
Vitamin D Status in Spanish Elite Team Sport Players

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Biochemical Analyses
2.2. Seasonality
2.3. Vitamin Supplementation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- González-Gross, M.; Valtuena, J.; Breidenassel, C.; Moreno, L.A.; Ferrari, M.; Kersting, M.; De Henauw, S.; Gottrand, F.; Azzini, E.; Widhalm, K.; et al. Vitamin D status among adolescents in Europe: The Healthy Lifestyle in Europe by Nutrition in Adolescence study. Br. J. Nutr. 2012, 107, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A. Demographic Differences and Trends of Vitamin D Insufficiency in the US Population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D: A D-Lightful health perspective. Nutr. Rev. 2008, 66, S182–S194. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Villacis, D.; Yi, A.; Jahn, R.; Kephart, C.J.; Charlton, T.; Gamradt, S.C.; Romano, R.; Tibone, J.E.; Hatch, I.G.F.R. Prevalence of Abnormal Vitamin D Levels Among Division I NCAA Athletes. Sports Health 2014, 6, 340–347. [Google Scholar] [CrossRef]
- Lovell, G. Vitamin D Status of Females in an Elite Gymnastics Program. Clin. J. Sport Med. 2008, 18, 159–161. [Google Scholar] [CrossRef]
- Constantini, N.W.; Arieli, R.; Chodick, G.; Dubnov-Raz, G. High Prevalence of Vitamin D Insufficiency in Athletes and Dancers. Clin. J. Sport Med. 2010, 20, 368–371. [Google Scholar] [CrossRef]
- Hamilton, B.; Grantham, J.; Racinais, S.; Chalabi, H. Vitamin D deficiency is endemic in Middle Eastern sportsmen. Public Health Nutr. 2010, 13, 1528–1534. [Google Scholar] [CrossRef]
- Close, G.; Russell, J.; Cobley, J.; Owens, D.; Wilson, G.; Gregson, W.; Fraser, W.; Morton, J. Assessment of vitamin D concentration in non-supplemented professional athletes and healthy adults during the winter months in the UK: Implications for skeletal muscle function. J. Sports Sci. 2013, 31, 344–353. [Google Scholar] [CrossRef]
- Magee, P.J.; Pourshahidi, L.K.; Wallace, J.M.W.; Cleary, J.; Conway, J.; Harney, E.; Madigan, S.M. Vitamin D status and supplementation in elite Irish athletes. Int. J. Sport Nutr. Exerc. Metab. 2013, 23, 441–448. [Google Scholar] [CrossRef]
- Valtueña, J.; Dominguez, D.; Til, L.; Gonzalez-Gross, M.; Drobnic, F. High prevalence of vitamin D insufficiency among elite Spanish athletes the importance of outdoor training adaptation. Nutr. Hosp. 2014, 30, 124–131. [Google Scholar]
