
Consequences of the COVID-19 Syndemic for Nutritional Health: A Systematic Review

 , ,
, ,  ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
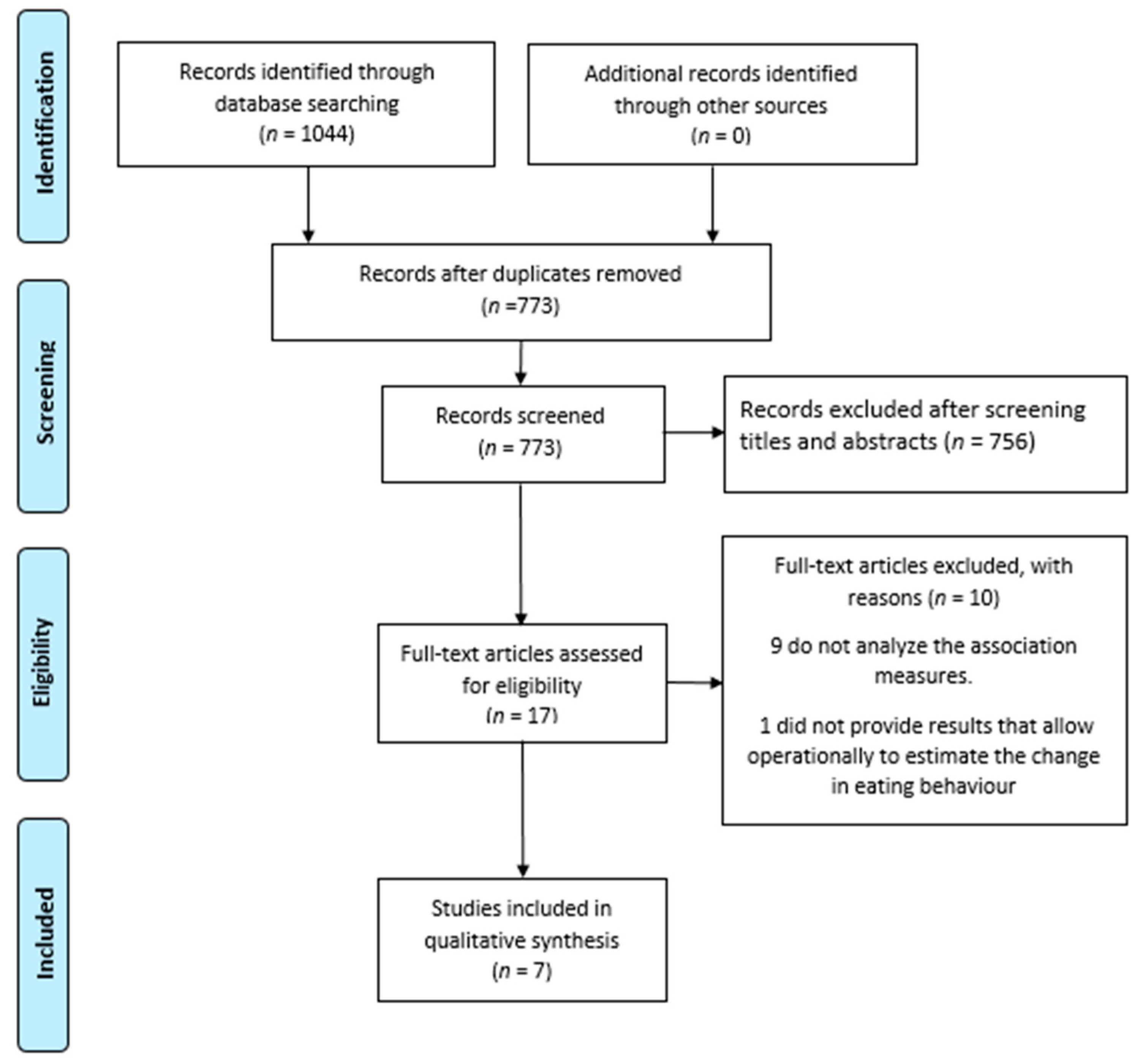
2.3. Studies Selection
2.4. Data Extraction
2.5. Methodological Quality Assessment
3. Results
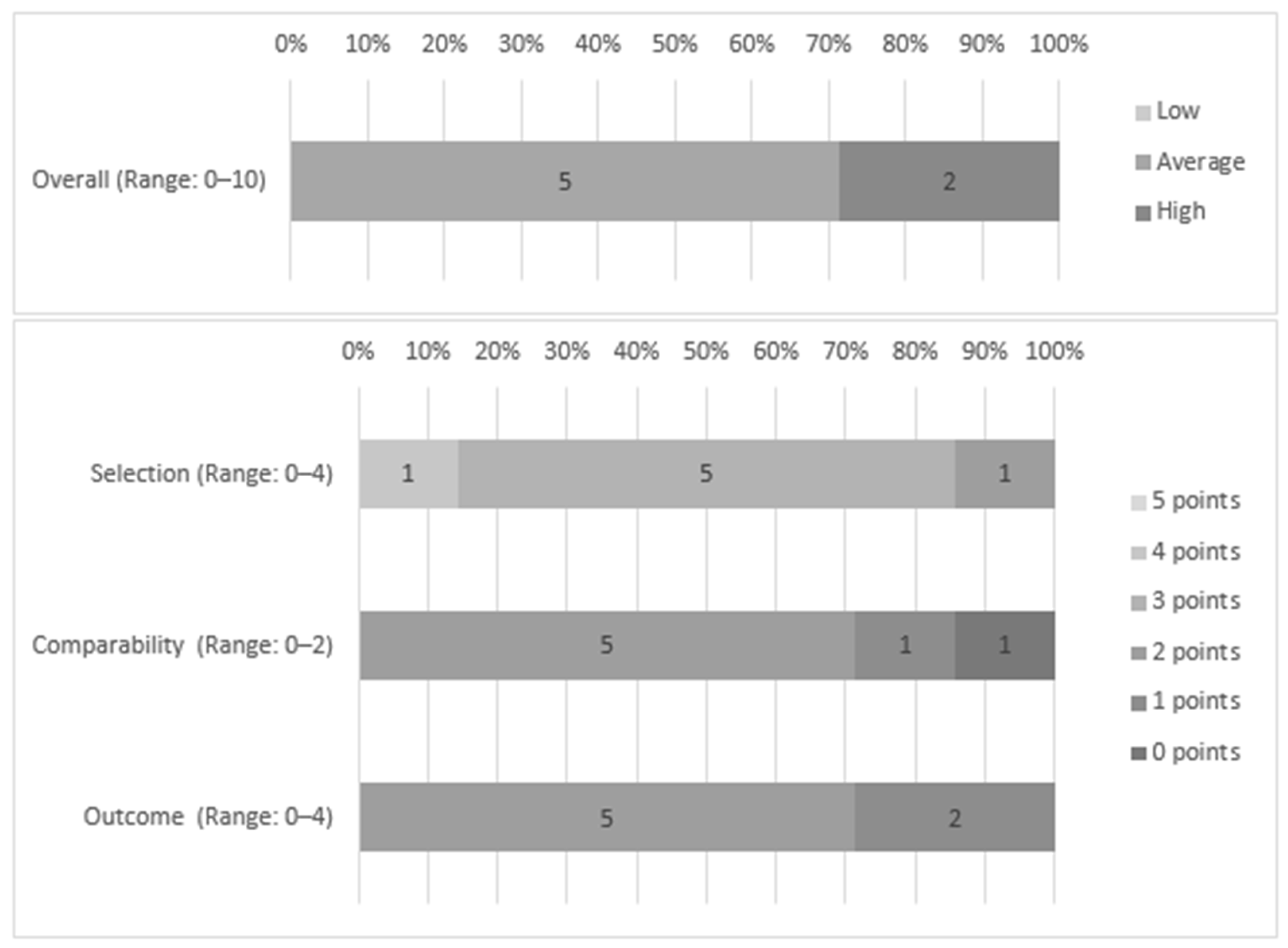
3.1. Methodological Quality Assessment
3.2. Studies Characteristics
3.3. Eating Behavior and Confinement or Social Distancing Measures
3.4. Changes in Food Intake
3.5. Weight Gain and BMI
3.6. Change in Eating Style
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Electronic Database | Keywords Combination and Boolean Operators |
|---|---|
| APA Scopus Web of Science Pubmed Embase Cochrane | “Social Distancing” and “Eating Behavior” |
| “Social Distancing” and “Feeding Behavior” | |
| “Social Distancing” and “Eating Habits” | |
| “Physical Distancing” and “Eating Behavior” | |
| “Physical Distancing” and “Feeding Behavior” | |
| “Physical Distancing” and “Eating Habits” | |
| “Social Isolation” and “Eating Behavior” | |
| “Social Isolation” and “Feeding Behavior” | |
| “Social Isolation” and “Eating Habits” | |
| Quarantine and “Eating Behavior” | |
| Quarantine and “Feeding Behavior” | |
| Quarantine and “Eating Habits” | |
| Pandemic and “Eating Behavior” | |
