
Assessment of Dietary Habits Using the Diet Quality Index—International in Cerebrovascular and Cardiovascular Disease Patients

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurements
2.3. Evaluation of Dietary Habits
2.4. Statistical Analysis
3. Results
3.1. Study Population Characteristics
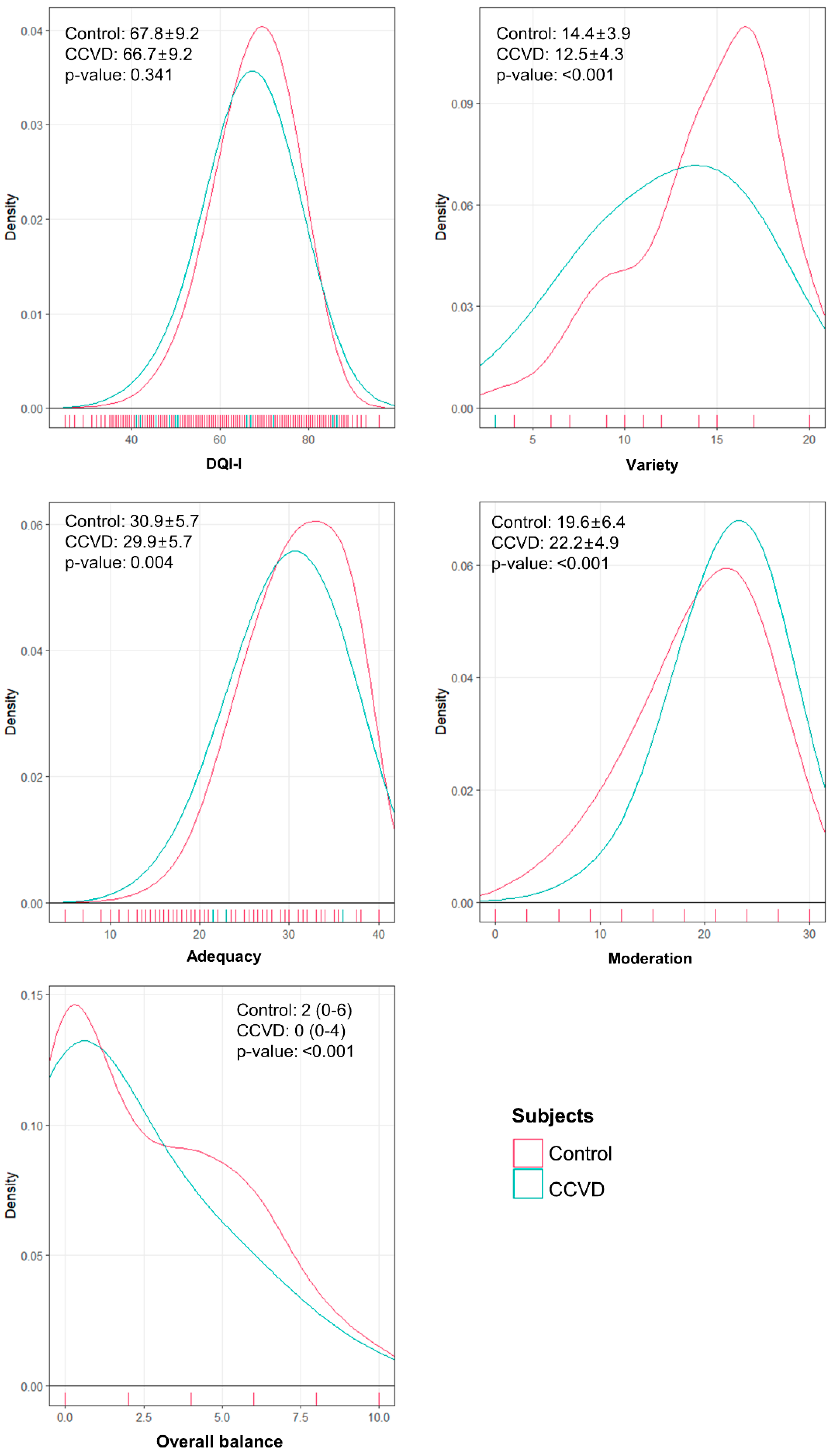
3.2. Univariate Analysis of Diet Quality Using the DQI-I
3.3. Adjusted Analysis of DQI-I Scores
3.4. Adjusted Analysis of DQI-I Components
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CCVD | Cerebrovascular and cardiovascular disease |
| DQI-I | Diet Quality Index—International |
| KNHANES | Korean National Health and Nutrition Examination Survey |
| IRB | Institutional Review Board |
| BMI | Body mass index |
| FFQ | Food frequency questionnaire |
| 24HR | 24-h dietary recall |
| IQR | Interquartile range |
References
- Korean Statistical Information Service. Annual Report on the Cause of Death Statistics. Available online: http://kosis.kr (accessed on 1 July 2019).
