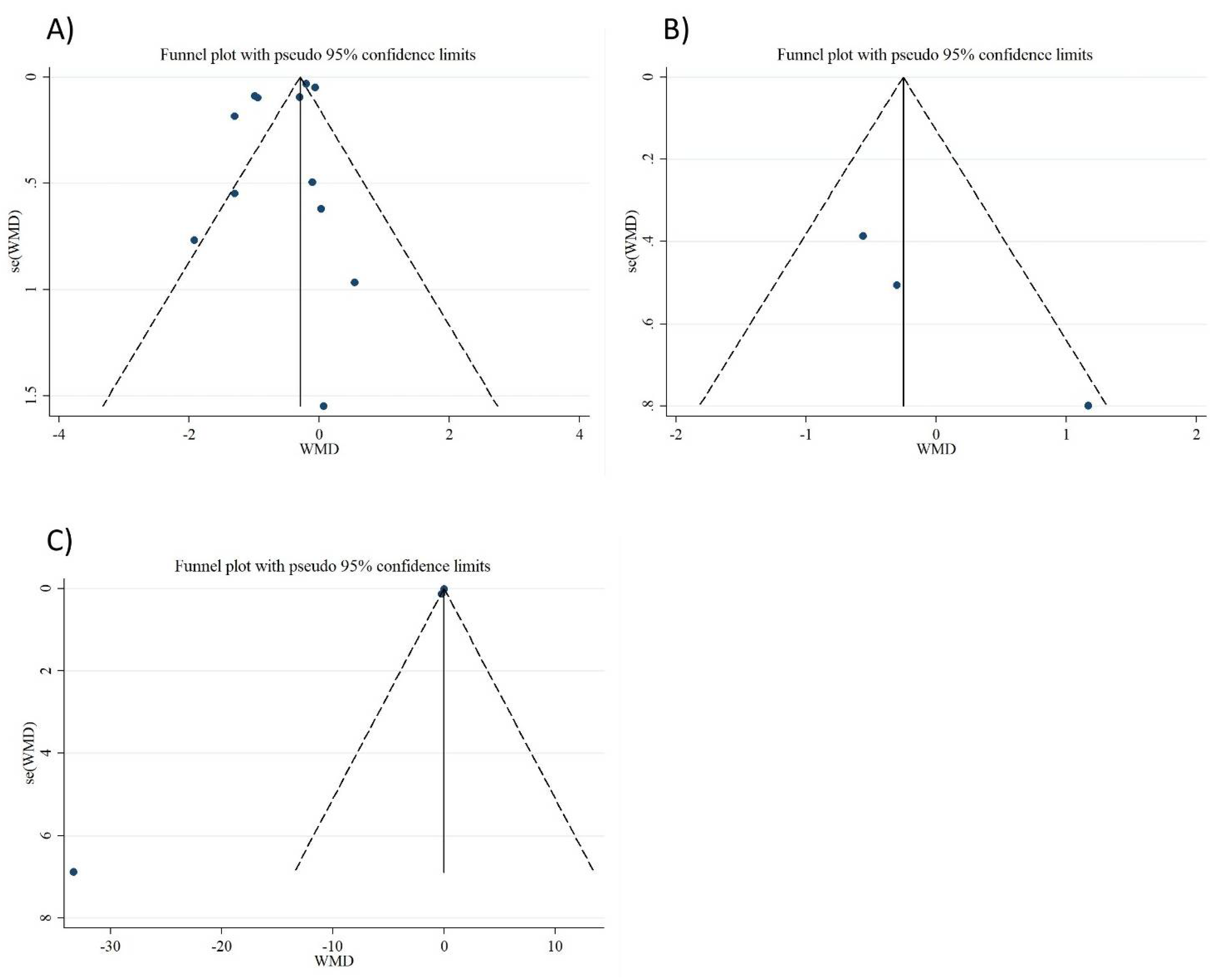
3.8. Publication Bias
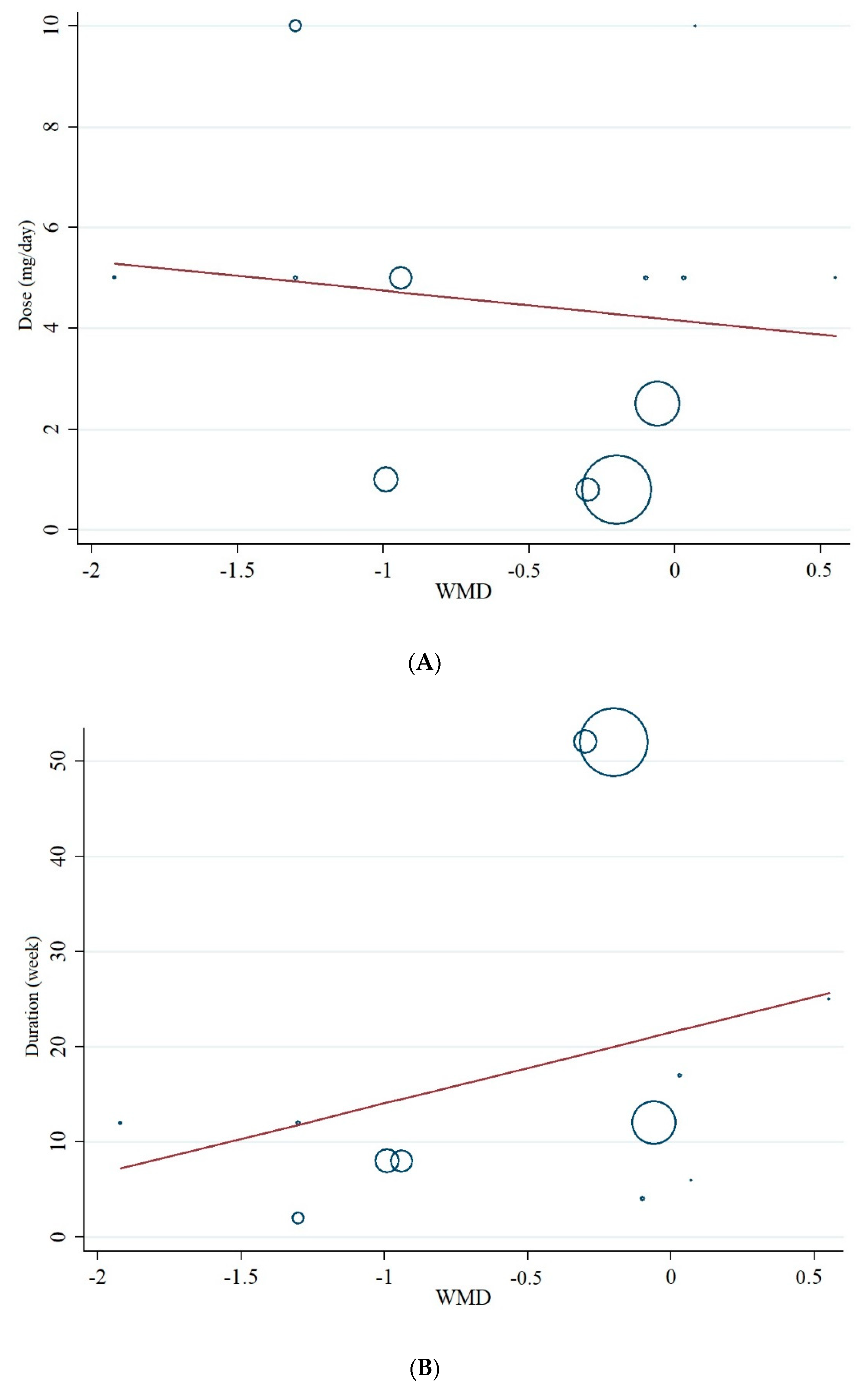
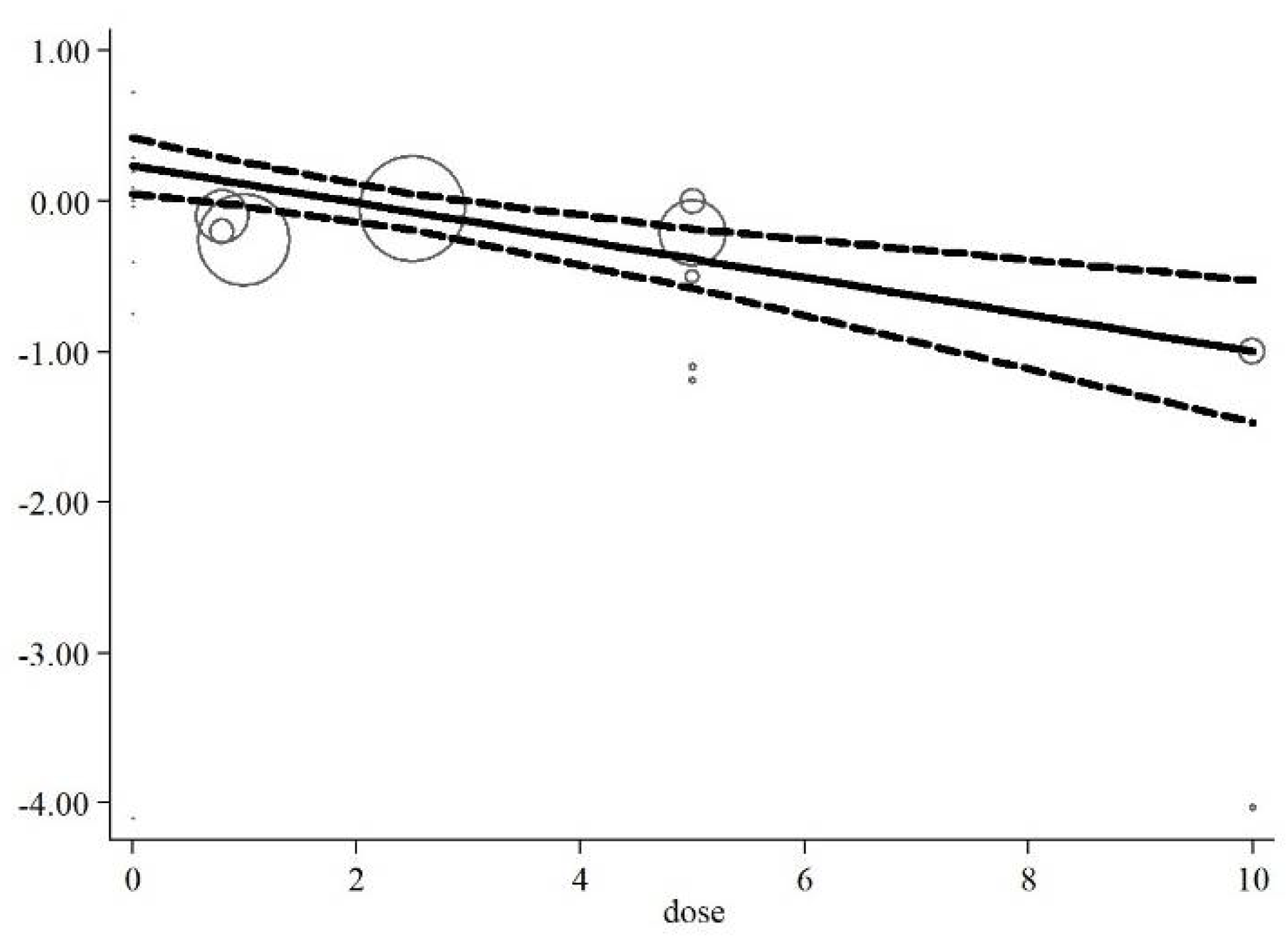
3.9. Meta-Regression and Non-Linear Dose–Response Analysis
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Stankov, S.V. Definition of inflammation, causes of inflammation and possible anti-inflammatory strategies. Open Inflamm. J. 2012, 5, 1–9. [Google Scholar] [CrossRef]
- Suzuki, K. Chronic inflammation as an immunological abnormality and effectiveness of exercise. Biomolecules 2019, 9, 223. [Google Scholar] [CrossRef] [PubMed]
- Ashtary-Larky, D.; Lamuchi-Deli, N.; Milajerdi, A.; Bakhtiar Salehi, M.; Alipour, M.; Kooti, W.; Ashtary-Larky, P.; Alamiri, F.; Sheikhi, A.; Afrisham, R. Inflammatory and biochemical biomarkers in response to high intensity resistance training in trained and untrained men. Asian J. Sports Med. 2017, 8, e13739. [Google Scholar] [CrossRef]
- Zatterale, F.; Longo, M.; Naderi, J.; Raciti, G.A.; Desiderio, A.; Miele, C.; Beguinot, F. Chronic adipose tissue inflammation linking obesity to insulin resistance and type 2 diabetes. Front. Physiol. 2020, 10, 1607. [Google Scholar] [CrossRef]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar] [PubMed]
- Zhang, Y.; Anoopkumar-Dukie, S.; Arora, D.; Davey, A.K. Review of the anti-inflammatory effect of SIRT1 and SIRT2 modulators on neurodegenerative diseases. Eur. J. Pharmacol. 2020, 867, 172847. [Google Scholar] [CrossRef]
- Moosavian, S.P.; Paknahad, Z.; Habibagahi, Z.; Maracy, M. The effects of garlic (Allium sativum) supplementation on inflammatory biomarkers, fatigue, and clinical symptoms in patients with active rheumatoid arthritis: A randomized, double-blind, placebo-controlled trial. Phytother. Res. 2020, 34, 2953–2962. [Google Scholar] [CrossRef]
- Murata, M. Inflammation and cancer. Environ. Health Prev. Med. 2018, 23, 1–8. [Google Scholar] [CrossRef]
- Esser, N.; Paquot, N.; Scheen, A.J. Anti-inflammatory agents to treat or prevent type 2 diabetes, metabolic syndrome and cardiovascular disease. Expert Opin. Investig. Drugs 2015, 24, 283–307. [Google Scholar] [CrossRef]
- Kalmarzi, R.N.; Naleini, S.N.; Ashtary-Larky, D.; Peluso, I.; Jouybari, L.; Rafi, A.; Ghorat, F.; Heidari, N.; Sharifian, F.; Mardaneh, J.; et al. Anti-Inflammatory and Immunomodulatory Effects of Barberry (Berberis vulgaris) and Its Main Compounds. Oxidative Med. Cell. Longev. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- Bagheri, R.; Rashidlamir, A.; Ashtary-Larky, D.; Wong, A.; Alipour, M.; Motevalli, M.S.; Chebbi, A.; Laher, I.; Zouhal, H. Does green tea extract enhance the anti-inflammatory effects of exercise on fat loss? Br. J. Clin. Pharmacol. 