
Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study

 ,
,  , , , , , , and
, , , , , , and
Abstract
1. Introduction
2. Materials and Methods
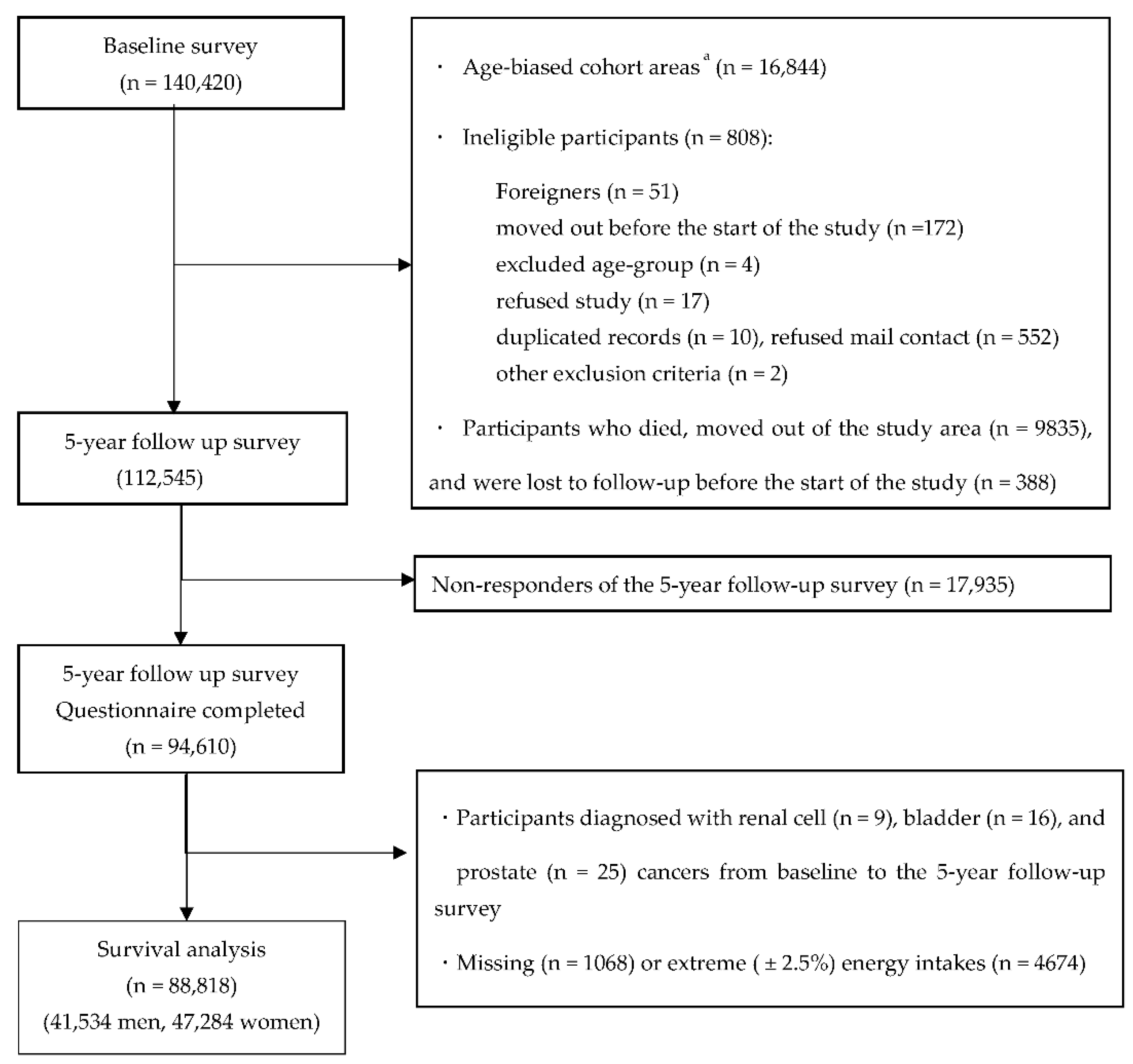
2.1. Study Participants
2.2. Acrylamide Intake Assessment
2.3. Follow-Up and Identification of Cancer Cases
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer. Some Industrial Chemicals. IARC Monogr. Eval. Carcinog. Risk Chem. Hum. 1994, 60, 560. [Google Scholar]
- Johnson, K.A.; Gorzinski, S.J.; Bodner, K.M.; Campbell, R.A.; Wolf, C.H.; Friedman, M.A.; Mast, R.W. Chronic Toxicity and Oncogenicity Study on Acrylamide Incorporated in the Drinking Water of Fischer 344 Rats. Toxicol. Appl. Pharmacol. 1986, 85, 154–168. [Google Scholar] [CrossRef]
- Friedman, M.A.; Dulak, L.H.; Stedham, M.A. A Lifetime Oncogenicity Study in Rats with Acrylamide. Fundam. Appl. Toxicol. 1995, 27, 95–105. [Google Scholar] [CrossRef]
- Besaratinia, A.; Pfeifer, G.P. A Review of Mechanisms of Acrylamide Carcinogenicity. Carcinogenesis 2007, 28, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Tareke, E.; Rydberg, P.; Karlsson, P.; Eriksson, S.; Törnqvist, M. Analysis of Acrylamide, a Carcinogen Formed in Heated Foodstuffs. J. Agric. Food Chem. 2002, 50, 4998–5006. [Google Scholar] [CrossRef]
- Hogervorst, J.G.; Schouten, L.J.; Konings, E.J.; Goldbohm, R.A.; van den Brandt, P.A. Dietary Acrylamide Intake and the Risk of Renal Cell, Bladder, and Prostate Cancer. Am. J. Clin. Nutr. 2008, 87, 1428–1438. [Google Scholar] [CrossRef]
- Hirvonen, T.; Kontto, J.; Jestoi, M.; Valsta, L.; Peltonen, K.; Pietinen, P.; Virtanen, S.M.; Sinkko, H.; Kronberg-Kippilä, C.; Albanes, D.; et al. Dietary Acrylamide Intake and the Risk of Cancer Among Finnish Male Smokers. Cancer Causes Control 2010, 21, 2223–2229. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Bosetti, C.; Galeone, C.; La Vecchia, C. Dietary acrylamide and cancer risk: An updated meta-analysis. Int. J. Cancer. 2015, 136, 2912–2922. [Google Scholar] [CrossRef] [PubMed]
