
Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS)

 , , , , , ,
, , , , , ,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. The Latin American Health and Nutrition Survey (ELANS) Overview
2.2. Sample
2.3. Socio-Demographic Factors
2.4. Weight Status
2.5. Energy–Balance Related Behaviors (EBRB)
2.5.1. Sedentary Behaviors
2.5.2. Dietary Intake
2.5.3. Beverage Intake
2.6. Statistical Analysis
3. Results
3.1. Sample Characteristics
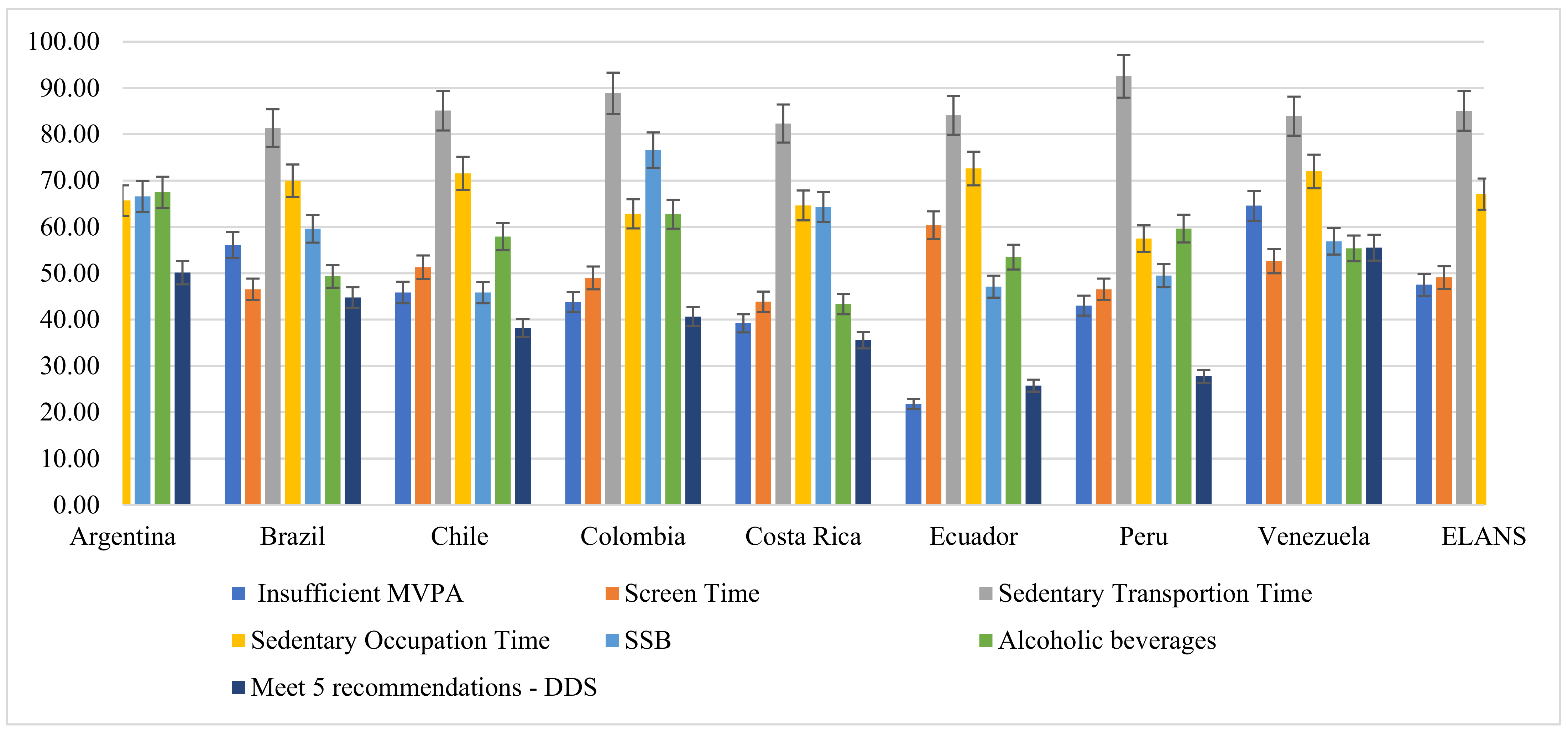
3.2. Individual Energy–Balance Related Behaviors (EBRB)
3.3. EBRB Clustering
3.4. EBRB and Socio-Demographic Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Kovalskys, I.; Fisberg, M.; Gomez, G.; Pareja, R.G.; Yepez Garcia, M.C.; Cortes Sanabria, L.Y.; Herrera-Cuenca, M.; Rigotti, A.; Guajardo, V.; Zalcman Zimberg, I.; et al. Energy intake and food sources of eight Latin American countries: Results from the Latin American Study of Nutrition and Health (ELANS). Public Health Nutr. 2018, 21, 2535–2547. [Google Scholar] [CrossRef]
- Finck Barboza, C.; Monteiro, S.M.; Barradas, S.C.; Sarmiento, O.L.; Rios, P.; Ramirez, A.; Mahecha, M.P.; Pratt, M. Physical activity, nutrition and behavior change in Latin America: A systematic review. Glob. Health Promot. 2013, 20, 65–81. [Google Scholar] [CrossRef]
- Malta, D.C.; Duncan, B.B.; Schmidt, M.I.; Teixeira, R.; Ribeiro, A.L.P.; Felisbino-Mendes, M.S.; Machado, Í.E.; Velasquez-Melendez, G.; Brant, L.C.C.; Silva, D.A.S.; et al. Trends in mortality due to non-communicable diseases in the Brazilian adult population: National and subnational estimates and projections for 2030. Popul. Health Metr. 2020, 18, 16. [Google Scholar] [CrossRef]
- Perez-Ferrer, C.; Auchincloss, A.H.; de Menezes, M.C.; Kroker-Lobos, M.F.; Cardoso, L.O.; Barrientos-Gutierrez, T. The food environment in Latin America: A systematic review with a focus on environments relevant to obesity and related chronic diseases. Public Health Nutr. 2019, 22, 3447–3464. [Google Scholar] [CrossRef] [PubMed]
- Dinkel, D.; Lu, K.; John, J.; Snyder, K.; Jacobson, L.T. A Cross-Sectional Examination of Physical Activity, Sedentary Time, and Sleep Between Adults with and without Children in the Home Using National Health and Nutrition Examination Survey. J. Phys. Act. Health 2021, 18, 391–399. [Google Scholar] [CrossRef]
- Du, Y.; Liu, B.; Sun, Y.; Snetselaar, L.G.; Wallace, R.B.; Bao, W. Trends in Adherence to the Physical Activity Guidelines for Americans for Aerobic Activity and Time Spent on Sedentary Behavior Among US Adults, 2007 to 2016. JAMA Netw. Open 2019, 2, e197597. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Mayne, S.L.; Virudachalam, S.; Fiks, A.G. Clustering of unhealthy behaviors in a nationally representative sample of U.S. children and adolescents. Prev. Med. 2020, 130, 105892. [Google Scholar] [CrossRef]
- Dieteren, C.M.; Brouwer, W.B.F.; van Exel, J. How do combinations of unhealthy behaviors relate to attitudinal factors and subjective health among the adult population in the Netherlands? BMC Public Health 2020, 20, 441. [Google Scholar] [CrossRef]