2020, 86, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Moosavian, S.P.; Rahimlou, M.; Saneei, P.; Esmaillzadeh, A. Effects of dairy products consumption on inflammatory biomarkers among adults: A systematic review and meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 872–888. [Google Scholar] [CrossRef] [PubMed]
- Galland, L.J. Diet and inflammation. Nutr. Clin. Prac. 2010, 25, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Gunter, B.R.; Butler, K.A.; Wallace, R.L.; Smith, S.M.; Harirforoosh, S. Non-steroidal anti-inflammatory drug-induced cardiovascular adverse events: A meta-analysis. J. Clin. Pharm. Ther. 2016, 42, 27–38. [Google Scholar] [CrossRef]
- Asbaghi, O.; Ashtary-Larky, D.; Bagheri, R.; Nazarian, B.; Olyaei, H.P.; Kelishadi, M.R.; Nordvall, M.; Wong, A.; Dutheil, F.; Naeini, A.A. Beneficial effects of folic acid supplementation on lipid markers in adults: A GRADE-assessed systematic review and dose-response meta-analysis of data from 21,787 participants in 34 randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 2021, 1–19. [Google Scholar] [CrossRef]
- Asbaghi, O.; Naeini, F.; Ashtary-Larky, D.; Moradi, S.; Zakeri, N.; Eslampour, E.; Kelishadi, M.R.; Naeini, A.A. Effects of chromium supplementation on lipid profile in patients with type 2 diabetes: A systematic review and dose-response meta-analysis of randomized controlled trials. J. Trace Elem. Med. Biol. 2021, 66, 126741. [Google Scholar] [CrossRef]
- Asbaghi, O.; Fatemeh, N.; Mahnaz, R.K.; Ehsan, G.; Elham, E.; Behzad, N.; Damoon, A.-L.; Amirmansour, A.N. Effects of chromium supplementation on glycemic control in patients with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. Pharmacol. Res. 2020, 161, 105098. [Google Scholar] [CrossRef]
- Stanhewicz, A.E.; Kenney, W.L. Role of folic acid in nitric oxide bioavailability and vascular endothelial function. Nutr. Rev. 2017, 75, 61–70. [Google Scholar] [CrossRef]
- Mönch, S.; Netzel, M.; Netzel, G.; Ott, U.; Frank, T.; Rychlik, M. Folate bioavailability from foods rich in folates assessed in a short term human study using stable isotope dilution assays. Food Funct. 2014, 6, 241–247. [Google Scholar] [CrossRef]
- Qin, X.; Huo, Y.; Xie, D.; Hou, F.; Xu, X.; Wang, X. Homocysteine-lowering therapy with folic acid is effective in cardiovascular disease prevention in patients with kidney disease: A meta-analysis of randomized controlled trials. Clin. Nutr. 2013, 32, 722–727. [Google Scholar] [CrossRef]
- Pieroth, R.; Paver, S.; Day, S.; Lammersfeld, C. Folate and Its Impact on Cancer Risk. Curr. Nutr. Rep. 2018, 7, 70–84. [Google Scholar] [CrossRef]
