
Effects of High Salt Intake on Detrusor Muscle Contraction in Dahl Salt-Sensitive Rats


Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Experimental Protocol
2.3. Isometric Tension Study
2.4. Real-Time Polymerase Chain Reaction
2.5. Statistical Analysis
3. Results
3.1. Heart Rate and Blood Pressure in Normal Salt Groups
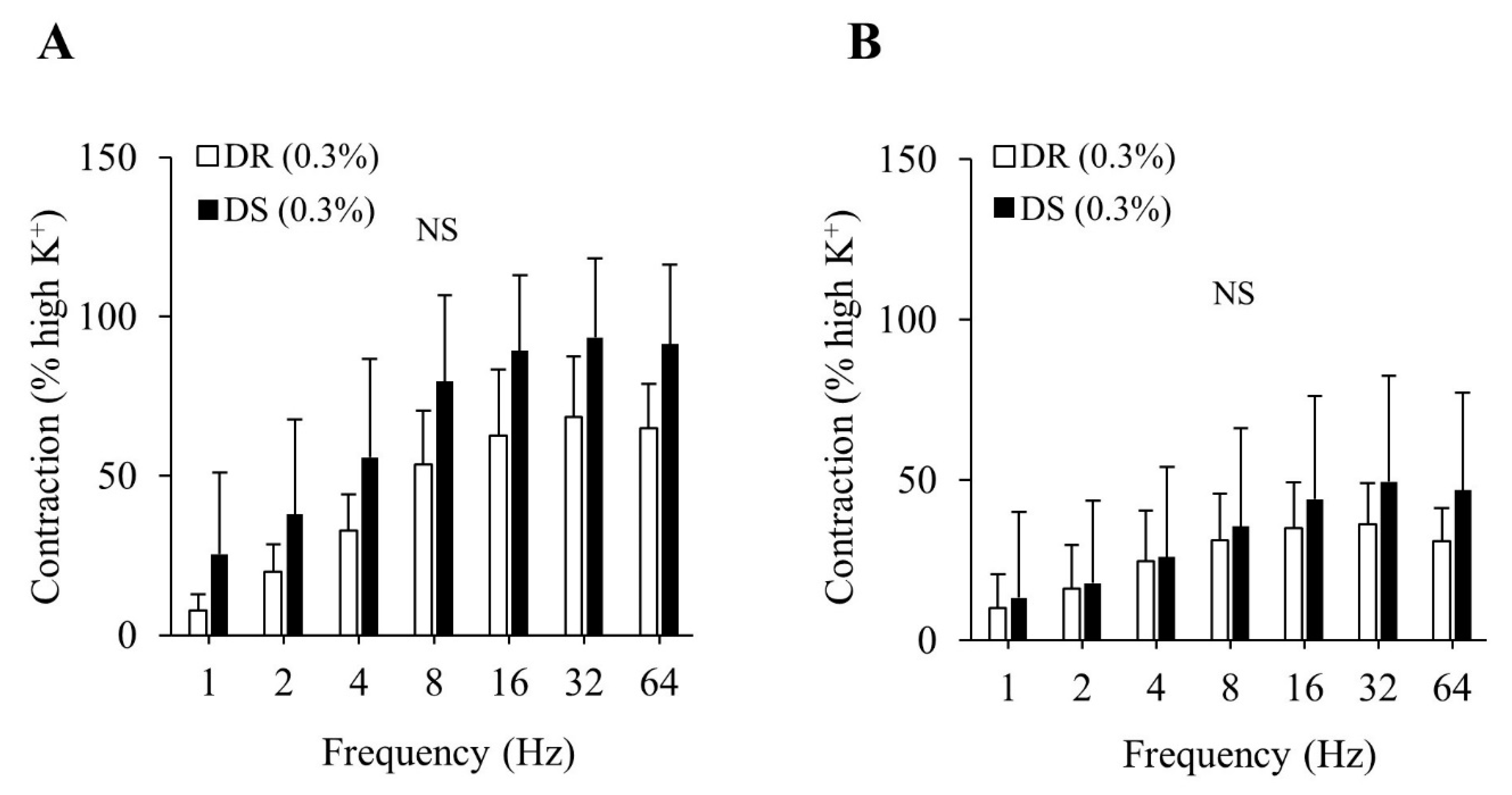
3.2. Isometric Tension Study of the Detrusor Muscle in Normal Salt Groups
3.3. Heart Rate and Blood Pressure in High Salt Groups
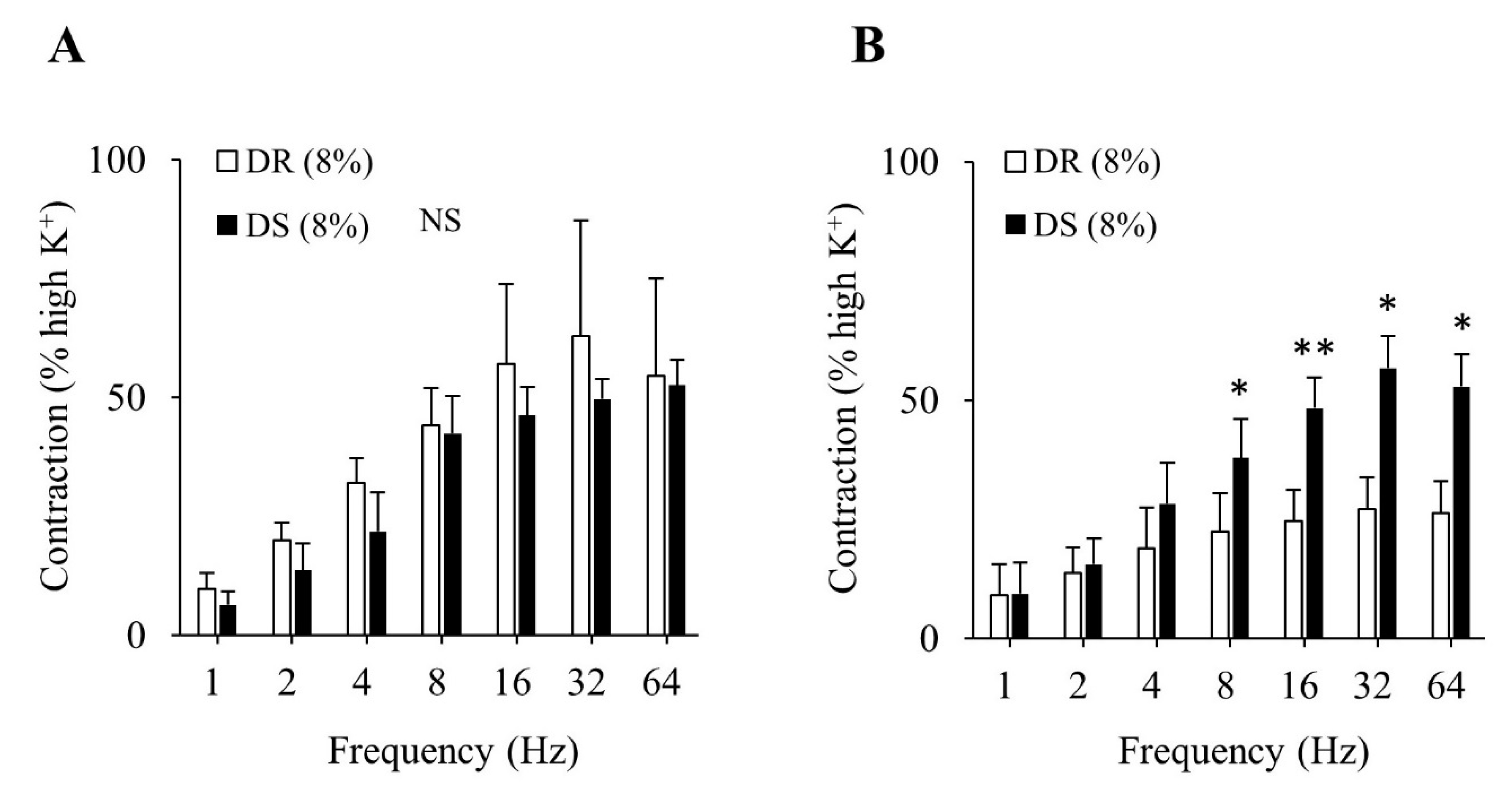
3.4. Isometric Tension Study of the Detrusor Muscle in High Salt Groups
3.5. Real-Time PCR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Abdelmoteleb, H.; Jefferies, E.R.; Drake, M.J. Assessment and management of male lower urinary tract symptoms (LUTS). Int. J. Surg. 2016, 25, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; van Kerrebroeck, P.; Victor, A.; Wein, A. Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the Standardisation Sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Yamaguchi, O.; Hayashi, K. Neurogenic Bladder Society Committee. Epidemiologic survey of lower urinary tract symptoms in Japan. Urology 2006, 68, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Gotoh, M.; Kawauchi, A.; Kojima, Y.; Masumori, N.; Nagai, A.; Saitoh, T.; Sakai, H.; Takahashi, S.; Ukimura, O.; et al. Clinical guidelines for male lower urinary tract symptoms and benign prostatic hyperplasia. Int. J. Urol. 2017, 24, 716–729. [Google Scholar] [CrossRef]
- Yamaguchi, O.; Nishizawa, O.; Takeda, M.; Yokoyama, O.; Homma, Y.; Kakizaki, H.; Obara, K.; Gotoh, M.; Igawa, Y.; Seki, N.; et al. Neurogenic Bladder Society. Clinical guidelines for overactive bladder. Int. J. Urol. 2009, 16, 126–142. [Google Scholar] [CrossRef] [PubMed]