- Braun, H.; Von Andrian-Werburg, J.; Schänzer, W.; Thevis, M. Nutrition Status of Young Elite Female German Football Players. Pediatr. Exerc. Sci. 2018, 30, 157–167. [Google Scholar] [CrossRef]
- Ceglia, L. Vitamin D and its role in skeletal muscle. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 628–633. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Importance in the prevention of cancers, type 1 diabetes, heart disease, and osteoporosis. Am. J. Clin. Nutr. 2004, 79, 362–371. [Google Scholar] [CrossRef]
- Medicine FaNBIo. Dietary Reference Intakes for Calcium and Vitamin D; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American college of sports medicine joint position statement. nutrition and athletic performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar]
- Bartoszewska, M.; Kamboj, M.; Patel, D.R. Vitamin D, Muscle Function, and Exercise Performance. Pediatr. Clin. N. Am. 2010, 57, 849–861. [Google Scholar] [CrossRef]
- Hamilton, B. Vitamin D and Human Skeletal Muscle. Scand. J. Med. Sci. Sports 2010, 20, 182–190. [Google Scholar] [CrossRef]
- Cannell, J.J.; Hollis, B.W.; Sorenson, M.B.; Taft, T.N.; Anderson, J.J.B. Athletic Performance and Vitamin D. Med. Sci. Sports Exerc. 2009, 41, 1102–1110. [Google Scholar] [CrossRef]
- Bandeira, F.; Griz, L.; Freese, E.; Lima, D.C.; Thé, A.C.; Diniz, E.T.; Marques, T.F.; Lucena, C.S. Vitamin D deficiency and its relationship with bone mineral density among postmenopausal women living in the tropics. Arq. Bras. Endocrinol. Metabol. 2010, 54, 227–232. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: The other steroid hormone for muscle function and strength. Menopause 2009, 16, 1077–1078. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic and consequences for nonskeletal health: Mechanisms of action. Mol. Asp. Med. 2008, 29, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Gordon, C.M.; DePeter, K.C.; Feldman, H.A.; Grace, E.; Emans, S.J. Prevalence of Vitamin D Deficiency among Healthy Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Neal, S.; Sykes, J.; Rigby, M.; Hess, B. A review and clinical summary of vitamin D in regard to bone health and athletic performance. Physician Sportsmed. 2015, 43, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Valtueña, J.; González-Gross, M.; Huybrechts, I.; Breidenassel, C.; Ferrari, M.; Mouratidou, T.; Gottrand, F.; Dallongeville, J.; Azzini, E.; Sioen, I.; et al. Factors Associated with Vitamin D Deficiency in European Adolescents: The HELENA Study. J. Nutr. Sci. Vitaminol. 