
A Systematic Review of Diet Quality Index and Obesity among Chinese Adults

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Exposure
2.4. Outcomes
2.5. Search Strategies
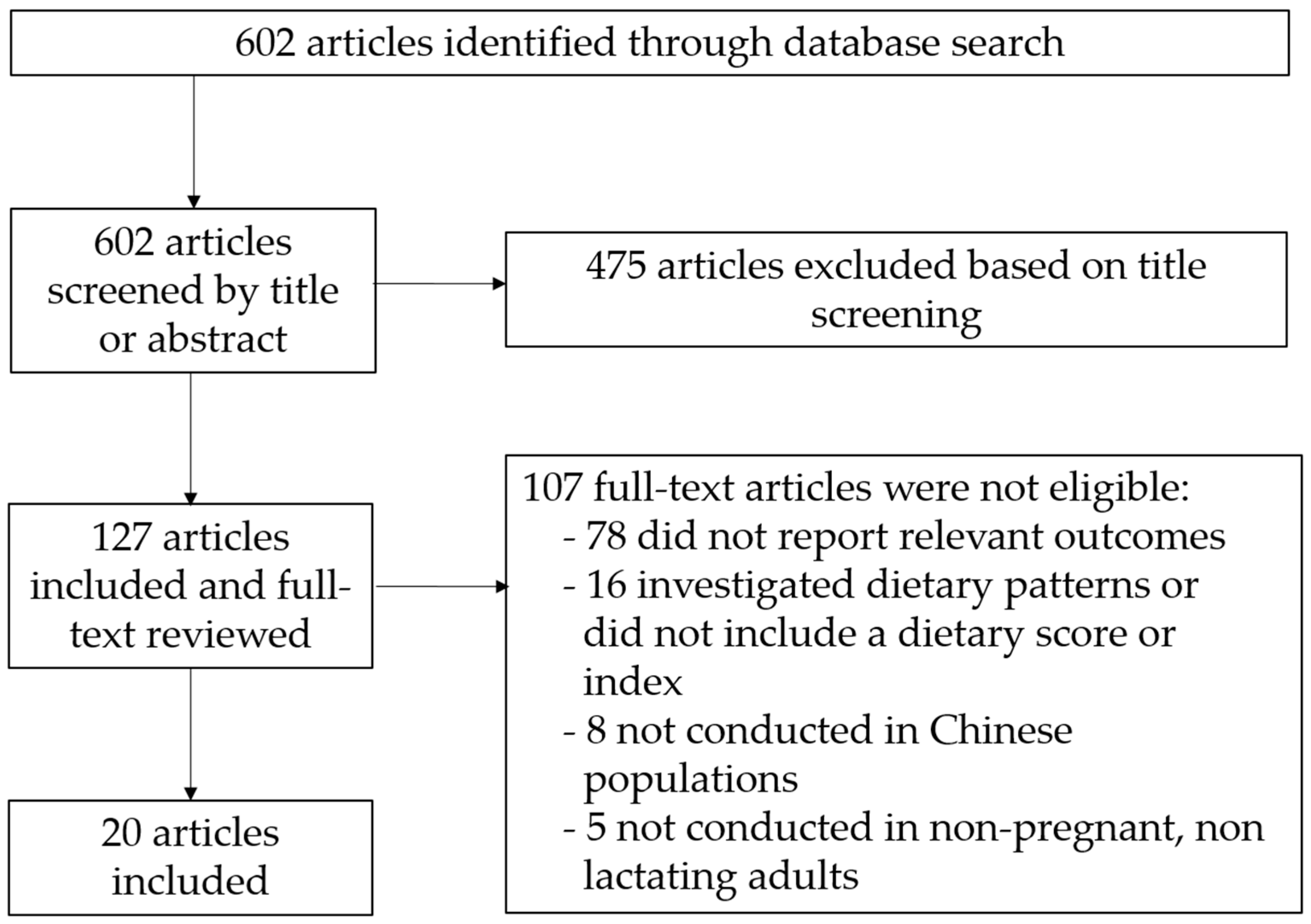
2.6. Study Selection
2.7. Study Quality Assessment
3. Results
3.1. HEI and Obesity-Related Outcomes
3.2. Adherence to the CHFP and Obesity-Related Outcomes
3.3. The China Diet Quality Index (DQI) and Obesity-Related Outcomes
3.4. The Dietary Balance Index (DBI) and Obesity-Related Outcomes
3.5. Food Diversity and Obesity-Related Outcomes
3.6. Dietary Approaches to Stop Hypertension (DASH) and Alternate Mediterranean Diets (aMED) Scores and Obesity-Related Outcomes
3.7. Quality of Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Biener, A.I.; Decker, S.L. Medical care use and expenditures associated with adult obesity in the United States. JAMA 2018, 319, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnes, A.S. The epidemic of obesity and diabetes: Trends and treatments. Tex. Heart Inst. J. 2011, 38, 142–144. [Google Scholar] [PubMed]
- Dwivedi, A.K.; Dubey, P.; Cistola, D.P.; Reddy, S.Y. Association between obesity and cardiovascular outcomes: Updated Evidence from Meta-analysis Studies. Curr. Cardiol. Rep. 2020, 22, 25. [Google Scholar] [CrossRef]
- Roberts, D.L.; Dive, C.; Renehan, A.G. Biological mechanisms linking obesity and cancer risk: New perspectives. Annu. Rev. Med. 2010, 61, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Furth, S.L.; Zoccali, C.; Committee, W.K.D.S. Obesity and kidney disease: Hidden consequences of the epidemic. Am. J. Nephrol. 2017, 45, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Qasim, A.; Turcotte, M.; de Souza, R.J.; Samaan, M.C.; Champredon, D.; Dushoff, J.; Speakman, J.R.; Meyre, D. On the origin of obesity: Identifying the biological, environmental and cultural drivers of genetic risk among human populations. Obes. Rev. 2018, 19, 121–149. [Google Scholar] [CrossRef]
- Chin, S.H.; Kahathuduwa, C.N.; Binks, M. Physical activity and obesity: What we know and what we need to know. Obes. Rev. 2016, 17, 1226–1244. [Google Scholar] [CrossRef] [PubMed]
- Komaroff, A.L. The microbiome and risk for obesity and diabetes. JAMA 2017, 317, 355–356. [Google Scholar] [CrossRef]
- Dhakal, C.K.; Khadka, S. Heterogeneities in consumer diet quality and health outcomes of consumers by store choice and income. Nutrients 2021, 13, 1046. [Google Scholar] [CrossRef]
- Ferretti, F.; Mariani, M.; Sarti, E. Is the development of obesogenic food environments a self-reinforcing process? Evidence from soft drink consumption. Glob. Health 2021, 17, 91. [Google Scholar] [CrossRef]
- McLaren, L. Socioeconomic status and obesity. Epidemiol. Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, A.M.; Jones, A.C.; Mizdrak, A.; Signal, L.; Genç, M.; Wilson, N. Impact of sugar-sweetened beverage taxes on purchases and dietary intake: Systematic review and meta-analysis. Obes. Rev. 2019, 20, 1187–1204. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Zhai, F.; Popkin, B.M. Impacts of China’s edible oil pricing policy on nutrition. Soc. Sci. Med. 2008, 66, 414–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, R.L.; Maulding, M.K.; Eicher-Miller, H.A. Effect of Supplemental Nutrition Assistance Program-Education (SNAP-Ed) on food security and dietary outcomes. Nutr. Rev. 2019, 77, 903–921. [Google Scholar] [CrossRef]
