
Saudi Arabia’s Healthy Food Strategy: Progress & Hurdles in the 2030 Road


 , , ,
, , ,
Abstract
:1. Introduction
2. Review of Nutrition Reforms Prior to the HFS Implementation
3. The HFS: Description of the Health Reforms
3.1. Display of Nutrition Information and Regulation of Juice Compositions in Food and Beverage Establishments
3.2. Front of Pack and Back of Pack Nutrition Labelling
3.3. Trans Fatty Acid Regulations
3.4. Restricting Sodium Content in Food Items
3.5. Sin Tax on all SSB
3.6. Educational Campaigns

{kind=link}
{kind=link}
| Policy Description and Reference | Type of Policies and Relevant Dates of Enactment and/or Enforcement | Key Collaborators | Policy Goal |
|---|---|---|---|
| Display of caloric information on food and beverage products in menus of food establishments (restaurants, hotels and coffee shops). SFDA.FD 20 [34] | Voluntary pledge in 2017 Enforced in 2019 | Food establishments (restaurants, hotels and coffee shop companies) | Empower individuals to make healthy decisions when eating out. |
| Declaration of allergens on food establishments’ menus. SFDA.FD 56 [36] | Issued in 2018 Enforced in 2019 | Food establishments (restaurants, hotels and coffee shops) | |
| Regulation of nutrient composition in fresh juices, nectars and fruit drinks and their display on products. SFDA.FD 5001 [37] | Issued in 2019 Enforced in 2020 | Food establishments (restaurants, hotels, coffee shops, juice shops and supermarkets that sell juices) | Encourage food and beverage establishments to withhold adding sugars to juices. Reduce consumption of sugars and empower individuals to make healthy choices while eating out. |
| Display of front of pack nutrition labels on prepackaged foods for sugar, sodium, saturated fat and total fat. Encourage the use of multiple traffic light labeling, a graphical illustration allowing individuals to understand nutrient composition from a color code. SFDA.FD 42 [40] | Voluntary scheme in 2018 | Food manufacturers | Encourage manufacturers to display nutrient content in a comprehensible way to consumers. Empower individuals to make healthy choices while shopping. Reduce consumption of added sugars. |
| Mandate for back of pack nutritional labels that display the added sugar, total cholesterol, fiber and TFA on prepackaged food items. SFDA.FD 2233 [42] | Issued in 2018 Enforced in 2021 | Food manufacturers | |