| Pandemic and “Feeding Behavior” | |
| Pandemic and “Eating Habits” | |
| Epidemic and “Eating Behavior” | |
| Epidemic and “Feeding Behavior” | |
| Epidemic and “Eating Habits” | |
| Loneliness and “Eating Behavior” | |
| Loneliness and “Feeding Behavior” | |
| Loneliness and “Eating Habits” | |
| H1N1 and “Eating Behavior” | |
| H1N1 and “Feeding Behavior” | |
| H1N1 and “Eating Habits” | |
| SARS-CoV and “Eating Behavior” | |
| SARS-CoV and “Feeding Behavior” | |
| SARS-CoV and “Eating Habits” | |
| COVID-19 and “Eating Behavior” | |
| COVID-19 and “Feeding Behavior” | |
| COVID-19 and “Eating Habits” | |
| Ebola and “Eating Behavior” | |
| Ebola and “Feeding Behavior” | |
| Ebola and “Eating Habits” |
Appendix B
| Selection | Compatibility | Outcome | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study (First Author) | Representativenesof the Sample | Sample Size | Non-Respondents | Acertainment of Exposure | Subtotal | Based on Design and Analysis | Subtotal | Assessment of Outcome | Statistical Test | Subtotal | Total | Risk of Bias |
| Ammar et al., 2020 | 1 | 1 | 0 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 7 | Average |
| Di Renzo et al., 2020 | 1 | 1 | 0 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 7 | Average |
| Phillipou et al., 2020 | 1 | 1 | 0 | 1 | 3 | 0 | 0 | 1 | 0 | 1 | 4 | Hihg |