- Kotemori, A.; Ishihara, J.; Nakadate, M.; Sawada, N.; Iwasaki, M.; Sobue, T.; Tsugane, S. Validity of a Self-Administered Food Frequency Questionnaire for the Estimation of Acrylamide Intake in the Japanese Population: The JPHC FFQ Validation Study. J. Epidemiol. 2018, 28, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Konings, E.J.; Hogervorst, J.G.; Rooij, L.; Schouten, L.J.; Sizoo, E.A.; Van Egmond, H.P.; Goldbohm, R.; Van Den Brandt, P.A. Validation of a Database on Acrylamide for Use in Epidemiological Studies. Eur. J. Clin. Nutr. 2010, 64, 534–540. [Google Scholar] [CrossRef]
- Watanabe, S.; Tsugane, S.; Sobue, T.; Konishi, M.; Baba, S. Study Design and Organization of the JPHC Study. Japan Public Health Center-Based Prospective Study on Cancer and Cardiovascular Disease. J. Epidemiol. 2011, 11 (Suppl. 6), S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S.; Sawada, N. The JPHC Study: Design and Some Findings on the Typical Japanese Diet. Jpn. J. Clin. Oncol. 2014, 44, 777–782. [Google Scholar] [CrossRef]
- Tsugane, S.; Sasaki, S.; Kobayashi, M.; Tsubono, Y.; Akabane, M.; JPHC. Validity and Reproducibility of the Self-Administered Food Frequency Questionnaire in the JPHC Study Cohort I: Study Design, Conduct and Participant Profiles. J. Epidemiol. 2003, 13 (Suppl. 1), S2–S12. [Google Scholar] [CrossRef]
- Ishihara, J.; Inoue, M.; Kobayashi, M.; Tanaka, S.; Yamamoto, S.; Iso, H.; Tsugane, S.; JPHC FFQ Validation Study Group. Impact of the Revision of a Nutrient Database on the Validity of a Self-Administered Food Frequency Questionnaire (FFQ). J. Epidemiol. 2006, 16, 107–116. [Google Scholar]
- Ishihara, J.; Sobue, T.; Yamamoto, S.; Yoshimi, I.; Sasaki, S.; Kobayashi, M.; Takahashi, T.; Iitoi, Y.; Akabane, M.; Tsugane, S.; et al. Validity and Reproducibility of a Self-Administered Food Frequency Questionnaire in the JPHC Study Cohort II: Study Design, Participant Profile and Results in Comparison with Cohort I. J. Epidemiol. 2003, 13 (Suppl. 1), S134–S147. [Google Scholar] [CrossRef] [PubMed]
- Resource Council, Science and Technology Agency; the Government of Japan. Standard Tables of Food Composition in Japan, 5th ed.; Printing Bureau, Ministry of Finance: Tokyo, Japan, 2002.
