
A Smartphone Intervention to Promote Time Restricted Eating Reduces Body Weight and Blood Pressure in Adults with Overweight and Obesity: A Pilot Study


 ,
,
Abstract
1. Introduction
2. Materials and Methods
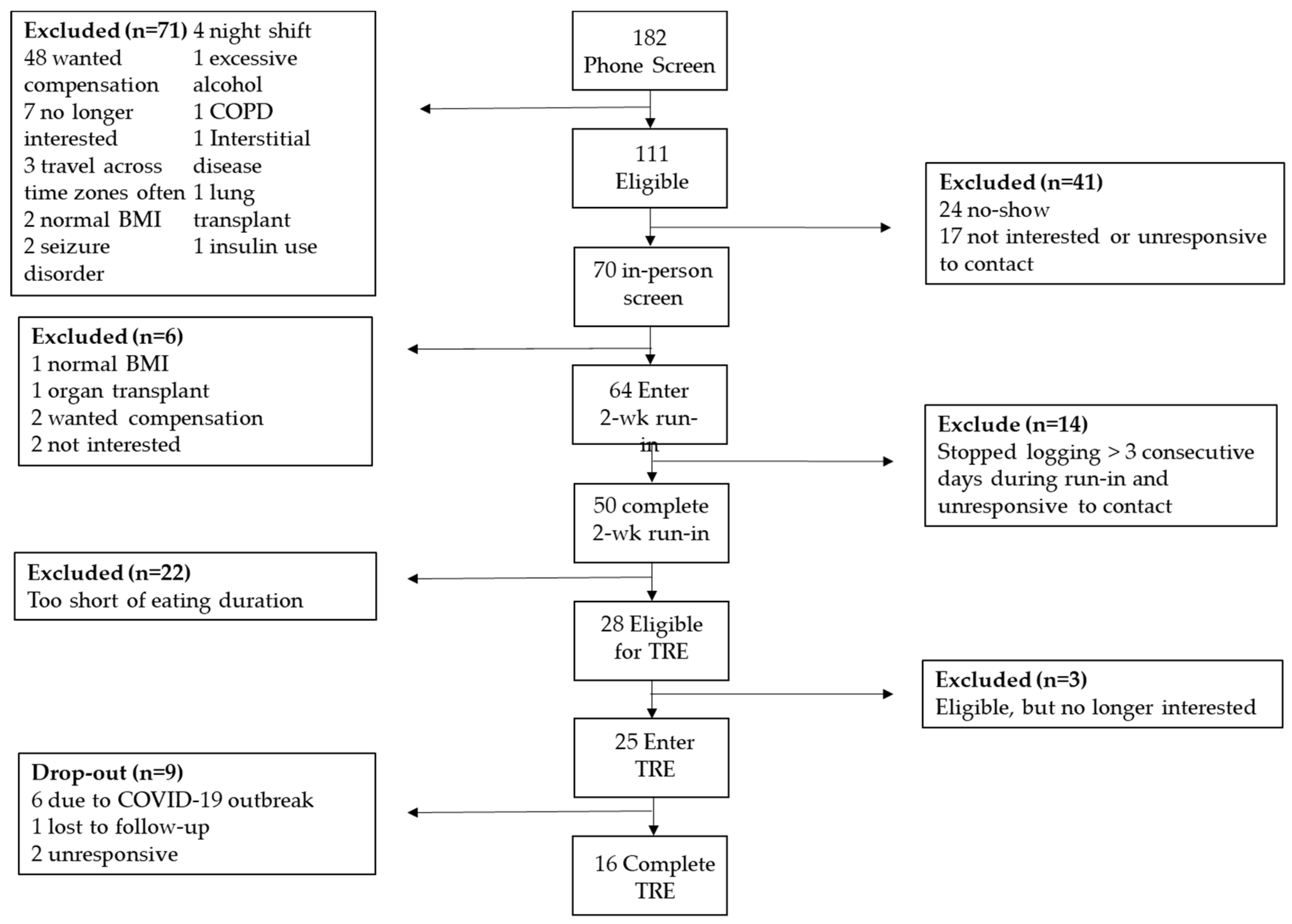