- Schlesinger, S.; Neuenschwander, M.; Schwedhelm, C.; Hoffmann, G.; Bechthold, A.; Boeing, H.; Schwingshackl, L. Food groups and risk of overweight, obesity, and weight gain: A wystematic review and dose-response meta-analysis of prospective studies. Adv. Nutr. 2019, 10, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Asghari, G.; Mirmiran, P.; Yuzbashian, E.; Azizi, F. A systematic review of diet quality indices in relation to obesity. Br. J. Nutr. 2017, 117, 1055–1065. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M. Synthesis and implications: China’s nutrition transition in the context of changes across other low- and middle-income countries. Obes. Rev. 2014, 15, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.; Xi, B.; Yang, L.; Sun, J.; Zhao, M.; Bovet, P. Trends in the prevalence of overweight, obesity, and abdominal obesity among Chinese adults between 1993 and 2015. Int. J. Obes. 2021, 45, 427–437. [Google Scholar] [CrossRef]
- Wei, J.M.; Li, S.; Claytor, L.; Partridge, J.; Goates, S. Prevalence and predictors of malnutrition in elderly Chinese adults: Results from the China Health and Retirement Longitudinal Study. Public Health Nutr. 2018, 21, 3129–3134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, E.T.; Ohls, J.; Carlson, S.; Fleming, K. The healthy eating index: Design and applications. J. Am. Diet. Assoc. 1995, 95, 1103–1108. [Google Scholar] [CrossRef]
- Fung, T.T.; McCullough, M.L.; Newby, P.K.; Manson, J.E.; Meigs, J.B.; Rifai, N.; Willett, W.C.; Hu, F.B. Diet-quality scores and plasma concentrations of markers of inflammation and endothelial dysfunction. Am. J. Clin. Nutr. 2005, 82, 163–173. [Google Scholar] [CrossRef]
- Yuan, Y.Q.; Li, F.; Dong, R.H.; Chen, J.S.; He, G.S.; Li, S.G.; Chen, B. The development of a Chinese healthy eating index and its application in the general population. Nutrients 2017, 9, 977. [Google Scholar] [CrossRef] [Green Version]
- Su, X.; Zhu, W.; Li, N.; Sun, J.; Zhu, Y.; Liu, T.; Xia, H.; Dai, Z.; Zhang, Y.; Pan, L.; et al. Adjusting DBI-2016 to dietary balance index for Chinese maternal women and assessing the association between maternal dietary quality and postpartum weight retention: A longitudinal study. PLoS ONE 2020, 15, e0237225. [Google Scholar] [CrossRef]
- Zhou, B.F. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults--study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Environ. Sci. 2002, 15, 83–96. [Google Scholar]
- Ren, Q.; Su, C.; Wang, H.; Wang, Z.; Du, W.; Zhang, B. Prospective study of optimal obesity index cut-off values for predicting incidence of hypertension in 18–65-year-old Chinese adults. PLoS ONE 2016, 11, e0148140. [Google Scholar] [CrossRef] [PubMed]
- Frandsen, T.F.; Bruun Nielsen, M.F.; Lindhardt, C.L.; Eriksen, M.B. Using the full PICO model as a search tool for systematic reviews resulted in lower recall for some PICO elements. J. Clin. Epidemiol. 2020, 127, 69–75. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. Study Quality Assessment Tools 2018. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessmenttools (accessed on 30 June 2021).
- Al-Ibrahim, A.A.; Jackson, R.T. Healthy eating index versus alternate healthy index in relation to diabetes status and health markers in U.S. adults: NHANES 2007–2010. Nutr. J. 2019, 18, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, L.T.F.; Chan, R.S.M.; Ko, G.T.C.; Lau, E.S.H.; Chow, F.C.C.; Kong, A.P.S. Diet quality is inversely associated with obesity in Chinese adults with type 2 diabetes. Nutr. J. 2018, 17, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitton, C.; Rebello, S.A.; Lee, J.; Tai, E.S.; van Dam, R.M. A healthy asian a posteriori dietary pattern correlates with a priori dietary patterns and is associated with