| Ban of all partially hydrogenated oils (PHO) in food manufacturing. SFDA.FD 2483 [29] | Issued in 2018 Enforced in 2020 | Food manufacturers | Encourage manufacturers to reformulate their products to reduce industrially produced TFA content. Reduce consumption of industrial TFA. |
| Mandate for a sodium limit for breads and (1 g/100 g) and ayran (yogurt drink) (1 g/100 g). SFDA.FD 2362 [43] SFDA.FD 57 [44] | Issued in 2018 Enforced in 2019 | Food manufacturers | Collaborate with manufacturers to reformulate their products to reduce sodium composition. Reduce sodium consumption. |
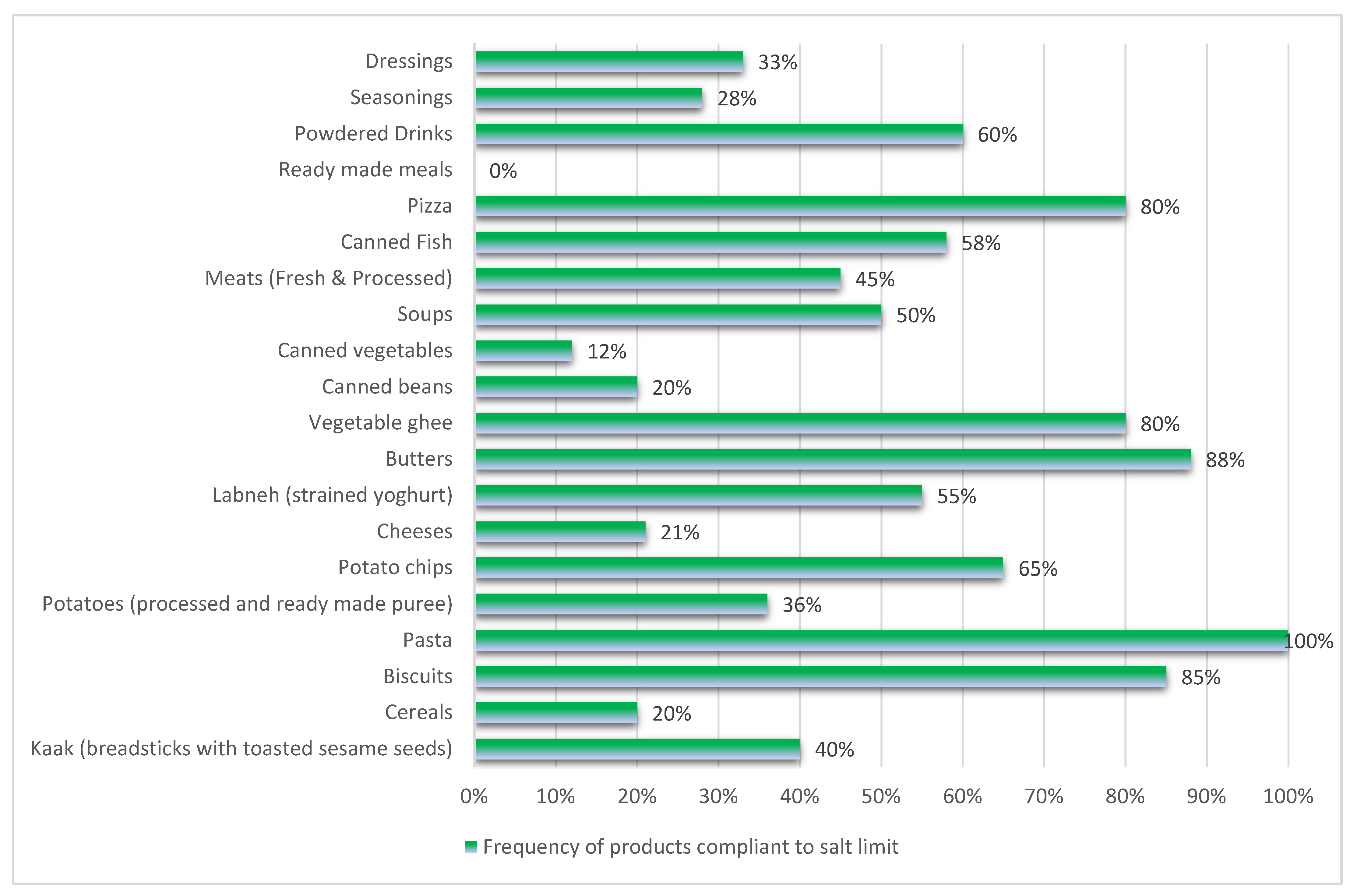
| Recommendation of a sodium limit for 22 processed food categories: cheeses, butter, fat spreads, beans, cooked and canned soups, ready meals, pizza, cakes, table sauces, biscuits, pasta, canned fish, meats, canned vegetables, chips, cooking sauces, potatoes, flavor enhancers and beverage powders. SFDA.FD 59 [46] | Voluntary scheme in 2018 | Food manufacturers | |
| Enforcement of a flat tax of 50% on all sugar-sweetened beverages, including carbonated drinks, juices, and dairy products [47]. | Enforced in 2019 | General Authority of Zakat, Tax and Customs | Reduce sugar-sweetened beverages consumption. |
4. Assessment of the HFS Acceptance and Implementation
4.1. Assessment of Nutrient and Allergens Information in Food Establishments
4.2. Front of Pack Nutrition Labels Evaluation
4.3. Surveillance of the Sodium Content in Breads and Food Products
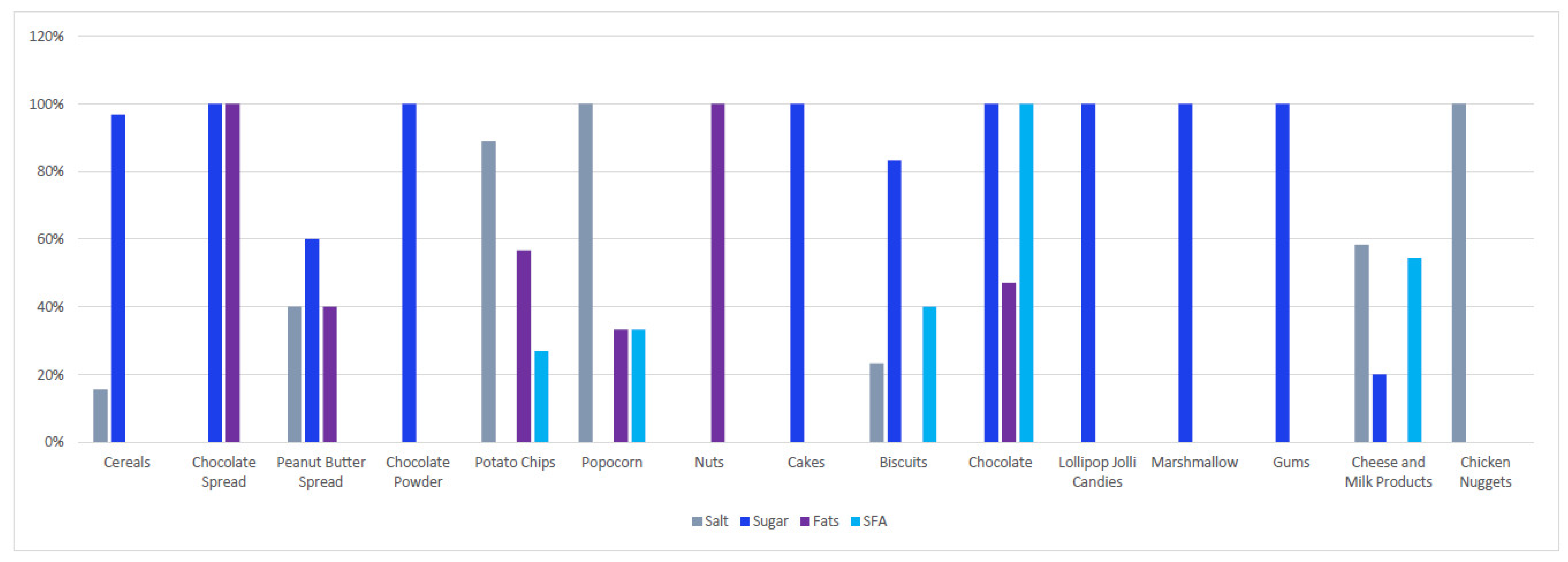
4.4. Surveillance of SSF in Children Food Products
4.5. Surveillance of TFA in Food Items
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Disclaimer
References
- Mozaffarian, D.; Angell, S.Y.; Lang, T.; Rivera, J.A. Role of government policy in nutrition—Barriers to and opportunities for healthier eating. BMJ 2018, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Tackling NCDs: ‘Best Buys’ and Other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Wilczek, M.M.; Olszewski, R.; Krupienicz, A. Trans-fatty acids and cardiovascular disease: Urgent need for legislation. Cardiology 2017, 138, 254–258. [Google Scholar] [CrossRef]
- Michels, N.; Van der Meulen, K.; Huybrechts, I. Dietary Trans Fatty Acid Intake in Relation to Cancer Risk: A Systematic Review; American Society of Clinical Oncology: Alexandria, VA, USA, 2018. [Google Scholar]
- WHO. Healthy Diet; World Health Organization: Cairo, Egypt, 2019. [Google Scholar]
