
Prevalence of Wheat/Gluten-Related Disorders and Gluten-Free Diet in Paraguay: An Online Survey-Based Study

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Questionnaire and Population Survey
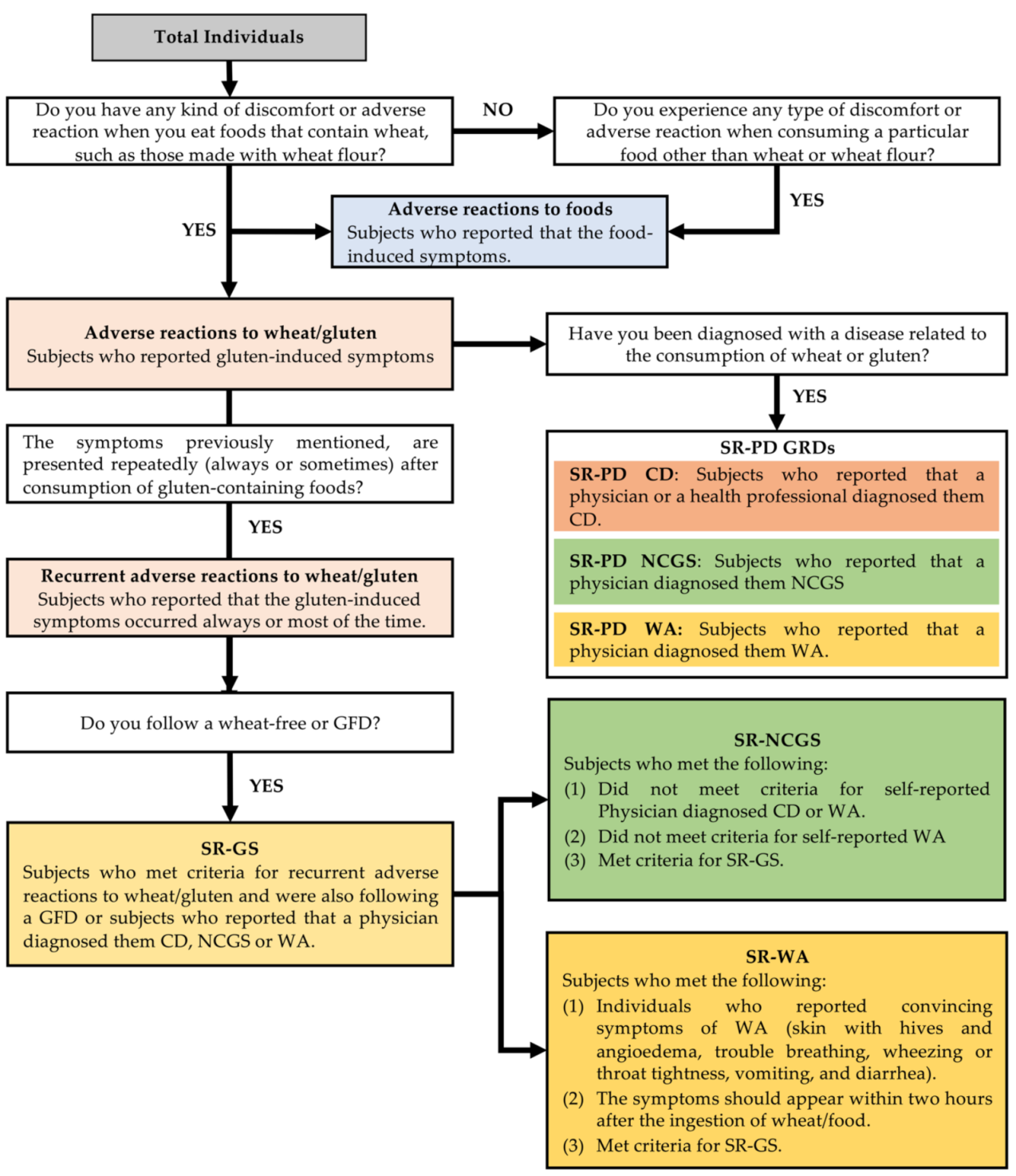
2.2. Classification of the Participants