- Sexton, C.C.; Notte, S.M.; Maroulis, C.; Dmochowski, R.R.; Cardozo, L.; Subramanian, D.; Coyne, K.S. Persistence and adherence in the treatment of overactive bladder syndrome with anticholinergic therapy: A systematic review of the literature. Int. J. Clin. Pract. 2011, 65, 567–585. [Google Scholar] [CrossRef]
- Benner, J.S.; Nichol, M.B.; Rovner, E.S.; Jumadilova, Z.; Alvir, J.; Hussein, M.; Fanning, K.; Trocio, J.N.; Brubaker, L. Patient-reported reasons for discontinuing overactive bladder medication. BJU Int. 2010, 105, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, K.; Terada, N.; Matsui, Y.; Terai, A.; Kinukawa, N.; Arai, Y. Prevalence of and risk factors for nocturia: Analysis of a health screening program. Int. J. Urol. 2004, 11, 282–287. [Google Scholar] [CrossRef]
- Ito, H.; Yoshiyasu, T.; Yamaguchi, O.; Yokoyama, O. Male lower urinary tract symptoms: Hypertension as a risk factor for storage symptoms, but not voiding symptoms. Low. Urin. Tract Symptoms 2012, 4, 68–72. [Google Scholar] [CrossRef]
- Sugaya, K.; Kadekawa, K.; Ikehara, A.; Nakayama, T.; Gakiya, M.; Nashiro, F.; Goya, M.; Hatano, T.; Ogawa, Y. Influence of hypertension on lower urinary tract symptoms in benign prostatic hyperplasia. Int. J. Urol. 2003, 10, 569–575. [Google Scholar] [CrossRef]
- Matsuo, T.; Miyata, Y.; Sakai, H. Daily salt intake is an independent risk factor for pollakiuria and nocturia. Int. J. Urol. 2017, 24, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Hotta, Y.; Maeda, K.; Kataoka, T.; Maeda, Y.; Hamakawa, T.; Shibata, Y.; Sasaki, S.; Ugawa, S.; Yasui, T.; et al. High salt loading induces urinary storage dysfunction via upregulation of epithelial sodium channel alpha in the bladder epithelium in Dahl salt-sensitive rats. J. Pharmacol. Sci. 2017, 135, 121–125. [Google Scholar] [CrossRef]