2013, 59, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Galan, F.; Ribas, J.; Sánchez-Martinez, P.M.; Calero, T.; Sánchez, A.B.; Muñoz, A. Serum 25-hydroxyvitamin D in early autumn to ensure vitamin D sufficiency in mid-winter in professional football players. Clin. Nutr. 2012, 31, 132–136. [Google Scholar] [CrossRef]
- García, R.B.; Guisado, F.A.R. Low levels of vitamin D in professional basketball players after wintertime: Relationship with dietary intake of vitamin D and calcium. Nutr. Hosp. 2011, 26, 945–951. [Google Scholar]
- Larson-Meyer, D.E.; Willis, K.S. Vitamin D and Athletes. Curr. Sports Med. Rep. 2010, 9, 220–226. [Google Scholar] [CrossRef]
- Farrokhyar, F.; Tabasinejad, R.; Dao, D.; Peterson, D.; Ayeni, O.R.; Hadioonzadeh, R.; Bhandari, M. Prevalence of Vitamin D Inadequacy in Athletes: A Systematic-Review and Meta-Analysis. Sports Med. 2015, 45, 365–378. [Google Scholar] [CrossRef]
- Maynard, L.M.; Wisemandle, W.; Roche, A.F.; Chumlea, W.C.; Guo, S.S.; Siervogel, R.M. Childhood Body Composition in Relation to Body Mass Index. Pediatrics 2001, 107, 344–350. [Google Scholar] [CrossRef]
- Valtueña, J.; Gracia-Marco, L.; Huybrechts, I.; Breidenassel, C.; Ferrari, M.; Gottrand, F.; Dallongeville, J.; Sioen, I.; Gutierrez, A.; Kersting, M.; et al. Cardiorespiratory fitness in males, and upper limbs muscular strength in females, are positively related with 25-hydroxyvitamin D plasma concentrations in European adolescents: The HELENA study. QJM Int. J. Med. 2013, 106, 809–821. [Google Scholar] [CrossRef]
- Holick, M.F.; Malabanan, A.; Veronikis, I.E. Redefining vitamin D insufficiency. Lancet 1998, 351, 805–806. [Google Scholar] [CrossRef]
- Holick, M.F. The Vitamin D Epidemic and its Health Consequences. J. Nutr. 2005, 135, 2739S–2748S. [Google Scholar] [CrossRef]
- Moreno, L.A.; Valtueña, J.; Pérez-López, F.; González-Gross, M. Health Effects Related to Low Vitamin D Concentrations: Beyond Bone Metabolism. Ann. Nutr. Metab. 2011, 59, 22–27. [Google Scholar] [CrossRef]
- Holick, M.F. Optimal Vitamin D Status for the Prevention and Treatment of Osteoporosis. Drugs Aging 2007, 24, 1017–1029. [Google Scholar] [CrossRef]
- Koundourakis, N.E.; Androulakis, N.E.; Malliaraki, N.; Margioris, A.N. Vitamin D and Exercise Performance in Professional Soccer Players. PLoS ONE 2014, 9, e101659. [Google Scholar] [CrossRef]