2.3. Statistical Analysis and Ethical Issues
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Prevalence Rates
3.3. Overlapping of Physician-Diagnosed Gluten-Related Disorder
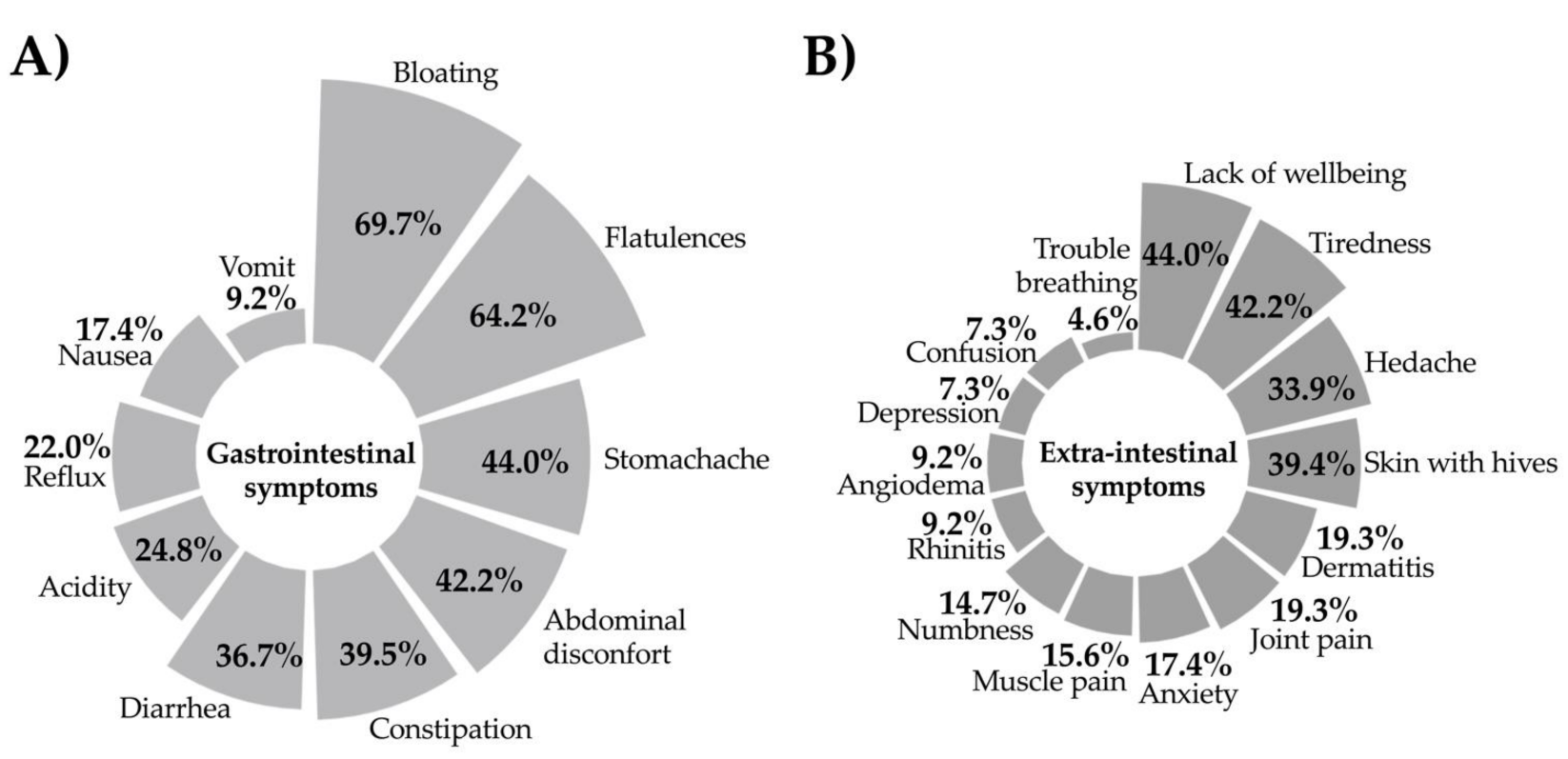
3.4. Symptoms Reported by SR-GS Cases
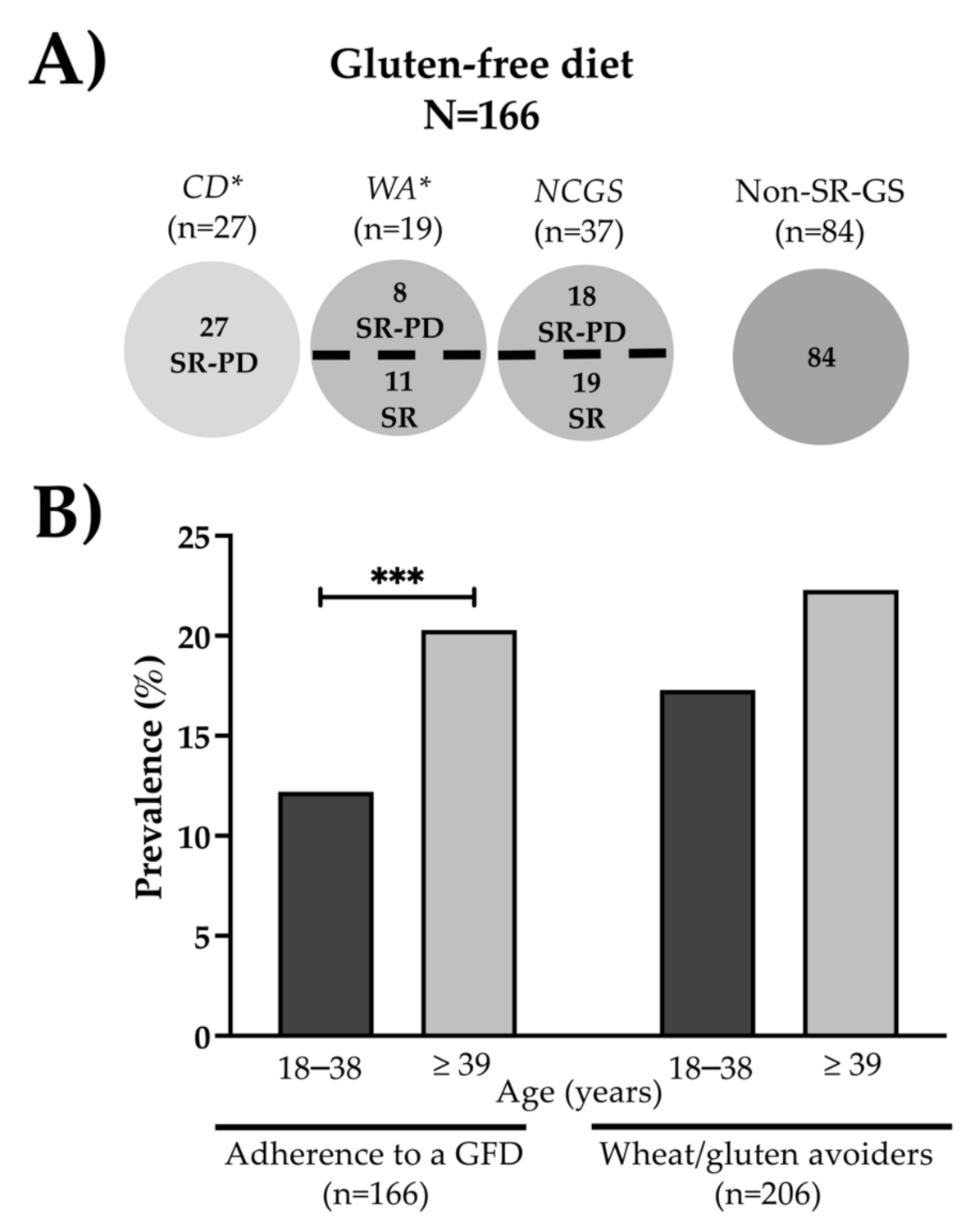
3.5. Gluten-Free Diet