- Kurokawa, T.; Zha, X.; Ito, H.; Aoki, Y.; Akino, H.; Kobayashi, M.; Yokoyama, O. Underlying mechanisms of urine storage dysfunction in rats with salt loading hypertension. Life Sci. 2015, 141, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Rapp, J.P. Dahl salt-susceptible and salt-resistant rats. A review. Hypertension 1982, 4, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, N.; de Groat, W.C. Neural control of the lower urinary tract. Int. J. Urol. 1997, 4, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Burnstock, G. Purinergic signalling in the urinary tract in health and disease. Purinergic. Signal 2014, 10, 103–155. [Google Scholar] [CrossRef]
- Yoshida, M.; Masunaga, K.; Nagata, T.; Yono, M.; Homma, Y. The forefront for novel therapeutic agents based on the pathophysiology of lower urinary tract dysfunction: Pathophysiology and pharmacotherapy of overactive bladder. J. Pharmacol. Sci. 2010, 112, 128–134. [Google Scholar] [CrossRef]
- Mumtaz, F.H.; Lau, D.H.; Siddiqui, E.J.; Morgan, R.J.; Thompson, C.S.; Mikhailidis, D.P. Changes in cholinergic and purinergic neurotransmission in the diabetic rabbit bladder. In Vivo 2006, 20, 1–4. [Google Scholar]
- de Jongh, R.; Van Koeveringe, G.A.; van Kerrebroeck, P.E.; Markerink-van Ittersum, M.; de Vente, J.; Gillespie, J.I. Damage to the bladder neck alters autonomous activity and its sensitivity to cholinergic agonists. BJU Int. 2007, 100, 919–929. [Google Scholar] [CrossRef]
- Clemow, D.B.; Steers, W.D.; McCarty, R.; Tuttle, J.B. Altered regulation of bladder nerve growth factor and neutrally mediated hyperactive voiding. Am. J. Physiol. 1998, 275, 1279–1286. [Google Scholar]