- Talari, H.; Rafiee, M.; Farrokhian, A.; Raygan, F.; Bahmani, F.; Mofrad, M.D.; Hamidian, Y.; Tamtaji, O.R.; Karamali, F.; Asemi, Z. The Effects of Folate Supplementation on Carotid Intima-Media Thickness and Metabolic Status in Patients with Metabolic Syndrome. Ann. Nutr. Metab. 2016, 69, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Mangoni, A.A.; Arya, R.; Ford, E.; Asonganyi, B.; Sherwood, R.A.; Ouldred, E.; Swift, C.G.; Jackson, S.H. Effects of folic acid supplementation on inflammatory and thrombogenic markers in chronic smokers. A randomised controlled trial. Thromb. Res. 2003, 110, 13–17. [Google Scholar] [CrossRef]
- Title, L.M.; Ur, E.; Giddens, K.; McQueen, M.J.; Nassar, B.A. Folic acid improves endothelial dysfunction in type 2 diabetes–An effect independent of homocysteine-lowering. Vasc. Med. 2006, 11, 101–109. [Google Scholar] [CrossRef]
- Gariballa, S.; Afandi, B.; AbuHaltem, M.; Yassin, J.; Habib, H.; Ibrahim, W. Oxidative damage and inflammation in obese diabetic Emirati subjects supplemented with antioxidants and B-vitamins: A randomized placebo-controlled trail. Nutr. Metab. 2013, 10, 21. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2009; p. 452. [Google Scholar]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef]
- Sahebkar, A. Are Curcuminoids Effective C-Reactive protein-lowering agents in clinical practice? Evidence from a meta-Analysis. Phytother. Res. 2013, 28, 633–642. [Google Scholar] [CrossRef]
- Xu, C.; Doi, S.A.R. The robust error meta-regression method for dose–response meta-analysis. JBI Evid. Implement. 2018, 16, 138–144. [Google Scholar] [CrossRef]
- Gordon, H.; Oxman, A.; Vist, G.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. Rating quality of evidence and strength of recommendations: GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar]
- Spoelstra-de Man, A.; Brouwer, C.; Terheggen, F.; Bollen, J.; Stehouwer, C.; Smulders, Y. No effect of folic acid on markers of endothelial dysfunction or inflammation in patients with type 2 diabetes mellitus and mild hyperhomocysteinaemia. Medicine 2004, 2, 1–6. [Google Scholar]
- Durga, J.; Van Tits, L.; Schouten, E.G.; Kok, F.J.; Verhoef, P. Effect of lowering of homocysteine levels on inflammatory markers: A randomized controlled trial. Arch. Intern. Med. 2005, 165, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Klerk, M.; Durga, J.; Schouten, E.G.; Kluft, C.; Kok, F.J.; Verhoef, P. No effect of folic acid supplementation in the course of 1 year on haemostasis markers and C-reactive protein in older adults. Thromb. Haemost. 2005, 94, 96–100. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moens, A.L.; Claeys, M.J.; Wuyts, F.L.; Goovaerts, I.; Van Hertbruggen, E.; Wendelen, L.C.; Van Hoof, V.O.; Vrints, C.J. Effect of folic acid on endothelial function following acute myocardial infarction. Am. J. Cardiol. 2007, 99, 476–481. [Google Scholar] [CrossRef]