- Close, G.L.; Leckey, J.; Patterson, M.; Bradley, W.; Owens, D.J.; Fraser, W.D.; Morton, J.P. The effects of vitamin D3supplementation on serum total 25[OH]D concentration and physical performance: A randomised dose–response study. Br. J. Sports Med. 2013, 47, 692–696. [Google Scholar] [CrossRef]
- Morton, J.P.; Iqbal, Z.; Drust, B.; Burgess, D.; Close, G.L.; Brukner, P.D. Seasonal variation in vitamin D status in professional soccer players of the English Premier League. Appl. Physiol. Nutr. Metab. 2012, 37, 798–802. [Google Scholar] [CrossRef]
- Pfeifer, M.; Begerow, B.; Minne, H.W. Vitamin D and Muscle Function. Osteoporos. Int. 2002, 13, 187–194. [Google Scholar] [CrossRef]
- Allison, R.J.; Close, G.L.; Farooq, A.; Riding, N.R.; Salah, O.; Hamilton, B.; Wilson, M.G. Severely vitamin D-deficient athletes present smaller hearts than sufficient athletes. Eur. J. Prev. Cardiol. 2015, 22, 535–542. [Google Scholar] [CrossRef]
- Halliday, T.M.; Peterson, N.J.; Thomas, J.J.; Kleppinger, K.; Hollis, B.W.; Larson-Meyer, D.E. Vitamin D Status Relative to Diet, Lifestyle, Injury, and Illness in College Athletes. Med. Sci. Sports Exerc. 2011, 43, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Ogan, D.; Pritchett, K. Vitamin D and the Athlete: Risks, Recommendations, and Benefits. Nutrients 2013, 5, 1856–1868. [Google Scholar] [CrossRef] [PubMed]
- Ovesen, L.; Andersen, R.; Jakobsen, J. Geographical differences in vitamin D status, with particular reference to European countries. Proc. Nutr. Soc. 2003, 62, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Goswami, R.; Kochupillai, N.; Gupta, N.; Goswami, D.; Singh, N.; Dudha, A. Presence of 25(OH) D deficiency in a rural North Indian village despite abundant sunshine. JAPI 2008, 56, 755–757. [Google Scholar]
- Maroon, J.C.; Mathyssek, C.M.; Bost, J.W.; Amos, A.; Winkelman, R.; Yates, A.P.; Duca, M.A.; Norwing, J.A. Vitamin D profile in National Football League Players. Am. J. Sports Med. 2015, 43, 1241–1245. [Google Scholar] [CrossRef]
- Sghaier-Ayadi, A.; Feki, M.; Ayed, I.B.-B.; Abene, O.; Ben Fredj, M.; Kaabachi, N.; Chaouachi, A. Vitamin D status and determinants of deficiency in non-supplemented athletes during the winter months in Tunisia. Biol. Sport 2015, 32, 281. [Google Scholar] [CrossRef]
- Valtueña, J.; Breidenassel, C.; Folle, J.; Gonzalez-Gross, M. Retinol, beta-carotene, alpha-tocopherol and vitamin D status in European adolescents; regional differences an variability: A review. Nutr. Hosp. 2011, 26, 280–288. [Google Scholar]
