
Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children

 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384S–392S. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Muller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Moore, L.V.; Galuska, D.; Wright, A.P.; Harris, D.; Grummer-Strawn, L.M.; Merlo, C.L.; Nihiser, A.J.; Rhodes, D.G. Vital signs: Fruit and vegetable intake among children—United States, 2003–2010. Morb. Mortal. Wkly. Rep. 2014, 63, 671–676. [Google Scholar]
- Craigie, A.M.; Lake, A.A.; Kelly, S.A.; Adamson, A.J.; Mathers, J.C. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas 2011, 70, 266–284. [Google Scholar] [CrossRef]
- Thompson, F.; Subar, A. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease, 3rd ed.; Coulson, A., Boushey, C., Ferruzzi, M.G., Eds.; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Sherwood, N.E. Diet Assessment in Children and Adolescents. In Handbook of Childhood and Adolescent Obesity; Springer: Boston, MA, USA, 2008; pp. 73–89. [Google Scholar]
- Thompson, F.E.; Kirkpatrick, S.I.; Subar, A.F.; Reedy, J.; Schap, T.E.; Wilson, M.M.; Krebs-Smith, S.M. The National Cancer Institute’s Dietary Assessment Primer: A resource for diet Rrsearch. J. Acad. Nutr. Diet. 2015, 115, 1986–1995. [Google Scholar] [CrossRef] [PubMed]
- Krinsky, N.I.; Johnson, E.J. Carotenoid actions and their relation to health and disease. Mol. Aspects Med. 2005, 26, 459–516. [Google Scholar] [CrossRef]
- Monsen, E.R. Dietary reference intakes for the antioxidant nutrients: Vitamin C, vitamin E, selenium, and carotenoids. J. Am. Diet. Assoc. 2000, 100, 637–640. [Google Scholar] [CrossRef]
- Ermakov, I.V.; Sharifzadeh, M.; Ermakova, M.; Gellermann, W. Resonance Raman detection of carotenoid antioxidants in living human tissue. J. Biomed. Opt. 2005, 10. [Google Scholar] [CrossRef]
- Ermakov, I.V.; Gellermann, W. Optical detection methods for carotenoids in human skin. Arch. Biochem. Biophys. 2015, 572, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Rerksuppaphol, S.; Rerksuppaphol, L. Carotenoid intake and asthma prevalence in Thai children. Pediatr. Rep. 2012, 4, e12. [Google Scholar] [CrossRef]
- Nguyen, L.M.; Scherr, R.E.; Linnell, J.D.; Ermakov, I.V.; Gellermann, W.; Jahns, L.; Keen, C.L.; Miyamoto, S.; Steinberg, F.M.; Young, H.M.; et al. Evaluating the relationship between plasma and skin carotenoids and reported dietary intake in elementary school children to assess fruit and vegetable intake. Arch. Biochem. Biophys. 2015, 572, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Beccarelli, L.M.; Scherr, R.E.; Dharmar, M.; Ermakov, I.V.; Gellermann, W.; Jahns, L.; Linnell, J.D.; Keen, C.L.; Steinberg, F.M.; Young, H.M.; et al. Using skin carotenoids to assess dietary changes in students after 1 academic year of participating in the shaping healthy choices program. J. Nutr. Educ. Behav. 