cardiovascular disease risk factors in a multiethnic Asian population. J. Nutr. 2018, 148, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, N.; Naidoo, N.; Koh, W.P.; Yuan, J.M.; van Dam, R.M. The alternative healthy eating index is associated with a lower risk of fatal and nonfatal acute myocardial infarction in a Chinese adult population. J. Nutr. 2016, 146, 1379–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, Y.C.; Lee, M.S.; Chiou, J.M.; Chen, T.F.; Chen, Y.C.; Chen, J.H. Association of diet quality and vegetable variety with the risk of cognitive decline in Chinese older adults. Nutrients 2019, 11, 1666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Adair, L.S.; Cai, J.; Gordon-Larsen, P.; Siega-Riz, A.M.; Zhang, B.; Popkin, B.M. Diet quality is linked to insulin resistance among adults in China. J. Nutr. 2017, 147, 2102–2108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Siega-Riz, A.M.; Gordon-Larsen, P.; Cai, J.; Adair, L.S.; Zhang, B.; Popkin, B.M. Diet quality and its association with type 2 diabetes and major cardiometabolic risk factors among adults in China. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 987–1001. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.K.; Beresford, S.A.A.; Frank, L.L.; Schreiner, P.J.; Burke, G.L.; Fitzpatrick, A.L. Modifications to the healthy eating index and its ability to predict obesity: The multi-ethnic study of atherosclerosis. Am. J. Clin. Nutr. 2008, 88, 64–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.-W.; McNaughton, S.A.; He, Q.-Q.; Leech, R. Longitudinal trajectories of diet quality and subsequent mortality among Chinese adults: Results from the China health and nutrition survey 1997–2015. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 51. [Google Scholar] [CrossRef]
- Poti, J.M.; Braga, B.; Qin, B. Ultra-processed food intake and obesity: What really aatters for health-processing or nutrient content? Curr. Obes. Rep. 2017, 6, 420–431. [Google Scholar] [CrossRef]
- Ge, K. The transition of Chinese dietary guidelines and food guide pagoda. Asia Pac. J. Clin. Nutr. 2011, 20, 439–446. [Google Scholar]
- Yu, D.; Zhang, X.; Xiang, Y.B.; Yang, G.; Li, H.; Gao, Y.T.; Zheng, W.; Shu, X.O. Adherence to dietary guidelines and mortality: A report from prospective cohort studies of 134,000 Chinese adults in urban Shanghai. Am. J. Clin. Nutr. 2014, 100, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, S.; Li, H.; Yu, D.; Gao, J.; Gao, Y.; Tran, H.; Xiang, Y.-B.; Zheng, W.; Shu, X.-O. Adherence to dietary recommendations and colorectal cancer risk: Results from two prospective cohort studies. Int. J. Epidemiol. 2020, 49, 270–280. [Google Scholar] [CrossRef]
- Wang, F.; Cai, H.; Gu, K.; Shi, L.; Yu, D.; Zhang, M.; Zheng, W.; Zheng, Y.; Bao, P.; Shu, X.O. Adherence to Dietary Recommendations among Long-Term Breast Cancer Survivors and Cancer Outcome Associations. Cancer Epidemiol. Biomark. Prev. 2020, 29, 386–395. [Google Scholar] [CrossRef]
- Stookey, J.D.; Wang, Y.; Ge, K.; Lin, H.; Popkin, B.M. Measuring diet quality in China: The INFH-UNC-CH diet quality index. Eur. J. Clin. Nutr. 2000, 54, 811–821. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Wang, H.; Tian, X. Changing diet quality in China during 2004–2011. Int. J. Environ. Res. Public Health 2016, 14, 13. [Google Scholar] [CrossRef] [Green Version]