| Rodríguez-Pérez et al., 2020 | 1 | 1 | 0 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 7 | Average |
| Romeo-Arroyo et al., 2020 | 1 | 0 | 0 | 1 | 2 | 1 | 1 | 1 | 0 | 1 | 4 | Hihg |
| Serin & Can Koç, 2020 | 1 | 1 | 0 | 2 | 4 | 2 | 2 | 1 | 1 | 2 | 8 | Average |
| Sidor and Rzymski, 2020 | 1 | 1 | 0 | 1 | 3 | 2 | 2 | 1 | 1 | 2 | 7 | Average |
References
- Lu, H.; Stratton, C.W.; Tang, Y. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef]
- Organização Pan-Americana da Saúde. Folha Informativa COVID-19-Escritório da OPAS e da OMS no Brasil. Available online: https://www.paho.org/pt/covid19 (accessed on 10 January 2020).
- Oliver, N.; Barber, X.; Roomp, K.; Roomp, K. Assessing the Impact of the COVID-19 Pandemic in Spain: Large-Scale, Online, Self-Reported Population Survey. J. Med Internet Res. 2020, 22, e21319. [Google Scholar] [CrossRef]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Social participation and life satisfaction of peoples during the COVID-19 home confinement: The ECLB-COVID19 mul-ticenter study. MedRxiv 2020, 5. Available online: https://www.medrxiv.org/content/10.1101/2020.05.05.20091066v1 (accessed on 18 February 2021).
- World Health Organization (WHO). Novel Coronavirus (2019-Ncov) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 1 October 2020).
