
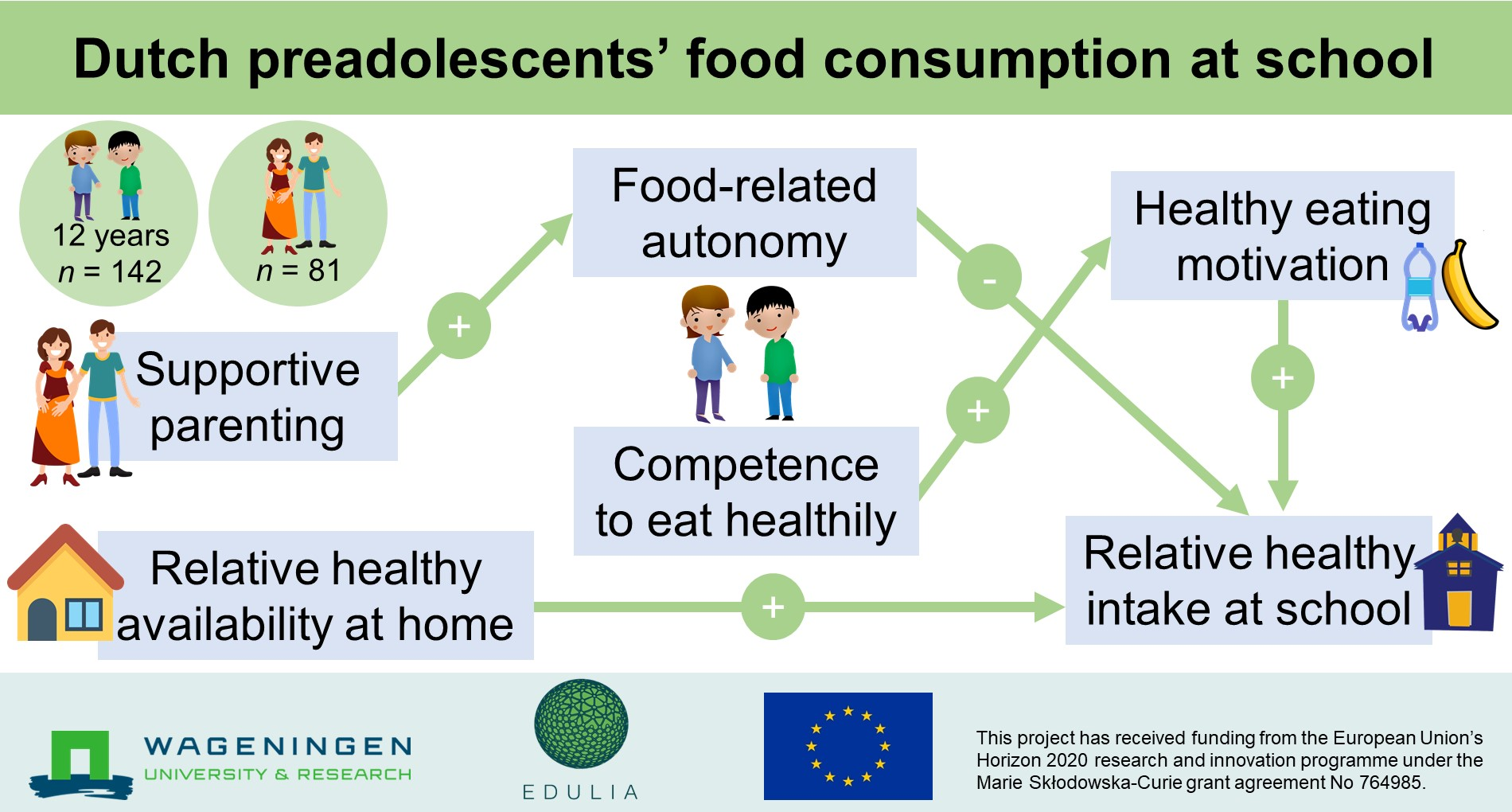
Dutch Preadolescents’ Food Consumption at School: Influence of Autonomy, Competence and Parenting Practices


Abstract

1. Introduction
- RQ1: How are food-related autonomy and competence to eat healthily perceived by preadolescents and parents?
- RQ2: How can parents support preadolescents’ food-related autonomy and competence, and what are the direct and indirect effects on their motivation to eat healthily and their healthy food consumption at school?
- RQ3: How does the relative availability of healthy foods at home influence preadolescents’ food consumption at school?
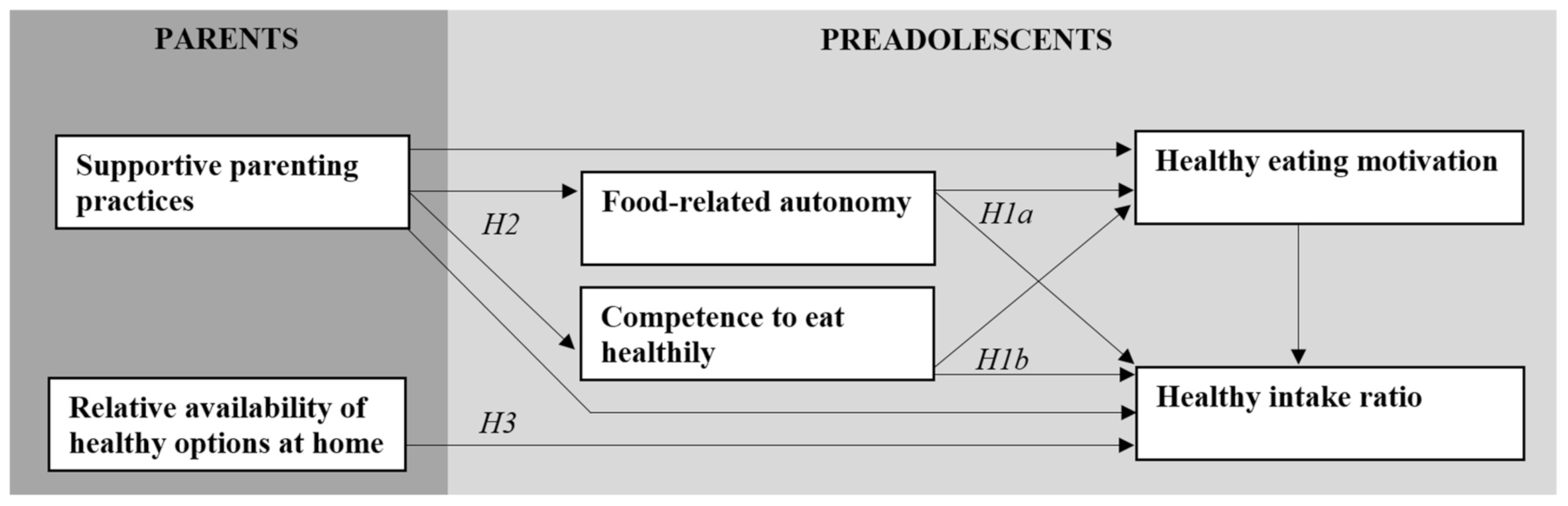
1.1. Theoretical Background and Hypotheses
1.1.1. Food-Related Autonomy and Competence to Make Healthy Food Choices
1.1.2. Supportive Parenting Practices Promoting Food-Related Autonomy and Competence
1.1.3. Relative Availability of Healthy Foods in the Home
2. Materials and Methods
2.1. Procedures
2.2. Measures Preadolescents
2.2.1. Healthy Intake Ratio
2.2.2. Food-Related Autonomy
2.2.3. Competence to Eat Healthily
2.2.4. Healthy Eating Motivation
2.2.5. School Environment and Eating Characteristics
2.3. Measures Parents
2.3.1. Food-Related Autonomy
2.3.2. Competence to Eat Healthily
2.3.3. Supportive Parenting Practices
2.3.4. Relative Availability of Healthy Options at Home
2.3.5. School Environment and Eating Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parenting Practice | Items | Source |
|---|---|---|
| Autonomy support | 1: I encourage my child to be curious, to explore, and to question things | Autonomy support subscale—Comprehensive General Parenting Questionnaire [83] |
| 2: I trust my child | ||
| 3: I respect my child’s opinion and encourage him/her to express it | ||
| 4: I encourage my child to be true to himself/herself | ||
| 5: I encourage my child to express his/her opinions even when I do not agree with him/her | ||
| Responsiveness | 6: I know exactly when things are not going very well for my child | Responsiveness subscale—Comprehensive General Parenting Questionnaire [83] |
| 7: When my child is sad, I know what is going on with him/her | ||
| 8: I feel good about the relationship I have with my child | ||
| 9: My child and I have warm affectionate moments together | ||
| 10: I know exactly when my child has difficulty with something | ||
| Encouraging healthy food intake | 11: I encourage my child to drink water a | Comprehensive Snack Parenting Questionnaire [84], adapted by focusing on specific healthy eating behaviors |
| 12: I encourage my child to eat fruits and vegetables b | ||
| Making healthy foods accessible | 13: I make sure my child has easy access to healthy foods c | Comprehensive Snack Parenting Questionnaire [84] |
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Descriptives
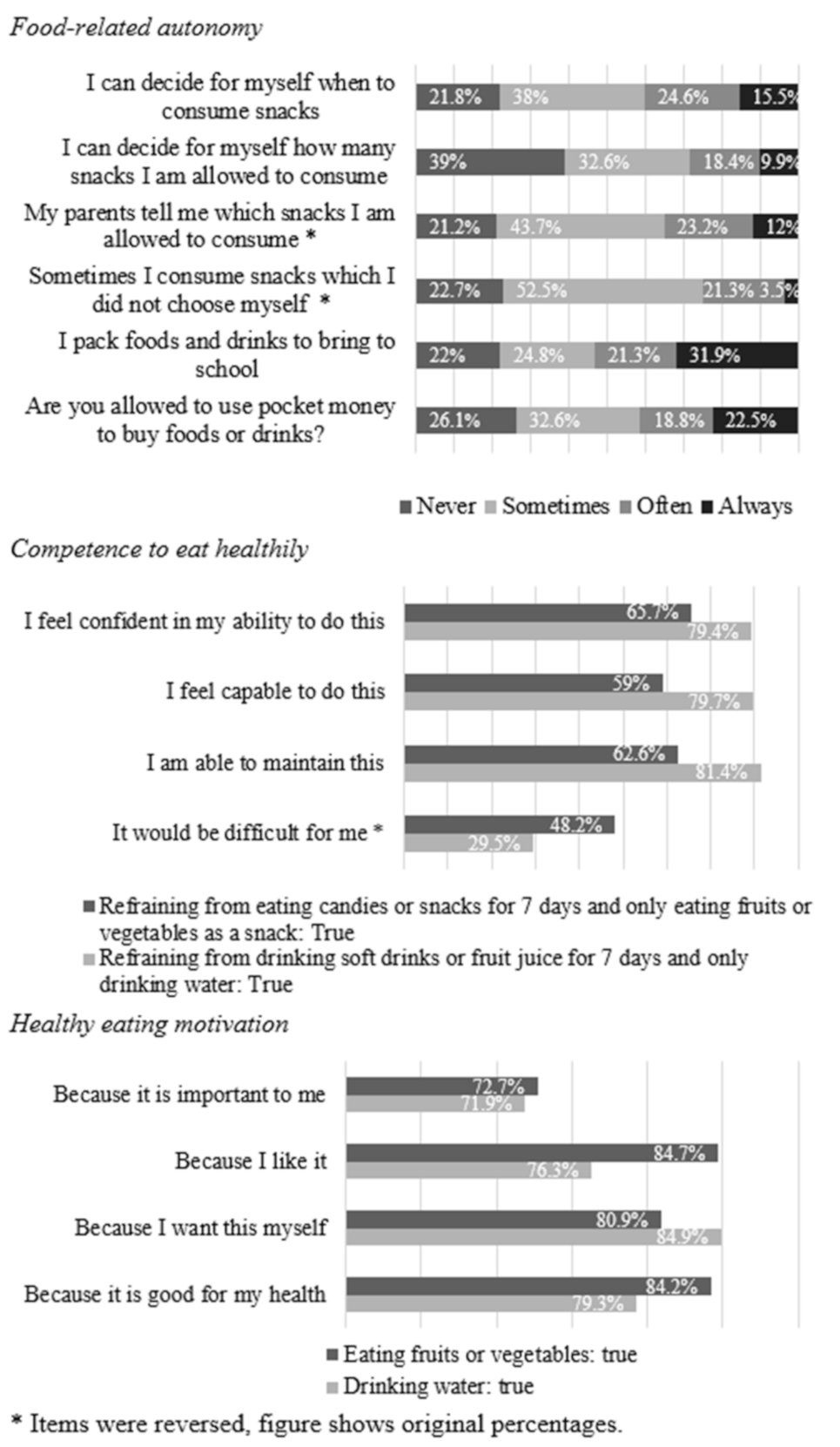
3.3. Preadolescents’ and Parents’ Perceptions of Food-Related Autonomy and Competence
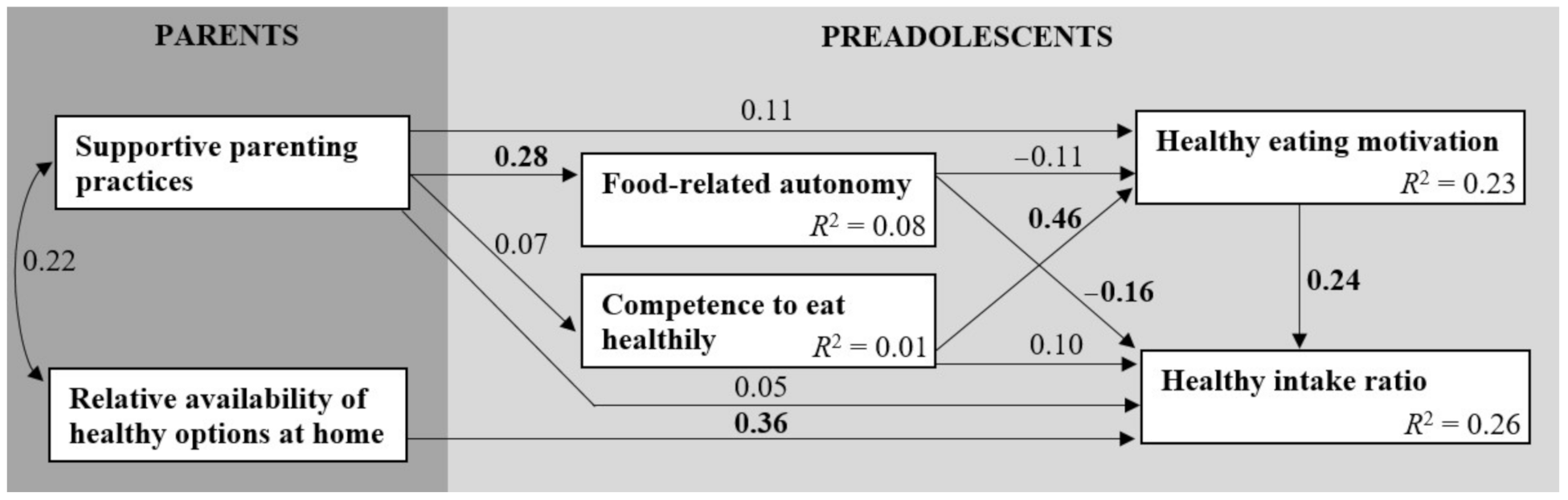
3.4. Effects of Food-Related Autonomy and Competence
3.5. Parenting Practices Supporting Food-Related Autonomy and Competence
3.6. Effect of Relative Availability of Healthy Options at Home
3.7. School Environment and Eating Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lytle, L.A.; Seifert, S.; Greenstein, J.; McGovern, P. How Do Children’s Eating Patterns and Food Choices Change over Time? Results from a Cohort Study. Am. J. Health Promot. 2000, 14, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Winpenny, E.M.; Corder, K.L.; Jones, A.; Ambrosini, G.L.; White, M.; Van Sluijs, E.M. Changes in diet from age 10 to 14 years and prospective associations with school lunch choice. Appetite 2017, 116, 259–267. [Google Scholar] [CrossRef]