- Hill, T.R.; Cotter, A.A.; Mitchell, S.; Boreham, C.A.; Dubitzky, W.; Murray, L.; Strain, J.J.; Flynn, A.; Robson, P.J.; Wallace, J.M.W.; et al. Vitamin D status and its determinants in adolescents from the Northern Ireland Young Hearts 2000 cohort. Br. J. Nutr. 2008, 99, 1061–1067. [Google Scholar] [CrossRef]
- Lehtonen-Veromaa, M.; Möttönen, T.; Irjala, K.; Kärkkäinen, M.; Lamberg-Allardt, C.; Hakola, P.; Viikari, J. Vitamin D intake is low and hypovitaminosis D common in healthy 9- to 15-year-old Finnish girls. Eur. J. Clin. Nutr. 1999, 53, 746–751. [Google Scholar] [CrossRef]
- Looker, A.C.; Pfeiffer, C.M.; Lacher, D.A.; Schleicher, R.L.; Picciano, M.F.; Yetley, E.A. Serum 25-hydroxyvitamin D status of the US population: 1988–1994 compared with 2000–2004. Am. J. Clin. Nutr. 2008, 88, 1519–1527. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C.; Lu, Z.; Sauter, E. Vitamin D and Skin Physiology: A D-Lightful Story. J. Bone Miner. Res. 2007, 22, V28–V33. [Google Scholar] [CrossRef]
- Alzaman, N.S.; Dawson-Hughes, B.; Nelson, J.; D’Alessio, D.; Pittas, A.G. Vitamin D status of black and white Americans and changes in vitamin D metabolites after varied doses of vitamin D supplementation. Am. J. Clin. Nutr. 2016, 104, 205–214. [Google Scholar] [CrossRef]
- Farrokhyar, F.; Sivakumar, G.; Savage, K.; Koziarz, A.; Jamshidi, S.; Ayeni, O.R.; Peterson, D.; Bhandari, M. Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations and Physical Performance in Athletes: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sports Med. 2017, 47, 2323–2339. [Google Scholar] [CrossRef]
- Fairbairn, K.A.; Ceelen, I.J.; Skeaff, C.M.; Cameron, C.M.; Perry, T.L. Vitamin D3 Supplementation Does Not Improve Sprint Performance in Professional Rugby Players: A Randomised, Placebo-Controlled Double Blind Intervention Study. Int. J. Sport Nutr. Exerc. Metab. 2017, 28, 1–9. [Google Scholar] [CrossRef]
- Wyon, M.A.; Koutedakis, Y.; Wolman, R.; Nevill, A.M.; Allen, N. The influence of winter vitamin D supplementation on muscle function and injury occurrence in elite ballet dancers: A controlled study. J. Sci. Med. Sport 2014, 17, 8–12. [Google Scholar] [CrossRef]
- Välimäki, V.V.; Alfthan, H.; Lehmuskallio, E.; Löyttyniemi, E.; Sahi, T.; Stenman, U.H.; Suominen, H.; Välimäki, M.J. Vitamin D Status as a Determinant of Peak Bone Mass in Young Finnish Men. J. Clin. Endocrinol. Metab. 2004, 89, 76–80. [Google Scholar] [CrossRef]