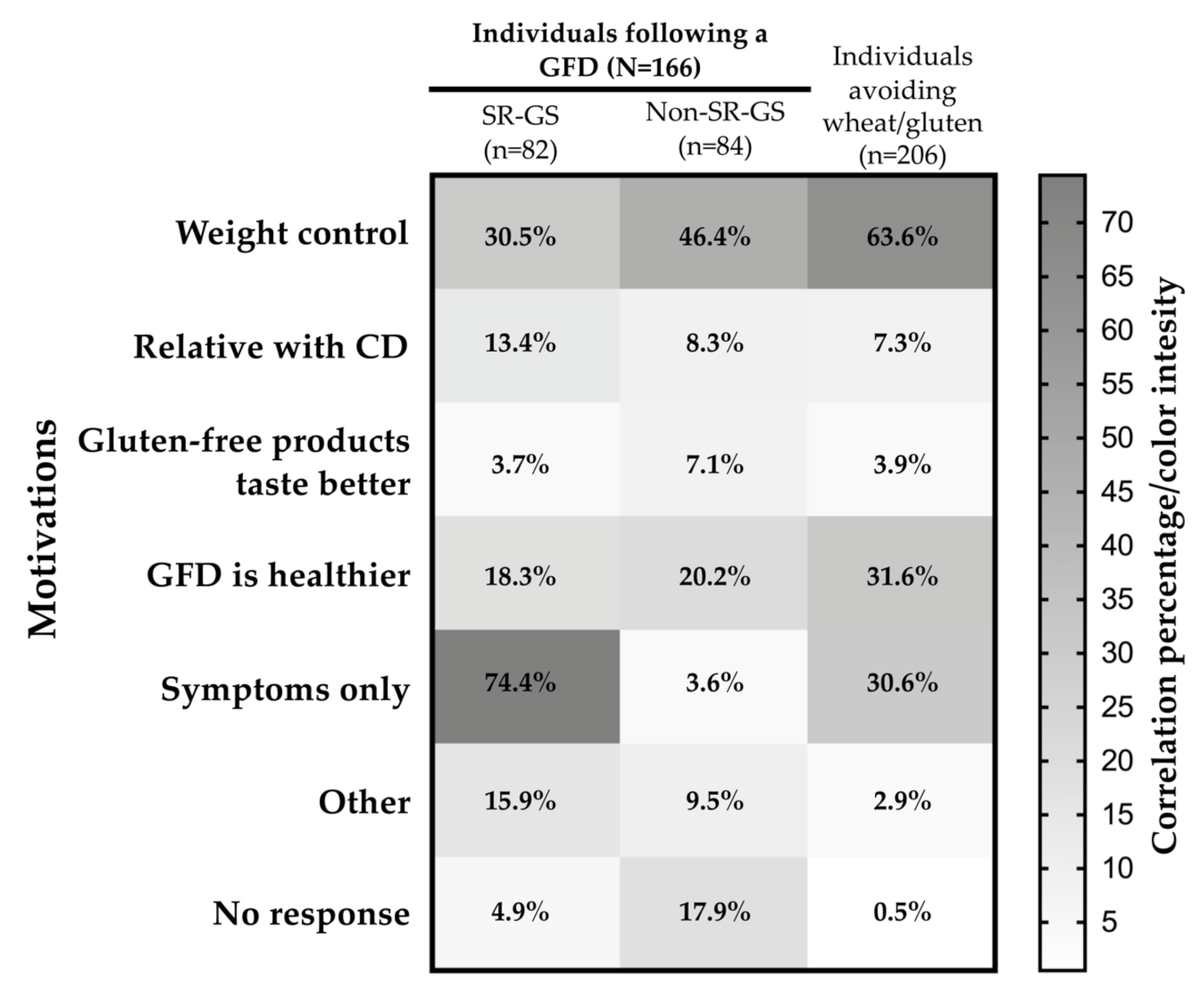
3.6. Reasons for Gluten-Free Dietary Non-Compliance and Motivations for Following a GFD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cabanillas, B. Gluten-related disorders: Celiac disease, wheat allergy, and nonceliac gluten sensitivity. Crit. Rev. Food Sci. Nutr. 2020, 60, 2606–2621. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Hardy, M.Y.; Cabrera-Chavez, F. Assessing of Celiac Disease and Nonceliac Gluten Sensitivity. Available online: https://www.hindawi.com/journals/grp/2015/723954/ (accessed on 29 December 2020).