2.1. Participants
2.2. Study Design
2.3. Questionnaires and Survey
2.4. myCircadianClock (mCC) App
2.5. Definition of Eating Window and Adherence
2.6. Statistical Analysis
3. Results
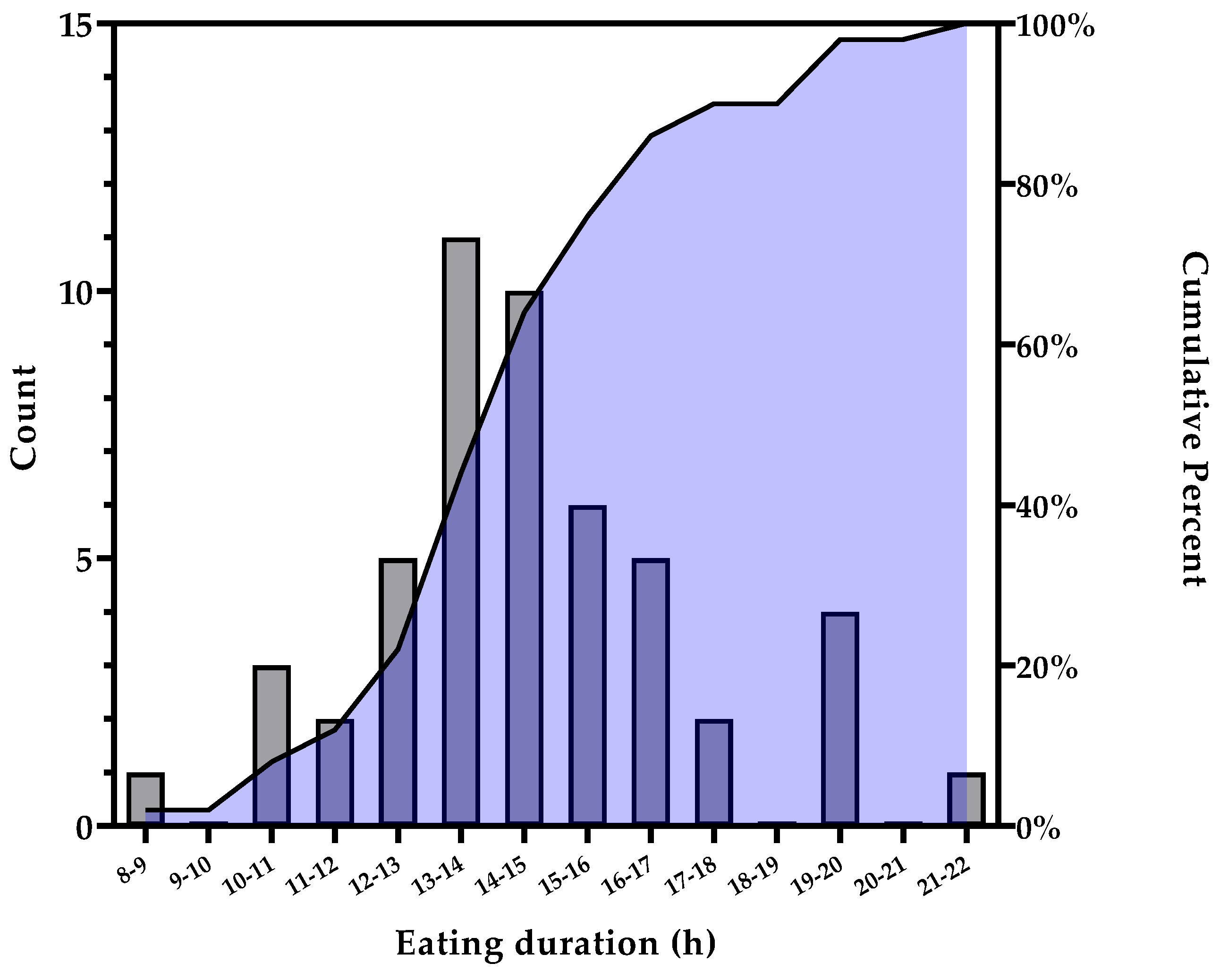