- He, Y.; Zhai, F.; Yang, X.; Ge, K. The Chinese Diet Balance Index revised. Acta Nutr. Sin. 2009, 31, 532–536. [Google Scholar]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Assessing dietary quality of older Chinese people using the Chinese Diet Balance Index (DBI). PLoS ONE 2015, 10, e0121618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zang, J.; Yu, H.; Zhu, Z.; Lu, Y.; Liu, C.; Yao, C.; Bai, P.; Guo, C.; Jia, X.; Zou, S.; et al. Does the dietary pattern of Shanghai residents change across seasons andarea of residence: Assessing dietary quality using the Chinese Diet Balance Index (DBI). Nutrients 2017, 9, 251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Qin, G.; Liu, Z.; Li, Z.; Li, J.; Varma, D.S.; Wan, Q.; Zhao, J.; Min, X.; Han, X.; et al. Dietary Balance Index-07 and the risk of anemia in middle aged and elderly people in southwest China: A cross sectional study. Nutrients 2018, 10, 162. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Leepromrath, S.; Tian, X.; Zhou, D. Dynamics of Chinese diet divergence from Chinese food pagoda and its association with adiposity and influential factors: 2004–2011. Int. J. Environ. Res. Public Health 2020, 17, 507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, X.; Wu, M.; Zang, J.; Zhu, Y.; Wang, H. Dietary diversity and adiposity in Chinese men and women: An analysis of four waves of cross-sectional survey data. Eur. J. Clin. Nutr. 2017, 71, 506–511. [Google Scholar] [CrossRef]
- Zhao, W.; Zhang, J.; Zhao, A.; Wang, M.; Wu, W.; Tan, S.; Guo, M.; Zhang, Y. Using an introduced index to assess the association between food diversity and metabolic syndrome and its components in Chinese adults. BMC Cardiovasc. Disord. 2018, 18, 189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, L.; Lu, H.; Wu, J.; Wang, X.; Wang, W.; Du, M.; Wang, P.; Du, S.; Su, Y.; Zhang, N. Association between diet quality and obesity indicators among the working-age adults in Inner Mongolia, Northern China: A cross-sectional study. BMC Public Health 2020, 20, 1165. [Google Scholar] [CrossRef]
- Xu, X.; Hall, J.; Byles, J.; Shi, Z. Dietary pattern is associated with obesity in older people in China: Data from China health and nutrition survey (CHNS). Nutrients 2015, 7, 5386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ervin, R.B. Healthy Eating Index—2005 total and component scores for adults aged 20 and over: National Health and Nutrition Examination Survey, 2003–2004. Natl. Health Stat. Rep. 2011, 44, 1–9. [Google Scholar]
- Harrington, J.M.; Fitzgerald, A.P.; Kearney, P.M.; McCarthy, V.J.; Madden, J.; Browne, G.; Dolan, E.; Perry, I.J. DASH diet score and distribution of blood pressure in middle-aged men and women. Am. J. Hypertens. 2013, 26, 1311–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popkin, B.M. The nutrition transition and obesity in the developing world. J. Nutr. 2001, 131, 871S–873S. [Google Scholar] [CrossRef]
- Popkin, B.M. Nutrition in transition: The changing global nutrition challenge. Asia Pac. J. Clin. Nutr. 2001, 10, S13–S18. [Google Scholar] [CrossRef]
- Wang, Z.; Zhai, F.; Du, S.; Popkin, B. Dynamic shifts in Chinese eating behaviors. Asia Pac. J. Clin. Nutr. 2008, 17, 123–130. [Google Scholar] [PubMed]
- Dearth-Wesley, T.; Wang, H.; Popkin, B.M. Under- and overnutrition dynamics in Chinese children and adults (1991–2004). Eur. J. Clin. Nutr. 2008, 62, 1302–1307. [Google Scholar] [CrossRef]
- Chinese Nutrition Society. Scientific Research Report on the Dietary Guidelines for Chinese Residents 2021; Chinese Nutrition Society: Beijing, China, 2021. [Google Scholar]
- Wang, L.; Zhou, B.; Zhao, Z.; Yang, L.; Zhang, M.; Jiang, Y.; Li, Y.; Zhou, M.; Huang, Z.; Zhang, X.; et al. Body-mass index and obesity in urban and rural China: Findings from consecutive nationally representative surveys during 2004–2018. Lancet 2021, 398, 53–63. [Google Scholar] [CrossRef]