- Del Pozo Cruz, B.; McGregor, D.E.; Del Pozo Cruz, J.; Buman, M.P.; Palarea-Albaladejo, J.; Alfonso-Rosa, R.M.; Chastin, S.F.M. Integrating Sleep, Physical Activity, and Diet Quality to Estimate All-Cause Mortality Risk: A Combined Compositional Clustering and Survival Analysis of the National Health and Nutrition Examination Survey 2005–2006 Cycle. Am. J. Epidemiol. 2020, 189, 1057–1064. [Google Scholar] [CrossRef]
- Ding, D.; Rogers, K.; van der Ploeg, H.; Stamatakis, E.; Bauman, A.E. Traditional and Emerging Lifestyle Risk Behaviors and All-Cause Mortality in Middle-Aged and Older Adults: Evidence from a Large Population-Based Australian Cohort. PLoS Med. 2015, 12, e1001917. [Google Scholar] [CrossRef] [PubMed]
- Felez-Nobrega, M.; Raine, L.B.; Haro, J.M.; Wijndaele, K.; Koyanagi, A. Temporal trends in leisure-time sedentary behavior among adolescents aged 12–15 years from 26 countries in Asia, Africa, and the Americas. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 102. [Google Scholar] [CrossRef]
- Huybrechts, I.; Lioret, S.; Mouratidou, T.; Gunter, M.J.; Manios, Y.; Kersting, M.; Gottrand, F.; Kafatos, A.; de Henauw, S.; Cuenca-Garcia, M.; et al. Using reduced rank regression methods to identify dietary patterns associated with obesity: A cross-country study among European and Australian adolescents. Br. J. Nutr. 2017, 117, 295–305. [Google Scholar] [CrossRef]
- Batis, C.; Mazariegos, M.; Martorell, R.; Gil, A.; Rivera, J.A. Malnutrition in all its forms by wealth, education and ethnicity in Latin America: Who are more affected? Public Health Nutr. 2020, 23, s1–s12. [Google Scholar] [CrossRef] [PubMed]
- Salmon, C.T.; Nichols, J.S. The Next-Birthday Method of Respondent Selection. Public Opin. Q. 1983, 47, 270–276. [Google Scholar] [CrossRef]
- Encyclopedia of Survey Research Methods; Sage Publications: Newbury Park, CA, USA, 2008. [CrossRef]
- Fisberg, M.; Kovalskys, I.; Gomez, G.; Rigotti, A.; Cortes, L.Y.; Herrera-Cuenca, M.; Yepez, M.C.; Pareja, R.G.; Guajardo, V.; Zimberg, I.Z.; et al. Latin American Study of Nutrition and Health (ELANS): Rationale and study design. BMC Public Health 2016, 16, 93. [Google Scholar] [CrossRef] [PubMed]
- WHO. Adolescence Health: Overview; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- WHO. Body Mass Index—BMI; WHO: Copenhagen, Denmark, 2021. [Google Scholar]
- Loyen, A.; Chau, J.Y.; Jelsma, J.G.M.; van Nassau, F.; van der Ploeg, H.P. Prevalence and correlates of domain-specific sedentary time of adults in the Netherlands: Findings from the 2006 Dutch time use survey. BMC Public Health 2019, 19, 538. [Google Scholar] [CrossRef]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Harnack, L. Nutrition Data System for Research (NDSR). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1348–1350. [Google Scholar] [CrossRef]
- Kovalskys, I.; Fisberg, M.; Gomez, G.; Rigotti, A.; Cortes, L.Y.; Yepez, M.C.; Pareja, R.G.; Herrera-Cuenca, M.; Zimberg, I.Z.; Tucker, K.L.; et al. Standardization of the Food Composition Database Used in the Latin American Nutrition and Health Study (ELANS). Nutrients 2015, 7, 7914–7924. [Google Scholar] [CrossRef]