3.1. Baseline Run-in Period
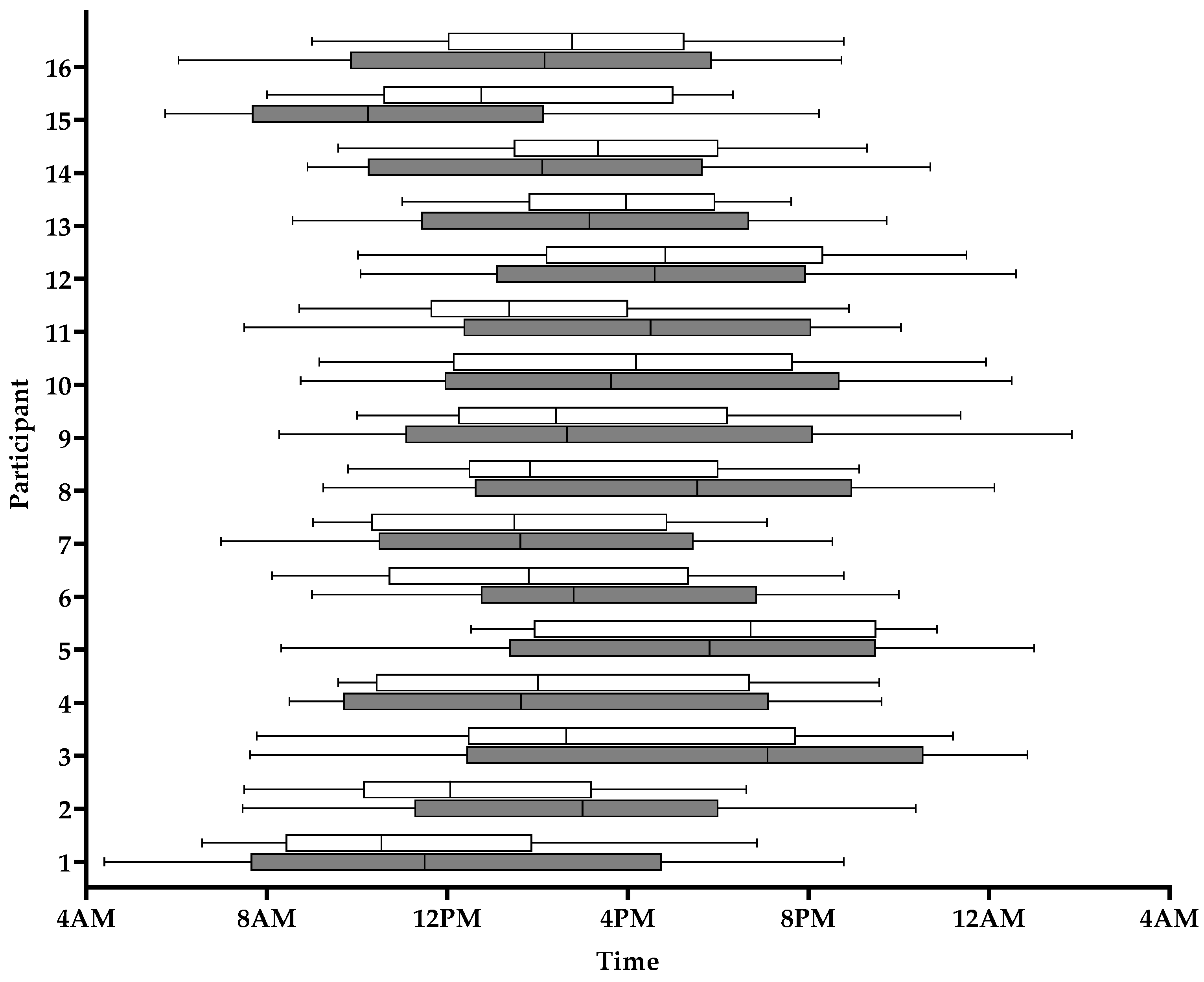
3.2. TRE Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Overweight and Obesity: Adult Obesity Facts. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 18 March 2021).