- Jones-Smith, J.C.; Gordon-Larsen, P.; Siddiqi, A.; Popkin, B.M. Emerging disparities in overweight by educational attainment in Chinese adults (1989–2006). Int. J. Obes. 2012, 36, 866–875. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef] [Green Version]
- Couch, S.C.; Saelens, B.E.; Khoury, P.R.; Dart, K.B.; Hinn, K.; Mitsnefes, M.M.; Daniels, S.R.; Urbina, E.M. Dietary approaches to stop hypertension dietary intervention improves blood pressure and vascular health in youth with elevated blood pressure. Hypertension 2021, 77, 241–251. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Babyak, M.A.; Hinderliter, A.; Watkins, L.L.; Craighead, L.; Lin, P.H.; Caccia, C.; Johnson, J.; Waugh, R.; Sherwood, A. Effects of the DASH diet alone and in combination with exercise and weight loss on blood pressure and cardiovascular biomarkers in men and women with high blood pressure: The ENCORE study. Arch. Intern. Med. 2010, 170, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Azadbakht, L.; Fard, N.R.; Karimi, M.; Baghaei, M.H.; Surkan, P.J.; Rahimi, M.; Esmaillzadeh, A.; Willett, W.C. Effects of the Dietary Approaches to Stop Hypertension (DASH) eating plan on cardiovascular risks among type 2 diabetic patients: A randomized crossover clinical trial. Diabetes Care 2011, 34, 55–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- D’Innocenzo, S.; Biagi, C.; Lanari, M. Obesity and the Mediterranean diet: A review of evidence of the role and sustainability of the Mediterranean diet. Nutrients 2019, 11, 1306. [Google Scholar] [CrossRef] [Green Version]
- Wei, K.; Nyunt, M.S.; Gao, Q.; Wee, S.L.; Yap, K.B.; Ng, T.P. Association of frailty and malnutrition with long-term functional and mortality outcomes among community-dwelling older adults: Results from the Singapore longitudinal aging study 1. JAMA Netw. Open 2018, 1, e180650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayawardena, R.; Byrne, N.M.; Soares, M.J.; Katulanda, P.; Yadav, B.; Hills, A.P. High dietary diversity is associated with obesity in Sri Lankan adults: An evaluation of three dietary scores. BMC Public Health 2013, 13, 314. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zhai, F. Programme and policy options for preventing obesity in China. Obes. Rev. 2013, 14, 134–140. [Google Scholar] [CrossRef] [Green Version]
- The State Council of China. National Nutrition Program 2017–2030; The State Council of China: Beijing, China, 2017. [Google Scholar]
- Development and Information Technology. Action for a Healthy China (2019–2030); The State Council of China: Beijing, China, 2019. [Google Scholar]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, L.; Gao, L.; Pan, A.; Xue, H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 446–461. [Google Scholar] [CrossRef]
- Anderson, C.; Harrigan, M.; George, S.M.; Ferrucci, L.M.; Sanft, T.; Irwin, M.L.; Cartmel, B. Changes in diet quality in a randomized weight loss trial in breast cancer survivors: The lifestyle, exercise, and nutrition (LEAN) study. NPJ Breast Cancer 2016, 2, 16026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allaire, B.T.; Tjaden, A.H.; Venditti, E.M.; Apolzan, J.W.; Dabelea, D.; Delahanty, L.M.; Edelstein, S.L.; Hoskin, M.A.; Temple, K.A.; Wylie-Rosett, J.; et al. Diet quality, weight loss, and diabetes incidence in the Diabetes Prevention Program (DPP). BMC Nutr. 2020, 6, 74. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Study Design | Number of Participants | Population | Dietary Assessment Method | Index | Outcome | Findings |