- Lappe, J.; Cullen, D.; Haynatzki, G.; Recker, R.; Ahlf, R.; Thompson, K. Calcium and Vitamin D Supplementation Decreases Incidence of Stress Fractures in Female Navy Recruits. J. Bone Miner. Res. 2008, 23, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Owens, D.J.; Tang, J.C.Y.; Bradley, W.J.; Sparks, A.S.; Fraser, W.D.; Morton, J.P.; Close, G.L. Efficacy of High-Dose Vitamin D Supplements for Elite Athletes. Med. Sci. Sports Exerc. 2017, 49, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Tylavsky, F.A.; Cheng, S.; Lyytikäinen, A.; Viljakainen, H.; Lamberg-Allardt, C. Strategies to Improve Vitamin D Status in Northern European Children: Exploring the Merits of Vitamin D Fortification and Supplementation. J. Nutr. 2006, 136, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P. Vitamin D in Health and Disease. Clin. J. Am. Soc. Nephrol. 2008, 3, 1535–1541. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % | Mean | SD | Min | Max | |
|---|---|---|---|---|---|
| Age (y) | – | 27.3 | 4.6 | 18.8 | 37.0 |
| Height (cm) | – | 184.7 | 11.1 | 167.0 | 218.0 |
| Weight (kg) | – | 82.5 | 12.4 | 64.0 | 120.0 |
| Race | – | ||||
| Caucasian | 87.4 | 93.6 | 23.2 | 52.6 | 159.8 |
| Black | 4.2 | 65.0 | 10.0 | 55.1 | 77.4 |
| Other | 8.4 | 85.1 | 17.2 | 69.8 | 118.4 |
| Whole Mean 25(OH)D | – | 91.9 | 23.1 | 52.6 | 159.8 |
| <75 nmol/L | 26.3 | 66.0 | 7.1 | 52.6 | 75.0 |
| ≥75 nmol/L | 73.7 | 101.2 | 23.1 | 75.7 | 159.8 |
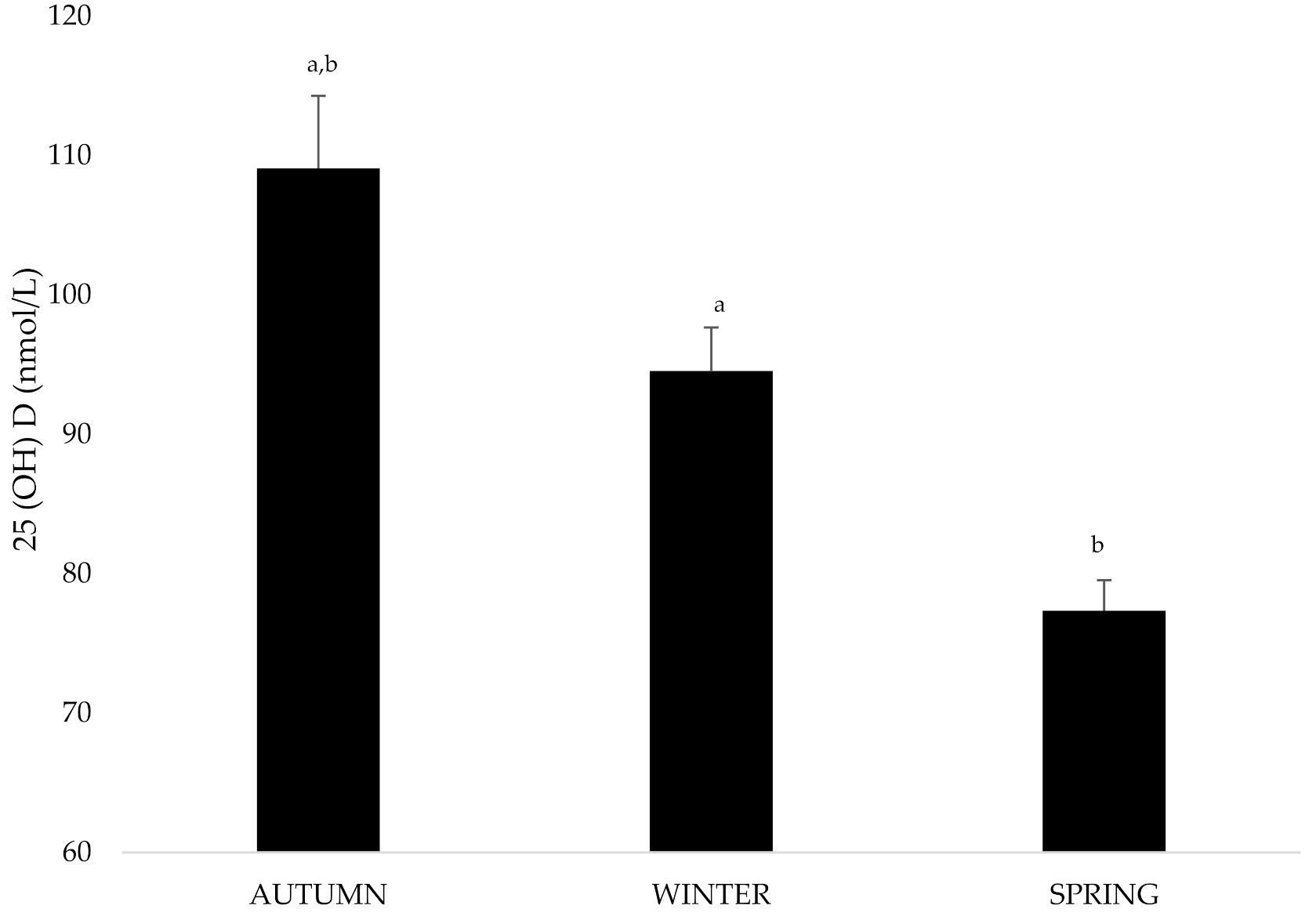
| Autumn 25(OH)D status | – | 109.8 | 32.8 | 60.8 | 220.3 |
| <75 nmol/L | 10 | 68.8 | 3.9 | 60.8 | 73.0 |
| ≥75 nmol/L | 90 | 114.4 | 31.4 | 75.3 | 220.3 |
| Winter 25(OH)D status | – | 84.9 | 22.5 | 43.0 | 142.5 |
| <75 nmol/L | 34.6 | 61.8 | 8.7 | 43.0 | 73.8 |
| ≥75 nmol/L | 65.4 | 97.2 | 17.3 | 75.8 | 142.5 |
| Spring 25(OH)D status | – | 82.2 | 21.8 | 31.8 | 138.3 |
| <75 nmol/L | 38.6 | 61.8 | 9.8 | 31.8 | 74.5 |
| ≥75 nmol/L | 61.4 | 94.9 | 17.0 | 75.3 | 138.3 |
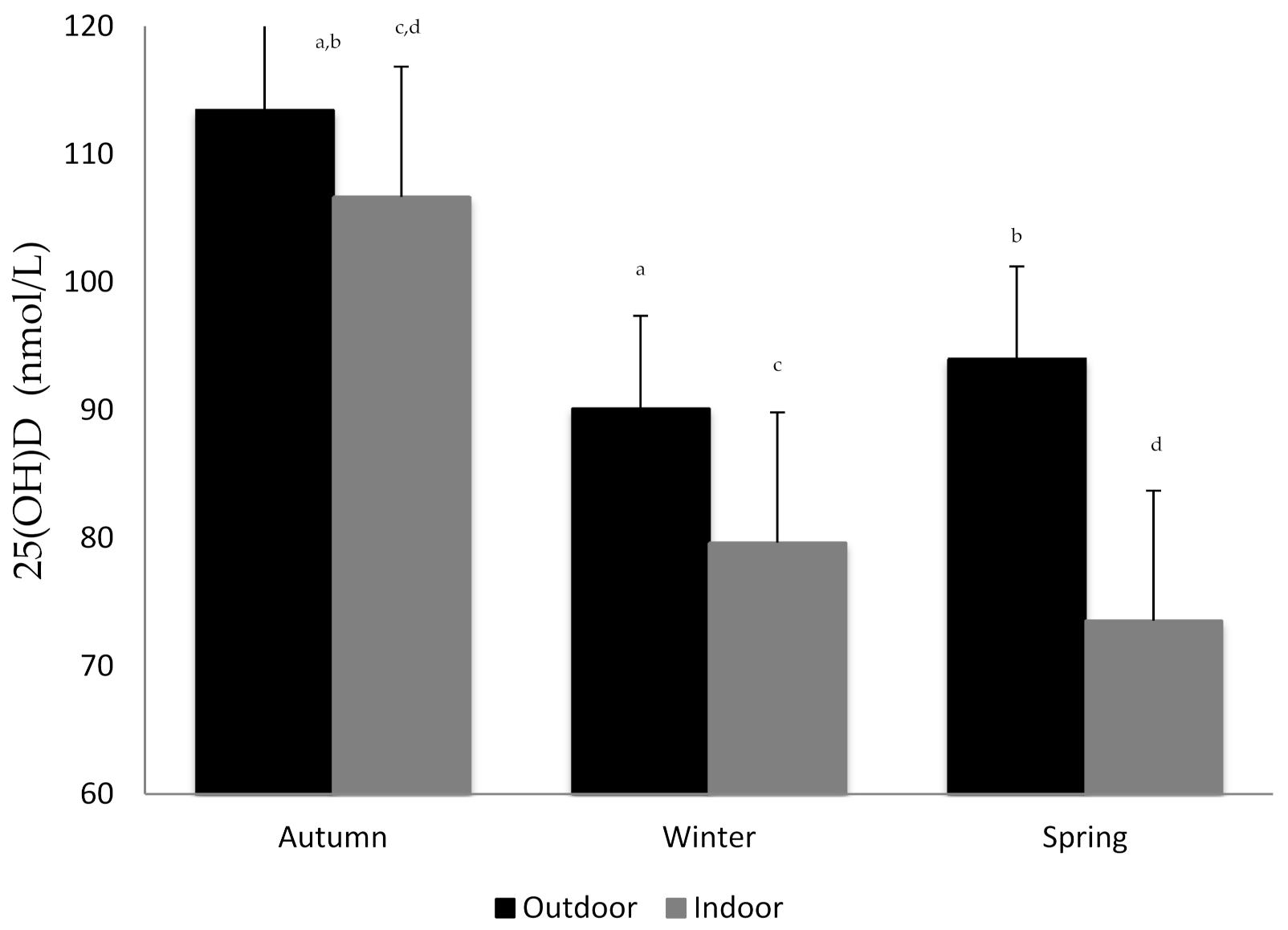
| 25(OH)D Indoor Training place | 54.7 | 85.3 | 23.1 | 52.6 | 159.8 |
| Handball | 17.9 | 95.5 | 24.5 | 52.6 | 145.8 |
| Basketball | 12.6 | 67.7 | 9.9 | 53.1 | 83.5 |
| Roller Hockey | 11.6 | 76.4 | 10.8 | 62.2 | 93.25 |
| Indoor Football | 12.6 | 98.0 | 25.1 | 69.8 | 159.8 |
| 25(OH)D Outdoor Training place | 45.3 | 99.5 | 21.0 | 58.0 | 141.2 |