- Kito, K.; Ishihara, J.; Yamamoto, J.; Hosoda, T.; Kotemori, A.; Takachi, R.; Nakamura, K.; Tanaka, J.; Yamaji, T.; Shimazu, T.; et al. Variations in the estimated intake of acrylamide from food in the Japanese polulation. Nutr. J. 2020, 19, 17. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Environmental Studies, Japan. Study on Statistical Estimate of Acrylamide Intake from Foods. Available online: http://www.fsc.go.jp/fsciis/technicalResearch/show/cho99920141408 (accessed on 15 July 2019).
- Ministry of Agriculture, Forestry and Fisheries. Risk Profile Sheet Relating to the Food Safety; for Acrylamide. Available online: http://www.maff.go.jp/j/syouan/seisaku/risk_analysis/priority/pdf/150807_rp_aa.pdf (accessed on 1 July 2019).
- Mizukami, Y.; Kohata, K.; Yamaguchi, Y.; Hayashi, N.; Sawai, Y.; Chuda, Y.; Ono, H.; Yada, H.; Yoshida, M. Analysis of Acrylamide in Green Tea by Gas Chromatography-Mass Spectrometry. J. Agric. Food Chem. 2006, 54, 7370–7377. [Google Scholar] [CrossRef]
- Takatsuki, S.; Nemoto, S.; Sasaki, K.; Maitani, T. Production of Acrylamide in Agricultural Products by Cooking. Shokuhin Eiseigaku Zasshi. 2004, 45, 44–48. [Google Scholar] [CrossRef][Green Version]
- Yoshida, M.; Miyoshi, K.; Horibata, K.; Mizukami, Y.; Takenaka, M.; Yasui, A. Estimation of Acrylamide Intake from Cooked Rice in Japan. Nippon Shokuhin Kagaku Kogaku Kaishi 2011, 58, 525–530. [Google Scholar] [CrossRef][Green Version]
- FAO/WHO. Health Implications of Acrylamide in Food; Report of a Joint FAO/WHO Consultation; FAO/WHO: Quebec City, QC, Canada, 2002. [Google Scholar]
- Food Safety Commission of Japan. Information Clearing Sheet for Acrylamide. (In Japanese). Available online: https://www.fsc.go.jp/fsciis/attachedFile/download?retrievalId=kai20111222sfc&fileId=520 (accessed on 1 August 2019).
- Schettgen, T.; Rossbach, B.; Kütting, B.; Letzel, S.; Drexler, H.; Angerer, J. De Termination of Haemoglobin Adducts of Acrylamide and Glycidamide in Smokin g and non-Sm Oking Persons of the General Population. Int. J. Hyg. Environ. Health 2004, 207, 531–539. [Google Scholar] [CrossRef]
- Mucci, L.A.; Dickman, P.W.; Steineck, G.; Adami, H.O.; Augustsson, K. Dietary Acrylamide and Cancer of the Large Bowel, Kidney, and Bladder: Absence of an Association in a Population-Based Study in Sweden. Br. J. Cancer 2003, 88, 84–89. [Google Scholar] [CrossRef]
- Mucci, L.A.; Lindblad, P.; Steineck, G.; Adami, H.O. Dietary Acrylamide and Risk of Renal Cell Cancer. Int. J. Cancer 2004, 109, 774–776. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Hodge, R.A.; Um, C.Y.; Gapstur, S.M. Dietary Acrylamide Is Not Associated with Renal Cell Cancer Risk in the CPS-II Nutrition Cohort. Cancer Epidemiol. Biomark. Prev. 2019, 28, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, L.; Sonderman, J.S.; Tarone, R.E.; McLaughlin, J.K. Review of Epidemiologic Studies of Dietary Acrylamide Intake and the Risk of Cancer. Eur. J. Cancer Prev. 2012, 21, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Food Safety Commission of Japan. Evaluation report of Acrylamide generated during heating. Internet. Available online: https://www.fsc.go.jp/osirase/acrylamide1.data/acrylamide_hyokasyo1.pdf (accessed on 24 July 2019).