|---|---|---|---|---|---|---|---|
| Stookey et al., 2000 [43] | Cross-sectional | 7450 | CHNS 1991, aged 20–59 years | 3-day 24-h recall | China DQI | BMI, underweight, overweight, obesity | The risk of being underweight decreased and the risk of being overweight increased with each unit increase in DQI total score. |
| Gao et al., 2008 [36] | Longitudinal | 790 (Chinese subgroup, 51.7% females) | Multi-Ethnic Study of Atherosclerosis (MESA), mean age at 62.9 years | FFQ | HEI-05, HEI-90 | BMI, WC | Inverse associations between HEI-05 and BMI at baseline or follow-up, no association with WC. |
| Xu et al., 2015 [53] | Cross-sectional | 2745 (1300 males, 1445 females) | Participants aged over 60 in the CHNS 2009 | 3-day 24-h recall | DBI-07 | BMI, underweight | Underweight was associated with lower dietary balance scores. |
| Neelakantan et al., 2016 [32] | Nested case-control | 751 incident cases of AMI (564 nonfatal and 288 fatal) and 1443 matched controls, 35% females in both groups | The Singapore Chinese Health Study, mean age at 59 years | FFQ | AHEI-2010 | BMI | BMI did not differ among quartiles of AHEI among controls. |
| Tian et al., 2016 [50] | Cross-sectional | 17,825 (9459 males, 8366 females) | CHNS (2004, 2006, 2009 and 2011), mean age at 45.4 ± 11.9 years | 3-day 24-h recall | DDS | BMI, overweight | A positive association between dietary diversity and being overweight in men only. |
| Huang et al., 2017 [44] | Cross-sectional | 13,833 (53% females) | Four waves (2004, 2006, 2009, and 2011) of the CHNS, mean age at 42.7 ± 10.4 years | 3-day 24-h recall | China DQI | BMI, overweight, obesity | Higher DQI scores were positively associated with BMI in overweight and obese individuals compared to normal weight. |
| Wang et al., 2017 [34] | Longitudinal | 4734 (2263 males, 2471 females). | Participants who had ≥2 waves of dietary data from 1991 to 2006 in the CHNS, aged 18–65 years | 3-day 24-h recall | tAHEI | BMI | No differences in baseline BMI in low versus high tAHEI scores; no differences in BMI in those that had different patterns of tAHEI changes over 1 year. |
| Yuan et al., 2017 [23] | Cross-sectional | 14,584 (52% females) | CHNS 2011 | 3-day 24-h recall | CHEI | BMI, underweight, overweight, obesity | People who were underweight had lower CHEI scores than people who were normal weight, but no significant difference between normal weight and overweight or obesity. |
| Zang et al., 2017 [47] | Cross-sectional | 1680 (836 males and 844 females) | The Shanghai Diet and Health Survey (SDHS), age ≥ 15 years) | 3-day 24-h recall | DBI-07 | BMI, obesity | Obese people had higher DQD scores than people with normal weight. |
| Cheung et al., 2018 [30] | Cross-sectional | 211 (115 males and 96 females) | Adults with type 2 diabetes in Hong Kong, China, age 18–65 years | FFQ | AHEI-2010, DASH, DQI-I | BMI, obesity | AHEI-2010, but not DQI-I and DASH, had an inverse association with obesity (BMI ≥ 30 kg/m2). |
| Wang et al., 2018 [35] | Cross-sectional | 4440 (2062 males and 2378 females) | CHNS 2006, aged 18–65 years | 3-day 24-hr recall | tAHEI; cDGI | BMI, WC | A higher proportion of men had higher BMIs and WCs in the top quintile compared with the bottom quintile of tAHEI scores; no significant differences in BMI across the quintiles of CDGI, yet men in the top quintile had lower odds of abdominal obesity (WC ≥ 90cm) than the bottom quintile. |