- Horton, R. Offline: COVID-19 is not a pandemic. Lancet 2020, 396, 874. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Gan, Y.; Ding, X.; Wu, J.; Duan, H. The relationship between perceived stress and emotional distress during the COVID-19 outbreak: Effects of boredom proneness and coping style. J. Anxiety Disord. 2021, 77, 102328. [Google Scholar] [CrossRef]
- Chao, M.; Chen, X.; Liu, T.; Yang, H.; Hall, B.J. Psychological distress and state boredom during the COVID-19 outbreak in China: The role of meaning in life and media use. Eur. J. Psychotraumatol. 2020, 11, 1769379. [Google Scholar] [CrossRef] [PubMed]
- Skoda, E.-M.; Bäuerle, A.; Schweda, A.; Dörrie, N.; Musche, V.; Hetkamp, M.; Kohler, H.; Teufel, M.; Weismüller, B. Severely increased generalized anxiety, but not COVID-19-related fear in individuals with mental illnesses: A population based cross-sectional study in Germany. Int. J. Soc. Psychiatry 2020. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef]
- Gibson-Smith, D.; Bot, M.; Brouwer, I.A.; Visser, M.; Giltay, E.J.; Penninx, B.W.J.H. Association of food groups with depression and anxiety disorders. Eur. J. Nutr. 2019, 59, 767–778. [Google Scholar] [CrossRef]
- Yannakoulia, M.; Panagiotakos, D.B.; Pitsavos, C.; Tsetsekou, E.; Fappa, E.; Papageorgiou, C.; Stefanadis, C. Eating habits in relations to anxiety symptoms among apparently healthy adults. A pattern analysis from the ATTICA Study. Appetite 2008, 51, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Järvelä-Reijonen, E.; Karhunen, L.; Sairanen, E.; Rantala, S.; Laitinen, J.; Puttonen, S.; Peuhkuri, K.; Hallikainen, M.; Juvonen, K.; Myllymäki, T.; et al. High perceived stress is associated with unfavorable eating behavior in overweight and obese Finns of working age. Appetite 2016, 103, 249–258. [Google Scholar] [CrossRef]
- Torres, S.J.; Nowson, C.A. Relationship between stress, eating behavior, and obesity. Nutr. 2007, 23, 887–894. [Google Scholar] [CrossRef]
- Martínez-De-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical activity, dietary habits and sleep quality before and during COVID-19 lockdown: A longitudinal study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gong, X.; Wang, L.; Guo, J. Effects of hypertension, diabetes and coronary heart disease on COVID-19 diseases severity: A systematic review and meta-analysis. medRxiv 2020, 3, 20043133. [Google Scholar] [CrossRef]
- Fang, L.; Karakiulakis, G.; Roth, M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir. Med. 2020, 8, e21. [Google Scholar] [CrossRef]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, J.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High Prevalence of Obesity in Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) Requiring Invasive Mechanical Ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Kalligeros, M.; Shehadeh, F.; Mylona, E.K.; Benitez, G.; Beckwith, C.G.; Chan, P.A.; Mylonakis, E. Association of Obesity with Disease Severity Among Patients with Coronavirus Disease 2019. Obesity 2020, 28, 1200–1204. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Food and Nutrition Tips During Self-Quarentine. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-COVID-19/publications-and-technical-guidance/food-and-nutrition-tips-during-self-quarantine (accessed on 10 January 2020).