- Albani, V.; Butler, L.T.; Traill, W.B.; Kennedy, O.B. Fruit and vegetable intake: Change with age across childhood and adolescence. Br. J. Nutr. 2017, 117, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Cruz, F.; Ramos, E.; Lopes, C.; Araújo, J. Tracking of food and nutrient intake from adolescence into early adulthood. Nutrition 2018, 55-56, 84–90. [Google Scholar] [CrossRef]
- Hu, T.; Jacobs, D.R., Jr.; Larson, N.I.; Cutler, G.J.; Laska, M.N.; Neumark-Sztainer, D. Higher Diet Quality in Adolescence and Dietary Improvements Are Related to Less Weight Gain during the Transition from Adolescence to Adulthood. J. Pediatr. 2016, 178, 188–193.e3. [Google Scholar] [CrossRef] [PubMed]
- Reicks, M.; Banna, J.C.; Cluskey, M.; Gunther, C.; Hongu, N.; Richards, R.; Topham, G.; Wong, S.S. Influence of Parenting Practices on Eating Behaviors of Early Adolescents during Independent Eating Occasions: Implications for Obesity Prevention. Nutrition 2015, 7, 8783–8801. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Afifi, R.; Bearinger, L.H.; Blakemore, S.-J.; Dick, B.; Ezeh, A.C.; Patton, G.C. Adolescence: A foundation for future health. Lancet 2012, 379, 1630–1640. [Google Scholar] [CrossRef]
- Banna, J.; Richards, R.; Jones, B.; Anderson, A.K.; Reicks, M.; Cluskey, M.; Gunther, C.; Hongu, N.K.; Lora, K.; Misner, S.; et al. Describing Independent Eating Occasions among Low-Income Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 981. [Google Scholar] [CrossRef] [PubMed]
- Briefel, R.R.; Wilson, A.; Gleason, P.M. Consumption of Low-Nutrient, Energy-Dense Foods and Beverages at School, Home, and Other Locations among School Lunch Participants and Nonparticipants. J. Am. Diet. Assoc. 2009, 109, S79–S90. [Google Scholar] [CrossRef]
- Story, M.; Neumark-Sztainer, D.; French, S. Individual and Environmental Influences on Adolescent Eating Behaviors. J. Am. Diet. Assoc. 2002, 102, S40–S51. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The general causality orientations scale: Self-determination in personality. J. Res. Pers. 1985, 19, 109–134. [Google Scholar] [CrossRef]
- Joussemet, M.; Landry, R.; Koestner, R. A self-determination theory perspective on parenting. Can. Psychol. Can. 2008, 49, 194–200. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.X.; Ullah, S.; Magarey, A.; Miller, J.; Leslie, E. Relationship between the home environment and fruit and vegetable consumption in children aged 6–12 years: A systematic review. Public Health Nutr. 2016, 20, 464–480. [Google Scholar] [CrossRef]
- Verstuyf, J.; Patrick, H.; Vansteenkiste, M.; Teixeira, P.J. Motivational dynamics of eating regulation: A self-determination theory perspective. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.Y.Y.; Ntoumanis, N.; Thøgersen-Ntoumani, C.; Deci, E.L.; Ryan, R.M.; Duda, J.L.; Williams, G.C. Self-Determination Theory Applied to Health Contexts. Perspect. Psychol. Sci. 2012, 7, 325–340. [Google Scholar] [CrossRef] [PubMed]
- McSpadden, K.E.; Patrick, H.; Oh, A.Y.; Yaroch, A.L.; Dwyer, L.A.; Nebeling, L.C. The association between motivation and fruit and vegetable intake: The moderating role of social support. Appetite 2016, 96, 87–94. [Google Scholar] [CrossRef]
- Kadhim, N.; Amiot, C.E.; Louis, W.R. Applying the self-determination theory continuum to unhealthy eating: Consequences on well-being and behavioral frequency. J. Appl. Soc. Psychol. 2020, 50, 381–393. [Google Scholar] [CrossRef]
- Pelletier, L.G.; Dion, S.C.; Slovinec-D’Angelo, M.; Reid, R. Why Do You Regulate What You Eat? Relationships Between Forms of Regulation, Eating Behaviors, Sustained Dietary Behavior Change, and Psychological Adjustment. Motiv. Emot. 2004, 28, 245–277. [Google Scholar] [CrossRef]