- Gomez, G.; Fisberg, R.M.; Nogueira Previdelli, A.; Hermes Sales, C.; Kovalskys, I.; Fisberg, M.; Herrera-Cuenca, M.; Cortes Sanabria, L.Y.; Garcia, M.C.Y.; Pareja Torres, R.G.; et al. Diet Quality and Diet Diversity in Eight Latin American Countries: Results from the Latin American Study of Nutrition and Health (ELANS). Nutrients 2019, 11, 1605. [Google Scholar] [CrossRef]
- Kennedy, G.; Ballard, T.; Dop, M.C. Guidelines for Measuring Household and Individual Dietary Diversity; Food and Agriculture Organization (FAO): Rome, Italy, 2013. [Google Scholar]
- Leme, A.C.; Muszynski, D.; Mirotta, J.A.; Carrol, N.; Hogan, J.; Jewell, K.; Yu, J.; Fisberg, R.; Duncan, A.; Ma, D.; et al. Diet quality of Canadian preschool children: Associations with socio-demographic characteristics. Can. Diet. J. Pract. Res. 2021, in press. [Google Scholar] [CrossRef]
- Food and Agriculture of the United Nations. Minimum Dietary Diversity for Women. In A Guide for Measurement; Food and Agriculture of the United Nations: Rome, Italy, 2016. [Google Scholar]
- Leme, A.C.; Baranowski, T.; Thompson, D.; Philippi, S.; O’Neil, C.E.; Fulgoni, V.L., 3rd; Nicklas, T.A. Food Sources of Shortfall Nutrients Among US Adolescents: National Health and Nutrition Examination Survey (NHANES) 2011–2014. Fam. Community Health 2020, 43, 59–73. [Google Scholar] [CrossRef] [PubMed]
- Leme, A.C.; Baranowski, T.; Thompson, D.; Philippi, S.; O’Neil, C.; Fulgoni, V.; Nicklas, T. Top food sources of percentage of energy, nutrients to limit and total gram amount consumed among US adolescents: National Health and Nutrition Examination Survey 2011–2014. Public Health Nutr. 2019, 22, 661–671. [Google Scholar] [CrossRef]
- Fausnacht, A.G.; Myers, E.A.; Hess, E.L.; Davy, B.M.; Hedrick, V.E. Update of the BEVQ-15, a beverage intake questionnaire for habitual beverage intake for adults: Determining comparative validity and reproducibility. J. Hum. Nutr. Diet. 2020, 33, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Fisberg, R.; Leme, A.C.; Nogueira, A.P.; Veroneze, A.M.; Arroyo, A.M.; Sales, C.H.; Gomez, G.S.; Kovalskys, I.; Cortes Sanabria, L.Y.; Herrera-Cuenca, M.; et al. Contribution of food groups to energy, grams, and nutrients-to-limit: The Latin American Study of Nutrition and Health/Estudio Latino Americano de Nutricíon y Salud (ELANS). Public Health Nutr. 2021, 24, 2424–2436, Accepted. [Google Scholar]
- Habinger, J.G.; Chavez, J.L.; Matsudo, S.M.; Kovalskys, I.; Gomez, G.; Rigotti, A.; Sanabria, L.Y.C.; Garcia, M.C.Y.; Pareja, R.G.; Herrera-Cuenca, M.; et al. Active Transportation and Obesity Indicators in Adults from Latin America: ELANS Multi-Country Study. Int J. Environ. Res. Public Health 2020, 17, 6974. [Google Scholar] [CrossRef]
- Perera, M.J.; Chirinos, D.A.; Brintz, C.E.; Schneiderman, N.; Daviglus, M.; Talavera, G.A.; Perreira, K.M.; Giacinto, R.A.E.; Qi, Q.; Llabre, M.M. Body Mass of U.S. Hispanics/Latinos From the Hispanic Community Health Study/Study of Latinos (HCHS/SOL): How Do Diet Quality and Sedentary Time Relate? Hisp. Health Care Int. 2020, 18, 55–63. [Google Scholar] [CrossRef]
