
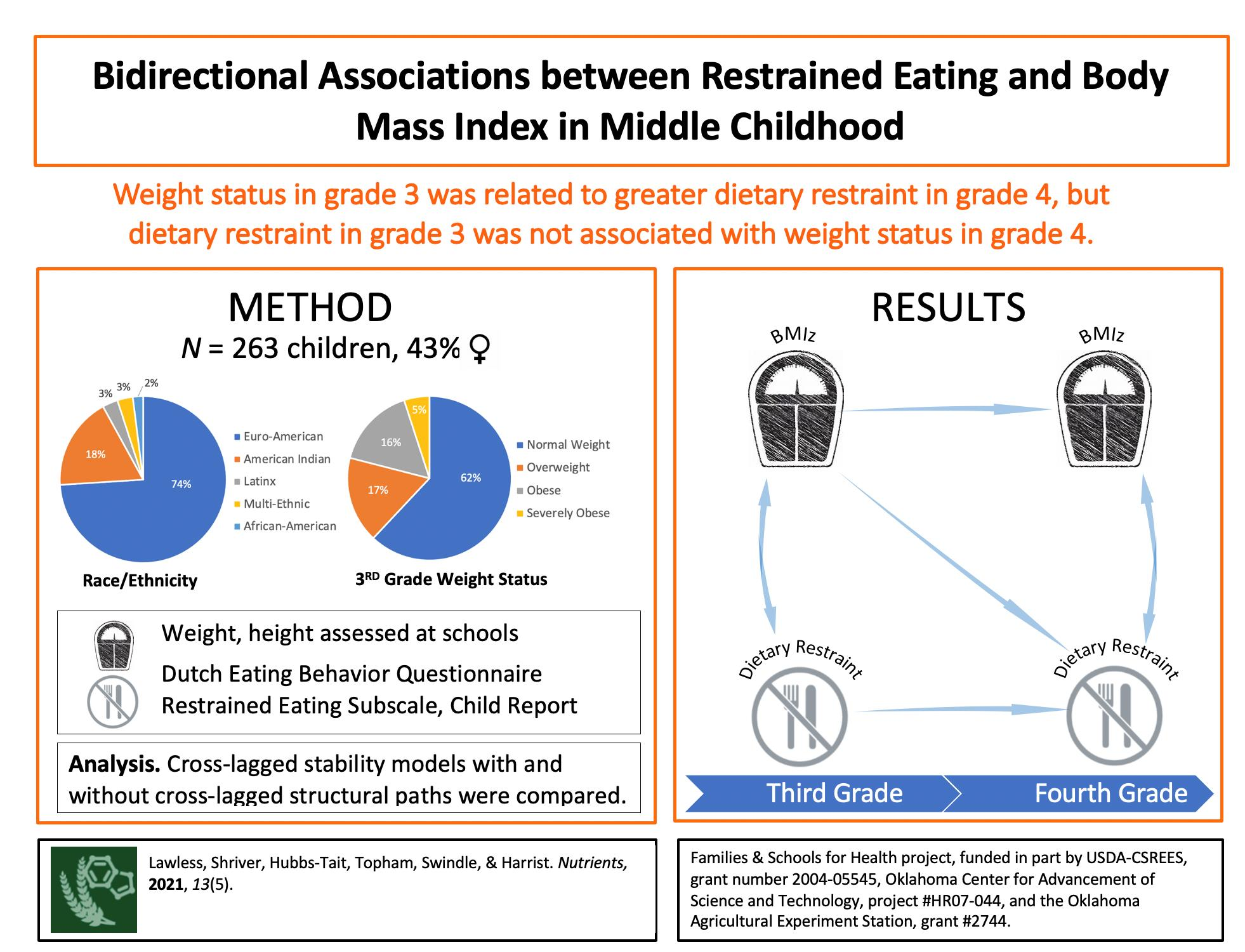
Bidirectional Associations between Restrained Eating and Body Mass Index in Middle Childhood


 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Procedures
2.2. Procedures
2.3. Study Measures
2.3.1. Dietary Restraint
2.3.2. Weight and Weight Status
2.4. Statistical Analysis
3. Results
3.1. Structural Model Comparisons
3.1.1. Stability Model
3.1.2. Cross-Lagged Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kochanek, K.D.; Murphy, S.L.; Xu, J.; Arias, E. National Vital Statistics Reports Volume 68, Number 9, 24 June 2019. In Deaths: Final Data for 2017; National Center for Health Statistics: Hyattsville, MD, USA, 24 June 2019. [Google Scholar]
- Ward, Z.J.; Long, M.W.; Resch, S.C.; Giles, C.M.; Cradock, A.L.; Gortmaker, S.L. Simulation of Growth Trajectories of Childhood Obesity into Adulthood. N. Engl. J. Med. 2017, 377, 2145–2153. [Google Scholar] [CrossRef]
- Li, C.; Goran, M.I.; Kaur, H.; Nollen, N.; Ahluwalia, J.S. Developmental Trajectories of Overweight during Childhood: Role of Early Life Factors. Obesity 2007, 15, 760–771. [Google Scholar] [CrossRef]
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. Obesity: A Chronic Relapsing Progressive Disease Process. A Position Statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- Churuangsuk, C.; Kherouf, M.; Combet, E.; Lean, M. Low-Carbohydrate Diets for Overweight and Obesity: A Systematic Review of the Systematic Reviews. Obes. Rev. 2018, 19, 1700–1718. [Google Scholar] [CrossRef]
- Gloy, V.L.; Briel, M.; Bhatt, D.L.; Kashyap, S.R.; Schauer, P.R.; Mingrone, G.; Bucher, H.C.; Nordmann, A.J. Bariatric Surgery versus Non-Surgical Treatment for Obesity: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ 2013, 347, f5934. [Google Scholar] [CrossRef] [PubMed]
- May, A.L.; Kim, S.A.; Sherry, B.; Blanck, H.M. Childhood Obesity Task Forces Established by State Legislatures, 2001–2010. Prev. Chronic Dis. 2013, 10, E144. [Google Scholar] [CrossRef]
- Boyce, J.A.; Gleaves, D.H.; Kuijer, R.G. Measuring Dietary Restraint Status: Comparisons between the Dietary Intent Scale and the Restraint Scale. Front. Nutr. 2015, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Hagan, K.E.; Forbush, K.T.; Chen, P.-Y. Is Dietary Restraint a Unitary or Multi-Faceted Construct? Psychol. Assess. 2017, 29, 1249–1260. [Google Scholar] [CrossRef]
- Herman, C.P.; Mack, D. Restrained and Unrestrained Eating. J. Personal. 1975, 43, 647–660. [Google Scholar] [CrossRef]