- Ontiveros, N.; Flores-Mendoza, L.K.; Canizalez-Román, V.A.; Cabrera-Chavez, F. Food Allergy: Prevalence and Food Technology Approaches for the Control of IgE-Mediated Food Allergy. Austin J. Nutr. Food Sci. 2014, 2, 1029. [Google Scholar]
- Figueroa-Salcido, O.G.; Ontiveros, N.; Cabrera-Chavez, F. Gluten Vehicle and Placebo for Non-Celiac Gluten Sensitivity Assessment. Medicina 2019, 55, 117. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Chavez, F.; Dezar, G.V.A.; Islas-Zamorano, A.P.; Espinoza-Alderete, J.G.; Vergara-Jiménez, M.D.J.; Magaña-Ordorica, D.; Ontiveros, N. Prevalence of Self-Reported Gluten Sensitivity and Adherence to a Gluten-Free Diet in Argentinian Adult Population. Nutrients 2017, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Arámburo-Gálvez, J.G.; Beltrán-Cárdenas, C.E.; André, T.G.; Gomes, I.C.; Macêdo-Callou, M.A.; Braga-Rocha, É.M.; Mye-Takamatu-Watanabe, E.A.; Rahmeier-Fietz, V.; Figueroa-Salcido, O.G.; Vergara-Jiménez, M.D.J.; et al. Prevalence of Adverse Reactions to Glutenand People Going on a Gluten-Free Diet:A Survey Study Conducted in Brazil. Medicina 2020, 56, 163. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; De Magistris, L.; Dolinsek, J.; et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef] [PubMed]
- Potter, M.D.E.; Walker, M.M.; Jones, M.P.; Koloski, N.A.; Keely, S.; Talley, N.J. Wheat Intolerance and Chronic Gastrointestinal Symptoms in an Australian Population-based Study: Association between Wheat Sensitivity, Celiac Disease and Functional Gastrointestinal Disorders. Am. J. Gastroenterol. 2018, 113, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; The Study Group for Non-Celiac Gluten Sensitivity; Bardella, M.T.; Calabrò, A.; Troncone, R.; McColl, K.E.L. An Italian prospective multicenter survey on patients suspected of having non-celiac gluten sensitivity. BMC Med. 2014, 12, 85. [Google Scholar] [CrossRef] [PubMed]
- Van Gils, T.; Nijeboer, P.; Ijssennagger, C.E.; Sanders, D.S.; Mulder, C.J.; Bouma, G. Prevalence and Characterization of Self-Reported Gluten Sensitivity in The Netherlands. Nutrients 2016, 8, 714. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Rodríguez-Bellegarrigue, C.I.; Galicia-Rodríguez, G.; Vergara-Jiménez, M.D.J.; Zepeda-Gómez, E.M.; Arámburo-Gálvez, J.G.; Gracia-Valenzuela, M.H.; Cabrera-Chavez, F. Prevalence of Self-Reported Gluten-Related Disorders and Adherence to a Gluten-Free Diet in Salvadoran Adult Population. Int. J. Environ. Res. Public Health 2018, 15, 786. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Chávez, F.; Granda-Restrepo, D.M.; Arámburo-Gálvez, J.G.; Franco-Aguilar, A.; Magaña-Ordorica, D.; Vergara-Jiménez, M.D.J.; Ontiveros, N. Self-Reported Prevalence of Gluten-Related Disorders and Adherence to Gluten-Free Diet in Colombian Adult Population. Available online: https://www.hindawi.com/journals/grp/2016/4704309/ (accessed on 27 December 2020).