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Biener, A.I.; Decker, S.L.; for the Agency for Healthcare Research and Quality. Medical Care Use and Expenditures Associated With Adult Obesity in the United States. JAMA 2018, 319, 218. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, F.X. Medical hazards of obesity. Ann. Intern. Med. 1993, 119 Pt 2, 655–660. [Google Scholar] [CrossRef]
- Liou, T.H.; Pi-Sunyer, F.X.; Laferrere, B. Physical disability and obesity. Nutr. Rev. 2005, 63, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Naghavi, M.; Murray, C.J.L. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- Heron, M. Deaths: Leading Causes for 2017. Natl. Vital Stat. Rep. 2019, 68, 1–77. [Google Scholar]
- Diabetes Prevention Program Research Group. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar]
- Antoni, R.; Robertson, T.M.; Robertson, M.D.; Johnston, J.D. A pilot feasibility study exploring the effects of a moderate time-restricted feeding intervention on energy intake, adiposity and metabolic physiology in free-living human subjects. J. Nutr. Sci. 2018, 7, 7. [Google Scholar] [CrossRef]
- Cioffi, I.; Evangelista, A.; Ponzo, V.; Ciccone, G.; Soldati, L.; Santarpia, L.; Contaldo, F.; Pasanisi, F.; Ghigo, E.; Bo, S. Intermittent versus continuous energy restriction on weight loss and cardiometabolic outcomes: A systematic review and meta-analysis of randomized controlled trials. J. Transl. Med. 2018, 16, 371. [Google Scholar] [CrossRef]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27, 1212–1221.e3. [Google Scholar] [CrossRef]
- Jamshed, H.; Beyl, R.A.; Della Manna, D.L.; Yang, E.S.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves 24-Hour Glucose Levels and Affects Markers of the Circadian Clock, Aging, and Autophagy in Humans. Nutrients 2019, 11, 1234. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Haggerty, N.; Song, J.; Kroeger, C.M.; Trepanowski, J.F.; Panda, S.; Varady, K.A. Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutr. Healthy Aging 2018, 4, 345–353. [Google Scholar] [CrossRef]
- Tinsley, G.M.; Forsse, J.S.; Butler, N.K.; Paoli, A.; Bane, A.A.; La Bounty, P.M.; Morgan, G.B.; Grandjean, P.W. Time-restricted feeding in young men performing resistance training: A randomized controlled trial. Eur. J. Sport Sci. 2017, 17, 200–207. [Google Scholar] [CrossRef]
- Gill, S.; Panda, S. A Smartphone App Reveals Erratic Diurnal Eating Patterns in Humans that Can Be Modulated for Health Benefits. Cell Metab. 2015, 22, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Stote, K.S.; Baer, D.J.; Spears, K.; Paul, D.R.; Harris, G.K.; Rumpler, W.V.; Strycula, P.; Najjar, S.S.; Ferrucci, L.; Ingram, D.K.; et al. A controlled trial of reduced meal frequency without caloric restriction in healthy, normal-weight, middle-aged adults. Am. J. Clin. Nutr. 2007, 85, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.C.; Burley, V.J.; Nykjaer, C.; Cade, J.E. Adherence to a smartphone application for weight loss compared to website and paper diary: Pilot randomized controlled trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef] [PubMed]