- Johnson, F.; Pratt, M.; Wardle, J. Dietary Restraint and Self-Regulation in Eating Behavior. Int. J. Obes. 2012, 36, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Greenway, F.L. Physiological Adaptations to Weight Loss and Factors Favouring Weight Regain. Int. J. Obes. 2015, 39, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Haines, J.; Story, M.; Eisenberg, M.E. Why Does Dieting Predict Weight Gain in Adolescents? Findings from Project EAT-II: A 5-Year Longitudinal Study. J. Am. Diet. Assoc. 2007, 107, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Story, M.; Standish, A.R. Dieting and Unhealthy Weight Control Behaviors during Adolescence: Associations with 10-Year Changes in Body Mass Index. J. Adolesc. Health 2012, 50, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Herman, C.P.; Polivy, J. A Boundary Model for the Regulation of Eating. Res. Publ.-Assoc. Res. Nerv. Ment. Dis. 1984, 62, 141–156. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Sysko, R.; Roberto, C.A.; Allison, S. Are Dietary Restraint Scales Valid Measures of Dietary Restriction? Additional Objective Behavioral and Biological Data Suggest Not. Appetite 2010, 54, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Fryar, C.D.; Carroll, M.D.; Freedman, D.S.; Ogden, C.L. Trendsinobesity and Severe Obesity Prevalence in Usyouth and Adultsby Sex and Age, 2007–2008 to 2015–2016. JAMA 2018, 319, 1723–1725. [Google Scholar] [CrossRef]
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-Processed Products Are Becoming Dominant in the Global Food System. Obes. Rev. 2013, 14, 21–28. [Google Scholar] [CrossRef]
- Bauer, K.W.; Chuisano, S. Intentional Self-Regulation of Eating Among Children and Adolescents. In Pediatric Food Preferences and Eating Behaviors; Elsevier, Academic Press: Cambridge, MA, USA, 2018; pp. 255–270. [Google Scholar]
- Ha, O.R.; Lim, S.L.; Bruce, J.M.; Bruce, A.S. Unhealthy Foods Taste Better among Children with Lower Self-Control. Appetite 2019, 139, 84–89. [Google Scholar] [CrossRef]
- Russell, C.G.; Russell, A. “food” and “Non-Food” Self-Regulation in Childhood: A Review and Reciprocal Analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 33. [Google Scholar] [CrossRef]
- Schaumberg, K.; Anderson, D.A.; Anderson, L.M.; Reilly, E.E.; Gorrell, S. Dietary Restraint: What’s the Harm? A Review of the Relationship between Dietary Restraint, Weight Trajectory and the Development of Eating Pathology. Clin. Obes. 2016, 6, 89–100. [Google Scholar] [CrossRef]
- Birch, L.L.; Davison, K.K. Family Environmental Factors Influencing the Developing Behavioral Controls of Food Intake and Childhood Overweight. Pediatri. Clin. N. Am. 2001, 48, 893–907. [Google Scholar] [CrossRef]