- Shipp, A.; Lawrence, G.; Gentry, R.; McDonald, T.; Bartow, H.; Bounds, J.; Macdonald, N.; Clewell, H.; Allen, B.; Van Landingham, C. Acrylamide: Review of Toxicity Data and Dose-Response Analyses for Cancer and Noncancer Effects. Crit. Rev. Toxicol. 2006, 36, 481–608. [Google Scholar] [CrossRef]
- Farker, K.; Lehmann, M.H.; Oelschlägel, B.; Haerting, J.; Hoffmann, A.; Janitzky, V.; Schubert, J. Impact of CYP2E1 Genotype in Renal Cell and Urothelial Cancer Patients. Exp. Toxicol. Pathol. 1998, 50, 425–431. [Google Scholar] [CrossRef]
- Kurahashi, N.; Inoue, M.; Iwasaki, M.; Sasazuki, S.; Tsugane, S.; Japan Public Health Center (JPHC) Study Group. Coffee, Green Tea, and Caffeine Consumption and Subsequent Risk of Bladder Cancer in Relation to Smoking Status: A Prospective Study in Japan. Cancer Sci. 2009, 100, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Riboldi, B.P.; Vinhas, Á.M.; Moreira, J.D. Risks of Dietary Acrylamide Exposure: A Systematic Review. Food Chem. 2014, 157, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Food Safety Commission of Japan. Study on Estimate of Acrylamide Intake from Food; Interim Report. Food Safety Commission of Japan. Internet. 2016. Available online: https://www.fsc.go.jp/fsciis/technicalResearch/show/cho99920151507 (accessed on 23 July 2019).


{kind=link}
| Tertile of Energy-Adjusted Acrylamide Intake | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Value c | |||||||||
| Number of participants | 29,606 | 29,606 | 29,606 | |||||||||
| Men, (%) | 50.6 | 44.6 | 45.1 | |||||||||
| Dietary variables | ||||||||||||
| Acrylamide intake | ||||||||||||
| Range, μg/d | 0.0 | - | 4.8 | 4.8 | - | 7.5 | 7.5 | - | 64.6 | |||
| Mean and SD,a μg/d | 3.6 | ± | 1.5 | 6.4 | ± | 2.0 | 11.2 | ± | 4.5 | |||
| Mean and SD, a μg·kg body weight-1·d-1 | 0.07 | ± | 0.06 | 0.12 | ± | 0.12 | 0.21 | ± | 0.24 | |||
| Coffee, a g/d | 44 | ± | 61 | 111 | ± | 117 | 275 | ± | 285 | <0.001 | ||
| Green tea, a g/d | 321 | ± | 340 | 523 | ± | 428 | 753 | ± | 664 | <0.001 | ||
| Alcohol intake, a g/d | 188 | ± | 336 | 156 | ± | 323 | 121 | ± | 279 | <0.001 | ||
| Vegetables, a g/d | 195 | ± | 146 | 236 | ± | 164 | 235 | ± | 175 | <0.001 | ||
| Potato, a g/d | 19 | ± | 19 | 30 | ± | 26 | 33 | ± | 38 | <0.001 | ||
| Fruit, a g/d | 198.0 | ± | 198.3 | 239.6 | ± | 204.1 | 224.8 | ± | 200.8 | <0.001 | ||
| Meat, a g/d | 64.7 | ± | 61.3 | 63.0 | ± | 51.2 | 58.8 | ± | 45.6 | <0.001 | ||
| Fish, a g/d | 94.5 | ± | 76.7 | 97.4 | ± | 68.9 | 86.7 | ± | 62.5 | <0.001 | ||
| Biscuits and cookies, a g/d | 0.8 | ± | 1.4 | 2.2 | ± | 3.1 | 5.2 | ± | 9.0 | <0.001 | ||
| Total energy intake, a kcal/d | 1911 | ± | 639 | 1936 | ± | 613 | 1868 | ± | 607 | <0.001 | ||
| Nondietary Variables | ||||||||||||
| Age at five-year follow-up study, a y | 58 | ± | 8 | 57 | ± | 8 | 56 | ± | 8 | <0.001 | ||
| Body mass index, a b kg/m2 | 24 | ± | 3 | 24 | ± | 3 | 23 | ± | 3 | <0.001 | ||
| Smoking status, % | ||||||||||||