- World Health Organization. Preventing chronic diseases: A vital investment. In WHO Global Report; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Kerr, A.J.; Broad, J.; Wells, S.; Riddell, T.; Jackson, R. Should the first priority in cardiovascular risk management be those with prior cardiovascular disease? Heart 2009, 95, 125–129. [Google Scholar] [CrossRef]
- Feng, W.; Hendry, R.M.; Adams, R.J. Risk of recurrent stroke, myocardial infarction, or death in hospitalized stroke patients. Neurology 2010, 74, 588–593. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Smith, S.C., Jr.; Stone, N.J.; Grundy, S.M. Secondary Prevention for Atherosclerotic Cardiovascular Disease: Comparing Recent US and European Guidelines on Dyslipidemia. Circulation 2020, 141, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; et al.; Authors/Task Force Members 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. J. Prev. Cardiol. 2016, 23, NP1–NP96. [Google Scholar] [CrossRef]
- Eilat-Adar, S.; Sinai, T.; Yosefy, C.; Henkin, Y. Nutritional recommendations for cardiovascular disease prevention. Nutrients 2013, 5, 3646–3683. [Google Scholar] [CrossRef]
- Hu, F.B.; Willett, W.C. Optimal diets for prevention of coronary heart disease. JAMA 2002, 288, 2569–2578. [Google Scholar] [CrossRef]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Brown, S.E.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; et al. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef]
- Van Horn, L.; McCoin, M.; Kris-Etherton, P.M.; Burke, F.; Carson, J.A.; Champagne, C.M.; Karmally, W.; Sikand, G. The evidence for dietary prevention and treatment of cardiovascular disease. J. Am. Diet. Assoc. 2008, 108, 287–331. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.; McDaniel, M.C.; Ashen, M.D.; Miller, J.I.; Sorrentino, M.; Chan, V.; Blumenthal, R.S.; Sperling, L.S. Diets and cardiovascular disease: An evidence-based assessment. J. Am. Coll. Cardiol. 2005, 45, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.G.; Wadden, T.A. The evolution of very-low-calorie diets: An update and meta-analysis. Obesity (Silver Spring) 2006, 14, 1283–1293. [Google Scholar] [CrossRef]
- Katcher, H.I.; Hill, A.M.; Lanford, J.L.; Yoo, J.S.; Kris-Etherton, P.M. Lifestyle approaches and dietary strategies to lower LDL-cholesterol and triglycerides and raise HDL-cholesterol. Endocrinol. Metab. Clin. N. Am. 2009, 38, 45–78. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Katan, M.B.; Ascherio, A.; Stampfer, M.J.; Willett, W.C. Trans fatty acids and cardiovascular disease. N. Engl. J. Med. 2006, 354, 1601–1613. [Google Scholar] [CrossRef]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef]
- Iestra, J.A.; Kromhout, D.; van der Schouw, Y.T.; Grobbee, D.E.; Boshuizen, H.C.; van Staveren, W.A. Effect size estimates of lifestyle and dietary changes on all-cause mortality in coronary artery disease patients: A systematic review. Circulation 2005, 112, 924–934. [Google Scholar] [CrossRef]
- Chow, C.K.; Jolly, S.; Rao-Melacini, P.; Fox, K.A.; Anand, S.S.; Yusuf, S. Association of diet, exercise, and smoking modification with risk of early cardiovascular events after acute coronary syndromes. Circulation 2010, 121, 750–758. [Google Scholar] [CrossRef]