- Garritty, C.; Gartlehner, G.; Kamel, C.; King, V.J.; Nussbaumer-Streit, B.; Stevens, A.; Hamel, C.; Affengruber, L. Cochrane Rapid Reviews. Interim Guidance from the Cochrane Rapid Reviews Methods Group. Available online: https://methods.cochrane.org/rapidreviews/sites/methods.cochrane.org.rapidreviews/files/public/uploads/cochrane_rr_-_guidance-23mar2020-final.pdf (accessed on 11 January 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? a systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Oremus, M.; Oremus, C.; Hall, G.B.C.; McKinnon, M.C.; ECT & Cognition Systematic Review Team. Inter-rater and test–retest reliability of quality assessments by novice student raters using the Jadad and Newcastle–Ottawa Scales. BMJ Open 2012, 2, e001368. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, C.; Molina-Montes, E.; Verardo, V.; Artacho, R.; García-Villanova, B.; Guerra-Hernández, E.J.; Ruíz-López, M.D. Changes in Dietary Behaviours during the COVID-19 Outbreak Confinement in the Spanish COVIDiet Study. Nutrients 2020, 12, 1730. [Google Scholar] [CrossRef]
- Serin, E.; Can Koç, M. Examination of the eating behaviours and depression states of the university students who stay at home during the coronavirus pandemic in terms of different variables. Prog. Nutr. 2020, 22, 33–43. [Google Scholar] [CrossRef]
- Sidor, A.; Rzymski, P. Dietary Choices and Habits during COVID-19 Lockdown: Experience from Poland. Nutrients 2020, 12, 1657. [Google Scholar] [CrossRef]
- Phillipou, A.; Meyer, D.; Neill, E.; Tan, E.J.; Toh, W.L.; Van Rheenen, T.E.; Rossell, S.L. Eating and exercise behaviors in eating disorders and the general population during the COVID-19 pandemic in Australia: Initial results from the COLLATE project. Int. J. Eat. Disord. 2020, 53, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Romeo-Arroyo, E.; Mora, M.; Vázquez-Araújo, L. Consumer behavior in confinement times: Food choice and cooking attitudes in Spain. Int. J. Gastron. Food Sci. 2020, 21, 100226. [Google Scholar] [CrossRef]
- Hou, F.; Xu, S.; Zhao, Y.; Lu, Q.; Zhang, S.; Zu, P.; Sun, Y.; Su, P.; Tao, F. Effects of emotional symptoms and life stress on eating behaviors among adolescents. Appetite 2013, 68, 63–68. [Google Scholar] [CrossRef]
- Koball, A.M.; Meers, M.R.; Storfer-Isser, A.; Domoff, S.E.; Musher-Eizenman, D.R. Eating when bored: Revision of the Emotional Eating Scale with a focus on boredom. Health Psychol. 2012, 31, 521–524. [Google Scholar] [CrossRef]
- Biviá-Roig, G.; La Rosa, V.L.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J.F. Analysis of the Impact of the Confinement Resulting from COVID-19 on the Lifestyle and Psychological Wellbeing of Spanish Pregnant Women: An Internet-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Kapczinski, F.; Cardoso, T.D.A.; Atienza-Carbonell, B.; Rosa, A.R.; Mota, J.C.; De Boni, R.B. The assessment of lifestyle changes during the COVID-19 pandemic using a multidimensional scale. Rev. Psiquiatr. Salud Mental 2021, 14, 16–26. [Google Scholar] [CrossRef]
- Opichka, K.; Smith, C.; Levine, A.S. Problematic Eating Behaviors Are More Prevalent in African American Women Who Are Overweight or Obese Than African American Women Who Are Lean or Normal Weight. Fam. Community Health 2019, 42, 81–89. [Google Scholar] [CrossRef]
- Barrington, W.E.; Beresford, S.A.A. Eating Occasions, Obesity and Related Behaviors in Working Adults: Does it Matter When You Snack? Nutr. 2019, 11, 2320. [Google Scholar] [CrossRef]
- Guajardo, E.G.P.; Peña, C.M. Ansiedad, Estrés y Obesidad en una muestra de adolescentes de México Anxiety, Stress and Obesity in a sample of adolescents in Mexico. Univ. Psychol. 2017, 16, 1. [Google Scholar] [CrossRef]