- Werneck, A.O.; Baldew, S.S.; Miranda, J.J.; Diaz Arnesto, O.; Stubbs, B.; Silva, D.R.; South American Physical Activity and Sedentary Behavior Network (SAPASEN). Physical activity and sedentary behavior patterns and sociodemographic correlates in 116,982 adults from six South American countries: The South American physical activity and sedentary behavior network (SAPASEN). Int. J. Behav. Nutr. Phys. Act. 2019, 16, 68. [Google Scholar] [CrossRef]
- Mello, A.V.; Pereira, J.L.; Leme, A.C.B.; Goldbaum, M.; Cesar, C.L.G.; Fisberg, R.M. Social determinants, lifestyle and diet quality: A population-based study from the 2015 Health Survey of Sao Paulo, Brazil. Public Health Nutr. 2020, 23, 1766–1777. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. Relationship between lifestyle behaviors and obesity in children ages 9–11: Results from a 12-country study. Obesity 2015, 23, 1696–1702. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Moon, J.H.; Kim, H.J.; Kong, M.H.; Oh, Y.H. Sedentary Lifestyle: Overview of Updated Evidence of Potential Health Risks. Korean J. Fam Med. 2020, 41, 365–373. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Li, S.; Lichtenstein, A.H.; Chen, S.; Na, M.; Veldheer, S.; Xing, A.; Wang, Y.; Wu, S.; et al. Alcohol consumption and risk of cardiovascular disease, cancer and mortality: A prospective cohort study. Nutr. J. 2021, 20, 13. [Google Scholar] [CrossRef]
- Zheng, H.; Echave, P. Are Recent Cohorts Getting Worse? Trends in U.S. Adult Physiological Status, Mental Health, and Health Behaviors across a Century of Birth Cohorts. Am. J. Epidemiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Leme, A.C.; Philippi, S.T. The “Healthy Habits, Healthy Girls” randomized controlled trial for girls: Study design, protocol, and baseline results. Cad. Saude Publica 2015, 31, 1381–1394. [Google Scholar] [CrossRef]


{kind=link}
| Total | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | |
|---|---|---|---|---|---|---|---|---|---|
| Total n | 1266 | 2000 | 879 | 1230 | 798 | 800 | 1113 | 1132 | 9218 |
| Continuous variables (Mean ± SE) | |||||||||
| Age, years | 35.82 ± 0.15 | 36.77 ± 0.39 | 36.51 ± 0.31 | 36.42 ± 0.48 | 36.93 ± 0.42 | 35.21 ± 0.49 | 34.25 ± 0.49 | 34.19 ± 0.41 | 34.99 ± 0.41 |
| Body Mass Index, kg/m2 | 26.91 ± 0.06 | 27.09 ± 0.17 | 26.72 ± 0.13 | 28.08 ± 0.18 | 25.71 ± 0.14 | 27.65 ± 0.22 | 26.76 ± 0.19 | 26.65 ± 0.15 | 27.27 ± 0.17 |
| Weight, kg | 71.77 ± 0.17 | 73.56 ± 0.49 | 73.32 ± 0.38 | 74.96 ± 0.54 | 68.47 ± 0.43 | 73.11 ± 0.59 | 68.25 ± 0.51 | 67.46 ± 0.42 | 73.89 ± 0.51 |
| Height, cm | 163 ± 0.01 | 165 ± 0.00 | 165 ± 0.00 | 163 ± 0.00 | 163 ± 0.00 | 163 ± 0.00 | 160 ± 0.00 | 159 ± 0.00 | 164 ± 0.00 |
| TV time, minutes/day | 134.46 ± 1.18 | 136.06 ± 2.91 | 143.64 ± 2.99 | 114.95 ± 2.81 | 136.88 ± 3.39 | 178.87 ± 6.11 | 101.19 ± 2.43 | 136.76 ± 2.95 | 120.10 ± 2.28 |