- WHO. Countdown to 2023: WHO Report on Global Trans-Fat Elimination 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- He, F.J.; Brinsden, H.C.; MacGregor, G.A. Salt reduction in the United Kingdom: A successful experiment in public health. J. Hum. Hypertens. 2014, 28, 345–352. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, Distribution, and Its Current Association with Various Health Conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; BinDhim, N.F.; Alqahtani, S.A. Prevalence of Self-Reported Food Allergies and Their Association with Other Health Conditions among Adults in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 347. [Google Scholar] [CrossRef] [PubMed]
- Gelhorn, H.L.; Boye, K.S.; Shalhoub, H.; Matza, L.S.; Jordan, J.B.; Alhammad, A.; Anand, S.B.; Ekhzaimy, A.A.; Strizek, A. Patient-Reported Outcomes and Impact of Type 2 Diabetes: A Cross-Sectional Study in the Kingdom of Saudi Arabia. Patient Prefer. Adherence 2020, 14, 2231–2242. [Google Scholar] [CrossRef]
- Moradi-Lakeh, M.; El Bcheraoui, C.; Afshin, A.; Daoud, F.; AlMazroa, M.A.; Al Saeedi, M.; Basulaiman, M.; Memish, Z.A.; Al Rabeeah, A.A.; Mokdad, A.H. Diet in Saudi Arabia: Findings from a nationally representative survey. Public Health Nutr. 2017, 20, 1075–1081. [Google Scholar] [CrossRef] [Green Version]
- Tyrovolas, S.; El Bcheraoui, C.; Alghnam, S.A.; Alhabib, K.F.; Almadi, M.A.H.; Al-Raddadi, R.M.; Bedi, N.; El Tantawi, M.; Krish, V.S.; Memish, Z.A. The burden of disease in Saudi Arabia 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet Planet. Health 2020, 4, e195–e208. [Google Scholar] [CrossRef]
- WHO. Saudi Arabia: Country Profile; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Al-Raddadi, R.; Bahijri, S.M.; Jambi, H.A.; Ferns, G.; Tuomilehto, J. The prevalence of obesity and overweight, associated demographic and lifestyle factors, and health status in the adult population of Jeddah, Saudi Arabia. Ther. Adv. Chronic Dis. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-J.; Yeh, T.-L.; Shih, M.-C.; Tu, Y.-K.; Chien, K.-L. Dietary sodium intake and risk of cardiovascular disease: A systematic review and dose-response meta-analysis. Nutrients 2020, 12, 2934. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Li, Y.; Pan, A.; De Koning, L.; Schernhammer, E.; Willett, W.C.; Hu, F.B. Long-term consumption of sugar-sweetened and artificially sweetened beverages and risk of mortality in US adults. Circulation 2019, 139, 2113–2125. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (Ed.) World Health Survey Saudia Arabia; Ministry of Health: Riyadh, Saudi Arabia, 2021. [Google Scholar]