- Jayne, J.M.; Ayala, R.; Karl, J.P.; Deschamps, B.A.; McGraw, S.M.; O’Connor, K.; DiChiara, A.J.; Cole, R.E. Body weight status, perceived stress, and emotional eating among US Army Soldiers: A mediator model. Eat. Behav. 2020, 36, 101367. [Google Scholar] [CrossRef] [PubMed]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. Ser. A Boil. Sci. Med Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [PubMed]
- Panno, A.; Carbone, G.A.; Massullo, C.; Farina, B.; Imperatori, C. COVID-19 Related Distress Is Associated with Alcohol Problems, Social Media and Food Addiction Symptoms: Insights from the Italian Experience During the Lockdown. Front. Psychiatry 2020, 11, 577135. [Google Scholar] [CrossRef]
- Ul-Haq, Z.; Mackay, D.F.; Fenwick, E.; Pell, J.P. Meta-analysis of the association between body mass index and health-related quality of life among adults, assessed by the SF-36. Obesity 2012, 21, E322–E327. [Google Scholar] [CrossRef]
- Emilien, C.; Hollis, J.H. A brief review of salient factors influencing adult eating behaviour. Nutr. Res. Rev. 2017, 30, 233–246. [Google Scholar] [CrossRef]
- Puhl, R.M.; Lessard, L.M.; Larson, N.; E Eisenberg, M.; Neumark-Stzainer, D. Weight Stigma as a Predictor of Distress and Maladaptive Eating Behaviors During COVID-19: Longitudinal Findings from the EAT Study. Ann. Behav. Med. 2020, 54, 738–746. [Google Scholar] [CrossRef]
- Garcia, G.D.; Pompeo, D.A.; Eid, L.P.; Cesarino, C.B.; Pinto, M.H.; Gonçalves, L.W.P. Relationship between anxiety, depressive symptoms and compulsive overeating disorder in patients with cardiovascular diseases. Rev. Lat. Am. Enferm. 2018, 26, 3040. [Google Scholar] [CrossRef]
- Eertmans, A.; Baeyens, F.; Bergh, O.V.D. Food likes and their relative importance in human eating behavior: Review and preliminary suggestions for health promotion. Health Educ. Res. 2001, 16, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Okumus, B.; Ozturk, A.B. The impact of perceived stress on US millennials’ external and emotional eating behavior. Br. Food J. 2020, 123, 1–11. [Google Scholar] [CrossRef]
- Flaudias, V.; Iceta, S.; Zerhouni, O.; Rodgers, R.F.; Billieux, J.; Llorca, P.-M.; Boudesseul, J.; De Chazeron, I.; Romo, L.; Maurage, P.; et al. COVID-19 pandemic lockdown and problematic eating behaviors in a student population. J. Behav. Addict. 2020, 24, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Uğurlu, Y.K.; Değirmenci, D.M.; Durgun, H.; Uğur, H.G. The examination of the relationship between nursing students’ depression, anxiety and stress levels and restrictive, emotional, and external eating behaviors in COVID-19 social isolation process. Perspect. Psychiatr. Care 2020, 12703. [Google Scholar] [CrossRef]
- Canetti, L.; Bachar, E.; Berry, E.M. Food and emotion. Behav. Process. 2002, 60, 157–164. [Google Scholar] [CrossRef]
- Castellini, G.; Cassioli, E.; Rossi, E.; Innocenti, M.; Gironi, V.; Sanfilippo, G.; Felciai, F.; Monteleone, A.M.; Ricca, V. The impact of COVID-19 epidemic on eating disorders: A longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. Int. J. Eat. Disord. 2020, 53, 1855–1862. [Google Scholar] [CrossRef]
- Badrasawi, M.M.; Zidan, S.J. Binge eating symptoms prevalence and relationship with psychosocial factors among female undergraduate students at Palestine Polytechnic University: A cross-sectional study. J. Eat. Disord. 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]


| Author(s), Year, and Country | Sample | Findings | |
|---|---|---|---|
| Primary Outcome | Measure of Association | ||
| Ammar et al., 2020, international | 1047 adults aged >18 years. Male 46%, female 54%. Asian 36%, African 40%, European 21%, and 3% other countries. | During home confinement, people eat more uncontrollably compared to before the pandemic. During confinement, food intake increased, especially snacks and unhealthy food, compared to before the pandemic. | t = −9.44, p < 0.001, d = 0.22 Increased number of main meals: t = −5.83, p < 0.001, d = 0.22. Snacks consumption increased: t = −6.89, p < 0.001, d = 0.30. Ingestion of unhealthy food increased: t = −3.46, p < 0.001, d = 0.14 |