- Morrison, S.S.; Dashiff, C.J.; Vance, D.E. Role of parental autonomy support on self-determination in influencing diet and exercise motivation in older adolescents. Nursing Res. Rev. 2013, 3, 77. [Google Scholar] [CrossRef]
- Bejarano, M.C.M.; Cushing, C.C. Dietary Motivation and Hedonic Hunger Predict Palatable Food Consumption: An Intensive Longitudinal Study of Adolescents. Ann. Behav. Med. 2018, 52, 773–786. [Google Scholar] [CrossRef] [PubMed]
- Graber, J.A.; Brooks-Gunn, J. Transitions and turning points: Navigating the passage from childhood through adolescence. Dev. Psychol. 1996, 32, 768. [Google Scholar] [CrossRef]
- Van Ansem, W.J.; Schrijvers, C.T.; Rodenburg, G.; Schuit, A.J.; Van De Mheen, D. School food policy at Dutch primary schools: Room for improvement? Cross-sectional findings from the INPACT study. BMC Public Health 2013, 13, 339. [Google Scholar] [CrossRef]
- Rongen, F.C.; Van Kleef, E.; Sanjaya, S.; Vingerhoeds, M.H.; Buurma-Rethans, E.J.M.; Bogaard, C.V.D.; Van Rossum, C.T.M.; Seidell, J.C.; Dijkstra, S.C. What’s for lunch? The content and quality of lunches consumed by Dutch primary schoolchildren and the differences between lunches consumed at home and at school. BMC Public Health 2019, 19, 1365. [Google Scholar] [CrossRef] [PubMed]
- Zeinstra, G.G.; van der Haar, S.; Haveman-Nies, A. Strategies to increase primary school children’s fruit and vegetable intake during 10AM snack time. Appetite 2021, 163, 105235. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Fielding-Singh, P. How Food Rules at Home Influence Independent Adolescent Food Choices. J. Adolesc. Health 2018, 63, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Di Pasquale, R.; Rivolta, A. A Conceptual Analysis of Food Parenting Practices in the Light of Self-Determination Theory: Relatedness-Enhancing, Competence-Enhancing and Autonomy-Enhancing Food Parenting Practices. Front. Psychol. 2018, 9, 2373. [Google Scholar] [CrossRef]
- Bailey-Davis, L.; Poulsen, M.N.; Hirsch, A.G.; Pollak, J.; Glass, T.A.; Schwartz, B.S. Home Food Rules in Relation to Youth Eating Behaviors, Body Mass Index, Waist Circumference, and Percent Body Fat. J. Adolesc. Health 2017, 60, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Van Assema, P.; Glanz, K.; Martens, M.; Brug, J. Differences Between Parents’ and Adolescents’ Perceptions of Family Food Rules and Availability. J. Nutr. Educ. Behav. 2007, 39, 84–89. [Google Scholar] [CrossRef]
- Bere, E.; Klepp, K.-I. Correlates of fruit and vegetable intake among Norwegian schoolchildren: Parental and self-reports. Public Health Nutr. 2004, 7, 991–998. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Lytle, L.A.; Murray, D.M.; Birnbaum, A.S.; Story, M. Perceptions of the Family Mealtime Environment and Adolescent Mealtime Behavior: Do Adults and Adolescents Agree? J. Nutr. Educ. 2001, 33, 128–133. [Google Scholar] [CrossRef]
- Noom, M.J.; Deković, M.; Meeus, W. Conceptual Analysis and Measurement of Adolescent Autonomy. J. Youth Adolesc. 2001, 30, 577–595. [Google Scholar] [CrossRef]
- Hermans, R.C.J.; De Bruin, H.; Larsen, J.K.; Mensink, F.; Hoek, A.C. Adolescents’ Responses to a School-Based Prevention Program Promoting Healthy Eating at School. Front. Public Health 2017, 5, 309. [Google Scholar] [CrossRef]
- Shepherd, J.; Harden, A.; Rees, R.; Brunton, G.; Garcia, J.; Oliver, S.; Oakley, A. Young people and healthy eating: A systematic review of research on barriers and facilitators. Health Educ. Res. 2005, 21, 239–257. [Google Scholar] [CrossRef] [PubMed]
- Bassett, R.; Chapman, G.E.; Beagan, B.L. Autonomy and control: The co-construction of adolescent food choice. Appetite 2008, 50, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Videon, T.M.; Manning, C.K. Influences on adolescent eating patterns: The importance of family meals. J. Adolesc. Health 2003, 32, 365–373. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Intrinsic and Extrinsic Motivations: Classic Definitions and New Directions. Contemp. Educ. Psychol. 2000, 25, 54–67. [Google Scholar] [CrossRef]