| Never | 62 | 65 | 60 | <0.001 | ||||||||
| Former | 9.4 | 8.5 | 8.0 | |||||||||
| Current | 22 | 21 | 26 | |||||||||
| Missing | 6.5 | 5.8 | 5.9 | |||||||||
| Number of cigarettes/d,a b only for current | 20.4 | ± | 14.7 | 20.8 | ± | 10.4 | 22.7 | ± | 12.2 | <0.001 | ||
| Physical activity (METs)a | 32.7 | ± | 6.5 | 32.9 | ± | 6.4 | 32.6 | ± | 6.4 | <0.001 | ||
| Tertile1 | Tertile2 | Tertile3 | p for Trend | ||||
|---|---|---|---|---|---|---|---|
| HRs | 95% CI | HRs | 95% CI | ||||
| Number of participant | 29,606 | 29,606 | 29,606 | ||||
| Cases (n = 208), n | 81 | 66 | 61 | ||||
| Person-years (n = 1,346,982), n | 447,582 | 451,430 | 447,970 | ||||
| Model 1 adjusted HRs (95% CI) | Reference | 0.90 | (0.65–1.25) | 0.89 | (0.63–1.24) | 0.471 | |
| Model 2 adjusted HRs (95% CI) | Reference | 0.83 | (0.45–1.53) | 0.71 | (0.38–1.34) | 0.294 | |
| Model 3 adjusted HRs (95% CI) | Reference | 0.82 | (0.43–1.59) | 0.67 | (0.34–1.32) | 0.25 | |
| Current or past smoker | |||||||
| Cases (n = 88), n | 29 | 30 | 29 | ||||
| Person-years (n = 407,260), n | 135,171 | 126,646 | 145,443 | ||||
| Model 1 adjusted HRs (95% CI) | Reference | 1.16 | (0.69–1.93) | 1.00 | (0.59–1.69) | 0.990 | |
| Model 2 adjusted HRs (95% CI) | Reference | 0.81 | (0.42–1.59) | 0.85 | (0.44–1.65) | 0.990 | |
| Model 3 adjusted HRs (95% CI) | Reference | 0.83 | (0.41–1.68) | 0.79 | (0.39–1.60) | 0.513 | |
| Never smoker | |||||||
| Cases (n = 110), n | 46 | 33 | 31 | ||||
| Person-years (n = 866,655), n | 286,730 | 301,249 | 278,676 | ||||
| Model 1 adjusted HRs (95% CI) | Reference | 0.78 | (0.50–1.23) | 0.90 | (0.56–1.44) | 0.592 | |
| Model 2 adjusted HRs (95% CI) | Reference | 0.81 | (0.51–1.27) | 0.93 | (0.58–1.50) | 0.711 | |
| Model 3 adjusted HRs (95% CI) | Reference | 0.77 | (0.47–1.25) | 0.96 | (0.58–1.58) | 0.784 | |
| Tertile1 | Tertile2 | Tertile3 | p for Trend | |||
|---|---|---|---|---|---|---|
| HRs | 95% CI | HRs | 95% CI | |||
| Number of participant | 13,845 | 13,845 | 13,844 | |||
| Cases (n = 1195), n | 405 | 418 | 372 | |||
| Person-years (n = 605,324), n | 200,942 | 202,858 | 201,524 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 1.02 | (0.89–1.17) | 0.98 | (0.85–1.13) | 0.748 |
| Model 2 adjusted HRs (95% CI) | Reference | 0.92 | (0.73–1.17) | 0.96 | (0.75–1.22) | 0.726 |
| Model 3 adjusted HRs (95% CI) | Reference | 0.93 | (0.73–1.18) | 0.93 | (0.72–1.18) | 0.540 |
| Current or past smoker | ||||||
| Cases (n = 650), n | 230 | 202 | 218 | |||
| Person-years (n = 366,518), n | 115,073 | 120,044 | 131,401 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 0.87 | (0.72–1.06) | 0.92 | (0.76–1.11) | 0.393 |
| Model 2 adjusted HRs (95% CI) | Reference | 0.91 | (0.71–1.16) | 0.94 | (0.74–1.21) | 0.393 |
| Model 3 adjusted HRs (95% CI) | Reference | 0.92 | (0.72–1.18) | 0.92 | (0.71–1.19) | 0.529 |
| Never smoker | ||||||
| Cases (n = 478), n | 159 | 187 | 132 | |||