| Di Renzo et al., 2020, Italy | 3553 subjects, with a mean age of 40.03 ± 13.53. Female 76.1%. Mean BMI 27.66 ± 4.1 | During the COVID-19 emergency, there was a decrease in junk food intake; its intake was associated with a higher BMI and a younger age. During the COVID-19 emergency, the perception of weight gain was positive and inversely associated with a higher consumption of junk food and healthy food, a higher BMI, the female gender, and to a modified labor routine. | Decrease (29.8%) vs. increase (25,6%), r2 = 9.560, p = 0.002. BMI: OR = 1.025, p = 0.005. Age: OR = 0.979, p < 0.001 Junk food consumption: OR = 3.122, p < 0.001. Health food consumption: OR = 0.805, p = 0.002. BMI: OR = 1.073, p < 0.001. Modification of labor routine: OR = 1.250, p = 0.037 |
| Phillipou et al., 2020, Australia | 5289 adults, no report of ED, with a mean age of 40.62 ± 13.67. Female 80%. 180 adults with a self-report of ED, with a mean age of 30.47 ± 8.19. Female 95.6%. AN (n = 88), BN (n = 23), PBED (n = 6), EDNOS (n = 4), SE (n = 68). | Changes in eating styles were reported both in the population without ED and in those with ED, compared to the period before the COVID-19 emergency. | The levels of ERB and ECB increased 27.6% and 34.6% in people without ED, respectively, while the level of ERB, ECB, and FPB increased 64.5%, 35.5%, and 18.9% in people with ED, respectively. |
| Rodríguez-Pérez et al., 2020, Spain | 7514 adults >18 years. Female 70.6%. | During the confinement period, there was an increase in the level of adherence to MedDiet, compared to the prior period, and an increase of 8% for every five days of greater confinement. | Prior confinement: Md = 6.0 (1–13). During confinement: Md = 7.0, (1–13), p < 0.001 |
| Romeo-Arroyo, Mora & Vázquez-Araújo 2020, Spain | 600 adults, with a mean age of 42.58 ± 12.25. Female 50.1%. | A change in the intake of different types of food was reported. | A little over 50% increase in the consumption of sweets; 30% to 40% enlarged consumption of meats, fruits, eggs, rice, pasta, bread, sausages and cold cuts, vegetables, and dairy products, and 33% decreased fish consumption. |
| Serin & Can Koç, 2020, Turkey | 1064 adults >18 years. Female 58.64%. | The DEBQ results showed differences in “External Eating” behavior between people who were self-isolated during the pandemic versus those who were not. | Self-isolation Md = 26 (20–30) vs. no isolation Md = 23 (15–28.5), p < 0.01 |
| Sidor and Rzymski, 2020, Poland | 1097 adults with a mean age of 27.7 ± 9. Female 95.1%. Mean BMI of 23.5 ± 4.8 | During quarantine, weight gain was observed, which was correlated with BMI and age, especially in overweight, obese, and individuals over 35. There was an increase in food intake that was associated with a higher BMI versus those with a lower BMI. | BMI: Rs = 0.21, p < 0.05 Age: Rs = 0.15, p < 0.05 BMI: M = 22.9 ± 4.6; M = 24.1 ± 5.1, p < 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neira, C.; Godinho, R.; Rincón, F.; Mardones, R.; Pedroso, J. Consequences of the COVID-19 Syndemic for Nutritional Health: A Systematic Review. Nutrients 2021, 13, 1168. https://doi.org/10.3390/nu13041168
Neira C, Godinho R, Rincón F, Mardones R, Pedroso J. Consequences of the COVID-19 Syndemic for Nutritional Health: A Systematic Review. Nutrients. 2021; 13(4):1168. https://doi.org/10.3390/nu13041168
Chicago/Turabian StyleNeira, Cristian, Rejane Godinho, Fabio Rincón, Rodrigo Mardones, and Janari Pedroso. 2021. "Consequences of the COVID-19 Syndemic for Nutritional Health: A Systematic Review" Nutrients 13, no. 4: 1168. https://doi.org/10.3390/nu13041168
APA StyleNeira, C., Godinho, R., Rincón, F., Mardones, R., & Pedroso, J. (2021). Consequences of the COVID-19 Syndemic for Nutritional Health: A Systematic Review. Nutrients, 13(4), 1168. https://doi.org/10.3390/nu13041168