2017, 49, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, S.S.; Wengreen, H.J.; Dew, J. Skin carotenoid response to a highcarotenoid juice in children: A randomized clinical trial. J. Acad. Nutr. Diet 2015, 115, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Aguilar, S.S.; Wengreen, H.J.; Lefevre, M.; Madden, G.J.; Gast, J. Skin carotenoids: A biomarker of fruit and vegetable intake in children. J. Acad. Nutr. Diet 2014, 114, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Scarmo, S.; Henebery, K.; Peracchio, H.; Cartmel, B.; Lin, H.; Ermakov, I.V.; Gellermann, W.; Berstein, P.S.; Duffy, V.B.; Mayne, S.T. Skin carotenoid status measured by resonance Raman spectroscopy as a biomarker of fruit and vegetable intake in preschool children. Eur. J. Clin. Nutr. 2012, 66, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Radtke, M.D.; Pitts, S.J.; Jahns, L.; Firnhaber, G.C.; Loofbourrow, B.M.; Zeng, A.; Scherr, R.E. Criterion-Related Validity of Spectroscopy-Based Skin Carotenoid Measurements as a Proxy for Fruit and Vegetable Intake: A Systematic Review. Adv. Nutr. 2020, 11, 1282–1299. [Google Scholar] [CrossRef]
- Mayne, S.T.; Cartmel, B.; Scarmo, S.; Jahns, L.; Ermakov, I.V.; Gellermann, W. Resonance Raman spectroscopic evaluation of skin carotenoids as a biomarker of carotenoid status for human studies. Arch. Biochem. Biophys. 2013, 539, 163–170. [Google Scholar] [CrossRef]
- Moran, N.E.; Mohn, E.S.; Hason, N.; Erdman, J.W.; Johnson, E.J. Intrinsic and extrinsic factors impacting absorption, metabolism, and health effects of dietary carotenoids. Adv. Nutr. 2018, 9, 465–492. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Rock, C.L.; Eldridge, A.L.; Kristal, A.R.; Patterson, R.E.; Cooper, D.A.; Neumark-Sztainer, D.; Cheskin, L.J.; Thornquist, M.D. Serum concentrations of retinol, alpha-tocopherol and the carotenoids are influenced by diet, race and obesity in a sample of healthy adolescents. J. Nutr. 2001, 131, 2184–2191. [Google Scholar] [CrossRef] [PubMed]
- Burkholder, S.; Pitts, S.J.; Wu, Q.; Bayles, J.; Baybutt, R.; Stage, V.C. Skin Carotenoid Status Over Time and Differences by Age and Sex Among Head Start Children (3–5 Years). J. Nutr. Ed. Behav. 2020. [Google Scholar] [CrossRef]
- Sanjeevi, N.; Lipsky, L.; Liu, A.; Nansel, T. Differential reporting of fruit and vegetable intake among youth in a randomized controlled trial of a behavioral nutrition intervention. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.A.; Morgan, E.H.; Hanson, K.L.; Ammerman, A.S.; Pitts, S.B.J.; Kolodinsky, J.; Sitaker, M.; Becot, F.A.; Connor, L.M.; Garner, J.A.; et al. Farm Fresh Foods for Healthy Kids (F3HK): An innovative community supported agriculture intervention to prevent childhood obesity in low-income families and strengthen local agricultural economies. BMC Public Health 2017, 17. [Google Scholar] [CrossRef] [PubMed]
- Holden, J.M.; Eldridge, A.L.; Beecher, G.R.; Buzzard, I.M.; Bhagwat, S.; Davis, C.S.; Douglass, L.W.; Gebhardt, S.; Haytowitz, D.; Schakel, S. Carotenoid content of U.S. foods: An update of the database. J. Food Compos. Anal. 1999, 12, 169–196. [Google Scholar] [CrossRef]
- Collins, C.E.; Watson, J.; Burrows, T. Measuring dietary intake in children and adolescents in the context of overweight and obesity. Int. J. Obes. 2010, 34, 1103–1115. [Google Scholar] [CrossRef]
- National Cancer Institute Division of Cancer Control and Population Sciences. Epidemiology and Genomics Research Program. “Scoring the All-Day Screener”. Available online: https://epi.grants.cancer.gov/diet/screeners/fruitveg/scoring/allday.html#how (accessed on 11 November 2018).