| Computer time, minutes/day | 114.26 ± 2.31 | 96.72 ± 4.00 | 155.34 ± 7.23 | 105.48 ± 4.75 | 114.99 ± 5.78 | 153.29 ± 11.39 | 73.68 ± 3.63 | 105.65 ± 6.39 | 83.06 ± 3.30 |
| Videogame time, minutes/day | 90.26 ± 0.02 | 75.83 ± 6.61 | 114.56 ± 7.92 | 74.82 ± 7.63 | 87.79 ± 7.11 | 123.19 ± 9.46 | 70.00 ± 5.78 | 88.11 ± 7.64 | 72.31 ± 7.17 |
| Reading time, minutes/day | 55.29 ± 1.09 | 64.44 ± 3.00 | 71.81 ± 3.69 | 47.88 ± 2.99 | 56.35 ± 2.66 | 75.95 ± 5.23 | 38.13 ± 2.23 | 44.71 ± 1.74 | 39.51 ± 1.88 |
| Socializing with friends, minutes/day | 92.71 ± 1.15 | 107.04 ± 3.02 | 101.24 ± 2.77 | 73.09 ± 2.89 | 101.28 ± 3.46 | 133.17 ± 5.58 | 64.02 ± 2.53 | 74.90 ± 2.76 | 78.36 ± 2.36 |
| Talking on the phone, minutes/day | 45.48 ± 0.79 | 47.55 ± 1.88 | 48.07 ± 1.76 | 35.50 ± 2.26 | 53.46 ± 2.67 | 51.40 ± 3.19 | 30.46 ± 1.78 | 53.07 ± 2.25 | 34.66 ± 1.88 |
| Driving time, minutes/day | 87.25 ± 2.01 | 80.52 ± 4.48 | 77.58 ± 2.96 | 63.95 ± 3.87 | 102.78 ± 7.61 | 130.73 ± 10.53 | 79.61 ± 5.07 | 96.77 ± 10.71 | 95.53 ± 5.80 |
| Screen time a, minutes/day | 192.65 ± 1.95 | 188.98 ± 4.25 | 224.97 ± 5.61 | 178.46 ± 4.84 | 193.13 ± 5.25 | 238.11 ± 8.58 | 140.17 ± 3.97 | 187.60 ± 4.92 | 160.13 ± 3.34 |
| Leisure time b, minutes/day | 263.80 ± 2.42 | 272.78 ± 5.58 | 304.19 ± 6.73 | 229.18 ± 5.85 | 271.52 ± 6.69 | 331.73 ± 10.91 | 191.38 ± 5.00 | 244.47 ± 5.91 | 223.18 ± 4.37 |
| Total Energy Intake, kcal/day | 1992.93 ± 6.47 | 2181.07 ± 18.89 | 1835.55 ± 13.64 | 1732.72 ± 18.49 | 2130.43 ± 16.77 | 1886.07 ± 21.88 | 2212.55 ± 21.34 | 2111.04 ± 16.58 | 1917.83 ± 16.96 |
| Categorical variables (n (%)) | |||||||||
| Sex | |||||||||
| Female | 4809 (52.17) | 693 (54.74) | 1058 (52.90) | 454 (51.65) | 627 (50.98) | 404 (50.63) | 403 (50.38) | 590 (53.01) | 580 (51.24) |
| Male | 4409 (47.83) | 573 (45.26) | 942 (47.10) | 425 (48.35) | 603 (49.02) | 394 (49.37) | 397 (49.63) | 523 (46.99) | 552 (48.76) |
| Socio-economic status | |||||||||
| Low income | 3856 (41.83) | 616 (48.66) | 261 (13.05) | 411 (46.76) | 779 (63.33) | 262 (32.83) | 114 (14.25) | 533 (47.89) | 880 (77.74) |
| Middle income | 3946 (42.81) | 585 (46.21) | 1034 (51.70) | 388 (44.14) | 384 (31.22) | 428 (53.68) | 582 (72.75) | 355 (31.90) | 190 (16.78) |
| High income | 1416 (15.36) | 65 (5.13) | 705 (35.25) | 80 (9.10) | 67 (5.45) | 108 (13.53) | 104 (13.00) | 225 (20.22) | 62 (5.48) |
| Educational background | |||||||||
| Don’t study | 107 (1.16) | 3 (0.24) | 82 (4.10) | - | 11 (0.89) | 1 (0.13) | 2 (0.25) | 1 (0.09) | 7 (0.62) |
| ≤ high school | 8233 (89.31) | 1209 (95.50) | 1750 (87.50) | 780 (88.74) | 1082 (87.97) | 751 (94.11) | 746 (93.25) | 1003 (90.12) | 912 (80.57) |
| College/University degree | 878 (9.52) | 54 (4.27) | 168 (8.40) | 99 (11.26) | 137 (11.14) | 46 (5.76) | 52 (6.50) | 109 (9.79) | 213 (18.82) |
| Marital Status | |||||||||
| Single or living alone | 4825 (52.34) | 632 (49.92) | 1071 (53.55) | 473 (53.81) | 668 (54.31) | 430 (53.88) | 386 (48.25) | 526 (47.26) | 639 (56.45) |
| Married or living partner | 4393 (47.66) | 634 (50.08) | 929 (46.45) | 406 (46.19) | 562 (45.69) | 368 (46.12) | 414 (51.75) | 587 (52.74) | 493 (43.55) |