- Dwyer, L.A.; Bolger, N.; Laurenceau, J.-P.; Patrick, H.; Oh, A.Y.; Nebeling, L.C.; Hennessy, E. Autonomous Motivation and Fruit/Vegetable Intake in Parent–Adolescent Dyads. Am. J. Prev. Med. 2017, 52, 863–871. [Google Scholar] [CrossRef]
- Niermann, C.Y.N.; Kremers, S.P.J.; Renner, B.; Wöll, A. Family Health Climate and Adolescents’ Physical Activity and Healthy Eating: A Cross-Sectional Study with Mother-Father-Adolescent Triads. PLoS ONE 2015, 10, e0143599. [Google Scholar] [CrossRef]
- Zhang, Z.; Farris, K.L.; Sun, M.; Dailey, R.M.; Donovan, E.E. Parenting Practices, Autonomous Motivation, and Adolescent Diet Habits. J. Res. Adolesc. 2020, 30, 800–816. [Google Scholar] [CrossRef]
- Fleary, S.A.; Joseph, P.; Chang, H. Applying the information-motivation-behavioral skills model to explain adolescents’ fruits and vegetables consumption. Appetite 2020, 147, 104546. [Google Scholar] [CrossRef] [PubMed]
- Parks, C.; Blaser, C.; Smith, T.M.; Calloway, E.; Oh, A.Y.; Dwyer, L.; Liu, B.; Nebeling, L.C.; Yaroch, A.L. Correlates of fruit and vegetable intake among parents and adolescents: Findings from the Family Life, Activity, Sun, Health, and Eating (FLASHE) study. Public Health Nutr. 2018, 21, 2079–2087. [Google Scholar] [CrossRef] [PubMed]
- Smit, C.R.; De Leeuw, R.N.H.; Bevelander, K.E.; Burk, W.J.; Buijs, L.; Van Woudenberg, T.J.; Buijzen, M. An integrated model of fruit, vegetable, and water intake in young adolescents. Health Psychol. 2018, 37, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Spear, H.J.; Kulbok, P. Autonomy and Adolescence: A Concept Analysis. Public Health Nurs. 2004, 21, 144–152. [Google Scholar] [CrossRef]
- Diamantopoulos, A.; Sarstedt, M.; Fuchs, C.; Wilczynski, P.; Kaiser, S. Guidelines for choosing between multi-item and single-item scales for construct measurement: A predictive validity perspective. J. Acad. Mark. Sci. 2012, 40, 434–449. [Google Scholar] [CrossRef]
- Bandura, A. The Explanatory and Predictive Scope of Self-Efficacy Theory. J. Soc. Clin. Psychol. 1986, 4, 359–373. [Google Scholar] [CrossRef]
- Sabiston, C.M.; Crocker, P.R. Examining an Integrative Model of Physical Activity and Healthy Eating Self-Perceptions and Behaviors Among Adolescents. J. Adolesc. Health 2008, 42, 64–72. [Google Scholar] [CrossRef]
- Cho, D.; Kim, S. Interplay Between Self-Efficacy and Perceived Availability at Home and in the School Neighborhood on Adolescents’ Fruit and Vegetable Intake and Energy-Dense, Low-Nutrient Food and Sugary Drink Consumption. J. Nutr. Educ. Behav. 2018, 50, 856–867. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Heary, C.; Kelly, C.; Nixon, E.; Shevlin, M. Self-efficacy for healthy eating and peer support for unhealthy eating are associated with adolescents’ food intake patterns. Appetite 2013, 63, 48–58. [Google Scholar] [CrossRef]
- Lubans, D.R.; Plotnikoff, R.C.; Morgan, P.J.; Dewar, D.; Costigan, S.; Collins, C.E. Explaining dietary intake in adolescent girls from disadvantaged secondary schools. A test of Social Cognitive Theory. Appetite 2012, 58, 517–524. [Google Scholar] [CrossRef]
- Pearson, N.; Ball, K.; Crawford, D. Predictors of changes in adolescents’ consumption of fruits, vegetables and energy-dense snacks. Br. J. Nutr. 2010, 105, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, W.M.; Markland, D.; Selzler, A.-M.; Murray, T.C.; Wilson, P.M. Distinguishing Perceived Competence and Self-Efficacy: An Example from Exercise. Res. Q. Exerc. Sport 2014, 85, 527–539. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Moller, A.C. Competence as central, but not sufficient, for high-quality motivation. In Handbook of Competence and Motivation: Theory and Application; The Guilford Press: New York, NY, USA, 2017; pp. 216–238. [Google Scholar]