| Football 1st division | 23.2 | 95.0 | 22.0 | 58.9 | 141.2 |
| Football 2nd division | 22.1 | 104.2 | 19.3 | 58.0 | 132.1 |
| Supplementation (YES) | 58.7 | – | – | – | – |
| N | Mean | SD | p-Value | ||
|---|---|---|---|---|---|
| Age | No supplementation | 35 | 28.1 | 4.0 | 0.046 |
| Supplementation | 60 | 26.9 | 4.9 | ||
| Height | No supplementation | 35 | 187.2 | 11.8 | NS |
| Supplementation | 60 | 182.6 | 10.6 | ||
| Weight | No supplementation | 35 | 84.8 | 13.1 | NS |
| Supplementation | 60 | 80.4 | 11.9 | ||
| Autumn (mean 25(OH)D) | No supplementation | 39 | 107.7 | 33.2 | NS |
| Supplementation | 56 | 111.2 | 32.8 | ||
| Winter (mean 25(OH)D) | No supplementation | 39 | 87.4 | 22.8 | NS |
| Supplementation | 56 | 82.7 | 22.0 | ||
| Spring (mean 25(OH)D) | No supplementation | 39 | 73.6 | 16.8 | 0.014 |
| Supplementation | 56 | 89.0 | 23.6 |
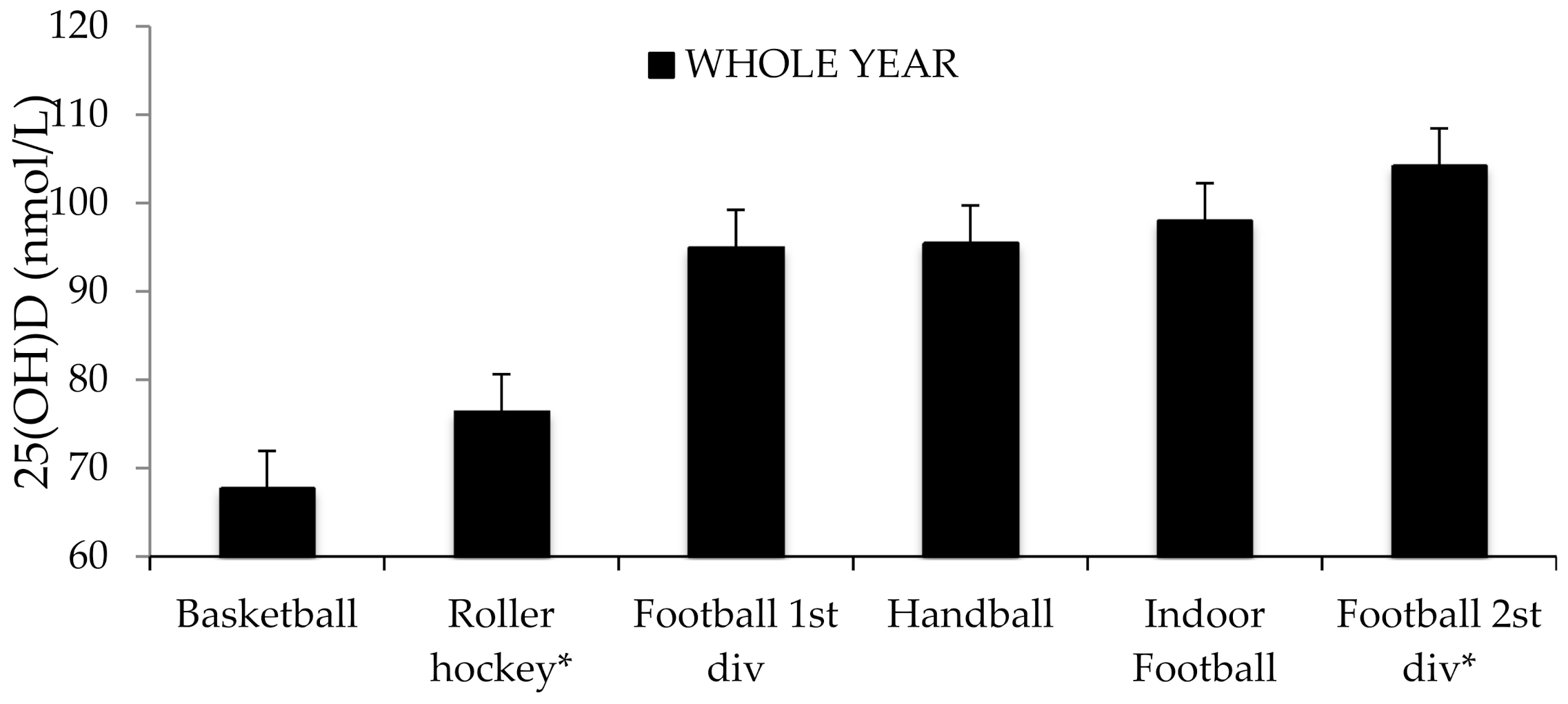
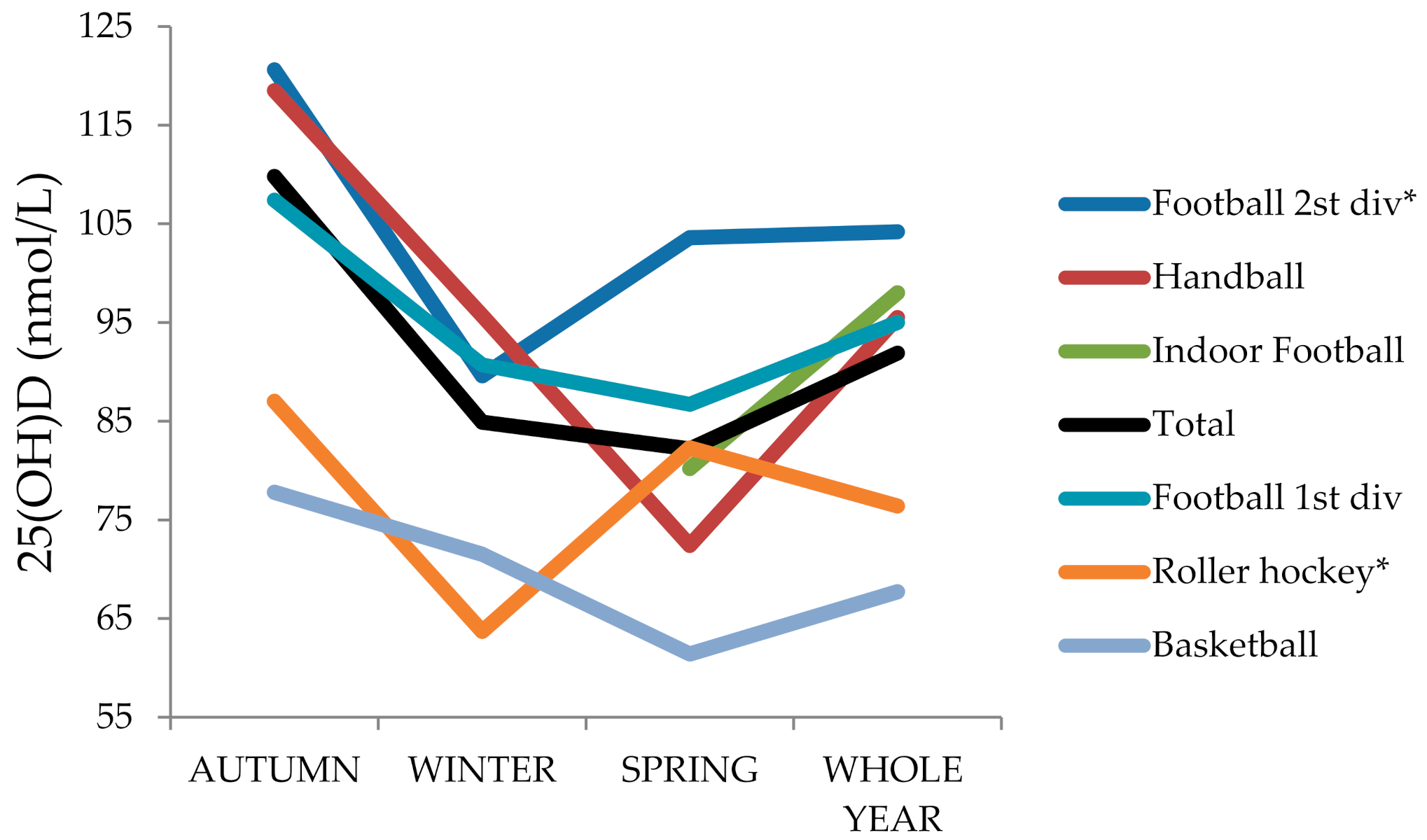
| Sports | Mean | SD | Min | Max | p-Value | |
|---|---|---|---|---|---|---|
| WHOLE YEAR | Handball | 95.5 | 24.5 | 52.6 | 145.8 | |
| No Supplementation | 93.7 | 24.0 | 52.6 | 145.8 | NS | |
| Supplementation | 125.6 | – | 125.6 | 125.6 | NS | |
| Basketball (BS) | 67.7 | 9.9 | 53.1 | 83.5 | <0.05 with all | |
| Roller hockey (RH) | 76.4 | 10.8 | 62.2 | 93.25 | <0.05 with football 2nd div | |
| Indoor Football | 98.0 | 25.1 | 69.8 | 159.8 | NS | |
| Football 1st div | 95.0 | 22.0 | 58.9 | 141.2 | NS | |
| No Supplementation | 90.0 | 19.8 | 58.9 | 127.1 | NS | |
| Supplementation | 108.5 | 23.6 | 83.3 | 141.2 | NS | |
| Football 2nd div | 104.2 | 19.3 | 58.0 | 132.1 | NS | |
| AUTUMN | Handball | 118.5 | 39.2 | 78.5 | 220.3 | NS |
| No Supplementation | 117.9 | 40.4 | 78.5 | 220.3 | NS | |
| Supplementation | 127.5 | – | 127.5 | 127.5 | NS | |
| Basketball | 77.8 | 19.2 | 60.75 | 105.3 | <0.05 with all except RH | |
| No Supplementation | 99.0 | 20.5 | 70.0 | 137.0 | NS | |
| Supplementation | 132.7 | 26.6 | 105.0 | 158.5 | NS | |
| Roller hockey | 87.0 | 13.6 | 71.6 | 116.5 | NS | |
| Indoor Football | 115.9 | 39.5 | 65.5 | 210.5 | NS | |
| Football 1st div | 107.4 | 26.1 | 70 | 158.5 | NS | |
| No Supplementation | 99.0 | 20.5 | 70.0 | 137.0 | <0.05 between suppl. | |
| Supplementation | 132.7 | 26.6 | 105.0 | 158.5 | NS | |
| Football 2nd div | 120.6 | 30.0 | 68.7 | 168.2 | NS | |
| WINTER | Handball | 95.7 | 25.8 | 43 | 142.5 | NS |