- Ontiveros, N.; Gallardo, J.A.-L.; Vergara-Jiménez, M.D.J.; Cabrera-Chavez, F. Self-Reported Prevalence of Symptomatic Adverse Reactions to Gluten and Adherence to Gluten-Free Diet in an Adult Mexican Population. Nutrients 2015, 7, 6000–6015. [Google Scholar] [CrossRef] [PubMed]
- Araya, M.; Bascuñán, K.A.; Alarcón-Sajarópulos, D.; Cabrera-Chavez, F.; Oyarzún, A.; Fernández, A.; Ontiveros, N. Living with Gluten and Other Food Intolerances: Self-Reported Diagnoses and Management. Nutrients 2020, 12, 1892. [Google Scholar] [CrossRef] [PubMed]
- Real Delor, R.E.; Arza, G.; Chamorro, M.E.; Dalles, I.; Ibarra Douglas, A. La Enfermedad celiaca en el Paraguay. Rev. Nac. 2011, 3, 7–15. [Google Scholar]
- Real Delor, R.E.; Centurión-Medina, I.C. Calidad de vida en adultos del Paraguay con enfermedad celiaca. Duazary Rev. Int. Cienc. Salud 2018, 15, 61–70. [Google Scholar] [CrossRef]
- Ferreira, S.; Chamorro, M.E.; Ortíz, J.; Carpinelli, M.M.; Giménez, V.; Langjahr, P. Anticuerpo Anti-Transglutaminasa Tisular En Adultos Con Enfermedad Celíaca y Su Relación Con La Presencia y Duración de La Dieta Libre de Gluten. Rev. Gastroenterol. Perú 2018, 38, 228–233. [Google Scholar] [PubMed]
- Paraguay: Grain and Feed Annual | USDA Foreign Agricultural Service. Available online: https://www.fas.usda.gov/data/paraguay-grain-and-feed-annual-1 (accessed on 27 December 2020).