- Ataey, A.; Jafarvand, E.; Adham, D.; Moradi-Asl, E. The Relationship between Obesity, Overweight, and the Human Development Index in World Health Organization Eastern Mediterranean Region Countries. J. Prev. Med. Public Health 2020, 53, 98–105. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Eastern Mediterranean; Alwan, A.; McColl, K.; Al-Jawaldeh, A. Proposed Policy Priorities for Preventing Obesity and Diabetes in the Eastern Mediterranean Region; World Health Organization, Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2017. [Google Scholar]
- El Mouzan, M.I.; Foster, P.J.; Al Herbish, A.S.; Al Salloum, A.A.; Al Omer, A.A.; Qurachi, M.M.; Kecojevic, T. Prevalence of overweight and obesity in Saudi children and adolescents. Ann. Saudi Med. 2010, 30, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hussaini, A.; Bashir, M.S.; Khormi, M.; AlTuraiki, M.; Alkhamis, W.; Alrajhi, M.; Halal, T. Overweight and obesity among Saudi children and adolescents: Where do we stand today? Saudi J. Gastroenterol. Off. J. Saudi Gastroenterol. Assoc. 2019, 25, 229–235. [Google Scholar] [CrossRef]
- Aljaadi, A.; Alharbi, M. Overweight and Obesity Among Saudi Children: Prevalence, Lifestyle Factors, and Health Impacts; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Al-Qahtani, A.M. Prevalence and Predictors of Obesity and Overweight among Adults Visiting Primary Care Settings in the Southwestern Region, Saudi Arabia. Biomed. Res. Int. 2019, 2019, 8073057. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization; United Nations Development Programme. The Investment Case for Noncommunicable Disease Prevention and Control in Mongolia: Return on Investment Analysis and Institutional Context Analysis; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Saudi Food and Drug Authority. SFDA Launches Healthy Food Regulation Strategy Tomorrow. Available online: https://old.sfda.gov.sa/en/food/news/Pages/f11-9-2018a1.aspx#:~:text=SFDA%20will%20sign%20agreements%20for,and%20fat%20in%20their%20products (accessed on 3 March 2021).
- Nutrition, General Directorate of Nutrition. Dietary Guidelines for Saudis: The Healthy Food Palm; Ministry of Health, Ed.; Ministry of Health: Riyadh, Saudi Arabia, 2012; pp. 1–32.
- GSO. About GSO. Available online: https://www.gso.org.sa/en/about-gso/ (accessed on 28 March 2021).