| Whitton et al., 2018 [31] | Cross-sectional | 4617 (Chinese subgroup), 56% females | Singapore Multi-Ethnic Cohort study (MEC), mean age at 44 years | FFQ | aHEI-2010, aMED, DASH | BMI, WC | BMI was negatively associated with aHEI and DASH scores, but not aMED. |
| Zhang et al., 2018 [48] | Cross-sectional | 738 (336 males and 402 females) | Participants aged 50–77 years in the 2010–2012 National Nutrition and Health Survey in Yunnan province, southwest China | 3-day 24-h recall | DBI-07 | BMI, underweight | Underweight people had higher LBS and DQD scores. |
| Zhao et al., 2018 [51] | Cross-sectional | 1520 (527 males and 993 females); 2398 (52.1% females) | Primary dataset: Chinese Urban Adults Diet and Health Study (CUADHS); verification dataset:CHNS 2009 | FFQ and 24-h recall | HFD | BMI, WC | Higher HFD was associated with lower WC in the CHNS but not the CUADHS dataset; BMI was not associated with HFD for both datasets. |
| Chou et al., 2019 [33] | Longitudinal * | 436 (195 males and 231 females) | Community-dwelling elders (aged 65 years or older) in Taipei, China | FFQ | mAHEI | BMI | BMI at baseline did not differ between mAHEI tertiles. |
| Jia et al., 2020 [52] | Cross-sectional | 1320 (621 males and 699 females) | Working age (18–60 years) adults in Inner Mongolia, China | 3-day 24-h recall | DASH, aMED | BMI, WC, WC/BMI | aMed was inversely associated with WC, BMI, and WC-BMI, while DASH was only associated with WC. |
| Nguyen et al., 2020 [41] | Longitudinal * | 60,161 men and 72,445 women | the Shanghai Women’s Health Study (SWHS) and the Shanghai Men’s Health Study (SMHS) | FFQ | CHFP score | BMI | Baseline BMI did not differ among quartiles of CHFP among participants |
| Wang et al., 2020 [42] | Longitudinal * | 3450 females | 5-year breast cancer survivors aged 25–70 years from the Shanghai Breast Cancer Survival Study | FFQ | CHFP scores, modified DASH, and HEI-2015 | BMI | Participants within the highest quartile of CHFP-2007 were more likely to have lower BMI than those in the lowest quartile. |
| Zhou et al., 2020 [49] | Longitudinal * | 30,626 (52.8% females) | CHNS (2004, 2006, 2009, and 2011), aged 18–65 years | 3-day 24-hr recall | DQD (2) | BMI, Obesity | As BMI increased, the DQD increased; the normal weight group had lower DQD (2) scores than the obesity and overweight groups |
| Liu et al., 2021 [37] | Longitudinal | 6398 (53% females) | CHNS from 1997 to 2015 | 3-day 24-h recall | CHEI | BMI | Those who had a low score and remained low over time were less likely to have a normal BMI at baseline |
| Dietary Index | Reference Guidelines | Food Groups Included | Foods and Nutrients to Limit | Scoring System | Note |
|---|---|---|---|---|---|
| Internationally Used Scores | |||||
| HEI-05 [54] | DGA | Total fruit, whole fruit, total vegetables, dark green and orange vegetables and legumes, total grains, whole grains, milk, meat and beans, oils, | Saturated fat, sodium, and energy from solid fats, alcohol, and added sugars | Sum of score for each food component; scale 0–100 | The most updated version of HEI, HEI-2015 has some revisions on the components such as removing alcohol and including a restriction on refined grains. |
| AHEI [29] | Alternative to the HEI, based on foods and nutrients which can prevent chronic disease risks | Vegetables, fruit, nuts and soy, ratio of white to red meat, total fiber, ratio of polyunsaturated fatty acids (PUFA) to saturated fatty acids (SFA), multivitamin use | Trans fat, alcohol consumption | Sum of score for each food component; scale 0–100 | |
| DASH [55] | the DASH diet | Fruits, vegetables, nuts and seeds and legumes, low-fat dairy, and whole grains | Sodium, sweetened beverages, and red and processed meat | This score is cohort-specific, according to quintile rankings of participants. | |
