
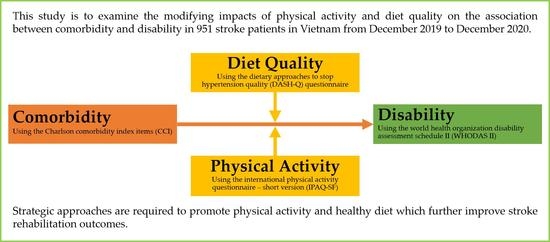
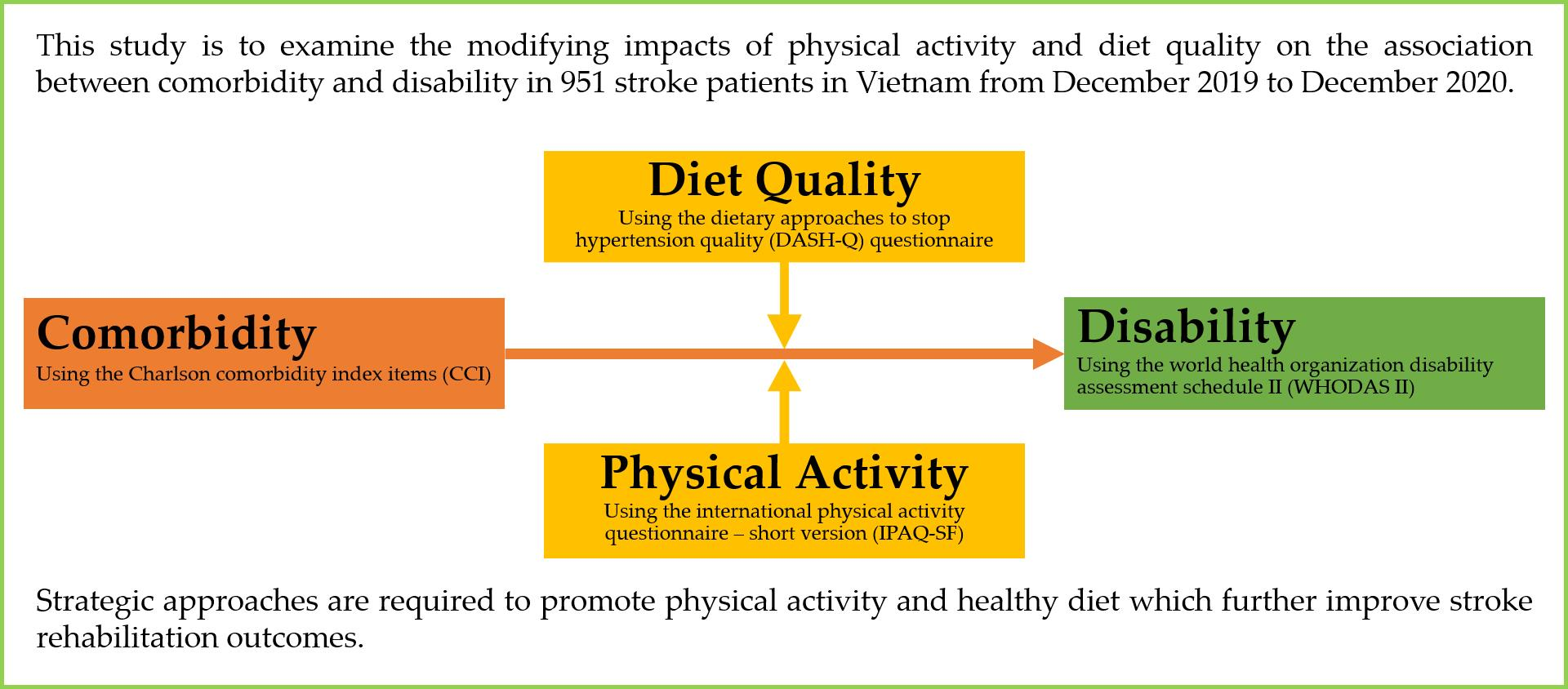
Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients

 , , , ,
, , , ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Sampling and Sample Size
2.3. Measurements
2.3.1. Patients’ Characteristics
2.3.2. Health-Related Behaviors
2.3.3. Clinical Parameters
2.3.4. Health Literacy
2.3.5. Diet Quality
2.3.6. Disability
2.4. Data Collection Procedure
2.5. Ethical Consideration
2.6. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Associations of Comorbidity, Physical Activity, Diet Quality with Disability
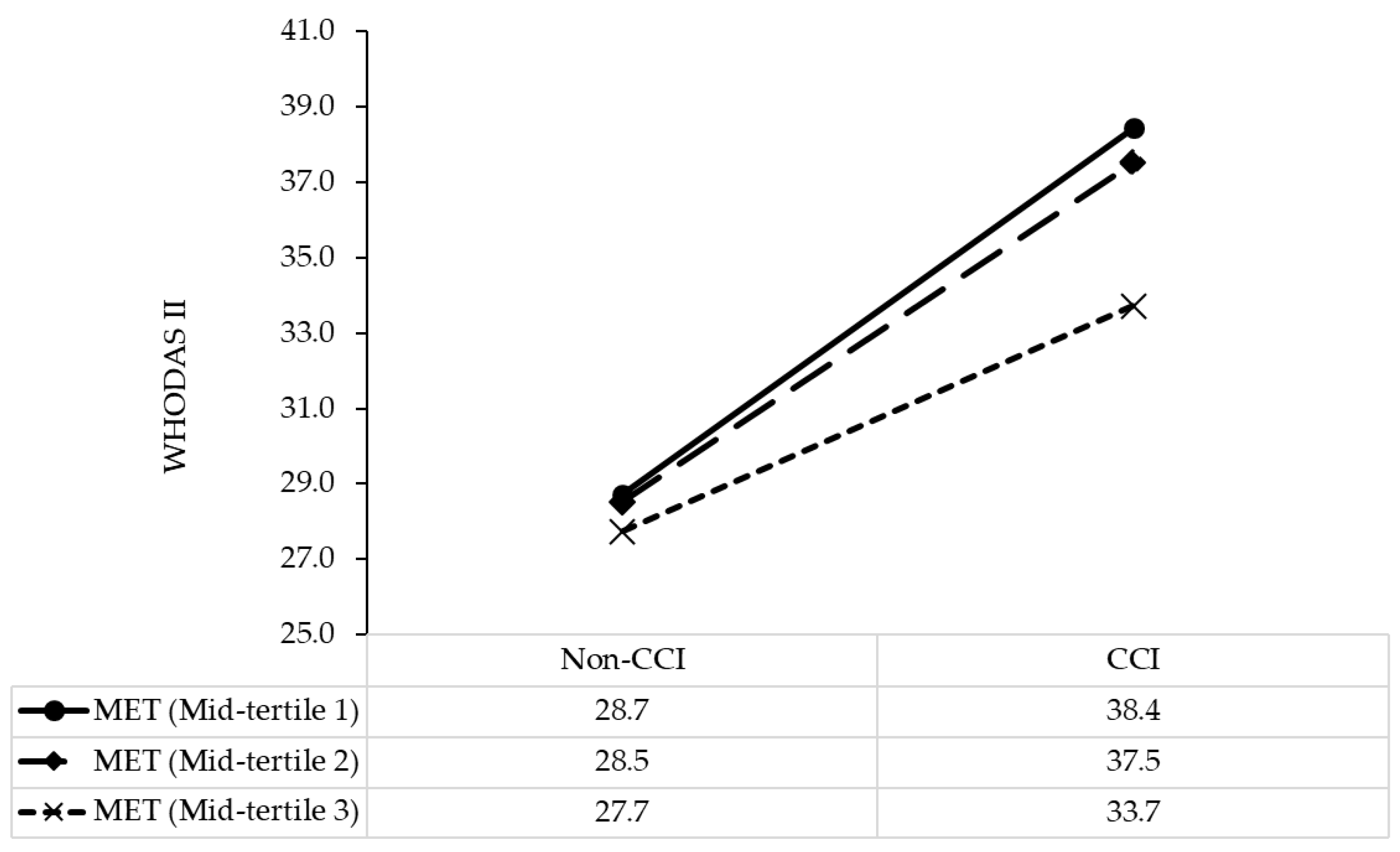
3.3. Modification Impacts of Physical Activity, Diet Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef]
- Feigin, V.L.; Krishnamurthi, R.V.; Parmar, P.; Norrving, B.; Mensah, G.A.; Bennett, D.A.; Barker-Collo, S.; Moran, A.E.; Sacco, R.L.; Truelsen, T.; et al. Update on the Global Burden of Ischemic and Hemorrhagic Stroke in 1990–2013: The GBD 2013 Study. Neuroepidemiology 2015, 45, 161–176. [Google Scholar] [CrossRef]
- Yamanashi, H.; Ngoc, M.Q.; Van Huy, T.; Suzuki, M.; Tsujino, A.; Toizumi, M.; Takahashi, K.; Thiem, V.D.; Anh, D.D.; Anh, N.T.H.; et al. Population-Based Incidence Rates of First-Ever Stroke in Central Vietnam. PLoS ONE 2016, 11, e0160665. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.L.; Blizzard, L.; Srikanth, V.; Thrift, A.G.; Lien, N.T.; Thang, N.H.; Gall, S.L. Case-fatality and functional status three months after first-ever stroke in Vietnam. J. Neurol. Sci. 2016, 365, 65–71. [Google Scholar] [CrossRef]
- Krishnamurthi, R.V.; Feigin, V.L.; Forouzanfar, M.H.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.M.; Truelsen, T.; et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet Glob. Health 2013, 1, e259–e281. [Google Scholar] [CrossRef]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics—2019 update: A report from the American heart association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, K.I.; Batty, G.D.; McLean, G.; Mercer, S.W.; Guthrie, B.; May, C.R.; Langhorne, P.; Mair, F.S. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: Implications for treatment burden. BMC Med. 2014, 12, 151. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Zomer, E.; Chin, K.L.; Si, S.; Markey, P.; Tacey, M.; Curtis, A.J.; Zoungas, S.; Liew, D. Effect of Comorbidity Assessed by the Charlson Comorbidity Index on the Length of Stay, Costs and Mortality among Older Adults Hospitalised for Acute Stroke. Int. J. Environ. Res. Public Health 2018, 15, 2532. [Google Scholar] [CrossRef]
- Mohamed, W.; Bhattacharya, P.; Shankar, L.; Chaturvedi, S.; Madhavan, R. Which Comorbidities and Complications Predict Ischemic Stroke Recovery and Length of Stay? Neurologist 2015, 20, 27–32. [Google Scholar] [CrossRef]
- Simić-Panić, D.; Bošković, K.; Milićević, M.; Žikić, T.R.; Bošnjak, M.C.; Tomašević-Todorović, S.; Jovićević, M. The Impact of Comorbidity on Rehabilitation Outcome after Ischemic Stroke. Acta Clin. Croat. 2018, 57, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Pandian, J.D.; Gall, S.L.; Kate, M.P.; Silva, G.S.; Akinyemi, R.O.; Ovbiagele, B.I.; Lavados, P.M.; Gandhi, D.B.C.; Thrift, A.G. Prevention of stroke: A global perspective. Lancet 2018, 392, 1269–1278. [Google Scholar] [CrossRef]
- Salehi-Abargouei, A.; Maghsoudi, Z.; Shirani, F.; Azadbakht, L. Effects of Dietary Approaches to Stop Hypertension (DASH)-style diet on fatal or nonfatal cardiovascular diseases—Incidence: A systematic review and meta-analysis on observational prospective studies. Nutrients 2013, 29, 611–618. [Google Scholar] [CrossRef]
- Struijk, E.A.; May, A.M.; Wezenbeek, N.L.; Fransen, H.P.; Soedamah-Muthu, S.S.; Geelen, A.; Boer, J.M.; van der Schouw, Y.T.; Bueno-De-Mesquita, H.B.; Beulens, J.W. Adherence to dietary guidelines and cardiovascular disease risk in the EPIC-NL cohort. Int. J. Cardiol. 2014, 176, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Paterson, K.E.; Myint, P.K.; Jennings, A.; Bain, L.K.; Lentjes, M.A.; Khaw, K.T.; Welch, A.A. Mediterranean Diet Reduces Risk of Incident Stroke in a Population With Varying Cardiovascular Disease Risk Profiles. Stroke 2018, 49, 2415–2420. [Google Scholar]