- McHill, A.W.; Phillips, A.J.; Czeisler, C.A.; Keating, L.; Yee, K.; Barger, L.K.; Garaulet, M.; Scheer, F.A.; Klerman, E.B. Later circadian timing of food intake is associated with increased body fat. Am. J. Clin. Nutr. 2017, 106, 1213–1219. [Google Scholar] [CrossRef]
- Belkacemi, L.; Selselet-Attou, G.; Louchami, K.; Sener, A.; Malaisse, W.J. Intermittent fasting modulation of the diabetic syndrome in sand rats. II. In vivo investigations. Int. J. Mol. Med. 2010, 26, 759–765. [Google Scholar]
- Karatzi, K.; Moschonis, G.; Choupi, E.; Manios, Y.; Healthy Growth Study Group. Late-night overeating is associated with smaller breakfast, breakfast skipping, and obesity in children: The Healthy Growth Study. Nutrition 2017, 33, 141–144. [Google Scholar] [CrossRef]
- Gupta, N.J.; Kumar, V.; Panda, S. A camera-phone based study reveals erratic eating pattern and disrupted daily eating-fasting cycle among adults in India. PLoS ONE 2017, 12, e0172852. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.S.; Manoogian, E.N.C.; Alvear, A.; Fleischer, J.G.; Thor, H.; Dietsche, K.; Wang, Q.; Hodges, J.S.; Esch, N.; Malaeb, S.; et al. Time-Restricted Eating Effects on Body Composition and Metabolic Measures in Humans who are Overweight: A Feasibility Study. Obesity (Silver Spring) 2020, 28, 860–869. [Google Scholar] [CrossRef]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Van Cauter, E.; Polonsky, K.S.; Scheen, A.J. Roles of circadian rhythmicity and sleep in human glucose regulation. Endocr. Rev. 1997, 18, 716–738. [Google Scholar]
- Morgan, L.; Hampton, S.; Gibbs, M.; Arendt, J. Circadian aspects of postprandial metabolism. Chronobiol. Int. 2003, 20, 795–808. [Google Scholar] [CrossRef]
- Clark, M.M.; Abrams, D.B.; Niaura, R.S.; Eaton, C.A.; Rossi, J.S. Self-efficacy in weight management. J. Consult. Clin. Psychol. 1991, 59, 739–744. [Google Scholar] [CrossRef]
- Horne, J.A.; Ostberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar] [PubMed]
- Hays, L.M.; Finch, E.A.; Saha, C.; Marrero, D.G.; Ackermann, R.T. Effect of self-efficacy on weight loss: A psychosocial analysis of a community-based adaptation of the diabetes prevention program lifestyle intervention. Diabetes Spectr. 2014, 27, 270–275. [Google Scholar] [CrossRef]
- Kant, A.K. Eating patterns of US adults: Meals, snacks, and time of eating. Physiol. Behav. 2018, 193 Pt B, 270–278. [Google Scholar] [CrossRef]
- Acharya, S.D.; Elci, O.U.; Sereika, S.M.; Music, E.; Styn, M.A.; Turk, M.W.; Burke, L.E. Adherence to a behavioral weight loss treatment program enhances weight loss and improvements in biomarkers. Patient Prefer Adherence 2009, 3, 151–160. [Google Scholar]