- Davison, K.K.; Birch, L.L. Childhood Overweight: A Contextual Model and Recommendations for Future Research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Carper, J.L.; Orlet Fisher, J.; Birch, L.L. Young Girls’ Emerging Dietary Restraint and Disinhibition Are Related to Parental Control in Child Feeding. Appetite 2000, 35, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Damiano, S.R.; Paxton, S.J.; Wertheim, E.H.; McLean, S.A.; Gregg, K.J. Dietary Restraint of 5-Year-Old Girls: Associations with Internalization of the Thin Ideal and Maternal, Media, and Peer Influences. Int. J. Eat. Disord. 2015, 48, 1166–1169. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Nichols, T.E.; Damiano, S.R.; Wertheim, E.H.; Paxton, S.J. Low Body Esteem and Dietary Restraint among 7-Year Old Children: The Role of Perfectionism, Low Self-Esteem, and Belief in the Rewards of Thinness and Muscularity. Eat. Behav. 2019, 32, 65–68. [Google Scholar] [CrossRef]
- Shunk, J.A.; Birch, L.L. Girls at Risk for Overweight at Age 5 Are at Risk for Dietary Restraint, Disinhibited Overeating, Weight Concerns, and Greater Weight Gain from 5 to 9 Years. J. Am. Diet. Assoc. 2004, 104, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch Eating Behavior Questionnaire (DEBQ) for Assessment of Restrained, Emotional, and External Eating Behavior. Int. J. Eat. Disord. 1986, 5, 295–315. [Google Scholar] [CrossRef]
- van Strien, T.; Oosterveld, P. The Children’s DEBQ for Assessment of Restrained, Emotional, and External Eating in 7- to 12-Year-Old Children. Int. J. Eat. Disord. 2008, 41, 72–81. [Google Scholar] [CrossRef]
- Shunk, J.A.; Birch, L.L. Validity of Dietary Restraint among 5- to 9-Year Old Girls. Appetite 2004, 42, 241–247. [Google Scholar] [CrossRef]
- Anschutz, D.J.; Kanters, L.J.A.; van Strien, T.; Vermulst, A.A.; Engels, R.C.M.E. Maternal Behaviors and Restrained Eating and Body Dissatisfaction in Young Children. Int. J. Eat. Disord. 2009, 42, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Markey, C.N.; Birch, L.L. A Longitudinal Examination of Patterns in Girls’ Weight Concerns and Body Dissatisfaction from Ages 5 to 9 Years. Int. J. Eat. Disord. 2003, 33, 320–332. [Google Scholar] [CrossRef] [PubMed]
- Snoek, H.M.; van Strien, T.; Janssens, J.M.A.M.; Engels, R.C.M.E. Restrained Eating and BMI: A Longitudinal Study among Adolescents. Health Psychol. 2008, 27, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Severo, M.; Vilela, S.; Fildes, A.; Oliveira, A. Bidirectional Relationships between Appetitive Behaviours and Body Mass Index in Childhood: A Cross-Lagged Analysis in the Generation XXI Birth Cohort. Eur. J. Nutr. 2020, 60, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.O.; Power, T.G.; O’Connor, T.M.; Fisher, J.O. Executive Functioning, Emotion Regulation, Eating Self-Regulation, and Weight Status in Low-Income Preschool Children: How Do They Relate? Appetite 2015, 89, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Power, T.G.; Hidalgo-Mendez, J.; Fisher, J.O.; O’Connor, T.M.; Micheli, N.; Hughes, S.O. Obesity Risk in Hispanic Children: Bidirectional Associations between Child Eating Behavior and Child Weight Status over Time. Eat. Behav. 2020, 36, 101366. [Google Scholar] [CrossRef] [PubMed]