- Bahmani, F.; Karamali, M.; Shakeri, H.; Asemi, Z. The effects of folate supplementation on inflammatory factors and biomarkers of oxidative stress in overweight and obese women with polycystic ovary syndrome: A randomized, double-blind, placebo-controlled clinical trial. Clin. Endocrinol. 2014, 81, 582–587. [Google Scholar] [CrossRef]
- Asemi, Z.; Vahedpoor, Z.; Jamilian, M.; Bahmani, F.; Esmaillzadeh, A. Effects of long-term folate supplementation on metabolic status and regression of cervical intraepithelial neoplasia: A randomized, double-blind, placebo-controlled trial. Nutrients 2016, 32, 681–686. [Google Scholar] [CrossRef]
- Chen, H.; Liu, S.; Ji, L.; Wu, T.; Ji, Y.; Zhou, Y.; Zheng, M.; Zhang, M.; Xu, W.; Huang, G. Folic acid supplementation mitigates Alzheimer’s disease by reducing inflammation: A randomized controlled trial. Mediat. Inflamm. 2016, 2016, 5912146. [Google Scholar] [CrossRef]
- Bahmani, F.; Galougahi, F.R.; Vahedpoor, Z.; Jamilian, M.; Mahmoodi, S.; Baghban, R.; Bagherian, T.; Mehrizi, M.Z.; Asemi, Z. The Effects of Folic Acid Supplementation on Recurrence and Metabolic Status in Endometrial Hyperplasia: A Randomized, Double-Blind, Placebo-Controlled Trial. Arch. Iran. Med. 2018, 21, 452–459. [Google Scholar]
- Solini, A.; Santini, E.; Ferrannini, E. Effect of short-term folic acid supplementation on insulin sensitivity and inflammatory markers in overweight subjects. Int. J. Obes. 2006, 30, 1197–1202. [Google Scholar] [CrossRef]
- González-Fernández, D.; Pons, E.D.C.; Rueda, D.; Sinisterra, O.T.; Murillo, E.; Scott, M.E.; Koski, K.G. C-reactive protein is differentially modulated by co-existing infections, vitamin deficiencies and maternal factors in pregnant and lactating indigenous Panamanian women. Infect. Dis. Poverty 2017, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ghafourian, M.; Ashtary-Larky, D.; Chinipardaz, R.; Eskandary, N.; Mehavaran, M. Inflammatory Biomarkers’ Response to Two Different Intensities of a Single Bout Exercise Among Soccer Players. Iran. Red Crescent Med. J. 2016, 18, e21498. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, Z.; Wong, E.B.; Ndung’U, T.; Kasprowicz, V.O.; Bishai, W.R. Latent and active tuberculosis infection increase immune activation in individuals co-infected with HIV. EBioMedicine 2015, 2, 334–340. [Google Scholar] [CrossRef]