- Lin, P.-H.; Yeh, W.-T.; Svetkey, L.P.; Chuang, S.-Y.; Chang, Y.-C.; Wang, C.; Pan, W.-H. Dietary intakes consistent with the DASH dietary pattern reduce blood pressure increase with age and risk for stroke in a Chinese population. Asia Pac. J. Clin. Nutr. 2013, 22, 482–491. [Google Scholar]
- Chan, R.; Chan, D.; Woo, J. The association of a priori and a posterior dietary patterns with the risk of incident stroke in Chinese older people in Hong Kong. J. Nutr. Health Aging 2013, 17, 866–874. [Google Scholar] [CrossRef]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.; Bui, L.; Nguyen, A.; Nguyen, B.; Tran, P.; Vu, P.; Dang, L. The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PLoS ONE 2019, 14, e0221432. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Nurjanah, N.; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Su, T.T.; et al. Development and validation of a new short-form health literacy instrument (HLS-SF12) for the general public in six Asian countries. Health Lit. Res. Pract. 2019, 3, e91–e102. [Google Scholar] [CrossRef]
- Van Duong, T.; Chiu, C.-H.; Lin, C.-Y.; Chen, Y.-C.; Wong, T.-C.; Chang, P.W.S.; Yang, S.-H. E-healthy diet literacy scale and its relationship with behaviors and health outcomes in Taiwan. Health Promot. Int. 2021, 36, 20–33. [Google Scholar] [CrossRef] [PubMed]
- Van Duong, T.; Nguyen, T.T.P.; Pham, K.M.; Nguyen, K.T.; Giap, M.H.; Tran, T.D.X.; Nguyen, C.X.; Yang, S.-H.; Su, C.-T. Validation of the Short-Form Health Literacy Questionnaire (HLS-SF12) and Its Determinants among People Living in Rural Areas in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 3346. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.V.; Hoang, G.T.; Pham, V.T.; Duong, T.V.; Pham, K.M. Factors associated with health literacy among the elderly people in Vietnam. BioMed Res. Int. 2020, 2020, 1–7. [Google Scholar]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.; Do, B.; Pham, K.; Kim, G.; Dam, H.; Nguyen, T.; Nguyen, T.; Nguyen, Y.; Sørensen, K.; Pleasant, A.; et al. Fear of COVID-19 Scale—Associations of Its Scores with Health Literacy and Health-Related Behaviors among Medical Students. Int. J. Environ. Res. Public Health 2020, 17, 4164. [Google Scholar] [CrossRef] [PubMed]