| No Supplementation | 92.8 | 23.5 | 43.0 | 137.0 | NS | |
| Supplementation | 142.5 | – | 142.5 | 142.5 | NS | |
| Basketball | 71.5 | 11.7 | 55.3 | 92.3 | <0.05 with all except RH | |
| No Supplementation | 77.8 | 8.1 | 68.8 | 92.3 | <0.05 between suppl. | |
| Supplementation | 58.8 | 5.1 | 55.3 | 66.3 | NS | |
| Roller hockey | 63.7 | 11.1 | 50.0 | 89.7 | <0.05 with all except BS | |
| Indoor Football | – | – | – | – | NS | |
| Football 1st div | 90.7 | 23.6 | 54.5 | 130.5 | NS | |
| No Supplementation | 86.8 | 24.5 | 54.5 | 130.5 | <0.05 between suppl. | |
| Supplementation | 100.3 | 19.6 | 83.5 | 130.5 | NS | |
| Football 2nd div | 89.6 | 17.5 | 50.0 | 121.0 | NS | |
| SPRING | Handball | 72.4 | 17.7 | 31.8 | 106.8 | <0.01 with football 2nd div |
| No Supplementation | 70.3 | 15.9 | 31.8 | 94.8 | NS | |
| Supplementation | 106.8 | 106.8 | 106.8 | NS | ||
| Basketball | 61.4 | 10.6 | 50.3 | 83.0 | <0.01 with football (both) | |
| No Supplementation | 71.6 | 14.9 | 54.8 | 83.0 | <0.05 between suppl. | |
| Supplementation | 57.9 | 6.8 | 50.3 | 70.0 | NS | |
| Roller hockey | 82.3 | 12.6 | 67.0 | 110.8 | NS | |
| Indoor Football | 80.2 | 16.7 | 51.5 | 109.25 | <0.05 with football 2nd div | |
| Football 1st div | 86.7 | 20.7 | 50.8 | 134.5 | NS | |
| No Supplementation | 81.1 | 17.1 | 50.8 | 114.3 | <0.05 between suppl. | |
| Supplementation | 100.8 | 23.7 | 77.8 | 134.5 | NS | |
| Football 2nd div | 103.6 | 22.3 | 55.3 | 138.3 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valtueña, J.; Aparicio-Ugarriza, R.; Medina, D.; Lizarraga, A.; Rodas, G.; González-Gross, M.; Drobnic, F. Vitamin D Status in Spanish Elite Team Sport Players. Nutrients 2021, 13, 1311. https://doi.org/10.3390/nu13041311
Valtueña J, Aparicio-Ugarriza R, Medina D, Lizarraga A, Rodas G, González-Gross M, Drobnic F. Vitamin D Status in Spanish Elite Team Sport Players. Nutrients. 2021; 13(4):1311. https://doi.org/10.3390/nu13041311
Chicago/Turabian StyleValtueña, Jara, Raquel Aparicio-Ugarriza, Daniel Medina, Antonia Lizarraga, Gil Rodas, Marcela González-Gross, and Franchek Drobnic. 2021. "Vitamin D Status in Spanish Elite Team Sport Players" Nutrients 13, no. 4: 1311. https://doi.org/10.3390/nu13041311
APA StyleValtueña, J., Aparicio-Ugarriza, R., Medina, D., Lizarraga, A., Rodas, G., González-Gross, M., & Drobnic, F. (2021). Vitamin D Status in Spanish Elite Team Sport Players. Nutrients, 13(4), 1311. https://doi.org/10.3390/nu13041311