- De Souza, A.B.; Okawa, R.T.; Silva, C.O.; Araújo, M.G. Short-term changes on C-reactive protein (CRP) levels after non-surgical periodontal treatment in systemically healthy individuals. Clin. Oral Investig. 2017, 21, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hwang, J.-Y.; Ha, E.-H.; Park, H.; Ha, M.; Lee, S.-J.; Hong, Y.-C.; Chang, N. Association of maternal folate nutrition and serum C-reactive protein concentrations with gestational age at delivery. Eur. J. Clin. Nutr. 2010, 65, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.C.; Furlanetto, T.W. Does serum 25-hydroxyvitamin D decrease during acute-phase response? A systematic review. Nutr. Res. 2015, 35, 91–96. [Google Scholar] [CrossRef]
- Gebreselassie, S.G.; Gase, F.E.; Deressa, M.U. Prevalence and correlates of prenatal vitamin A deficiency in rural Sidama, Southern Ethiopia. J. Health Popul. Nutr. 2013, 31, 185–194. [Google Scholar] [CrossRef]
- Fatahi, S.; Pezeshki, M.; Mousavi, S.; Teymouri, A.; Rahmani, J.; Varkaneh, H.K.; Ghaedi, E. Effects of folic acid supplementation on C-reactive protein: A systematic review and meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 432–439. [Google Scholar] [CrossRef]
- Haynes, B.M.H.; Pfeiffer, C.M.; Sternberg, M.R.; Schleicher, R.L. Selected physiologic variables are weakly to moderately associated with 29 biomarkers of diet and nutrition, NHANES 2003–2006. J. Nutr. 2013, 143, 1001S–1010S. [Google Scholar] [CrossRef]
- Mierzecki, A.; Kłoda, K.; Jastrzębska, M.; Chełstowski, K.; Honczarenko, K.; Kozłowska-Wojciechowska, M.; Naruszewicz, M. Is there an effect of folic acid supplementation on the coagulation factors and C-reactive protein concentrations in subjects with atherosclerosis risk factors? Postępy Hig. Med. Doświadczalnej 2012, 66. [Google Scholar] [CrossRef]
- Brönstrup, A.; Hages, M.; Prinz-Langenohl, R.; Pietrzik, K. Effects of folic acid and combinations of folic acid and vitamin B-12 on plasma homocysteine concentrations in healthy, young women. Am. J. Clin. Nutr. 1998, 68, 1104–1110. [Google Scholar] [CrossRef]
- Papatheodorou, L.; Weiss, N. Vascular Oxidant Stress and Inflammation in Hyperhomocysteinemia. Antioxid. Redox Signal. 2007, 9, 1941–1958. [Google Scholar] [CrossRef]
- Xie, J.-J.; Yu, X.; Liao, Y.-H.; Chen, J.; Yao, R.; Chen, Y.; Liao, M.Y.; Ding, Y.; Tang, T.T.; Cheng, X. Poly(ADP-Ribose) polymerase inhibition attenuates atherosclerotic plaque development in ApoE−/− mice with hyperhomocysteinemia. J. Atheroscler. Thromb. 2009, 16, 641–653. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Huang, X.; He, Z.; Jiang, X.; Hou, M.; Tang, Z.; Zhen, X.; Liang, Y.; Ma, J. Folic acid represses hypoxia-induced inflammation in THP-1 cells through inhibition of the PI3K/Akt/HIF-1α pathway. PLoS ONE 2016, 11, e0151553. [Google Scholar] [CrossRef] [PubMed]