- HLS-EU Consortium. Comparative Report of Health Literacy in Eight EU Member States. The European Health Literacy Project 2009–2012. Available online: https://www.healthliteracyeurope.net/hls-eu (accessed on 22 October 2012).
- Warren-Findlow, J.; Reeve, C.L.; Racine, E.F. Psychometric Validation of a Brief Self-report Measure of Diet Quality: The DASH-Q. J. Nutr. Educ. Behav. 2017, 49, 92–99.e1. [Google Scholar] [CrossRef]
- World Health Organization. WHO Disability Assessment Schedule 2.0 (WHODAS 2.0). Available online: https://www.who.int/classifications/icf/whodasii/en/ (accessed on 15 October 2019).
- Üstün, T.B.; Kostanjesek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule (WHODAS 2.0); World Health Organization: Geneva, Switzerland, 2010; 88p. [Google Scholar]
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; Von Korff, M.; Pull, C. Developing the World Health Organization Disability Assessment Schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef]
- Prime Minister of Vietnam. Gov’t Extends Social Distancing for at Least One Week in 28 Localities. Available online: http://news.chinhphu.vn/Home/Govt-extends-social-distancing-for-at-least-one-week-in-28-localities/20204/39735.vgp (accessed on 15 April 2020).
- Prime Minister of Vietnam. Gov’t to Gradually Ease COVID-19 Control Measure in Cautious Manner. Available online: http://primeminister.chinhphu.vn/Home/Govt-to-gradually-ease-COVID19-control-measure-in-cautious-manner/20204/3759.vgp (accessed on 20 April 2020).
- National Center for Immunization and Respiratory Diseases (NCIRD) Division of Viral Diseases. What Healthcare Personnel Should Know about Caring for Patients with Confirmed or Possible 2019-nCoV Infection. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/caring-for-patients.html (accessed on 7 February 2020).
- World Health Organization (WHO). Country & Technical Guidance—Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance (accessed on 10 February 2020).
- Ministry of Health. Coronavirus Disease (COVID-19) Outbreak in Vietnam. Available online: https://ncov.moh.gov.vn/ (accessed on 4 May 2020).