| aMed [22] | the Mediterranean diet | Whole grains, vegetables, fruits, legumes, nuts, fish, ratio of monounsaturated fat (MUFA) to SFA | Red and processed meats, alcohol | This score is cohort-specific, according to the median intake of each component in the cohort (0 point for ≤ median and 1 point for > median); total score is the sum of each component score (total scale 0–9) | |
| Scores tailored to Chinese | |||||
| CHEI [23] | CHFP | Total grains, whole grains and mixed beans, tubers, total vegetables, dark vegetables, fruits, dairy, soybeans, fish and seafood, poultry, eggs, and seeds and nuts | Red meat, cooking oil, sodium, added sugar and alcohol | Sum of score for each food component; scale 0–100 | |
| CHFP [40] | CHFP | Grains, vegetables, fruits, dairy, beans, meat and poultry, fish and shrimp, eggs | Fats and oils, and salt | Sum of score for each food component; scale 0–100 | |
| China DQI [43] | DGC | Diet variety, total carbohydrate, fruit and vegetables, protein calcium, protein | Total fat, SFA, total energy, sodium, and alcoholic beverages | Sum of score for each food component | |
| DBI [45] | CHFP | Cereals, vegetables and fruits, dairy products, soybean and soybean products, animal food, dietary variety, drinking water | Condiments and alcoholic beverage | With both negative and positive scores indicating inadequacy and excessive intake for each food component, thus the total score converges at 0. | The DBI contains a set of scores: LBS assesses food groups consumption not meeting recommendations; HBS assesses those exceeding recommendations; DQD assesses imbalanced intakes (i.e. the absolute values of LBS + HBS) |
| DQD [49] | CHFP | Cereal and potatoes, fruits, vegetables, eggs, aquatic products, meat, and poultry, legumes, and nuts, milk, and milk products | This score sums up all the divergences for eight food categories | ||
| DDS [50] | Grains; vegetables; fruits; meat, poultry, and seafood; dairy; and beans, eggs, and nuts | Sum of score for each component; scale 0–6 | |||
| HFD [51] | Whole grains and legumes, tubers, other vegetables, vitamin A or C rich vegetables, fruits, dairy, soy products, nuts and seeds, aquatic products, refined grains, meat and poultry, eggs, oils | Salt, added sugar | Scoring is based on an algorithm. The total score ranges from 0 to 1 with 1 being more diverse. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadam, I.; Neupane, S.; Wei, J.; Fullington, L.A.; Li, T.; An, R.; Zhao, L.; Ellithorpe, A.; Jiang, X.; Wang, L. A Systematic Review of Diet Quality Index and Obesity among Chinese Adults. Nutrients 2021, 13, 3555. https://doi.org/10.3390/nu13103555
Kadam I, Neupane S, Wei J, Fullington LA, Li T, An R, Zhao L, Ellithorpe A, Jiang X, Wang L. A Systematic Review of Diet Quality Index and Obesity among Chinese Adults. Nutrients. 2021; 13(10):3555. https://doi.org/10.3390/nu13103555
Chicago/Turabian StyleKadam, Isma’il, Sudeep Neupane, Jingkai Wei, Lee Ann Fullington, Tricia Li, Ruopeng An, Li Zhao, Amy Ellithorpe, Xinyin Jiang, and Liang Wang. 2021. "A Systematic Review of Diet Quality Index and Obesity among Chinese Adults" Nutrients 13, no. 10: 3555. https://doi.org/10.3390/nu13103555
APA StyleKadam, I., Neupane, S., Wei, J., Fullington, L. A., Li, T., An, R., Zhao, L., Ellithorpe, A., Jiang, X., & Wang, L. (2021). A Systematic Review of Diet Quality Index and Obesity among Chinese Adults. Nutrients, 13(10), 3555. https://doi.org/10.3390/nu13103555