- Steers, W.D.; Ciambotti, J.; Erdman, S.; de Groat, W.C. Morphological plasticity in efferent pathways to the urinary bladder of the rat following urethral obstruction. J. Neurosci. 1990, 10, 1943–1951. [Google Scholar] [CrossRef]
- Seth, J.H.; Sahai, A.; Khan, M.S.; van der Aa, F.; de Ridder, D.; Panicker, J.N.; Dasgupta, P.; Fowler, C.J. Nerve growth factor (NGF): A potential urinary biomarker for overactive bladder syndrome (OAB)? BJU Int. 2013, 111, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.T.; Edwards, D.G.; Farquhar, W.B. The Influence of Dietary Salt beyond Blood Pressure. Curr. Hypertens. Rep. 2019, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- Frisoli, T.M.; Schmieder, R.E.; Grodzicki, T.; Messerli, F.H. Salt and hypertension: Is salt dietary reduction worth the effort? Am. J. Med. 2012, 125, 433–439. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Sequence (5′–3′) | |
|---|---|---|
| M1 | F | GCACAGGCACCCACCAAGCAG |
| R | AGAGCAGCAGCAGGCGGAACG | |
| M2 | F | TTTGGGACCTGTAGTATGTGACC |
| R | GCTTAACTGGGTAGGTCAGAGGT | |
| M3 | F | TATCCAGCACAGAGAATCCAGAC |
| R | GCGCTAACAGTGCAGGAGACAGT | |
| Rock1 | F | CTGGACATTTGAAGTTAGCCG |
| R | CCACTGCTGTATCACATCGTACC | |
| Rock2 | F | GAACCTACTCCTCGAAGCCG |
| R | TGCTTCAGCAGCTCATTCAGTTT | |
| Ngf | F | CATGGTACAATCTCCTTCAAC |
| R | CCAACCCACACACTGACACTG | |
| β-actin | F | TGTGTGGATTGGTGGCTCTATC |
| R | CATCGTACTCCTGCTTGCTGATC |
| Initial | Final | |||||
|---|---|---|---|---|---|---|
| DR (0.3%) | DS (0.3%) | p-Value | DR (0.3%) | DS (0.3%) | p-Value | |
| Heart rate (beats per min) | 416.7 ± 20.8 | 434.6 ± 29.8 | NS | 399.1 ± 25.2 | 392.8 ± 28.7 | NS |
| Systolic blood pressure (mmHg) | 101.9 ± 7.3 | 114.0 ± 9.3 | NS | 112.6 ± 5.2 | 114.8 ± 4.2 | NS |