- Mokhtari, S.; Grace, B.; Pak, Y.; Reina, A.; Durand, Q.; Yee, J.K. Motivation and perceived competence for healthy eating and exercise among overweight/obese adolescents in comparison to normal weight adolescents. BMC Obes. 2017, 4, 36. [Google Scholar] [CrossRef]
- Blaine, R.E.; Kachurak, A.; Davison, K.K.; Klabunde, R.; Fisher, J.O. Food parenting and child snacking: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 146. [Google Scholar] [CrossRef]
- Kiefner-Burmeister, A.; Hinman, N. The Role of General Parenting Style in Child Diet and Obesity Risk. Curr. Nutr. Rep. 2020, 9, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Yee, A.Z.H.; Lwin, M.O.; Ho, S.S. The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–14. [Google Scholar] [CrossRef]
- Ryan, R.M.; Solky, J.A. What is supportive about social support? In Handbook of Social Support and the Family; Springer: Berlin/Heidelberg, Germany, 1996; pp. 249–267. [Google Scholar]
- Grolnick, W.S.; Ryan, R.M. Parent styles associated with children’s self-regulation and competence in school. J. Educ. Psychol. 1989, 81, 143–154. [Google Scholar] [CrossRef]
- Baumrind, D. The Influence of Parenting Style on Adolescent Competence and Substance Use. J. Early Adolesc. 1991, 11, 56–95. [Google Scholar] [CrossRef]
- Darling, N.; Steinberg, L. Parenting style as context: An integrative model. Psychol. Bull. 1993, 113, 487–496. [Google Scholar] [CrossRef]
- Berge, J.M.; Wall, M.; Loth, K.; Neumark-Sztainer, D. Parenting Style as a Predictor of Adolescent Weight and Weight-Related Behaviors. J. Adolesc. Health 2010, 46, 331–338. [Google Scholar] [CrossRef]
- Vaughn, A.E.; Ward, D.S.; Fisher, J.O.; Faith, M.S.; Hughes, S.O.; Kremers, S.P.; Musher-Eizenman, D.R.; O’Connor, T.M.; Patrick, H.; Power, T.G. Fundamental constructs in food parenting practices: A content map to guide future research. Nutr. Rev. 2016, 74, 98–117. [Google Scholar] [CrossRef]
- Pearson, N.; Biddle, S.J.H.; Gorely, T. Family correlates of fruit and vegetable consumption in children and adolescents: A systematic review. Public Health Nutr. 2009, 12, 267–283. [Google Scholar] [CrossRef]
- Fleary, S.A.; Ettienne, R. The relationship between food parenting practices, parental diet and their adolescents’ diet. Appetite 2019, 135, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Loth, K.A.; MacLehose, R.F.; Larson, N.; Berge, J.M.; Neumark-Sztainer, D. Food availability, modeling and restriction: How are these different aspects of the family eating environment related to adolescent dietary intake? Appetite 2016, 96, 80–86. [Google Scholar] [CrossRef]
- Haughton, C.F.; Waring, M.E.; Wang, M.L.; Rosal, M.C.; Pbert, L.; Lemon, S.C. Home Matters: Adolescents Drink More Sugar-Sweetened Beverages When Available at Home. J. Pediatr. 2018, 202, 121–128. [Google Scholar] [CrossRef]
- Ding, D.; Sallis, J.F.; Norman, G.J.; Saelens, B.E.; Harris, S.K.; Kerr, J.; Rosenberg, D.; Durant, N.; Glanz, K. Community Food Environment, Home Food Environment, and Fruit and Vegetable Intake of Children and Adolescents. J. Nutr. Educ. Behav. 2012, 44, 634–638. [Google Scholar] [CrossRef]
- CBS. Inkomensverdeling Per Postcodegebied (PC4). 2017. Available online: https://www.cbs.nl/nl-nl/maatwerk/2019/50/inkomensverdeling-per-postcodegebied--pc4---2017 (accessed on 28 April 2021).
- CBS. Kerncijfers Per Postcode. Available online: https://www.cbs.nl/nl-nl/dossier/nederland-regionaal/geografische-data/gegevens-per-postcode (accessed on 28 April 2021).
- Neuhouser, M.L.; Lilley, S.; Lund, A.; Johnson, D.B. Development and Validation of a Beverage and Snack Questionnaire for Use in Evaluation of School Nutrition Policies. J. Am. Diet. Assoc. 2009, 109, 1587–1592. [Google Scholar] [CrossRef]