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017; pp. 120–141. [Google Scholar]
- IBM SPSS. IBM SPSS Statistics for Windows; Version 20.0; IBM Corp: New York, NY, USA, 2011. [Google Scholar]
- Denti, L.; Artoni, A.; Casella, M.; Giambanco, F.; Scoditti, U.; Ceda, G.P. Validity of the Modified Charlson Comorbidity Index as Predictor of Short-term Outcome in Older Stroke Patients. J. Stroke Cerebrovasc. Dis. 2015, 24, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Caballero, P.E.J.; Espuela, F.L.; Cuenca, J.C.P.; Moreno, J.M.R.; Zamorano, J.D.P.; Naranjo, I.C. Charlson Comorbidity Index in Ischemic Stroke and Intracerebral Hemorrhage as Predictor of Mortality and Functional Outcome after 6 Months. J. Stroke Cerebrovasc. Dis. 2013, 22, e214–e218. [Google Scholar] [CrossRef] [PubMed]
- Corraini, P.; Szépligeti, S.K.; Henderson, V.W.; Ording, A.G.; Horváth-Puhó, E.; Sørensen, H.T. Comorbidity and the increased mortality after hospitalization for stroke: A population-based cohort study. J. Thromb. Haemost. 2017, 16, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Rand, D.; Eng, J.J.; Tang, P.-F.; Hung, C.; Jeng, J.-S. Daily physical activity and its contribution to the health-related quality of life of ambulatory individuals with chronic stroke. Health Qual. Life Outcomes 2010, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Ezeugwu, V.E.; Manns, P.J. Sleep Duration, Sedentary Behavior, Physical Activity, and Quality of Life after Inpatient Stroke Rehabilitation. J. Stroke Cerebrovasc. Dis. 2017, 26, 2004–2012. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Brewster, S.; Wyke, S.; Gill, J.M.R.; Alexander, G.; Dybus, A.; Rafferty, D. Physical activity profiles and sedentary behaviour in people following stroke: A cross-sectional study. Disabil. Rehabil. 2015, 38, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Wondergem, R.; Veenhof, C.; Wouters, E.M.; De Bie, R.A.; Visser-Meily, J.M.; Pisters, M.F. Movement Behavior Patterns in People With First-Ever Stroke. Stroke 2019, 50, 3553–3560. [Google Scholar] [CrossRef] [PubMed]
- Kramer, S.F.; Hung, S.H.; Brodtmann, A. The Impact of Physical Activity Before and After Stroke on Stroke Risk and Recovery: A Narrative Review. Curr. Neurol. Neurosci. Rep. 2019, 19, 28. [Google Scholar] [CrossRef]
- Peçanha, T.; Goessler, K.F.; Roschel, H.; Gualano, B. Social isolation during the COVID-19 pandemic can increase physical inactivity and the global burden of cardiovascular disease. Am. J. Physiol. Circ. Physiol. 2020, 318, H1441–H1446. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef] [PubMed]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, CD009825. [Google Scholar] [CrossRef] [PubMed]
- Chareonrungrueangchai, K.; Wongkawinwoot, K.; Anothaisintawee, T.; Reutrakul, S. Dietary Factors and Risks of Cardiovascular Diseases: An Umbrella Review. Nutrients 2020, 12, 1088. [Google Scholar] [CrossRef] [PubMed]
- Chiavaroli, L.; Viguiliouk, E.; Nishi, S.K.; Blanco Mejia, S.; Rahelić, D.; Kahleová, H.; Salas-Salvadó, J.; Kendall, C.W.; Sievenpiper, J.L. DASH Dietary Pattern and Cardiometabolic Outcomes: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutrients 2019, 11, 338. [Google Scholar] [CrossRef]