- Lemstra, M.; Bird, Y.; Nwankwo, C.; Rogers, M.; Moraros, J. Weight loss intervention adherence and factors promoting adherence: A meta-analysis. Patient Prefer Adherence 2016, 10, 1547–1559. [Google Scholar]
- Welton, S.; Minty, R.; O’Driscoll, T.; Willms, H.; Poirier, D.; Madden, S.; Kelly, L. Intermittent fasting and weight loss: Systematic review. Can. Fam. Physician 2020, 66, 117–125. [Google Scholar]
- Kesztyus, D.; Cermak, P.; Gulich, M.; Kesztyus, T. Adherence to Time-Restricted Feeding and Impact on Abdominal Obesity in Primary Care Patients: Results of a Pilot Study in a Pre-Post Design. Nutrients 2019, 11, 2854. [Google Scholar] [CrossRef]
- Lowe, D.A.; Wu, N.; Rohdin-Bibby, L.; Moore, A.H.; Kelly, N.; Liu, Y.E.; Philip, E.; Vittinghoff, E.; Heymsfield, S.B.; Olgin, J.E.; et al. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern. Med. 2020, 180, 1491–1499. [Google Scholar] [CrossRef]
- Wu, M.L.; Whittemore, A.S.; Jung, D.L. Errors in reported dietary intakes. II. Long-term recall. Am. J. Epidemiol. 1988, 128, 1137–1145. [Google Scholar] [CrossRef]
- Vaughan, K.L.; Mattison, J.A. Watch the Clock, Not the Scale. Cell Metab. 2018, 27, 1159–1160. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A.T.; Regmi, P.; Manoogian, E.N.C.; Fleischer, J.G.; Wittert, G.A.; Panda, S.; Heilbronn, L.K. Time-Restricted Feeding Improves Glucose Tolerance in Men at Risk for Type 2 Diabetes: A Randomized Crossover Trial. Obesity (Silver Spring) 2019, 27, 724–732. [Google Scholar] [CrossRef] [PubMed]
- Phillips, N.E.; Mareschal, J.; Schwab, N.; Manoogian, E.N.C.; Borloz, S.; Ostinelli, G.; Gauthier-Jaques, A.; Umwali, S.; Rodriguez, E.G.; Aeberli, D.; et al. The Effects of Time-Restricted Eating versus Standard Dietary Advice on Weight, Metabolic Health and the Consumption of Processed Food: A Pragmatic Randomised Controlled Trial in Community-Based Adults. Nutrients 2021, 13, 1042. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 50) | Eating Duration ≤14 h (n = 22) | Eating Duration >14 h (n = 28) | p-Value |
|---|---|---|---|---|
| Age, y | 51 ± 12 | 53 ± 13 | 50 ± 11 | 0.455 |
| Gender, % (n) | ||||
| Male | 18.0 (9) | 22.7 (5) | 14.3 (4) | 0.441 |
| Female | 82.0 (41) | 77.3 (17) | 85.7 (24) | |
| Non-Hispanic, % (n) | ||||
| Non-Hispanic | 62.0 (31) | 63.6 (14) | 60.7 (17) | 0.833 |
| Hispanic | 38.0 (19) | 36.4 (8) | 39.3 (11) | |
| Race, % (n) | ||||
| White | 56.0 (28) | 63.6 (14) | 50.0 (14) | 0.266 |
| Black | 42.0 (21) | 31.8 (7) | 50.0 (14) | |
| Asian | 2.0 (1) | 4.6 (1) | (0) | |
| Other | 0 (0) | (0) | (0) | |
| Height (cm) | 165.3 ± 6.7 | 164.0 ± 6.0 | 166.4 ± 7.2 | 0.218 |
| Weight (kg) | 92.1 ± 18.2 | 93.5 ± 17.7 | 91.1 ± 18.8 | 0.645 |
| + BMI (kg/m2) | 31.0 ± 10.8 | 33.1 ± 11.4 | 30.1 ± 9.2 | 0.287 |
| + SBP (mmHg) (n = 45) | 115.0 ± 20.0 | 120.0 ± 30.0 | 113.5 ± 20.0 | 0.881 |
| DBP (mmHg) (n = 45) | 75.2 ± 9.6 | 75.3 ± 9.7 | 75.1 ± 9.7 | 0.950 |
| + WC (cm) (n = 49) | 96.3 ± 15.7 | 95.3± 15.6 | 98.6 ± 16.6 | 0.968 |