- Wilson, A.M.; Magarey, A.M.; Mastersson, N. Reliability and relative validity of a child nutrition questionnaire to simultaneously assess dietary patterns associated with positive energy balance and food behaviours, attitudes, knowledge and environments associated with healthy eating. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 5–12. [Google Scholar] [CrossRef]
- Dutch Nutrition Centre. Wat staat er in de Schijf van Vijf? Available online: https://www.voedingscentrum.nl/nl/gezond-eten-met-de-schijf-van-vijf/wat-staat-er-in-de-vakken-van-de-schijf-van-vijf.aspx (accessed on 28 April 2021).
- De Cock, N.; Van Lippevelde, W.; Vangeel, J.; Notebaert, M.; Beullens, K.; Eggermont, S.; Deforche, B.; Maes, L.; Goossens, L.; Verbeken, S.; et al. Feasibility and impact study of a reward-based mobile application to improve adolescents’ snacking habits. Public Health Nutr. 2018, 21, 2329–2344. [Google Scholar] [CrossRef]
- Gevers, D.W.; van Assema, P.; Sleddens, E.F.; de Vries, N.K.; Kremers, S.P. Associations between general parenting, restrictive snacking rules, and adolescent’s snack intake. The roles of fathers and mothers and interparental congruence. Appetite 2015, 87, 184–191. [Google Scholar] [CrossRef]
- Chen, B.; Vansteenkiste, M.; Beyers, W.; Boone, L.; Deci, E.L.; Van Der Kaap-Deeder, J.; Duriez, B.; Lens, W.; Matos, L.; Mouratidis, A.; et al. Basic psychological need satisfaction, need frustration, and need strength across four cultures. Motiv. Emot. 2015, 39, 216–236. [Google Scholar] [CrossRef]
- Peters, G.-J. The alpha and the omega of scale reliability and validity: Why and how to abandon Cronbach’s alpha and the route towards more comprehensive assessment of scale quality. Eur. Health Psychol. 2014, 16, 56–69. [Google Scholar]
- Williams, G.C.; Freedman, Z.R.; Deci, E.L. Supporting Autonomy to Motivate Patients with Diabetes for Glucose Control. Diabetes Care 1998, 21, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Quick, V.; Lipsky, L.M.; Nansel, T.R. Psychometric properties and factor structure of the adapted Self-Regulation Questionnaire assessing autonomous and controlled motivation for healthful eating among youth with type 1 diabetes and their parents. Child Care Health Dev. 2018, 44, 651–658. [Google Scholar] [CrossRef]
- Tabachnick, B.; Fidell, L.; Tabachnick, B.; Fidell, L. Using Multivariate Statistics, 6th ed.; Pearson: Essex, UK, 2014; Volume 235, p. 284. [Google Scholar]
- Hanson, N.; Neumark-Sztainer, D.; Eisenberg, M.; Story, M.; Wall, M. Associations between parental report of the home food environment and adolescent intakes of fruits, vegetables and dairy foods. Public Health Nutr. 2005, 8, 77–85. [Google Scholar] [CrossRef]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef]
- Sleddens, E.F.C.; O’Connor, T.M.; Watson, K.B.; Hughes, S.; Power, T.G.; Thijs, C.; De Vries, N.K.; Kremers, S.P.J. Development of the Comprehensive General Parenting Questionnaire for caregivers of 5–13 year olds. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 15. [Google Scholar] [CrossRef]
- Gevers, D.W.M.; Kremers, S.P.J.; De Vries, N.K.; Van Assema, P. The Comprehensive Snack Parenting Questionnaire (CSPQ): Development and Test-Retest Reliability. Int. J. Environ. Res. Public Health 2018, 15, 862. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Perinetti, G. StaTips Part IV: Selection, interpretation and reporting of the intraclass correlation coefficient. South Eur. J. Orthod. Dentofac. Res. 2018, 5, 3–5. [Google Scholar] [CrossRef]
- Streiner, D.L. Finding Our Way: An Introduction to Path Analysis. Can. J. Psychiatry 2005, 50, 115–122. [Google Scholar] [CrossRef]