- Greene, G.W.; Resnicow, K.; Thompson, F.E.; Peterson, K.E.; Hurley, T.G.; Hebert, J.R.; Toobert, D.J.; Williams, G.C.; Elliot, D.L.; Sher, T.G.; et al. Correspondence of the NCI Fruit and Vegetable Screener to repeat 24-h recalls and serum carotenoids in behavioral intervention trials. J. Nutr. 2008, 138, 200S–204S. [Google Scholar] [CrossRef] [PubMed]
- Peterson, K.E.; Hebert, J.R.; Hurley, T.G.; Resnicow, K.; Thompson, F.E.; Greene, G.W.; Shaikh, A.R.; Yaroch, A.L.; Williams, G.C.; Salkeld, J.; et al. Accuracy and precision of two short screeners to assess change in fruit and vegetable consumption among diverse populations participating in health promotion intervention trials. J. Nutr. 2008, 138, 218S–225S. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F.; Smith, A.F.; Midthune, D.; Radimer, K.L.; Kahle, L.L.; Kipnis, V. Fruit and vegetable assessment: Performance of 2 new short instruments and a food frequency questionnaire. J. Am. Diet. Assoc. 2002, 102, 1764–1772. [Google Scholar] [CrossRef]
- National Cancer Institute. Automated Self-Administered 24-Hour Recall (ASA-24); National Cancer Institute: Bethesda, MD, USA, 2014. [Google Scholar]
- U.S. Department of Health and Human Services; U.S. Department of Agriculture. 2015—2020 Dietary Guidelines for Americans, 8th ed.; Health and Human Services Dept.: Washington, DC, USA, 2015. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat. 2002, 11, 1–190. [Google Scholar]
- Jilcott Pitts, S.B.; Johnson, N.; Wu, Q.; Firnhaber, G.; Kaur, A.; Obasohan, J. A meta-analysis of studies examining associations between resonance Raman spectroscopy-assessed skin carotenoids and plasma carotenoids among adults and children. Nutr. Rev. 2021. accepted. [Google Scholar]
- Jahns, L.; Johnson, L.K.; Conrad, Z.; Bukowski, M.; Raatz, S.K.; Jilcott Pitts, S.; Wang, Y.; Ermakov, I.V.; Gellermann, W. Concurrent validity of skin carotenoid status as a concentration biomarker of vegetable and fruit intake compared to multiple 24-h recalls and plasma carotenoid concentrations across one year: A cohort study. Nutr. J. 2019, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Scarmo, S.; Cartmel, B.; Lin, H.Q.; Leffell, D.J.; Ermakov, I.V.; Gellermann, W.; Bernstein, P.S.; Mayne, S.T. Single v. multiple measures of skin carotenoids by resonance Raman spectroscopy as a biomarker of usual carotenoid status. Br. J. Nutr. 2013, 110, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.H.; Graham, M.L.; Marshall, G.A.; Hanson, K.L.; Seguin-Fowler, R.A. Serum Carotenoids Are Strongly Associated with Dermal Carotenoids but Not Self-reported Fruit and Vegetable Intake among Overweight and Obese Women. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 104. [Google Scholar] [CrossRef] [PubMed]
- Jilcott Pitts, S.; Jahns, L.; Wu, Q.; Moran, N.; Bell, R.; Truesdale, K.; Laska, M. A non-invasive assessment of skin carotenoid status through reflection spectroscopy is a feasible, reliable and potentially valid measure of fruit and vegetable consumption in a diverse community sample. Public Health Nutr. 2018, 21, 1664–1670. [Google Scholar] [CrossRef]
- Yaroch, A.L.; Tooze, J.; Thompson, F.E.; Blanck, H.M.; Thompson, O.M.; Colon-Ramos, U.; Shaikh, A.R.; McNutt, S.; Nebeling, L.C. Evaluation of three short dietary instruments to assess fruit and vegetable intake: The National Cancer Institute’s food attitudes and behaviors survey. J. Acad. Nutr. Diet. 2012, 112, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Trends in adolescent fruit and vegetable consumption, 1999–2004: Project EAT. Am. J. Prev. Med. 2007, 32, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Demory-Luce, D.; Morales, M.; Nicklas, T.; Baranowski, T.; Zakeri, I.; Berenson, G. Changes in food group consumption patterns from childhood to young adulthood: The Bogalusa Heart Study. J. Am. Diet. Assoc. 2004, 104, 1684–1691. [Google Scholar] [CrossRef] [PubMed]
- Comparative Climatic Data: Cloudiness—Mean Number of Days. Available online: https://www1.ncdc.noaa.gov/pub/data/ccd-data/clpcdy18.dat (accessed on 26 March 2020).