- Feng, D.; Zhou, Y.; Xia, M.; Ma, J. Folic acid inhibits lipopolysaccharide-induced inflammatory response in RAW264.7 macrophages by suppressing MAPKs and NF-κB activation. Inflamm. Res. 2011, 60, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Tak, P.P.; Firestein, G.S. NF-κB: A key role in inflammatory diseases. J. Clin. Investig. 2001, 107, 7–11. [Google Scholar] [CrossRef]
- Niki, E. Lipid peroxidation products as oxidative stress biomarkers. BioFactors 2008, 34, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Tominaga, T.; Ruhee, R.T.; Ma, S. Characterization and modulation of systemic inflammatory response to exhaustive exercise in relation to oxidative stress. Antioxidants 2020, 9, 401. [Google Scholar] [CrossRef] [PubMed]
- Joshi, R.; Adhikari, S.; Patro, B.; Chattopadhyay, S.; Mukherjee, T. Free radical scavenging behavior of folic acid: Evidence for possible antioxidant activity. Free Radic. Biol. Med. 2001, 30, 1390–1399. [Google Scholar] [CrossRef]
- Kostyuk, V.A.; Potapovich, A.I.; Suhan, T.O.; de Luca, C.; Korkina, L.G. Antioxidant and signal modulation properties of plant polyphenols in controlling vascular inflammation. Eur. J. Pharmacol. 2011, 658, 248–256. [Google Scholar] [CrossRef]
- Asbaghi, O.; Ghanavati, M.; Ashtary-Larky, D.; Bagheri, R.; RezaeiKelishadi, M.; Nazarian, B.; Nordvall, M.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2021, 10, 871. [Google Scholar] [CrossRef]
- Field, M.; Stover, P.J. Safety of folic acid. Ann. N. Y. Acad. Sci. 2017, 1414, 59–71. [Google Scholar] [CrossRef]
- Finglas, P.M.; Allen, L.; Bailey, L. Dietary Reference intakes for thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin and choline. Trends Food Sci. Technol. 2000, 11, 296–297. [Google Scholar] [CrossRef]







| Studies | Country | Study Design | Participant | Sample Size and Sex | Sample Size | Trial Duration (Week) | Means Age | Means BMI | Intervention | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IG | CG | IG | CG | IG | CG | Acid Folic Dose (mg/d) | Control Group | Adverse Effects | ||||||
| Mangoni et al., 2003 [23] | United Kingdom | RA/PC (parallel) | healthy smokers | 24: 9M, 15F | 12 | 12 | 4 | 39.7 ± 11.77 | 36 ± 12.47 | 25.7 ± 2.77 | 24.9 ± 3.11 | 5 | Placebo | No |