| Race/Ethnicity | |||||||||
| Caucasian | 3216 (36.74) | 856 (71.82) | 797 (41.27) | 279 (39.52) | 290 (25.33) | 394 (51.10) | 39 (4.88) | 96 (8.79) | 462 (41.51) |
| Non-Caucasian | 5537 (63.26) | 337 (28.18) | 1134 (58.73) | 427 (60.48) | 855 (74.67) | 377 (48.90) | 760 (95.12) | 996 (91.21) | 651 (58.49) |
| Weight Status | |||||||||
| Underweight | 306 (3.32) | 37 (2.92) | 87 (4.35) | 5 (0.57) | 59 (4.80) | 27 (3.38) | 28 (3.50) | 24 (2.18) | 39 (3.45) |
| Normal weight | 3420 (37.14) | 493 (38.94) | 749 (37.45) | 271 (30.83) | 548 (44.55) | 267 (33.46) | 288 (36.00) | 414 (37.53) | 390 (34.45) |
| Overweight | 3167 (34.39) | 399 (31.52) | 664 (33.20) | 332 (37.77) | 419 (34.07) | 260 (32.58) | 287 (35.88) | 422 (38.26) | 384 (33.92) |
| Obese | 2315 (25.14) | 337 (26.62) | 500 (25.00) | 271 (30.83) | 204 (16.59) | 244 (30.58) | 197 (24.63) | 243 (22.03) | 319 (28.18) |
| Screen-time | |||||||||
| Meeting | 4690 (50.88) | 670 (52.92) | 1069 (53.45) | 428 (48.69) | 627 (50.98) | 448 (56.14) | 317 (39.63) | 595 (53.46) | 536 (47.35) |
| Not meeting | 45.28 (49.12) | 596 (47.08) | 931 (46.55) | 451 (51.31) | 603 (49.02) | 350 (43.86) | 483 (60.38) | 518 (46.54) | 596 (52.65) |
| Leisure time | |||||||||
| Meeting | - | - | - | - | - | - | - | - | - |
| Not meeting | 9218 (100.00) | 1266 (100.00) | 2000 (100.00) | 879 (100.00) | 1230 (100.00) | 798 (100.00) | 800 (100.00) | 1113 (100.00) | 1132 (100.00) |
| Occupation | |||||||||
| Meeting | 3032 (32.89) | 434 (34.28) | 600 (30.00) | 250 (28.44) | 457 (37.15) | 282 (35.34) | 219 (27.38) | 473 (42.50) | 317 (28.00) |
| Not meeting | 6186 (67.11) | 832 (65.72) | 1400 (70.00) | 629 (71.56) | 773 (62.85) | 516 (64.66) | 581 (72.63) | 640 (57.50) | 815 (72.00) |
| Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS | |
|---|---|---|---|---|---|---|---|---|---|
| Total n | 1266 | 2000 | 879 | 1230 | 798 | 800 | 1113 | 1132 | 9218 |
| Number of unhealthy behaviors | |||||||||
| Clustering (≥2 unhealthy behaviors) | 48.74% | 39.50% | 35.49% | 49.27% | 45.36% | 33.88% | 40.97% | 34.28% | 41.25% |
| Prevalence of unhealthy behaviors pairs | |||||||||
| Screen time + occupation time | 19.43% | 18.75% | 15.36% | 20.81% | 21.43% | 13.38% | 25.52% | 15.19% | 18.94% |
| Screen time + transportation time | 9.08% | 11.75% | 7.74% | 6.10% | 10.90% | 9.38% | 4.49% | 8.75% | 8.72% |
| Screen time + poor diet | 26.46% | 29.65% | 31.06% | 29.84% | 35.46% | 29.88% | 38.54% | 22.44% | 30.08% |
| Screen time + SSB | 35.70% | 31.95% | 22.18% | 38.05% | 35.84% | 19.13% | 28.21% | 26.86% | 30.49% |
| Screen time + alcohol | 36.10% | 28.10% | 28.10% | 34.07% | 26.32% | 24.25% | 32.97% | 28.18% | 30.10% |
| Socialization with friends + screen time | 33.33% | 30.80% | 22.18% | 30.41% | 30.45% | 18.88% | 24.98% | 25.53% | 27.95% |
| Socialization with friends + occupation time | 20.85% | 17.25% | 12.29% | 21.46% | 19.17% | 11.13% | 18.24% | 12.63% | 17.02% |
| Socialization with friends + transportation time | 9.16% | 11.25% | 6.71% | 6.10% | 10.28% | 6.50% | 3.41% | 7.95% | 8.00% |