- Geocoder. Available online: https://geocoding.geo.census.gov/ (accessed on 26 March 2020).
- Mayne, S.T.; Cartmel, B.; Scarmo, S.; Lin, H.; Leffell, D.J.; Welch, E.; Ermakov, I.; Bhosale, P.; Bernstein, P.S.; Gellermann, W. Noninvasive assessment of dermal carotenoids as a biomarker of fruit and vegetable intake. Am. J. Clin. Nutr. 2010, 92, 794–800. [Google Scholar] [CrossRef]


{kind=link}
| Mean | SD | Count | Percent | |
|---|---|---|---|---|
| Characteristics | ||||
| Age (years) | 5.9 | 2.8 | ||
| Sex | ||||
| Female | 94 | 53.1 | ||
| Male | 83 | 46.9 | ||
| Race | ||||
| Black/African-American | 15 | 8.5 | ||
| White | 131 | 74.0 | ||
| Multi-racial/other 1 | 31 | 17.5 | ||
| Hispanic | 9 | 5.1 | ||
| State | ||||
| New York | 66 | 37.3 | ||
| North Carolina | 22 | 12.4 | ||
| Vermont | 50 | 28.2 | ||
| Washington | 39 | 22.0 | ||
| Health-related Factors | ||||
| General health status | ||||
| Excellent | 74 | 41.8 | ||
| Very good | 68 | 38.4 | ||
| Good | 30 | 16.9 | ||
| Fair | 5 | 2.8 | ||
| Poor | 0 | 0.0 | ||
| Smoker(s) in household | 28 | 15.8 | ||
| BMI-for-age percentile | 66.8 | 30.2 | ||
| Dietary Intake | ||||
| Total FV intake (NCI FV cups) | 3.7 | 3.5 | ||
| Total FV intake (24H FV cups) | 2.7 | 1.5 | ||
| Total energy intake (%EER) 2 | 114.6 | 33.5 | ||
| Daily fat intake (%kcal) | 34.4 | 6.4 |
| Unadjusted Model | Field-Based Model | Research-Setting Model | ||||
|---|---|---|---|---|---|---|
| β | SE | β | SE | β | SE | |
| Log NCI FV cups | 2265.7 | 1737.3 | 1067.4 | 1673.9 | 1198.7 | 1679.4 |
| Age (years) | −1111.2 ** | 340.3 | −1042.6 ** | 341.7 | ||
| White (ref) | ||||||
| Black/African-American | −1435.0 | 4000.0 | −1741.6 | 3991.0 | ||