| Chronotype Score (n = 47) | 55.0 ± 13.4 | 55.4 ± 11.7 | 54.8 ± 14.7 | 0.889 |
| Chronotype, % (n = 47) | ||||
| Morning Type | 40.4 (19) | 35.0 (7) | 44.4 (12) | 0.673 |
| Neither Type | 42.6 (20) | 50.0(10) | 37.0 (10) | |
| Evening Type | 17.0 (8) | 15.0 (3) | 18.5 (5) | |
| + EO/Day | 5.3 ± 3.2 | 3.6 ± 3.5 | 5.6 ± 2.1 | 0.027 |
| + Eating Duration | 14 h 18 m ± 2 h 48 m | 13 h 00 m± 2 h 00 m | 15 h 30 m ± 2 h 36 m | <0.001 |
| First EO Time (hh:mm) | 9:09 ± 3:05 | 9:20 ± 2:15 | 8:54 ± 3:47 | 0.003 |
| Final EO Time (hh:mm) | 20:16 ± 2:34 | 19:53 ± 2:14 | 20:32 ± 2:44 | 0.004 |
| + Logging Adherence (%) | 92.6 ± 28.6 | 85.2 ± 38.5 | 92.9 ± 21.4 | 0.134 |
| WEL Score (n = 41) | 125.3 ± 32.3 | 132.2 ±27.6 | 120.8 ± 34.8 | 0.269 |
| Variable | Pre-TRE | Post-TRE | p-Value + | Median of the % Change |
|---|---|---|---|---|
| Weight (kg) | 91.6 ± 17.1 | 90.1± 19.1 | 0.017 | −2.2 |
| BMI (kg/m2) | 29.4 ± 7.5 | 28.9 ± 8.7 | 0.017 | −2.3 |
| WC (cm) | 98.9 ± 10.7 | 96.9 ± 7.5 | 0.002 | −2.1 |
| * SBP (mmHg) | 124.0 ± 27.5 | 114.0 ± 17.3 | 0.002 | −10.1 |
| * DBP (mmHg) | 78.5 ± 9.3 | 75.0 ± 10.3 | 0.229 | −10.0 |
| Variable | Run-in | Intervention | p-Value |
|---|---|---|---|
| Eating Duration | 16 h 04 m ± 1 h 24 m | 11 h 54 m ± 2 h 06 m | <0.001 |
| First EO Time (hh:mm) | 8:56 ± 2:35 | 10:30 ± 2:23 | <0.001 |
| Final EO Time (hh:mm) | 20:14 ± 2:43 | 19:15 ± 2:35 | <0.001 |
| EO/Day | 6.3 ± 1.9 | 3.9 ± 1.5 | <0.001 |
| Logging Adherence (%) | 94 ± 10 | 64 ± 22 | <0.001 |
| Window Adherence (%) | N/A | 47 ± 19 | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prasad, M.; Fine, K.; Gee, A.; Nair, N.; Popp, C.J.; Cheng, B.; Manoogian, E.N.C.; Panda, S.; Laferrère, B. A Smartphone Intervention to Promote Time Restricted Eating Reduces Body Weight and Blood Pressure in Adults with Overweight and Obesity: A Pilot Study. Nutrients 2021, 13, 2148. https://doi.org/10.3390/nu13072148
Prasad M, Fine K, Gee A, Nair N, Popp CJ, Cheng B, Manoogian ENC, Panda S, Laferrère B. A Smartphone Intervention to Promote Time Restricted Eating Reduces Body Weight and Blood Pressure in Adults with Overweight and Obesity: A Pilot Study. Nutrients. 2021; 13(7):2148. https://doi.org/10.3390/nu13072148
Chicago/Turabian StylePrasad, Malini, Keenan Fine, Allen Gee, Nandini Nair, Collin J. Popp, Bin Cheng, Emily N. C. Manoogian, Satchidananda Panda, and Blandine Laferrère. 2021. "A Smartphone Intervention to Promote Time Restricted Eating Reduces Body Weight and Blood Pressure in Adults with Overweight and Obesity: A Pilot Study" Nutrients 13, no. 7: 2148. https://doi.org/10.3390/nu13072148
APA StylePrasad, M., Fine, K., Gee, A., Nair, N., Popp, C. J., Cheng, B., Manoogian, E. N. C., Panda, S., & Laferrère, B. (2021). A Smartphone Intervention to Promote Time Restricted Eating Reduces Body Weight and Blood Pressure in Adults with Overweight and Obesity: A Pilot Study. Nutrients, 13(7), 2148. https://doi.org/10.3390/nu13072148