- Kim, S.; Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The Diet Quality Index-International (DQI-I) provides an effective tool for cross-national comparison of diet quality as illustrated by China and the United States. J. Nutr. 2003, 133, 3476–3484. [Google Scholar] [CrossRef]
- Lee, Y.; Koo, H.Y.; Cho, I.Y.; Jo, M.; Kim, K.C.; Eum, Y.H.; Kim, J.Y.; Lee, K.; Lee, K.H.; Jung, S.Y.; et al. Dietary Patterns Assessed by the Diet Quality Index-International Among Cancer Survivors Compared with Healthy Control Subjects: Using the Korea National Health and Nutrition Examination Surveys 2013–2015. KJFP 2019, 9, 204–211. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Wen, C.P.; David Cheng, T.Y.; Tsai, S.P.; Chan, H.T.; Hsu, H.L.; Hsu, C.C.; Eriksen, M.P. Are Asians at greater mortality risks for being overweight than Caucasians? Redefining obesity for Asians. Public Health Nutr. 2009, 12, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Kweon, S.; Kim, Y.; Jang, M.-j.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data Resource Profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.W.; Song, S.; Lee, J.E.; Oh, K.; Shim, J.; Kweon, S.; Paik, H.Y.; Joung, H. Reproducibility and validity of an FFQ developed for the Korea National Health and Nutrition Examination Survey (KNHANES). Public Health Nutr. 2015, 18, 1369–1377. [Google Scholar] [CrossRef] [PubMed]
- The Korean Nutrition Society. Dietary Reference Intakes for Koreans. Available online: http://www.kns.or.kr/FileRoom/FileRoom_view.asp?idx=79&BoardID=Kdr (accessed on 20 June 2019).
- Ministry of Health and Welfare. Chronic Disease Status and Issues. Available online: http://www.cdc.go.kr/contents.es?mid=a20303020300 (accessed on 20 June 2019).
- World Health Organization. Prevention of Cardiovascular Disease: Guidelines for Assessment and Management of Total Cardiovascular Risk; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Drewnowski, A. Concept of a nutritious food: Toward a nutrient density score. Am. J. Clin. Nutr. 2005, 82, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.; Joung, H.; Lim, J.H.; Lee, Y.-S.; Song, Y.J. Secular Trend in Dietary Patterns in a Korean Adult Population, Using the 1998, 2001, and 2005 Korean National Health and Nutrition Examination Survey. Korean J. Nutr. 2011, 44, 152–161. [Google Scholar] [CrossRef]
- Kim, S.H.; Oh, S.Y. Cultural and nutritional aspects of traditional Korean diet. World Rev. Nutr. Diet. 1996, 79, 109–132. [Google Scholar] [CrossRef]
- Lee, M.J.; Popkin, B.M.; Kim, S. The unique aspects of the nutrition transition in South Korea: The retention of healthful elements in their traditional diet. Public Health Nutr 2002, 5, 197–203. [Google Scholar] [CrossRef]
- Anderson, K.M.; Odell, P.M.; Wilson, P.W.F.; Kannel, W.B. Cardiovascular disease risk profiles. Am. Heart J. 1991, 121, 293–298. [Google Scholar] [CrossRef]
- Korean Academy of Medical Sciences. Evidence-Based Guideline for Hypertension in Primary Care. Available online: https://www.cdc.go.kr/board/board.es?mid=a20503050000&bid=0021&tag=&act=view&list_no=127643 (accessed on 29 July 2019).
- Korean Academy of Medical Sciences. Evidence-Based Guideline for Type 2 Diabetes in Primary Care. Available online: https://www.cdc.go.kr/board/board.es?mid=a20503050000&bid=0021 (accessed on 29 July 2019).