- Kline, T.J.B. Psychological Testing: A Practical Approach to Design and Evaluation; SAGE Publications: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equat. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation Analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, E.; Hughes, S.O.; Goldberg, J.P.; Hyatt, R.R.; Economos, C.D. Permissive Parental Feeding Behavior Is Associated with an Increase in Intake of Low-Nutrient-Dense Foods among American Children Living in Rural Communities. J. Acad. Nutr. Diet. 2012, 112, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Alsharairi, N.A.; Somerset, S.M. Associations between Parenting Styles and Children’s Fruit and Vegetable Intake. Ecol. Food Nutr. 2014, 54, 93–113. [Google Scholar] [CrossRef]
- Van Der Horst, K.; Kremers, S.; Ferreira, I.; Singh, A.; Oenema, A.; Brug, J. Perceived parenting style and practices and the consumption of sugar-sweetened beverages by adolescents. Health Educ. Res. 2006, 22, 295–304. [Google Scholar] [CrossRef]
- Hill, A.J. Developmental issues in attitudes to food and diet. Proc. Nutr. Soc. 2002, 61, 259–266. [Google Scholar] [CrossRef]
- Green, E.M.; Spivak, C.; Dollahite, J.S. Early adolescent food routines: A photo-elicitation study. Appetite 2021, 158, 105012. [Google Scholar] [CrossRef]
- Wray-Lake, L.; Crouter, A.C.; McHale, S.M. Developmental Patterns in Decision-Making Autonomy Across Middle Childhood and Adolescence: European American Parents’ Perspectives. Child Dev. 2010, 81, 636–651. [Google Scholar] [CrossRef]
- Shaw, S.; Simao, S.C.; Jenner, S.; Lawrence, W.T.; Woods-Townsend, K.; Vogel, C.; Farrell, D.; Inskip, H.; Baird, J.; Morrison, L.; et al. Parental perspectives on negotiations over diet and physical activity: How do we involve parents in adolescent health interventions? Public Health Nutr. 2021, 1–10. [Google Scholar] [CrossRef]
- Palascha, A.; Van Kleef, E.; De Vet, E.; Van Trijp, H.C.M. Internally regulated eating style: A comprehensive theoretical framework. Br. J. Nutr. 2020, 1–13. [Google Scholar] [CrossRef]
- Adamo, K.B.; Brett, K.E. Parental Perceptions and Childhood Dietary Quality. Matern. Child Health J. 2013, 18, 978–995. [Google Scholar] [CrossRef]
- Reinaerts, E.; De Nooijer, J.; De Vries, N.K. Parental versus child reporting of fruit and vegetable consumption. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 33. [Google Scholar] [CrossRef][Green Version]
- Fulkerson, J.A.; Neumark-Sztainer, D.; Story, M. Adolescent and Parent Views of Family Meals. J. Am. Diet. Assoc. 2006, 106, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Lundahl, A.; Kidwell, K.M.; Nelson, T.D. Parental Underestimates of Child Weight: A Meta-analysis. Pediatrics 2014, 133, e689–e703. [Google Scholar] [CrossRef] [PubMed]
- Blanchet, R.; Kengneson, C.-C.; Bodnaruc, A.M.; Gunter, A.; Giroux, I. Factors Influencing Parents’ and Children’s Misperception of Children’s Weight Status: A Systematic Review of Current Research. Curr. Obes. Rep. 2019, 8, 373–412. [Google Scholar] [CrossRef]
- Balantekin, K.N.; Anzman-Frasca, S.; Francis, L.A.; Ventura, A.K.; Fisher, J.O.; Johnson, S.L. Positive parenting approaches and their association with child eating and weight: A narrative review from infancy to adolescence. Pediatr. Obes. 2020, 15, e12722. [Google Scholar] [CrossRef] [PubMed]
- Tugault-Lafleur, C.N.; Black, J.L.; Barr, S. A Systematic Review of Methods to Assess Children’s Diets in the School Context. Adv. Nutr. 2017, 8, 63–79. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Public Health and the Environment (RIVM). Overgewicht, Cijfers & Context, Huidige Situatie. Available online: https://www.volksgezondheidenzorg.info/onderwerp/overgewicht/cijfers-context/huidige-situatie#!node-overgewicht-kinderen (accessed on 28 April 2021).