| Person-years (n = 209,501), n | 75,381 | 73,550 | 60,570 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 1.14 | (0.93–1.42) | 1.02 | (0.81–1.29) | 0.791 |
| Model 2 adjusted HRs (95% CI) | Reference | 1.15 | (0.93–1.43) | 1.04 | (0.81–1.32) | 0.722 |
| Model 3 adjusted HRs (95% CI) | Reference | 1.17 | (0.94–1.46) | 1.01 | (0.79–1.30) | 0.859 |
| Tertile1 | Tertile2 | Tertile3 | p for Trend | |||
|---|---|---|---|---|---|---|
| HRs | 95% CI | HRs | 95% CI | |||
| Number of participant | 29,606 | 29,606 | 29,606 | |||
| Cases (n = 392), n | 132 | 127 | 133 | |||
| Person-years (n = 1,346,982), n | 447,582 | 451,430 | 447,970 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 1.04 | (0.82–1.33) | 1.18 | (0.92–1.51) | 0.191 |
| Model 2 adjusted HRs (95% CI) | Reference | 0.89 | (0.62–1.32) | 0.87 | (0.59–1.29) | 0.491 |
| Model 3 adjusted HRs (95% CI) | Reference | 0.82 | (0.54–1.25) | 0.88 | (0.58–1.34) | 0.56 |
| Current or past smoker | ||||||
| Cases (n = 224), n | 80 | 68 | 76 | |||
| Person-years (n = 407,260), n | 135,171 | 126,646 | 145,443 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 0.98 | (0.71–1.36) | 1.05 | (0.76–1.45) | 0.764 |
| Model 2 adjusted HRs (95% CI) | Reference | 0.88 | (0.60–1.31) | 0.87 | (0.58–1.30) | 0.764 |
| Model 3 adjusted HRs (95% CI) | Reference | 0.81 | (0.53–1.24) | 0.88 | (0.58–1.34) | 0.557 |
| Never smoker | ||||||
| Cases (n = 140), n | 42 | 50 | 48 | |||
| Person-years (n = 866,655), n | 286,730 | 301,249 | 278,676 | |||
| Model 1 adjusted HRs (95% CI) | Reference | 1.17 | (0.77–1.77) | 1.36 | (0.89–2.08) | 0.155 |
| Model 2 adjusted HRs (95% CI) | Reference | 1.23 | (0.81–1.87) | 1.44 | (0.93–2.21) | 0.099 |
| Model 3 adjusted HRs (95% CI) | Reference | 1.20 | (0.76–1.87) | 1.43 | (0.90–2.27) | 0.128 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, S.; Sobue, T.; Kitamura, T.; Ishihara, J.; Kotemori, A.; Zha, L.; Liu, R.; Sawada, N.; Iwasaki, M.; Tsugane, S.; et al. Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study. Nutrients 2021, 13, 780. https://doi.org/10.3390/nu13030780
Ikeda S, Sobue T, Kitamura T, Ishihara J, Kotemori A, Zha L, Liu R, Sawada N, Iwasaki M, Tsugane S, et al. Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study. Nutrients. 2021; 13(3):780. https://doi.org/10.3390/nu13030780
Chicago/Turabian StyleIkeda, Sayaka, Tomotaka Sobue, Tetsuhisa Kitamura, Junko Ishihara, Ayaka Kotemori, Ling Zha, Rong Liu, Norie Sawada, Motoki Iwasaki, Shoichiro Tsugane, and et al. 2021. "Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study" Nutrients 13, no. 3: 780. https://doi.org/10.3390/nu13030780
APA StyleIkeda, S., Sobue, T., Kitamura, T., Ishihara, J., Kotemori, A., Zha, L., Liu, R., Sawada, N., Iwasaki, M., Tsugane, S., & on behalf of the JPHC Study Group. (2021). Dietary Acrylamide Intake and the Risks of Renal Cell, Prostate, and Bladder Cancers: A Japan Public Health Center-Based Prospective Study. Nutrients, 13(3), 780. https://doi.org/10.3390/nu13030780