- Rhee, E.J.; Kim, H.C.; Kim, J.H.; Lee, E.Y.; Kim, B.J.; Kim, E.M.; Song, Y.; Lim, J.H.; Kim, H.J.; Choi, S.; et al. 2018 Guidelines for the management of dyslipidemia. Korean J. Intern. Med. 2019, 34, 723–771. [Google Scholar] [CrossRef]
- Seo, M.H.; Lee, W.Y.; Kim, S.S.; Kang, J.H.; Kang, J.H.; Kim, K.K.; Kim, B.Y.; Kim, Y.H.; Kim, W.J.; Kim, E.M.; et al. 2018 Korean Society for the Study of Obesity Guideline for the Management of Obesity in Korea. J. Obes. Metab. Syndr. 2019, 28, 40–45. [Google Scholar] [CrossRef]
- Schatzkin, A.; Kipnis, V.; Carroll, R.J.; Midthune, D.; Subar, A.F.; Bingham, S.; Schoeller, D.A.; Troiano, R.P.; Freedman, L.S. A comparison of a food frequency questionnaire with a 24-hour recall for use in an epidemiological cohort study: Results from the biomarker-based Observing Protein and Energy Nutrition (OPEN) study. Int. J. Epidemiol. 2003, 32, 1054–1062. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total (n = 12,683) | CCVD (n = 718) | Non-CCVD (n = 11,965) | p-Value 1 | |
|---|---|---|---|---|
| Age (y) | 53.3 ± 16.5 | 68.8 ± 8.9 | 52.3 ± 16.4 | <0.001 |
| 19–29 | 1172 (9.2) | 1 (0.1) | 1171 (9.8) | <0.001 |
| 30–39 | 1862 (14.7) | 2 (0.3) | 1860 (15.6) | |
| 40–49 | 2196 (17.3) | 17 (2.4) | 2179 (18.2) | |
| 50–64 | 3618 (28.5) | 181 (25.2) | 3437 (28.7) | |
| ≥65 | 3835 (30.2) | 517 (72.0) | 3318 (27.7) | |
| Sex | ||||
| Male | 5325 (42.0) | 388 (54.0) | 4937 (41.2) | <0.001 |
| Female | 7358 (58.0) | 330 (46.0) | 7028 (58.7) | |
| BMI (kg/m2) | 23.8 ± 3.5 | 24.6 ± 3.4 | 23.7 ± 3.5 | <0.001 |
| Underweight (<18) | 545 (4.3) | 20 (2.8) | 525 (4.4) | <0.001 |
| Normal weight (18–22.9) | 4979 (39.3) | 210 (29.3) | 4769 (39.9) | |
| Overweight (23–24.9) | 3005 (23.7) | 180 (25.1) | 2825 (23.6) | |
| Obese (≥25) | 4154 (32.8) | 308 (43.0) | 3846 (32.1) | |
| Spouse | ||||
| With spouse | 9171 (72.3) | 506 (70.5) | 8665 (72.4) | <0.001 |
| Without spouse | 1947 (15.4) | 202 (28.1) | 1745 (14.6) | |
| Unmarried | 1565 (12.3) | 10 (1.4) | 1555 (13.0) | |
| Education | ||||
| ≥College | 3749 (29.6) | 56 (7.8) | 3693 (30.9) | <0.001 |
| Middle/high school | 5521 (43.5) | 265 (36.9) | 5256 (44.0) | |
| ≤Elementary school | 3413 (26.9) | 397 (55.3) | 3016 (25.2) | |
| Monthly income | ||||
| >3000 | 5853 (46.2) | 162 (22.6) | 5691 (47.6) | <0.001 |
| 1000–3000 | 4237 (33.4) | 242 (33.7) | 3995 (33.4) | |
| <1000 | 2593 (20.4) | 314 (43.7) | 2279 (19.1) | |
| Residential area | ||||
| Urban | 10,057 (79.3) | 524 (73.0) | 9533 (79.7) | 0.002 |
| Rural | 2626 (20.7) | 194 (27.0) | 2432 (20.3) | |
| Smoking | ||||
| Current smoker | 2139 (16.9) | 113 (15.7) | 2026 (16.9) | 0.01 |
| Ex-smoker | 2685 (21.2) | 250 (34.8) | 2435 (20.4) | |
| Never smoker | 7859 (62.0) | 355 (49.4) | 7504 (62.7) | |
| Alcohol | ||||
| Current drinker | 8603 (67.8) | 382 (53.2) | 8221 (68.7) | <0.001 |