- Moussa, H. Food and Agricultural Import Regulations and Standards Country Report, 1st ed.; Network, United States Department of Agriculture Foreign Agriculture Service and Global Agriculture Information Network; USDA: Washington, DC, USA, 2020. [Google Scholar]
- SFDA. Trans Fatty Acids; SFDA.FD 2483; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2016, 4, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Alsukait, R.; Bleich, S.; Wilde, P.; Singh, G.; Folta, S. Sugary drink excise tax policy process and implementation: Case study from Saudi Arabia. Food Policy 2020, 90, 101789. [Google Scholar] [CrossRef]
- Alsukait, R.; Wilde, P.; Bleich, S.N.; Singh, G.; Folta, S.C. Evaluating Saudi Arabia’s 50% carbonated drink excise tax: Changes in prices and volume sales. Econ. Hum. Biol. 2020, 38, 100868. [Google Scholar] [CrossRef]
- Megally, R.; Al-Jawaldeh, A. Impact of sin taxes on consumption volumes of sweetened beverages and soft drinks in Saudi Arabia [version 2; peer review: 2 approved]. F1000Research 2021, 9. [Google Scholar] [CrossRef]
- SFDA. Putting Calories on Food Establishments Menu’s Selling Away-From-Home Foods; SFDA FD 20; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2019. [Google Scholar]
- SFDA. Sourat. Available online: https://calories.sfda.gov.sa/ (accessed on 10 May 2021).
- SFDA. Declaration of Allergens on Food Establishments Menus; SFDA.FD 56; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- SFDA. Fresh Juices, Mixes and Beverages, Sold at Juice Stores, Restaurants and Cafes; SFDA FD 5001; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2019. [Google Scholar]
- Malam, S.; Clegg, S.; Kirwan, S.; McGinigal, S.; Raats, M.; Shepherd, R.; Barnett, J.; Senior, V.; Hodgkins, C.; Dean, M. Comprehension and Use of UK Nutrition Signpost Labelling Schemes; Food Standards Agency: London, UK, 2009. [Google Scholar]
- Al-Jawaldeh, A.; Rayner, M.; Julia, C.; Elmadfa, I.; Hammerich, A.; McColl, K. Improving Nutrition Information in the Eastern Mediterranean Region: Implementation of Front-of-Pack Nutrition Labelling. Nutrients 2020, 12, 330. [Google Scholar] [CrossRef]
- SFDA. Traffic Light Labeling; SFDA.FD 42; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- Scarborough, P.; Matthews, A.; Eyles, H.; Kaur, A.; Hodgkins, C.; Raats, M.M.; Rayner, M. Reds are more important than greens: How UK supermarket shoppers use the different information on a traffic light nutrition label in a choice experiment. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SFDA. Requirements of Nutritional Labeling; SFDA.FD 2233; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- SFDA. Technical Requirements of Bread Production; SFDA.FD 2362; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- SFDA. SFDA.FD 57: Laban, Flavoured Laban, and Laban Drink; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- Public Health England. Salt Reduction Targets for 2017; Crown: London, UK, 2017. [Google Scholar]
- SFDA. Salt Limits in Food Products; SFDA.FD 59; Saudi Food and Drug Authority: Riyadh, Saudi Arabia, 2018. [Google Scholar]
- Tax, General Authority of Zakat and Tax. Sin Taxation 2019; General Authority of Zakat and Tax: Riyadh, Saudi Arabia, 2019. [Google Scholar]
- United Nations. International Year of Fruits and Vegetables; Food and Agriculture Organization of the United Nations, Ed.; UN General Assembly: New York, NY, USA, 2021. [Google Scholar]
- Kamel, S.; Hala Al, O. Trans-Fats Declaration, Awareness and Consumption in Saudi Arabia. Curr. Res. Nutr. Food Sci. 2018, 6, 748–756. [Google Scholar] [CrossRef]
- Jradi, H.; AlMughthem, A.; Bawazir, A.A. Does the current Scope of nutrition labelling provided in the Saudi markets cope with the increasing trend of chronic disease? Res. Sq. 2020. [Google Scholar] [CrossRef] [Green Version]