| Spoelstra-de Man et al., 2004 [33] | The Netherlands | RA/DB/PC (parallel) | type 2 diabetes mellitus | 41: 24M, 10F | 23 | 18 | 17 | 63.7 ± 8.6 | 66.1 ± 8.5 | 29.3 ± 3.9 | 28.8 ± 3.4 | 5 | Placebo | NR |
| Durga et al., 2005 [34] | The Netherlands | RA/DB/PC (parallel) | men and postmenopausal women | 530: 378M, 152F | 264 | 266 | 52 | 60 ± 5 | 60 ± 6 | NR | NR | 0.8 | Placebo | NR |
| Klerk et al., 2005 [35] | The Netherlands | RA/DB/PC (parallel) | older adults | 276 | 137 | 139 | 52 | 59.5 ± 5.8 | 60.2 ± 5.2 | 26.8 ± 3.9 | 26.8 ± 3.9 | 0.8 | Placebo | NR |
| Solini et al., 2006 [41] | Italy | RA/PC (parallel) | overweight subjects | 60: 19M, 41F | 30 | 30 | 12 | 50 ± 7 | 49 ± 8 | 27.5 ± 0.6 | 27.4 ± 0.6 | 2.5 | Placebo | NR |
| Title et al., 2006 [24] | Canada | RA/DB/PC (cross-over) | type 2 diabetes | 19: 9M,10F | 19 | 19 | 2 | 54.5 ± 5.9 | 54.5 ± 5.9 | NR | NR | 10 | Placebo | NR |
| Moens et al., 2007 [36] | Belgium | RA/DB/PC (cross-over) | acute myocardial infarction | 40: 35M, 5F | 20 | 20 | 6 | 57 ± 11 | 56 ± 14 | NR | NR | 10 | Placebo | No |
| Bahmani et al., 2014 (A) [37] | Iran | RA/DB/PC (parallel) | overweight and obese women with polycystic ovary syndrome | 46: 46F | 23 | 23 | 8 | 24.1 ± 5.4 | 24.9 ± 5.9 | 26.1 ± 6.2 | 27.6 ± 5.7 | 1 | Placebo | NR |
| Bahmani et al., 2014 (B) [37] | Iran | RA/DB/PC (parallel) | overweight and obese women with polycystic ovary syndrome | 46: 46F | 23 | 23 | 8 | 25.1 ± 4.9 | 24.9 ± 5.9 | 29 ± 5.9 | 27.6 ± 5.7 | 5 | Placebo | NR |
| Asemi et al., 2016 [38] | Iran | RA/DB/PC (parallel) | cervical intraepithelial neoplasia grade 1 | 58: 58F | 29 | 29 | 25 | 36.8 ± 8.8 | 39.1 ± 9.1 | 28.2 ± 3.5 | 29.8 ± 6.4 | 5 | Placebo | No |
| Chen et al., 2016 [39] | China | RA/SB (parallel) | Alzheimer’s disease | 121: 61M, 60F | 61 | 60 | 25 | 68.1 ± 8.5 | 67.63 ± 7.92 | 23.25 ± 3.06 | 23.58 ± 4.28 | 1.25 | No intervention | NR |
| Talari et al. 2016 [22] | Iran | RA/DB/PC (parallel) | metabolic syndrome | 60: 26M, 34F | 30 | 30 | 12 | 62.1 ± 9.6 | 65.4 ± 11.5 | 29.8 ± 3.8 | 29.8 ± 4.4 | 5 | Placebo | NR |
| Bahmani et al., 2018 [35] | Iran | RA/DB/PC (parallel) | endometrial hyperplasia | 60: 60F | 30 | 30 | 12 | 44.4 ± 6.5 | 44.7 ± 3.1 | 30.7 ± 4.6 | 30.5 ± 3.8 | 5 | Placebo | No |
| NO | WMD (95%CI) | P-value | Heterogeneity | ||||
|---|---|---|---|---|---|---|---|
| P Heterogeneity | I2 | P between Sub-Groups | Tau-Squared | ||||
| Subgroup analyses of folic acid supplementation on serum concentraitons of CRP | |||||||
| Overall effect | 12 | −0.59 (−0.85, −0.32) | <0.001 | <0.001 | 91.3% | 0.1186 | |
| Baseline CRP (mg/L) | |||||||
| <3 | 7 | −0.44 (−0.73, −0.14) | 0.003 | <0.001 | 95.4% | <0.001 | 0.1186 |
| ≥3 | 5 | −1.19 (−1.72, −0.65) | <0.001 | 0.284 | 20.5% | 0.0907 | |