- Lagström, H.; Stenholm, S.; Akbaraly, T.; Pentti, J.; Vahtera, J.; Kivimäki, M.; Head, J. Diet quality as a predictor of cardiometabolic disease–free life expectancy: The Whitehall II cohort study. Am. J. Clin. Nutr. 2020, 111, 787–794. [Google Scholar] [CrossRef]
- Glenn, A.J.; Viguiliouk, E.; Seider, M.; Boucher, B.A.; Khan, T.A.; Blanco Mejia, S.; Jenkins, D.J.A.; Kahleová, H.; Rahelić, D.; Salas-Salvadó, J.; et al. Relation of Vegetarian Dietary Patterns With Major Cardiovascular Outcomes: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. Front. Nutr. 2019, 6, 80. [Google Scholar] [CrossRef]
- Sakai, K.; Kinoshita, S.; Tsuboi, M.; Fukui, R.; Momosaki, R.; Wakabayashi, H. Effects of Nutrition Therapy in Older Stroke Patients Undergoing Rehabilitation: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2019, 23, 21–26. [Google Scholar] [CrossRef]
- Agarwal, P.; Wang, Y.; Buchman, A.S.; Bennett, D.A.; Morris, M.C. Dietary Patterns and Self-reported Incident Disability in Older Adults. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 74, 1331–1337. [Google Scholar] [CrossRef]
- Tanaka, T.; Talegawkar, S.; Jin, Y.; Bandinelli, S.; Ferrucci, L. Association of Adherence to the Mediterranean-Style Diet with Lower Frailty Index in Older Adults. Nutrients 2021, 13, 1129. [Google Scholar] [CrossRef]
- Huang, C.H.; Martins, B.A.; Okada, K.; Matsushita, E.; Uno, C.; Satake, S.; Kuzuya, M. A 3-year prospective cohort study of dietary patterns and frailty risk among community-dwelling older adults. Clin. Nutr. 2021, 40, 229–236. [Google Scholar] [CrossRef]
- Huang, C.H.; Okada, K.; Matsushita, E.; Uno, C.; Satake, S.; Martins, B.A.; Kuzuya, M. Dietary Patterns and Muscle Mass, Muscle Strength, and Physical Performance in the Elderly: A 3-Year Cohort Study. J. Nutr. Health Aging 2021, 25, 108–115. [Google Scholar] [CrossRef]
- Sato, Y.; Yoshimura, Y.; Abe, T. Nutrition in the First Week after Stroke Is Associated with Discharge to Home. Nutrients 2021, 13, 943. [Google Scholar] [CrossRef]
- Bonaccio, M.; Pounis, G.; Cerletti, C.; Donati, M.B.; Iacoviello, L.; De Gaetano, G.; MOLI-SANI Study Investigators. Mediterranean diet, dietary polyphenols and low grade inflammation: Results from the MOLI-SANI study. Br. J. Clin. Pharmacol. 2016, 83, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Zabetakis, I.; Lordan, R.; Norton, C.; Tsoupras, A. COVID-19: The Inflammation Link and the Role of Nutrition in Potential Mitigation. Nutrients 2020, 12, 1466. [Google Scholar] [CrossRef]
- Detopoulou, P.; Demopoulos, C.; Antonopoulou, S. Micronutrients, Phytochemicals and Mediterranean Diet: A Potential Protective Role against COVID-19 through Modulation of PAF Actions and Metabolism. Nutrients 2021, 13, 462. [Google Scholar] [CrossRef] [PubMed]
- Tsoupras, A.; Lordan, R.; Zabetakis, I. Thrombosis and COVID-19: The Potential Role of Nutrition. Front. Nutr. 2020, 7, 583080. [Google Scholar] [CrossRef]
- Fraiman, P.; Junior, C.G.; Moro, E.; Cavallieri, F.; Zedde, M. COVID-19 and Cerebrovascular Diseases: A Systematic Review and Perspectives for Stroke Management. Front. Neurol. 2020, 11, 574694. [Google Scholar] [CrossRef]