| Multi-racial/other | 1341.7 | 2581.4 | 796.3 | 2575.3 | ||
| Hispanic | −3360.0 | 4675.7 | −2725.3 | 4660.5 | ||
| New York (ref) | ||||||
| North Carolina | −11,660.8 ** | 3520.3 | −11,944.6 *** | 3529.6 | ||
| Vermont | −2295.6 | 2437.0 | −2817.0 | 2427.5 | ||
| Washington | −5710.1 * | 2593.8 | −6236.6 * | 2616.5 | ||
| Smoker(s) in household | −930.7 | 2659.5 | −1139.4 | 2639.2 | ||
| BMI-for-age (percentile) | −31.0 | 33.4 | ||||
| Total energy (%EER) | 10.6 | 29.9 | ||||
| Daily fat intake (%kcal) | 356.9 * | 156.3 | ||||
| R2 | 0.01 | 0.16 | 0.19 | |||
| R2 change | 0.15 *** | 0.03 | ||||
| Log 24H FV cups | 8016.0 ** | 2612.3 | 7458.7 ** | 2510.9 | 9637.6 *** | 2697.1 |
| Age (years) | −1096.4 ** | 331.3 | −1072.7 ** | 328.8 | ||
| White (ref) | ||||||
| Black/African-American | −1546.4 | 3890.4 | −2028.0 | 3842.0 | ||
| Multi-racial/other | 51.1 | 2553.9 | −820.0 | 2522.1 | ||
| Hispanic | −4089.0 | 4546.2 | −3405.3 | 4472.9 | ||
| New York (ref) | ||||||
| North Carolina | −11,104.0 ** | 3434.5 | −12,005.4 *** | 3399.4 | ||
| Vermont | −2578.0 | 2379.7 | −3113.0 | 2343.1 | ||
| Washington | −6382.2 * | 2525.3 | −7049.3 ** | 2513.8 | ||
| Smoker(s) in household | −824.3 | 2589.1 | −933.0 | 2541.1 | ||
| BMI-for-age (percentile) | −20.7 | 32.2 | ||||
| Total energy (%EER) | −27.0 | 30.8 | ||||
| Daily fat intake (%kcal) | 486.8 ** | 155.2 | ||||
| R2 | 0.05 | 0.20 | 0.25 | |||
| R2 change | 0.15 *** | 0.05 * | ||||
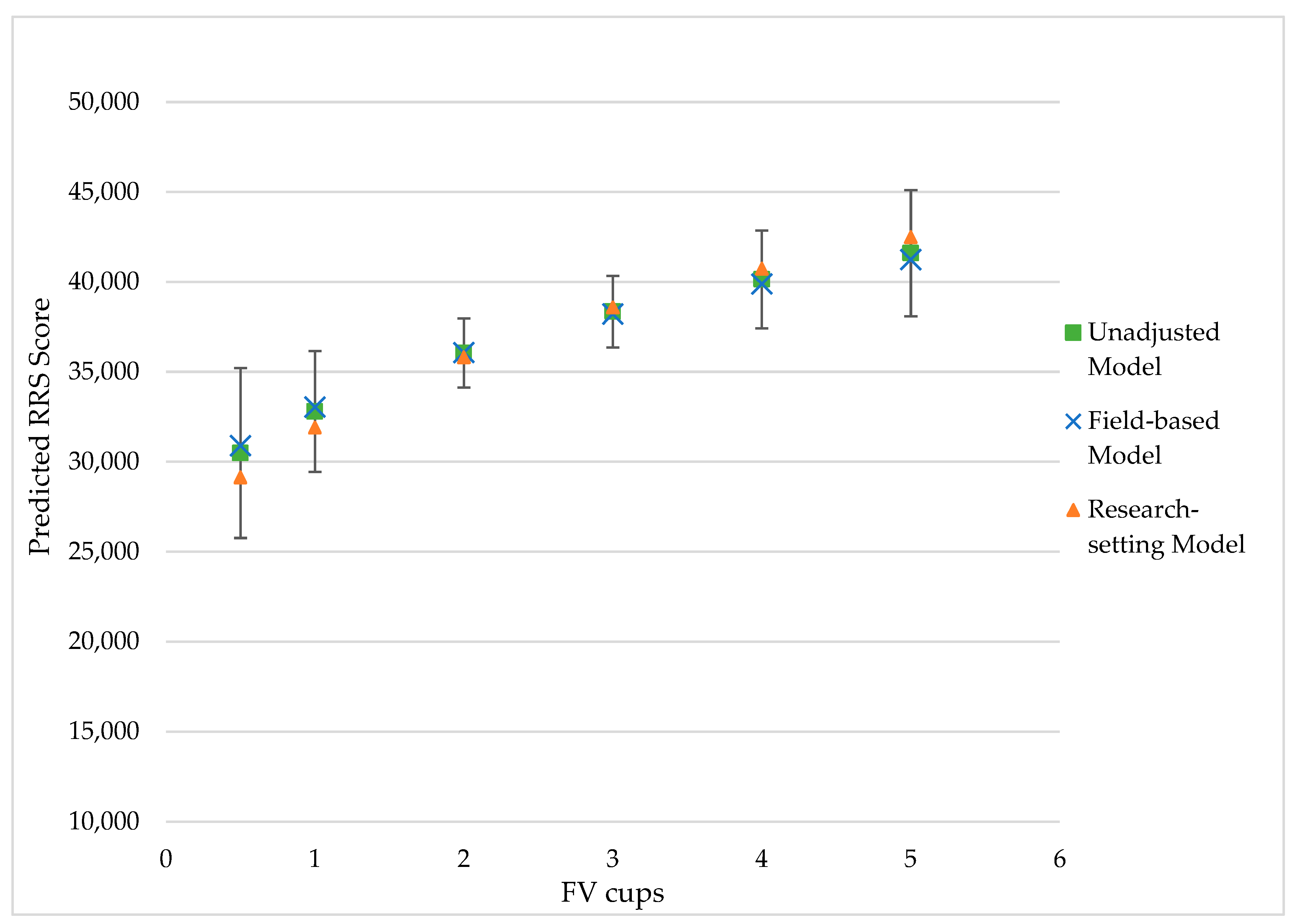
| Unadjusted Model | Field-Based Model | Research-Setting Model | ||||
|---|---|---|---|---|---|---|
| Predicted Value | Margin of Error (±) | Predicted Value | Margin of Error (±) | Predicted Value | Margin of Error (±) | |