| Occupation time + Transportation time | 5.92% | 7.00% | 4.66% | 3.90% | 6.52% | 5.50% | 3.68% | 6.27% | 5.55% |
| Socialization with friends + poor diet | 28.20% | 26.20% | 20.93% | 29.59% | 32.23% | 25.13% | 26.68% | 21.38% | 26.33% |
| Socialization with friends + SSB | 37.05% | 29.80% | 16.27% | 37.32% | 32.71% | 17.38% | 19.68% | 26.15% | 28.01% |
| Socialization with friends + alcohol | 39.18% | 27.40% | 22.98% | 32.76% | 21.93% | 21.88% | 23.27% | 26.41% | 27.74% |
| Occupation time + poor diet | 18.48% | 18.35% | 17.75% | 24.55% | 24.31% | 20.63% | 30.73% | 12.72% | 20.66% |
| Occupation time + SSB | 21.17% | 17.90% | 12.63% | 27.15% | 22.56% | 12.83% | 21.56% | 16.87% | 19.34% |
| Occupation time + alcohol | 21.88% | 13.65% | 16.72% | 22.93% | 14.41% | 15.25% | 23.90% | 14.49% | 17.86% |
| Transportation time + poor diet | 8.53% | 11.70% | 9.44% | 6.91% | 11.90% | 13.00% | 5.03% | 8.30% | 9.32% |
| Transportation time + SSB | 10.43% | 11.25% | 8.08% | 8.54% | 12.28% | 7.38% | 3.95% | 10.51% | 9.25% |
| Transportation time + alcohol | 13.19% | 10.90% | 11.04% | 7.97% | 9.65% | 10.38% | 5.12% | 11.31% | 10.03% |
| Poor diet + SSB | 32.94% | 33.30% | 28.44% | 45.20% | 40.60% | 35.00% | 35.76% | 26.24% | 34.58% |
| Poor diet + alcohol | 34.52% | 26.95% | 37.54% | 36.75% | 28.95% | 39.88% | 42.86% | 26.33% | 33.45% |
| SSB + Alcohol | 45.50% | 30.15% | 29.12% | 48.29% | 28.45% | 28.75% | 31.81% | 33.22% | 34.89% |
| ELANS | Argentina | Brazil | Chile | Colombia | |
|---|---|---|---|---|---|
| OR (95%CI) | |||||
| Age (years) | 0.01 (0.01, 0.02) *** | 0.011 (0.00; 0.02) ** | 0.01 (0.01; 0.02) *** | −0.14 (−0.52, 0.24) | 0.02 (0.01, 0.03) *** |
| Sex | |||||
| Female | 0.59 (0.51, 0.68) *** | 0.55 (0.33, 0.78) *** | 0.59 (0.41, 0.77) *** | 0.56 (0.28, 0.84) *** | 0.59 (0.36, 0.82) *** |
| Male | Ref | Ref | Ref | Ref | Ref |
| Educational Background | |||||
| ≤ High school | 0.68 (0.54, 0.82) *** | 0.80 (0.21, 1.39) ** | 1.19 (0.86, 1.53) *** | 0.67 (0.21, 1.13) ** | 0.66 (0.28, 1.04) *** |
| College/University | Ref | Ref | Ref | Ref | Ref |
| Marital Status | |||||
| Single or living alone | 0.27 (0.35, 0.18) *** | 0.23 (0.45, −0.00) | 0.08 (0.27, −0.09) | 0.27 (0.58, −0.03) | 0.44 (0.67, 0.20) ** |
| Married or living with partner | Ref | ||||
| Race/Ethnicity | |||||
| White | 0.01 (−0.08, 0.09) | 0.34 (0.09, 0.59) ** | 0.04 (−0.14, 0.23) | 0.02 (−0.29, 0.34) | −0.05 (−0.30, 0.21) |
| Non-White | Ref | Ref | Ref | Ref | Ref |
| SES | |||||
| Low | 0.66 (0.53, 0.78) *** | 0.82 (0.30, 1.37) ** | 1.04 (0.73, 1.36) *** | 0.97 (0.49, 1.46) *** | 0.62 (0.11, 1.14) * |
| Middle | 0.40 (0.28, 0.53) *** | 0.54 (0.02, 1.09) * | 0.50 (0.31, 0.69) *** | 0.57 (0.09, 1.06) ** | 0.10 (−0.42, 0.64) |
| High | Ref | Ref | Ref | Ref | Ref |
| Weight Status | |||||
| Underweight | 0.15 (0.39, −0.10) | 0.03 (0.72, −0.66) | 0.07 (0.53, −0.40) | --- | 0.26 (0.84, −0.32) |
| Normal Weight | 0.18 (0.30, 0.08) ** | 0.23 (0.51, −0.04) | 0.07 (0.16, −0.30) | 0.52 (0.88, 0.15) ** | 0.25 (0.57, −0.07) |