- Oliveira, D.M.G.; Aguiar, L.T.; Limones, M.V.D.O.; Gomes, A.G.; Da Silva, L.C.; Faria, C.D.C.D.M.; Scalzo, P.L. Aerobic Training Efficacy in Inflammation, Neurotrophins, and Function in Chronic Stroke Persons: A Randomized Controlled Trial Protocol. J. Stroke Cerebrovasc. Dis. 2019, 28, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Friedman, E.; Shorey, C. Inflammation in multimorbidity and disability: An integrative review. Health Psychol. 2019, 38, 791–801. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bise, T.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Yamaga, M.; Koga, H. Systemic Inflammation in the Recovery Stage of Stroke: Its Association with Sarcopenia and Poor Functional Rehabilitation Outcomes. Prog. Rehabil. Med. 2018, 3, 20180011. [Google Scholar] [CrossRef] [PubMed]
- Brummel, N.E.; Hughes, C.G.; Thompson, J.L.; Jackson, J.C.; Pandharipande, P.; McNeil, J.B.; Raman, R.; Orun, O.M.; Ware, L.B.; Bernard, G.R.; et al. Inflammation and Coagulation during Critical Illness and Long-Term Cognitive Impairment and Disability. Am. J. Respir. Crit. Care Med. 2021, 203, 699–706. [Google Scholar] [CrossRef] [PubMed]
- May, A.M.; Struijk, E.A.; Fransen, H.P.; Onland-Moret, N.C.; De Wit, G.A.; Boer, J.M.A.; Van Der Schouw, Y.T.; Hoekstra, J.; Bueno-De-Mesquita, H.B.; Peeters, P.H.M.; et al. The impact of a healthy lifestyle on Disability-Adjusted Life Years: A prospective cohort study. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef]
- Sánchez-Sánchez, E.; Ramírez-Vargas, G.; Avellaneda-López, Y.; Orellana-Pecino, J.I.; García-Marín, E.; Díaz-Jimenez, J. Eating Habits and Physical Activity of the Spanish Population during the COVID-19 Pandemic Period. Nutrients 2020, 12, 2826. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Ismail, L.C.; Osaili, T.M.; Mohamad, M.N.; Al Marzouqi, A.; Jarrar, A.H.; Abu Jamous, D.O.; Magriplis, E.; Ali, H.I.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Niewada, M.; Michel, P. Lifestyle modification for stroke prevention: Facts and fiction. Curr. Opin. Neurol. 2016, 29, 9–13. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Variables | Total | WHODAS II | p * |
|---|---|---|---|
| n (%) | (Mean ± SD) | ||
| Age, years | <0.001 | ||
| 19–59 | 285 (30.0) | 30.4 ± 13.1 | |
| 60–69 | 286 (30.1) | 31.2 ± 13.5 | |
| 70–79 | 222 (23.3) | 33.3 ± 13.4 | |
| 80–99 | 158 (16.6) | 36.5 ± 13.3 | |
| Gender | 0.035 | ||
| Women | 388 (40.8) | 33.5 ± 13.3 | |
| Men | 563 (59.2) | 31.6 ± 13.5 | |
| Marital status | 0.040 | ||
| Married | 837 (88.0) | 32.0 ± 13.6 | |
| Single or Widowed/Divorced/Separated | 114 (12.0) | 34.8 ± 12.4 | |
| Education attainment | 0.002 | ||
| Illiterate or elementary | 215 (22.6) | 34.4 ± 12.3 | |
| Junior high | 257 (27.1) | 33.6 ± 14.3 | |
| Senior high | 251 (26.4) | 31.4 ± 14.5 | |
| College/university or higher | 227 (23.9) | 30.1 ± 12.0 | |
| Occupation | <0.001 | ||
| Working | 518 (54.5) | 29.6 ± 12.9 | |
| Retired or infirmity | 433 (45.5) | 35.6 ± 13.4 | |
| Ability to pay for medication | 0.528 | ||
| Very or fairly difficult | 423 (44.5) | 32.7 ± 13.7 | |
| Very or fairly easy | 528 (55.5) | 32.1 ± 13.3 | |
| Social status | 0.344 | ||
| Low | 111 (11.7) | 33.5 ± 12.3 | |
| Middle or high | 840 (88.3) | 32.2 ± 13.6 | |
| BMI, kg/m2 | 0.203 | ||
| Underweight (<18.5) | 90 (9.5) | 33.5 ± 14.6 | |
| Normal weight (18.5 ≤ BMI < 24.0) | 794 (83.7) | 32.4 ± 13.4 | |
| Overweight/obese (BMI ≥ 25.0) | 65 (6.8) | 29.7 ± 12.8 | |
| CCI | <0.001 | ||
| None | 476 (50.1) | 28.1 ± 11.8 | |
| One or more | 475 (49.9) | 36.6 ± 13.8 | |
| Stroke occurrence | 0.261 | ||