- Ragelienė, T.; Grønhøj, A. The influence of peers’ and siblings’ on children’s and adolescents’ healthy eating behavior. A systematic literature review. Appetite 2020, 148, 104592. [Google Scholar] [CrossRef]



| Variable | Preadolescents (n = 142) | Preadolescent–Parent Dyads (n = 81) | |
|---|---|---|---|
| M (SD) | Preadolescents M (SD) | Parents M (SD) | |
| Preadolescents | |||
| Age (years) | 12.18 (0.43) | 12.17 (0.38) | |
| Gender | |||
| Boys | 55.6% | 61.7% | |
| Girls | 44.4% | 38.3% | |
| Ethnicity: Dutch | 97.9% | 98.8% | |
| Siblings | 1.49 (0.91) | 1.47 (0.92) | |
| 0 siblings | 6.3% | 8.6% | |
| 1 sibling | 53.5% | 49.4% | |
| 2 or more siblings | 40.2% | 41.9% | |
| Pocket money per week (EUR) | 2.44 (2.23) | 2.49 (2.44) | |
| Perceived weight status (parent-reported) | |||
| Underweight | 18.5% | ||
| Healthy weight | 64.2% | ||
| Overweight | 17.3% | ||
| Healthy intake ratio | 62.91 (24.98) | 63.82 (25.23) | |
| Food-related autonomy a | 1.51 (0.53) | 1.54 (0.57) | 0.99 (0.35) |
| Competence to eat healthily b | 5.41 (2.79) | 5.37 (2.87) | 6.17 (1.82) |
| Healthy eating motivation | 6.19 (2.08) | 6.12 (1.99) | |
| Number of schooldays bread is taken to school | 4.48 (1.08) | 4.46 (1.14) | |
| Food purchasing | 0.44 (0.91) | 0.46 (0.90) | 0.49 (0.59) |
| Food responsiveness (parent-reported) | 2.24 (0.67) | ||
| School encouragement to eat FV: Yes | 62.4% | 59.7% | 79% |
| School encouragement to drink water: Yes | 36.2% | 40.7% | 60.5% |
| Parents | |||
| Age | 43.04 (5.35) | ||
| Relationship to child | |||
| Mother | 91.4% | ||
| Father | 8.6% | ||
| Ethnicity of mother: Dutch | 90.8% | 95.1% | |
| Ethnicity of father: Dutch | 88.7% | 96.3% | |
| Relationship: Yes | 84% | ||
| Highest educational level | |||
| Low | 1.2% | ||
| Middle | 34.6% | ||
| High | 64.2% | ||
| Highest educational level of partner | |||
| Low | 2.9% | ||
| Middle | 39.7% | ||
| High | 57.4% | ||
| Difficulties with financial situation: No | 95.1% | ||
| Supportive parenting practices | 4.59 (0.34) | ||
| Relative availability of healthy options at home | 49.16 (5.68) | ||
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1: Healthy intake ratio | ||||||||||
| 2: Food-related autonomy | −0.16 | |||||||||
| 3: Competence to eat healthily | 0.27 ** | 0.04 | ||||||||
| 4: Healthy eating motivation | 0.32 ** | −0.06 | 0.46 ** | |||||||
| 5: Supportive parenting practices (parent-reported) | 0.12 | 0.31 ** | 0.05 | 0.08 | ||||||
| 6: Relative availability of healthy options at home (parent-reported) | 0.44 ** | −0.02 | 0.21 | 0.05 | 0.23 * | |||||
| 7: School encouragement to eat healthily | 0.13 | −0.06 | −0.16 | −0.03 | −0.08 | −0.11 | ||||
| 8: Number of schooldays bread is taken to school | 0.16 | −0.12 | 0.17 | 0.20 * | −0.12 | 0.19 | −0.10 | |||
| 9: Food purchasing | −0.25 ** | 0.22 ** | −0.17 * | −0.20 * | −0.05 | −0.09 | −0.01 | −0.05 | ||
| 10: Food responsiveness (parent-reported) | 0.03 | −0.24 * | 0.02 | 0.01 | −0.07 | −0.10 | 0.01 | 0.05 | −0.12 |
| Variable | Preadolescents M (SD) | Parents M (SD) | Mean Difference (95% CI) | ICC (95% CI) |
|---|---|---|---|---|
| Food-related autonomy (mean score total scale 0–3) | 1.54 (0.57) | 0.99 (0.35) | 0.55 (0.44–0.66) * | 0.27 (−0.07–0.54) |
| I can decide for myself when to consume snacks | 1.35 (0.99) | 0.94 (0.64) | 0.09 (−0.10–0.29) | |
| I can decide for myself how many snacks I am allowed to consume | 1.04 (1.07) | 0.50 (0.60) | 0.09 (−0.09–0.28) | |
| My parents tell me which snacks I am allowed to consume a | 1.77 (0.98) | 1.00 (0.76) | 0.11 (−0.07–0.29) | |
| Sometimes I consume snacks which I did not choose myself a | 1.89 (0.81) | 1.75 (0.52) | 0.26 (0.05–0.46) | |
| I pack foods and drinks to bring to school | 1.71 (1.12) | 1.08 (1.09) | 0.44 (0.17–0.63) | |
| Are you allowed to use pocket money to buy foods or drinks? | 1.45 (1.23) | 0.66 (0.64) | 0.19 (−0.02–0.39) | |
| Competence to eat healthily b(sum score total scale 0–8) | 5.37 (2.87) | 6.17 (1.82) | −0.80 (−1.54–−0.07) * | 0.04 (−0.17–0.24) |
| Effect | Estimate | SE | t | p |
|---|---|---|---|---|
| Supportive parenting practices → Food-related autonomy | 0.44 | 0.16 | 2.66 | 0.01 |
| Supportive parenting practices → Competence to eat healthily | 0.58 | 0.90 | 0.64 | 0.52 |
| Food-related autonomy → Healthy eating motivation | −0.43 | 0.31 | −1.37 | 0.17 |
| Competence to eat healthily → Healthy eating motivation | 0.34 | 0.06 | 6.18 | <0.001 |
| Supportive parenting practices → Healthy eating motivation | 0.66 | 0.63 | 1.05 | 0.29 |
| Healthy eating motivation → Healthy intake ratio | 2.85 | 1.03 | 2.78 | 0.01 |
| Relative availability of healthy options at home → Healthy intake ratio | 1.56 | 0.41 | 3.80 | <0.001 |
| Food-related autonomy → Healthy intake ratio | −7.68 | 3.80 | −2.02 | 0.04 |
| Competence to eat healthily → Healthy intake ratio | 0.90 | 0.75 | 1.20 | 0.23 |
| Supportive parenting practices → Healthy intake ratio | 3.99 | 7.65 | 0.52 | 0.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Nee, R.L.; van Kleef, E.; van Trijp, H.C.M. Dutch Preadolescents’ Food Consumption at School: Influence of Autonomy, Competence and Parenting Practices. Nutrients 2021, 13, 1505. https://doi.org/10.3390/nu13051505
van Nee RL, van Kleef E, van Trijp HCM. Dutch Preadolescents’ Food Consumption at School: Influence of Autonomy, Competence and Parenting Practices. Nutrients. 2021; 13(5):1505. https://doi.org/10.3390/nu13051505
Chicago/Turabian Stylevan Nee, Roselinde L., Ellen van Kleef, and Hans C. M. van Trijp. 2021. "Dutch Preadolescents’ Food Consumption at School: Influence of Autonomy, Competence and Parenting Practices" Nutrients 13, no. 5: 1505. https://doi.org/10.3390/nu13051505
APA Stylevan Nee, R. L., van Kleef, E., & van Trijp, H. C. M. (2021). Dutch Preadolescents’ Food Consumption at School: Influence of Autonomy, Competence and Parenting Practices. Nutrients, 13(5), 1505. https://doi.org/10.3390/nu13051505