- Aziz, I.; Lewis, N.R.; Hadjivassiliou, M.; Winfield, S.N.; Rugg, N.; Kelsall, A.; Newrick, L.; Sanders, D.S. A UK study assessing the population prevalence of self-reported gluten sensitivity and referral characteristics to secondary care. Eur. J. Gastroenterol. Hepatol. 2014, 26, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Croall, I.; Trott, N.; Rej, A.; Aziz, I.; O’Brien, D.; George, H.A.; Hossain, M.Y.; Marks, L.J.S.; Richardson, J.I.; Sanders, D.S.; et al. A Population Survey of Dietary Attitudes towards Gluten. Nutrients 2019, 11, 1276. [Google Scholar] [CrossRef] [PubMed]
- Katz, R.; Jung, J.; Callorda, F. El Estado de La Digitalización de América Latina Frente a La Pandemia Del COVID-19; CAF: Caracas, Venezuela, 2020. [Google Scholar]
- Vavricka, S.R.; Stelzer, T.; Lattmann, J.; Stotz, M.; Lehmann, R.; Zeitz, J.; Scharl, M.; Misselwitz, B.; Pohl, D.; Fried, M.; et al. Celiac Disease is Misdiagnosed Based on Serology Only in a Substantial Proportion of Patients. J. Clin. Gastroenterol. 2018, 52, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Händel, N.; Mothes, T.; Petroff, D.; Baber, R.; Jurkutat, A.; Flemming, G.; Kiess, W.; Hiemisch, A.; Körner, A.; Schlumberger, W.; et al. Will the Real Coeliac Disease Please Stand Up? Coeliac Disease Prevalence in the German LIFE Child Study. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Le, T.T.K.; Tran, T.T.B.; Ho, H.T.M.; Vu, A.T.L.; Lopata, A.L. Prevalence of food allergy in Vietnam: Comparison of web-based with traditional paper-based survey. World Allergy Organ. J. 2018, 11, 16. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable * | % | n (Male/Female) |
|---|---|---|
| Gender | 34.9/65.1 | 369/689 |
| Non-food allergy | 6.90 | 73 |
| IBS ** | 8.79 | 93 |
| Colitis | 1.42 | 15 |
| Lactose intolerance | 8.70 | 92 |
| Psychiatric disease | 1.51 | 16 |
| Food intolerance | 1.70 | 18 |
| Food allergy | 3.21 | 34 |
| Eating disorsers | 1.42 | 15 |
| Diabetes mellitus | 4.73 | 50 |
| Gastrointestinal cancer | 0.09 | 1 |
| Assessment | (+) Cases * | Mean Age in Years (Range) | Prevalence by Gender % (95% CI) | p Value | General Prevalence % (95% CI) |
|---|---|---|---|---|---|
| Adverse reactions to food | Total = 337 | 40.9 (19–84) | M 19.24% (15.34–23.64) F 38.60% (34.95–42.36) | <0.0001 | 31.85% (29.05–34.76) |
| M = 71 | |||||
| F = 266 | |||||
| Adverse reactions to wheat/gluten | Total = 225 | 42.5 (19–84) | M 9.21% (6.46–12.64) F 27.72% (24.41–31.23) | <0.0001 | 21.26% (18.84–23.86) |
| M = 34 | |||||
| F = 191 | |||||
| Recurrent adverse reactions to wheat/gluten | Total = 177 | 42.6 (19–84) | M 6.23% (3.99–9.20) F 22.35% (19.29–25.65) | <0.0001 | 16.72% (14.53–19.12) |
| M = 23 | |||||
| F = 154 | |||||
| (a) SR-GS * | Total = 109 † | 42.89 (21–84) | M 4.06% (2.29–6.61) F 13.64% (11.17–16.43) | <0.0001 | 10.30% (8.53–12.29) |
| M = 15 | |||||
| F = 94 | |||||
| (b) Celiac disease | Total = 33 | 42.84 (22–84) | M 1.89% (0.76–3.87) F 3.77% (2.48–5.48) | 0.1361 | 3.11% (2.15–4.35) |
| M = 7 | |||||
| F = 26 | |||||
| (c) Wheat allergy | Total = 22 | 44.0 (21–84) | M 0.27% (0.006–1.50) F 3.04% (1.89–4.62) | 0.0012 | 2.07% (1.30–3.13) |
| M = 1 | |||||
| F = 21 | |||||
| (d) SR-NCGS ** | Total = 55 | 43.2 (21–66) | M 1.89% (0.76–3.87) F 6.96% (5.18–9.13) | 0.0002 | 5.19% (3.94–6.71) |
| M = 7 | |||||
| F = 48 | |||||