- Alkhaldy, A.A.; Taha, D.S.; Alsahafi, S.E.; Naaman, R.K.; Alkhalaf, M.M. Response of the public and restaurant owners to the mandatory menu energy-labelling implementation in restaurants in Saudi Arabia. Public Health Nutr. 2020, 23, 3435–3447. [Google Scholar] [CrossRef] [PubMed]
- Hanbazaza, M.A.; Mumena, W.A. Knowledge and Practices Related to Salt Intake among Saudi Adults. Int. J. Environ. Res. Public Health 2020, 17, 5749. [Google Scholar] [CrossRef]
- Knowledge, attitudes, and practices toward added sugar consumption among female undergraduate students in Madinah, Saudi Arabia: A cross-sectional study. Nutrition 2020, 79–80. [CrossRef]
- Sami, R.; Bushnaq, T.; Benajiba, N.; Helal, M. Food consumption and lifestyle habits among university students in Saudi Arabia. Afr. J. Food Agric. Nutr. Dev. 2021, 21, 17711–17726. [Google Scholar] [CrossRef]
- Alfawaz, H.; Khan, N.; Alhuthayli, H.; Wani, K.; Aljumah, M.A.; Khattak, M.N.K.; Alghanim, S.A.; Al-Daghri, N.M. Awareness and Knowledge Regarding the Consumption of Dietary Fiber and Its Relation to Self-Reported Health Status in an Adult Arab Population: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 4226. [Google Scholar] [CrossRef]
- Al-Jawaldeh, A.; Hammerich, A.; Doggui, R.; Engesveen, K.; Lang, K.; McColl, K. Implementation of WHO Recommended Policies and Interventions on Healthy Diet in the Countries of the Eastern Mediterranean Region: From Policy to Action. Nutrients 2020, 12, 3700. [Google Scholar] [CrossRef]
- Al Jawaldeh, A.; Al-Khamaiseh, M. Assessment of salt concentration in bread commonly consumed in the Eastern Mediterranean Region. East. Mediterr. Health J. 2018, 24, 18–24. [Google Scholar] [CrossRef]
- MG, M.A. Traffic Light’ Labels to Guide Iranians toward Healthier Food. Tehran Times 7 May 2017. 2017. Available online: https://www.tehrantimes.com/news/413178/Traffic-light-labels-to-guide-Iranians-toward-healthier-food (accessed on 15 May 2021).
- Ghazavi, N.; Rahimi, E.; Esfandiari, Z.; Shakerian, A. Accuracy of the amount of trans-fatty acids in traffic light labelling of traditional sweets distributed in Isfahan, Iran. Arya Atheroscler. 2020, 16, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Esfandiari, Z.; Marasi, M.R.; Estaki, F.; Sanati, V.; Panahi, E.; Akbari, N.; Madani, R.A.; Mosberian Tanha, J. Influence of education on knowledge, attitude and practices of students of Isfahan University of Medical Sciences to traffic light inserted on food labeling. Tehran Univ. Med. J. Tums Publ. 2019, 77, 54–62. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin Sunaid, F.F.; Al-Jawaldeh, A.; Almutairi, M.W.; Alobaid, R.A.; Alfuraih, T.M.; Bensaidan, F.N.; Alragea, A.S.; Almutairi, L.A.; Duhaim, A.F.; Alsaloom, T.A.; et al. Saudi Arabia’s Healthy Food Strategy: Progress & Hurdles in the 2030 Road. Nutrients 2021, 13, 2130. https://doi.org/10.3390/nu13072130
Bin Sunaid FF, Al-Jawaldeh A, Almutairi MW, Alobaid RA, Alfuraih TM, Bensaidan FN, Alragea AS, Almutairi LA, Duhaim AF, Alsaloom TA, et al. Saudi Arabia’s Healthy Food Strategy: Progress & Hurdles in the 2030 Road. Nutrients. 2021; 13(7):2130. https://doi.org/10.3390/nu13072130
Chicago/Turabian StyleBin Sunaid, Faisal Fahad, Ayoub Al-Jawaldeh, Meshal Wasel Almutairi, Rawan Abdulaziz Alobaid, Tagreed Mohammad Alfuraih, Faisal Naser Bensaidan, Atheer Shayea Alragea, Lulu Ali Almutairi, Ali F. Duhaim, Talal Ali Alsaloom, and et al. 2021. "Saudi Arabia’s Healthy Food Strategy: Progress & Hurdles in the 2030 Road" Nutrients 13, no. 7: 2130. https://doi.org/10.3390/nu13072130
APA StyleBin Sunaid, F. F., Al-Jawaldeh, A., Almutairi, M. W., Alobaid, R. A., Alfuraih, T. M., Bensaidan, F. N., Alragea, A. S., Almutairi, L. A., Duhaim, A. F., Alsaloom, T. A., & Jabbour, J. (2021). Saudi Arabia’s Healthy Food Strategy: Progress & Hurdles in the 2030 Road. Nutrients, 13(7), 2130. https://doi.org/10.3390/nu13072130