| Diastolic blood pressure (mmHg) | 69.1 ± 12.0 | 86.8 ± 5.6 | NS | 81.6 ± 12.4 | 85.1 ± 5.4 | NS |
| DR (0.3%) | DS (0.3%) | p-Value | |
|---|---|---|---|
| log EC50 (mol/L) | −6.10 ± 0.31 | −6.23 ± 0.29 | NS |
| Emax (% high K+) | 85.7 ± 27.9 | 98.3 ± 22.6 | NS |
| Initial | Final | |||||
|---|---|---|---|---|---|---|
| DR (8%) | DS (8%) | p-Value | DR (8%) | DS (8%) | p-Value | |
| Heart rate (beats per min) | 415.2 ± 4.9 | 429.1 ± 18.6 | NS | 435.0 ± 19.5 | 410.5 ± 30.7 | NS |
| Systolic blood pressure (mmHg) | 102.6 ± 4.5 | 117.7 ± 13.2 | NS | 116.3 ± 4.2 | 142.4 ± 8.5 | ** |
| Diastolic blood pressure (mmHg) | 78.3 ± 6.6 | 86.1 ± 12.1 | NS | 87.7 ± 7.4 | 100.5 ± 5.5 | ** |
| DR (8%) | DS (8%) | p-Value | |
|---|---|---|---|
| log EC50 (mol/L) | −6.04 ± 0.05 | −6.43 ± 0.12 | * |
| Emax (% high K+) | 99.6 ± 20.4 | 112.4 ± 9.9 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawata, R.; Hotta, Y.; Maeda, K.; Kataoka, T.; Kimura, K. Effects of High Salt Intake on Detrusor Muscle Contraction in Dahl Salt-Sensitive Rats. Nutrients 2021, 13, 539. https://doi.org/10.3390/nu13020539
Kawata R, Hotta Y, Maeda K, Kataoka T, Kimura K. Effects of High Salt Intake on Detrusor Muscle Contraction in Dahl Salt-Sensitive Rats. Nutrients. 2021; 13(2):539. https://doi.org/10.3390/nu13020539
Chicago/Turabian StyleKawata, Ryoya, Yuji Hotta, Kotomi Maeda, Tomoya Kataoka, and Kazunori Kimura. 2021. "Effects of High Salt Intake on Detrusor Muscle Contraction in Dahl Salt-Sensitive Rats" Nutrients 13, no. 2: 539. https://doi.org/10.3390/nu13020539
APA StyleKawata, R., Hotta, Y., Maeda, K., Kataoka, T., & Kimura, K. (2021). Effects of High Salt Intake on Detrusor Muscle Contraction in Dahl Salt-Sensitive Rats. Nutrients, 13(2), 539. https://doi.org/10.3390/nu13020539