| Adherence to GFD *** | Total = 166 | 42.7 (18–84) | M 8.13% (5.55–11.4) F 19.73% (16.83–22.91) | <0.0001 | 15.69% (13.55–18.02) |
| M = 30 | |||||
| F = 136 | |||||
| Avoidance of wheat/gluten-containing foods | Total = 206 | 40.0 (18–77) | M 15.17% (11.67–19.25) F 21.77% (18.74–25.04) | 0.0114 | 19.47% (17.13–21.99) |
| M = 56 | |||||
| F = 150 |
| Individual | Diagnosed by | Diagnosed Disorder | Following a GFD | Recurrent Symptoms to Wheat/Gluten | Excluded or Re-Classified | Criteria for Exclusion/Inclusion |
|---|---|---|---|---|---|---|
| I-1 | Physician and dietitian | NCGS CD | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. The participant met the criteria for SR-GS and CD. |
| I-2 | Physician and dietitian | NCGS CD | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. The participant met the criteria for SR-GS and CD. |
| I-3 | Profesor | NCGS WA | No | Yes | Excluded | CD or WA does not co-exist with NCGS. The participant neither met criteria for WA nor SR-GS and WA. |
| I-4 | Profesor | NCGS WA | No | No | Excluded | CD or WA does not co-exist with NCGS. The participant neither met criteria for WA nor SR-GS and WA. |
| I-5 | Gastroenterologist and dietitian | NCGS WA | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. The participant met the criteria for SR-GS and WA |
| I-6 | Endocrinologist | NCGS WA | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. Met the criteria for SR-GS and WA |
| I-7 | Physician | NCGS CD | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. The participant met the criteria for SR-GS and CD |
| I-8 | Dermatologist | NCGS CD WA | Yes | Yes | Re-classified | CD or WA does not co-exist with NCGS. The participant met the criteria for SR-GS, CD and WA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ontiveros, N.; Real-Delor, R.E.; Mora-Melgem, J.A.; Beltrán-Cárdenas, C.E.; Figueroa-Salcido, O.G.; Vergara-Jiménez, M.d.J.; Cárdenas-Torres, F.I.; Flores-Mendoza, L.K.; Arámburo-Gálvez, J.G.; Cabrera-Chávez, F. Prevalence of Wheat/Gluten-Related Disorders and Gluten-Free Diet in Paraguay: An Online Survey-Based Study. Nutrients 2021, 13, 396. https://doi.org/10.3390/nu13020396
Ontiveros N, Real-Delor RE, Mora-Melgem JA, Beltrán-Cárdenas CE, Figueroa-Salcido OG, Vergara-Jiménez MdJ, Cárdenas-Torres FI, Flores-Mendoza LK, Arámburo-Gálvez JG, Cabrera-Chávez F. Prevalence of Wheat/Gluten-Related Disorders and Gluten-Free Diet in Paraguay: An Online Survey-Based Study. Nutrients. 2021; 13(2):396. https://doi.org/10.3390/nu13020396
Chicago/Turabian StyleOntiveros, Noé, Raúl Emilio Real-Delor, José Antonio Mora-Melgem, Carlos Eduardo Beltrán-Cárdenas, Oscar Gerardo Figueroa-Salcido, Marcela de Jesús Vergara-Jiménez, Feliznando Isidro Cárdenas-Torres, Lilian Karem Flores-Mendoza, Jesús Gilberto Arámburo-Gálvez, and Francisco Cabrera-Chávez. 2021. "Prevalence of Wheat/Gluten-Related Disorders and Gluten-Free Diet in Paraguay: An Online Survey-Based Study" Nutrients 13, no. 2: 396. https://doi.org/10.3390/nu13020396
APA StyleOntiveros, N., Real-Delor, R. E., Mora-Melgem, J. A., Beltrán-Cárdenas, C. E., Figueroa-Salcido, O. G., Vergara-Jiménez, M. d. J., Cárdenas-Torres, F. I., Flores-Mendoza, L. K., Arámburo-Gálvez, J. G., & Cabrera-Chávez, F. (2021). Prevalence of Wheat/Gluten-Related Disorders and Gluten-Free Diet in Paraguay: An Online Survey-Based Study. Nutrients, 13(2), 396. https://doi.org/10.3390/nu13020396