- Haines, J.; Neumark-Sztainer, D. Prevention of Obesity and Eating Disorders: A Consideration of Shared Risk Factors. Health Educ. Res. 2006, 21, 770–782. [Google Scholar] [CrossRef] [PubMed]
- Harrist, A.W.; Topham, G.L.; Hubbs-Tait, L.; Shriver, L.H.; Swindle, T.M. Psychosocial Factors in Children’s Obesity: Examples From An Innovative Line of Inquiry. Child Dev. Perspect. 2017, 11, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Harrist, A.W.; Swindle, T.M.; Hubbs-Tait, L.; Topham, G.L.; Shriver, L.H.; Page, M.C. The Social and Emotional Lives of Overweight, Obese, and Severely Obese Children. Child Dev. 2016, 87, 1564–1580. [Google Scholar] [CrossRef] [PubMed]
- Shriver, L.H.; Hubbs-Tait, L.; Harrist, A.W.; Topham, G.; Page, M. Child Gender and Weight Status Moderate the Relation of Maternal Feeding Practices to Body Esteem in 1st Grade Children. Appetite 2015, 89, 62–69. [Google Scholar] [CrossRef]
- Topham, G.L.; Hubbs-Tait, L.; Rutledge, J.M.; Page, M.C.; Kennedy, T.S.; Shriver, L.H.; Harrist, A.W. Parenting Styles, Parental Response to Child Emotion, and Family Emotional Responsiveness Are Related to Child Emotional Eating. Appetite 2011, 56, 261–264. [Google Scholar] [CrossRef]
- Barlow, S.E. Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics 2007, 120 (Suppl. 4), S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Wei, R.; Ogden, C. Weight-for-Stature Compared with Body Mass Index-for-Age Growth Charts for the United States from the Centers for Disease Control and Prevention. Am. J. Clin. Nutr. 2002, 75, 761–766. [Google Scholar] [CrossRef]
- Krebs, N.F.; Himes, J.H.; Jacobson, D.; Nicklas, T.A.; Guilday, P.; Styne, D. Assessment of Child and Adolescent Overweight and Obesity. Pediatrics 2007, 120 (Suppl. 4), S193–S228. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.A.; Shapiro, J.R.; Lundgren, J.D.; Spataro, L.E.; Frye, C.A. Self-Reported Dietary Restraint Is Associated with Elevated Levels of Salivary Cortisol. Appetite 2002, 38, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Inokuchi, M.; Matsuo, N.; Takayama, J.I.; Hasegawa, T. BMI Z-Score Is the Optimal Measure of Annual Adiposity Change in Elementary School Children. Ann. Hum. Biol. 2011, 38, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, H.J. Use of Percentiles and Z-Scores in Anthropometry. In Handbook of Anthropometry: Physical Measures of Human Form in Health and Disease; Springer: New York, NY, USA, 2012; pp. 29–48. ISBN 9781441917881. [Google Scholar]
- Mplus User’s Guide. Available online: https://www.statmodel.com/html_ug.shtml (accessed on 22 January 2021).