| FV cups | ||||||
| 0.5 | 30,489.8 | 4667.1 | 30,902.2 | 4467.9 | 29,133.8 | 4728.9 |
| 1.0 | 32,795.9 | 3378.4 | 33,048.0 | 3221.6 | 31,906.4 | 3363.1 |
| 2.0 | 36,046.1 | 2066.4 | 36,072.2 | 1943.8 | 35,814.1 | 1924.8 |
| 3.0 | 38,352.2 | 2121.8 | 38,218.0 | 1998.9 | 38,586.7 | 1991.0 |
| 4.0 | 40,140.9 | 2777.0 | 39,882.3 | 2639.2 | 40,737.2 | 2719.9 |
| 5.0 | 41,602.4 | 3507.0 | 41,242.2 | 3347.9 | 42,494.4 | 3507.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seguin-Fowler, R.A.; Hanson, K.L.; Marshall, G.A.; Belarmino, E.H.; Jilcott Pitts, S.B.; Kolodinsky, J.; Sitaker, M.; Ammerman, A. Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children. Nutrients 2021, 13, 980. https://doi.org/10.3390/nu13030980
Seguin-Fowler RA, Hanson KL, Marshall GA, Belarmino EH, Jilcott Pitts SB, Kolodinsky J, Sitaker M, Ammerman A. Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children. Nutrients. 2021; 13(3):980. https://doi.org/10.3390/nu13030980
Chicago/Turabian StyleSeguin-Fowler, Rebecca A., Karla L. Hanson, Grace A. Marshall, Emily H. Belarmino, Stephanie B. Jilcott Pitts, Jane Kolodinsky, Marilyn Sitaker, and Alice Ammerman. 2021. "Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children" Nutrients 13, no. 3: 980. https://doi.org/10.3390/nu13030980
APA StyleSeguin-Fowler, R. A., Hanson, K. L., Marshall, G. A., Belarmino, E. H., Jilcott Pitts, S. B., Kolodinsky, J., Sitaker, M., & Ammerman, A. (2021). Fruit and Vegetable Intake Assessed by Repeat 24 h Recalls, but Not by A Dietary Screener, Is Associated with Skin Carotenoid Measurements in Children. Nutrients, 13(3), 980. https://doi.org/10.3390/nu13030980