| Ex-drinker | 8890 (18.1) | 193 (26.9) | 2097 (17.5) | |
| Never drinker | 1790 (14.1) | 143 (19.9) | 1647 (13.8) | |
| Chronic disease | ||||
| 0 | 7508 (59.2) | 125 (17.4) | 7383 (61.7) | <0.001 |
| 1 | 2732 (21.5) | 221 (30.8) | 2511 (21.0) | |
| 2 | 1624 (12.8) | 200 (27.9) | 1424 (11.9) | |
| ≥3 | 819 (6.5) | 172 (24.0) | 647 (5.4) |
| Model | Regression Coefficient | 95% CI | p-Value |
|---|---|---|---|
| Model 1 | −0.43 | −1.32 ~ 0.46 | 0.341 |
| Model 2 | −1.96 | −2.89 ~ −1.02 | <0.001 |
| Model 3 | −1.13 | −2.00 ~ −0.26 | 0.011 |
| DQI-I Components | Regression Coefficient | 95% CI | p-Value |
|---|---|---|---|
| Variety | −0.54 | −0.90 ~ −0.17 | 0.004 |
| Overall food group variety | −0.38 | −0.63 ~ −0.13 | 0.003 |
| Within-group variety | −0.16 | −0.29 ~ −0.17 | 0.028 |
| Adequacy | −0.86 | −1.38 ~ −0.34 | 0.001 |
| Vegetable | −0.04 | −0.10 ~ 0.02 | 0.206 |
| Fruit | −0.12 | −0.31 ~ 0.07 | 0.201 |
| Grain | −0.01 | −0.06 ~ 0.04 | 0.769 |
| Fiber | −0.22 | −0.34 ~ −0.97 | <0.001 |
| Protein | −0.03 | −0.10 ~ 0.04 | 0.433 |
| Iron | −0.14 | −0.22 ~ −0.06 | 0.001 |
| Calcium | −0.10 | −0.22 ~ 0.03 | 0.124 |
| Vitamin C | −0.21 | −0.37 ~ −0.05 | 0.012 |
| Moderation | 0.32 | −0.12 ~ 0.76 | 0.159 |
| Total fat | 0.04 | −0.08 ~ 0.17 | 0.509 |
| Saturated fat | −0.02 | −0.14 ~ 0.09 | 0.697 |
| Cholesterol | 0.24 | 0.08 ~ 0.40 | 0.004 |
| Sodium | 0.19 | −0.04 ~ 0.42 | 0.100 |
| Empty calorie foods | −0.13 | −0.34 ~ 0.09 | 0.238 |
| Overall balance | −0.05 | −0.31 ~ 0.21 | 0.704 |
| Macronutrient ratio | −0.02 | −0.23 ~ 0.18 | 0.824 |
| Fatty acid ratio | −0.03 | −0.18 ~ 0.12 | 0.721 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, I.Y.; Lee, K.M.; Lee, Y.; Paek, C.M.; Kim, H.J.; Kim, J.Y.; Lee, K.; Han, J.S.; Bae, W.K. Assessment of Dietary Habits Using the Diet Quality Index—International in Cerebrovascular and Cardiovascular Disease Patients. Nutrients 2021, 13, 542. https://doi.org/10.3390/nu13020542
Cho IY, Lee KM, Lee Y, Paek CM, Kim HJ, Kim JY, Lee K, Han JS, Bae WK. Assessment of Dietary Habits Using the Diet Quality Index—International in Cerebrovascular and Cardiovascular Disease Patients. Nutrients. 2021; 13(2):542. https://doi.org/10.3390/nu13020542
Chicago/Turabian StyleCho, In Young, Kyung Min Lee, Yoojin Lee, Chuel Min Paek, Ha Jin Kim, Ju Young Kim, Kiheon Lee, Jong Soo Han, and Woo Kyung Bae. 2021. "Assessment of Dietary Habits Using the Diet Quality Index—International in Cerebrovascular and Cardiovascular Disease Patients" Nutrients 13, no. 2: 542. https://doi.org/10.3390/nu13020542
APA StyleCho, I. Y., Lee, K. M., Lee, Y., Paek, C. M., Kim, H. J., Kim, J. Y., Lee, K., Han, J. S., & Bae, W. K. (2021). Assessment of Dietary Habits Using the Diet Quality Index—International in Cerebrovascular and Cardiovascular Disease Patients. Nutrients, 13(2), 542. https://doi.org/10.3390/nu13020542