- Bohrer, B.K.; Forbush, K.T.; Hunt, T.K. Are Common Measures of Dietary Restraint and Disinhibited Eating Reliable and Valid in Obese Persons? Appetite 2015, 87, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Meule, A. Cultural Reflections on Restrained Eating. Front. Psychol. 2016, 7, 205. [Google Scholar] [CrossRef]
- Rodgers, R.F.; Paxton, S.J.; McLean, S.A. A Biopsychosocial Model of Body Image Concerns and Disordered Eating in Early Adolescent Girls. J. Youth Adolesc. 2014, 43, 814–823. [Google Scholar] [CrossRef]
- de Jonge, J.; Dormann, C.; Janssen, P.P.M.; Dollard, M.F.; Landeweerd, J.A.; Nijhuis, F.J.N. Testing Reciprocal Relationships between Job Characteristics and Psychological Well-Being: A Cross-Lagged Structural Equation Model. J. Occup. Organ. Psychol. 2001, 74, 29–46. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Jackson, S.L.; Cunningham, S.A. The Stability of Children’s Weight Status over Time, and the Role of Television, Physical Activity, and Diet. Prev. Med. 2017, 100, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H. Body Image Concerns among Children. J. Pediatr. 2001, 138, 158–160. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tremblay, L.; Lariviere, M. The Influence of Puberty Onset, Body Mass Index, and Pressure to Be Thin on Disordered Eating Behaviors in Children and Adolescents. Eat. Behav. 2009, 10, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Mäkinen, M.; Puukko-Viertomies, L.R.; Lindberg, N.; Siimes, M.A.; Aalberg, V. Body Dissatisfaction and Body Mass in Girls and Boys Transitioning from Early to Mid-Adolescence: Additional Role of Self-Esteem and Eating Habits. BMC Psychiatry 2012, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- van den Berg, P.A.; Mond, J.; Eisenberg, M.; Ackard, D.; Neumark-Sztainer, D. The Link between Body Dissatisfaction and Self-Esteem in Adolescents: Similarities across Gender, Age, Weight Status, Race/Ethnicity, and Socioeconomic Status. J. Adolesc. Health 2010, 47, 290–296. [Google Scholar] [CrossRef]
- Loth, K.A.; MacLehose, R.; Bucchianeri, M.; Crow, S.; Neumark-Sztainer, D. Predictors of Dieting and Disordered Eating Behaviors From Adolescence to Young Adulthood. J. Adolesc. Health 2014, 55, 705–712. [Google Scholar] [CrossRef]
- Paxton, S.J.; Eisenberg, M.E.; Neumark-Sztainer, D. Prospective Predictors of Body Dissatisfaction in Adolescent Girls and Boys: A Five-Year Longitudinal Study. Dev. Psychol. 2006, 42, 888–899. [Google Scholar] [CrossRef]
- Ruderman, A.J.; Christensen, H. Restraint Theory and Its Applicability to Overweight Individuals. J. Abnorm. Psychol. 1983, 92, 210–215. [Google Scholar] [CrossRef]
- Zarychta, K.; Kulis, E.; Gan, Y.; Chan, C.K.Y.; Horodyska, K.; Luszczynska, A. Why Are You Eating, Mom? Maternal Emotional, Restrained, and External Eating Explaining Children’s Eating Styles. Appetite 2019, 141, 104335. [Google Scholar] [CrossRef]