| Overweight | 0.08 (0.19, −0.03) | 0.17 (0.46, −0.12) | 0.06 (0.29, −0.18) | 0.51 (0.88, 0.15) ** | 0.02 (0.36, −0.32) |
| Obese | Ref | Ref | Ref | Ref | Ref |
| Costa Rica | Ecuador | Peru | Venezuela | ||
| OR (95%CI) | |||||
| Age (years) | 0.02 (0.01, 0.03) ** | 0.02 (0.01, 0.03) *** | 0.01 (0.01, 0.02) ** | 0.01 (0.00, 0.02) * | |
| Sex | |||||
| Female | 0.74 (0.46, 1.03) *** | 0.88 (0.58, 1.18) *** | 0.66 (0.42, 0.90) *** | 0.42 (0.18, 0.67) ** | |
| Male | Ref | Ref | Ref | Ref | |
| Educational Background | |||||
| ≤High school | 0.64 (0.03, 1.26) * | 0.97 (0.39, 1.54) ** | 0.42 (0.02, 0.82) * | 0.66 (0.36, 0.97) *** | |
| College/University | Ref | Ref | Ref | Ref | |
| Marital Status | |||||
| Single or living alone | 0.42 (0.70, 0.13) ** | −0.47 (−0.77, −0.18) ** | −0.42 (−0.69, −0.21) ** | −0.05 (−0.31, 0.19) | |
| Married or living with partner | Ref | Ref | Ref | Ref | |
| Race/Ethnicity | |||||
| White | 0.14 (−0.14, 0.43) | 0.03 (−0.64, 0.74) | 0.27 (−0.17, 0.71) | 0.15 (−0.11, 0.39) | |
| Non-White | Ref | Ref | Ref | Ref | |
| SES | |||||
| Low | 0.96 (0.49, 1.42) *** | 1.26 (0.68, 1.85) *** | 0.95 (0.63, 1.26) *** | 0.57 (0.04, 1.08) * | |
| Middle | 0.20 (−0.23, 0.61) | 0.75 (0.33, 1.17) ** | 0.73 (0.39, 1.07) *** | 0.50 (−0.08, 1.08) | |
| High | Ref | Ref | Ref | Ref | |
| Weight Status | |||||
| Underweight | 0.19 (0.61, −1.03) | 0.05 (0.88, −0.84) | 0.77 (1.63, −0.08) | 0.39 (0.32, −1.16) | |
| Normal Weight | 0.07 (0.42, −0.28) | 0.39 (0.78, 0.01) * | 0.49 (0.81, 0.16) ** | 0.19 (0.12, −0.51) | |
| Overweight | 0.07 (0.29, −0.42) | 0.05 (−0.35, 0.44) | −0.09 (−0.42, 0.24) | 0.08 (0.23, −0.39) | |
| Obesity | Ref | Ref | Ref | Ref | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
B. Leme, A.C.; Ferrari, G.; Fisberg, R.M.; Kovalskys, I.; Gómez, G.; Cortes, L.Y.; Yépez Gárcia, M.C.; Herrera-Cuenca, M.; Rigotti, A.; Liria-Domínguez, M.R.; et al. Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS). Nutrients 2021, 13, 1809. https://doi.org/10.3390/nu13061809
B. Leme AC, Ferrari G, Fisberg RM, Kovalskys I, Gómez G, Cortes LY, Yépez Gárcia MC, Herrera-Cuenca M, Rigotti A, Liria-Domínguez MR, et al. Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS). Nutrients. 2021; 13(6):1809. https://doi.org/10.3390/nu13061809
Chicago/Turabian StyleB. Leme, Ana Carolina, Gerson Ferrari, Regina M. Fisberg, Irina Kovalskys, Georgina Gómez, Lilia Yadira Cortes, Martha Cecilia Yépez Gárcia, Marianella Herrera-Cuenca, Attilo Rigotti, María Reyna Liria-Domínguez, and et al. 2021. "Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS)" Nutrients 13, no. 6: 1809. https://doi.org/10.3390/nu13061809
APA StyleB. Leme, A. C., Ferrari, G., Fisberg, R. M., Kovalskys, I., Gómez, G., Cortes, L. Y., Yépez Gárcia, M. C., Herrera-Cuenca, M., Rigotti, A., Liria-Domínguez, M. R., & Fisberg, M. (2021). Co-Occurrence and Clustering of Sedentary Behaviors, Diet, Sugar-Sweetened Beverages, and Alcohol Intake among Adolescents and Adults: The Latin American Nutrition and Health Study (ELANS). Nutrients, 13(6), 1809. https://doi.org/10.3390/nu13061809