| First ever | 785 (82.5) | 32.1 ± 13.2 | |
| Recurrent | 166 (17.5) | 33.4 ± 14.8 | |
| Smoking | 0.028 | ||
| Never smoked | 544 (57.2) | 31.5 ± 13.5 | |
| Ever smoked | 407 (42.8) | 33.5 ± 13.4 | |
| Drinking alcohol | 0.071 | ||
| No | 661 (69.5) | 32.9 ± 13.7 | |
| Yes | 290 (30.5) | 31.2 ± 13.0 | |
| Physical activity, MET-min/wk | <0.001 | ||
| Tertile 1 (MET ≤ 597) | 324 (34.1) | 38.4 ± 13.3 | |
| Tertile 2 (597 < MET ≤ 3726) | 312 (32.8) | 31.0 ± 13.2 | |
| Tertile 3 (MET > 3726) | 315 (33.1) | 27.5 ± 11.6 | |
| DASH-Q, mean ± SD | 29.2 ± 11.8 | ||
| HL index, mean ± SD | 23.4 ± 10.0 | ||
| WHODAS II, mean ± SD | 32.3 ± 13.5 |
| Variables | WHODAS II | WHODAS II | ||
|---|---|---|---|---|
| B (95%CI) * | p | B (95%CI) ** | p | |
| CCI | ||||
| None | Reference | Reference | ||
| One or more | 8.51 (6.88, 10.14) | <0.001 | 8.24 (6.66, 9.83) | <0.001 |
| Physical activity, MET-min/wk | ||||
| Tertile 1 | Reference | |||
| Tertile 2 | −7.40 (−9.37, −5.42) | <0.001 | −6.49 (−8.51, −4.47) | <0.001 |
| Tertile 3 | −10.82 (−12.80, −8.85) | <0.001 | −9.00 (−11.06, −6.94) | <0.001 |
| DASH-Q, 1-point increment | −0.27 (−0.34, −0.20) | <0.001 | −0.20 (−0.27, −0.13) | <0.001 |
| Interactions | WHODAS II | WHODAS II | ||
|---|---|---|---|---|
| B (95%CI) * | p | B (95%CI) ** | p | |
| CCI and MET | ||||
| Non-CCI × MET (tertile 1) | Reference | Reference | ||
| CCI × MET (tertile 1) | 10.70 (7.93, 13.47) | <0.001 | 10.67 (7.96, 13.37) | <0.001 |
| Non-CCI × MET (tertile 2) | −2.74 (−5.59, 0.11) | 0.059 | −2.50 (−5.31, 0.32) | 0.082 |
| Non-CCI × MET (tertile 3) | −6.23 (−9.08, −3.39) | <0.001 | −4.56 (−7.40, −1.72) | 0.002 |
| CCI × MET (tertile 2) | −5.47 (−9.37, −1.58) | 0.006 | −4.65 (−8.44, −0.85) | 0.016 |
| CCI × MET (tertile 3) | −5.39 (−9.27, −1.50) | 0.007 | −5.48 (−9.27, −1.70) | 0.005 |
| CCI and DASH-Q | ||||
| Non-CCI × DASH-Q (lowest score) | ||||
| CCI × DASH-Q (lowest score) | 18.62 (14.36, 22.88) | <0.001 | 17.12 (12.98, 21.45) | <0.001 |
| Non-CCI × DASH-Q (1-point increment) | −0.03 (−0.13, 0.07) | 0.523 | −0.01 (−0.09, 0.09) | 0.990 |
| CCI × DASH-Q (1-point increment) | −0.37 (−0.51, −0.24) | <0.001 | −0.32 (−0.45, −0.19) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, L.T.K.; Do, B.N.; Vu, D.N.; Pham, K.M.; Vu, M.-T.; Nguyen, H.C.; Tran, T.V.; Le, H.P.; Nguyen, T.T.P.; Nguyen, Q.M.; et al. Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients. Nutrients 2021, 13, 1641. https://doi.org/10.3390/nu13051641
Nguyen LTK, Do BN, Vu DN, Pham KM, Vu M-T, Nguyen HC, Tran TV, Le HP, Nguyen TTP, Nguyen QM, et al. Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients. Nutrients. 2021; 13(5):1641. https://doi.org/10.3390/nu13051641
Chicago/Turabian StyleNguyen, Lien T. K., Binh N. Do, Dinh N. Vu, Khue M. Pham, Manh-Tan Vu, Hoang C. Nguyen, Tuan V. Tran, Hoang P. Le, Thao T. P. Nguyen, Quan M. Nguyen, and et al. 2021. "Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients" Nutrients 13, no. 5: 1641. https://doi.org/10.3390/nu13051641
APA StyleNguyen, L. T. K., Do, B. N., Vu, D. N., Pham, K. M., Vu, M.-T., Nguyen, H. C., Tran, T. V., Le, H. P., Nguyen, T. T. P., Nguyen, Q. M., Tran, C. Q., Nguyen, K. T., Yang, S.-H., Chao, J. C.-J., & Van Duong, T. (2021). Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients. Nutrients, 13(5), 1641. https://doi.org/10.3390/nu13051641