- Urbanek, J.K.; Metzgar, C.J.; Hsiao, P.Y.; Piehowski, K.E.; Nickols-Richardson, S.M. Increase in Cognitive Eating Restraint Predicts Weight Loss and Change in Other Anthropometric Measurements in Overweight/Obese Premenopausal Women. Appetite 2015, 87, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, Ö.; Pott, W.; Hebebrand, J.; de Zwaan, M.; Pauli-Pott, U. Baseline Dietary Restraint Predicts Negative Treatment Outcomes after 12 Months in Children and Adolescents with Obesity Participating in a Lifestyle Intervention. Obes. Facts 2019, 12, 179–189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Age, Years (Range) | 9.34 (8.51–10.73) |
|---|---|
| Girls | 114 (43.4) |
| Race/ethnicity | |
| American Indian | 48 (18.1) |
| African American | 5 (1.9) |
| Hispanic | 8 (3.0) |
| Asian | 1 (4) |
| White | 196 (74.0) |
| Multiethnic | 7 (2.6) |
| Weight Status | |
| Normal weight | 166 (61.9) |
| Overweight | 46 (17.2) |
| Obese | 44 (16.4) |
| Severe Obese | 12 (4.5) |
| n = 263, expressed as n (%) | |
| M | SD | Range | Skewness | |
|---|---|---|---|---|
| Grade 3 BMIz a | 0.65 | 1.13 | −2.2–2.7 | −0.23 |
| Grade 4 BMIz | 0.66 | 1.23 | −2.6–2.72 | −0.28 |
| Grade 3 Restraint | 1.52 | 0.24 | 0.88–2.80 | 0.71 |
| Grade 4 Restraint | 1.45 | 0.22 | 0.89–3.00 | 0.96 |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1.Grade 3 BMIz | --- | |||
| 2.Grade 4 BMIz | 0.95 *** | --- | ||
| 3.Grade 3 Restraint | 0.26 *** | 0.25 *** | --- | |
| 4.Grade 4 Restraint | 0.29 *** | 0.34 *** | 0.43 **** | --- |
| Model | χ2 | df | CFI | RMSEA | SRMR | Comparison | Δχ2 | Δdf |
|---|---|---|---|---|---|---|---|---|
| Model 1 a | 15.17 * | 8 | 0.99 | 0.06 | 0.06 | |||
| Model 2 b | 14.66 * | 7 | 0.99 | 0.06 | 0.06 | M1–M2 | 0.41 | 1 |
| Model 3 c | 3.69 * | 7 | 1 | 0 | 0.01 | M1–M3 | 9.51 ** | 1 |
| Model 4 d | 3.47 | 6 | 1 | 0 | 0.01 | M1–M4 | 10.80 ** | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lawless, M.; Shriver, L.H.; Hubbs-Tait, L.; Topham, G.L.; Swindle, T.; Harrist, A.W. Bidirectional Associations between Restrained Eating and Body Mass Index in Middle Childhood. Nutrients 2021, 13, 1485. https://doi.org/10.3390/nu13051485
Lawless M, Shriver LH, Hubbs-Tait L, Topham GL, Swindle T, Harrist AW. Bidirectional Associations between Restrained Eating and Body Mass Index in Middle Childhood. Nutrients. 2021; 13(5):1485. https://doi.org/10.3390/nu13051485
Chicago/Turabian StyleLawless, Meg, Lenka H. Shriver, Laura Hubbs-Tait, Glade L. Topham, Taren Swindle, and Amanda W. Harrist. 2021. "Bidirectional Associations between Restrained Eating and Body Mass Index in Middle Childhood" Nutrients 13, no. 5: 1485. https://doi.org/10.3390/nu13051485
APA StyleLawless, M., Shriver, L. H., Hubbs-Tait, L., Topham, G. L., Swindle, T., & Harrist, A. W. (2021). Bidirectional Associations between Restrained Eating and Body Mass Index in Middle Childhood. Nutrients, 13(5), 1485. https://doi.org/10.3390/nu13051485