| Trial duration (week) | |||||||
| ≤8 | 5 | −0.99 (−1.19, −0.79) | <0.001 | 0.152 | 40.4% | <0.001 | 0.0242 |
| >8 | 7 | −0.20 (−0.36, −0.05) | 0.008 | 0.007 | 65.9% | 0.0157 | |
| Intervention dose (mg/d) | |||||||
| <5 | 4 | −0.37 (−0.68, −0.07) | 0.014 | <0.001 | 96.4% | <0.001 | 0.0611 |
| ≥5 | 8 | −0.89 (−1.27, −0.51) | <0.001 | 0.057 | 49.0% | 0.1139 | |
| Age (year) | |||||||
| <50 | 5 | −0.92 (−1.13, −0.71) | <0.001 | 0.203 | 32.7% | <0.001 | 0.0558 |
| >50 | 7 | −0.40 (−0.64, −0.16) | 0.001 | <0.001 | 87.8% | 0.0238 | |
| Sex | |||||||
| Both sexes | 8 | −0.38 (−0.62, −0.15) | 0.001 | <0.001 | 85.8% | <0.001 | 0.0541 |
| Male | 4 | −0.96 (−1.09, −0.83) | <0.001 | 0.397 | 0.0% | 0.0000 | |
| Health status | |||||||
| Healthy | 4 | −0.16 (−0.27, −0.06) | 0.002 | 0.057 | 60.2% | 0.006 | |
| Type 2 diabetes | 2 | −0.76 (−2.04, 0.51) | 0.239 | 0.040 | 76.2% | <0.001 | 0.674 |
| Polycystic ovary syndrome | 2 | −0.96 (−1.13, −0.79) | <0.001 | 0.775 | 0.0% | 0.0000 | |
| Subgroup analyses of folic acid supplementation on serum concentraitons on IL-6 | |||||||
| Overall effect | 3 | −0.11 (−0.95, 0.71) | 0.780 | 0.149 | 47.5% | 0.2572 | |
| Subgroup analyses of folic acid supplementation on serum concentraitons of TNF-α | |||||||
| Overall effect | 3 | −0.18 (−0.85, 0.49) | 0.594 | <0.001 | 92.2% | 0.2278 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asbaghi, O.; Ashtary-Larky, D.; Bagheri, R.; Moosavian, S.P.; Nazarian, B.; Afrisham, R.; Kelishadi, M.R.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials. Nutrients 2021, 13, 2327. https://doi.org/10.3390/nu13072327
Asbaghi O, Ashtary-Larky D, Bagheri R, Moosavian SP, Nazarian B, Afrisham R, Kelishadi MR, Wong A, Dutheil F, Suzuki K, et al. Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials. Nutrients. 2021; 13(7):2327. https://doi.org/10.3390/nu13072327
Chicago/Turabian StyleAsbaghi, Omid, Damoon Ashtary-Larky, Reza Bagheri, Seyedeh Parisa Moosavian, Behzad Nazarian, Reza Afrisham, Mahnaz Rezaei Kelishadi, Alexei Wong, Frédéric Dutheil, Katsuhiko Suzuki, and et al. 2021. "Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials" Nutrients 13, no. 7: 2327. https://doi.org/10.3390/nu13072327
APA StyleAsbaghi, O., Ashtary-Larky, D., Bagheri, R., Moosavian, S. P., Nazarian, B., Afrisham, R., Kelishadi, M. R., Wong, A., Dutheil, F., Suzuki, K., & Alavi Naeini, A. (2021). Effects of Folic Acid Supplementation on Inflammatory Markers: A Grade-Assessed Systematic Review and Dose–Response Meta-Analysis of Randomized Controlled Trials. Nutrients, 13(7), 2327. https://doi.org/10.3390/nu13072327