Quercetin Supplementation Improves Neuromuscular Function Recovery from Muscle Damage

 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
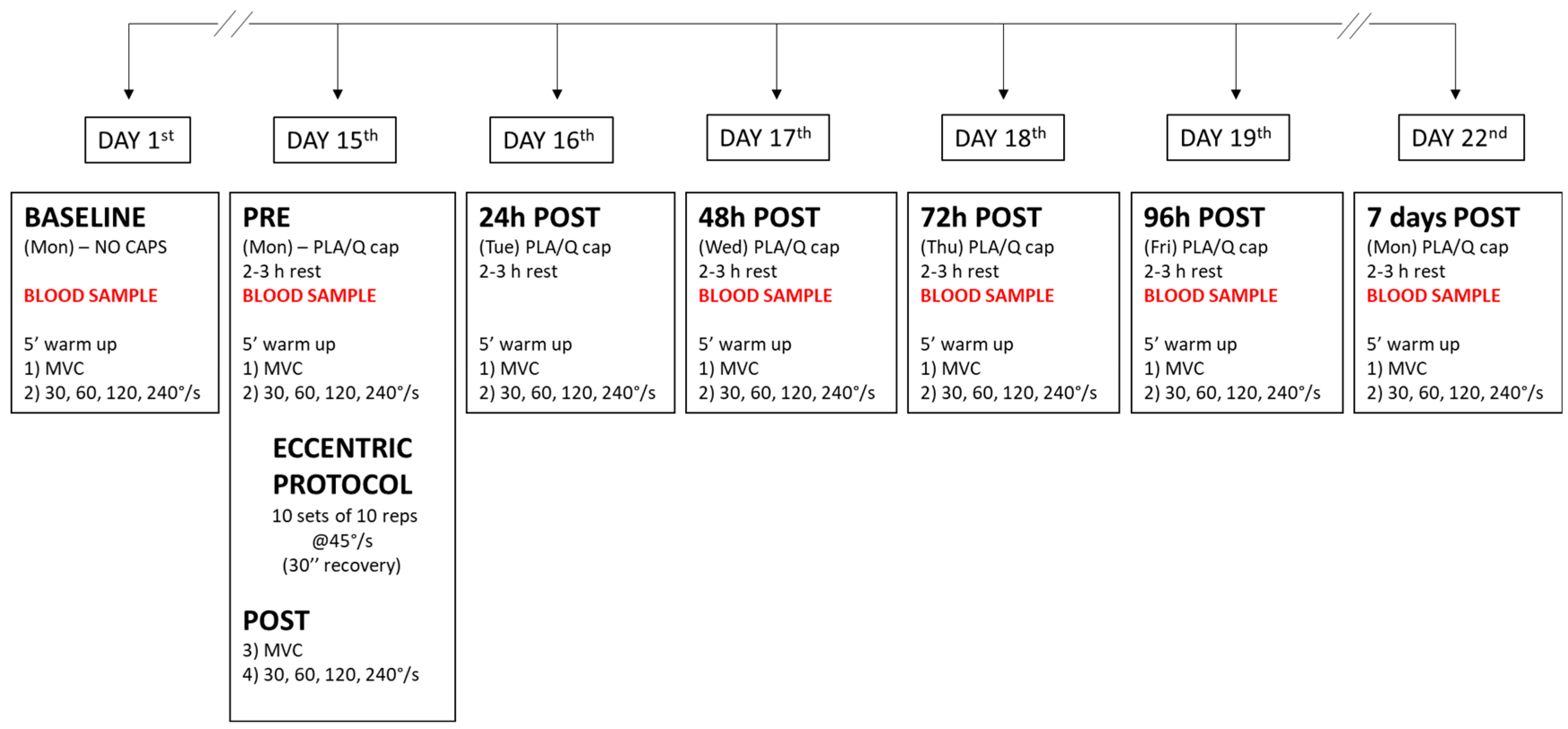
2.2. Research Design
2.3. Treatment
2.4. NM Evaluation
- (1)
- MVIC. The joint angle was fixed at 90° (0°, full extension). The MVIC task consisted of rapidly increasing the force exerted by elbow flexors to a maximum. All participants were verbally encouraged to exceed the target force, producing a maximal contraction “as hard as possible” and to maintain it for at least 2–3 s before relaxing. A minimum of 3 maximal attempts were performed separated by 5 min to recover from fatigue.
- (2)
2.5. Eccentric Protocol
2.6. Indices of EEIMD
2.7. EMG Data Analysis
2.8. Biochemical Analyses
2.9. Reliability
2.10. Statistical Analysis
3. Results
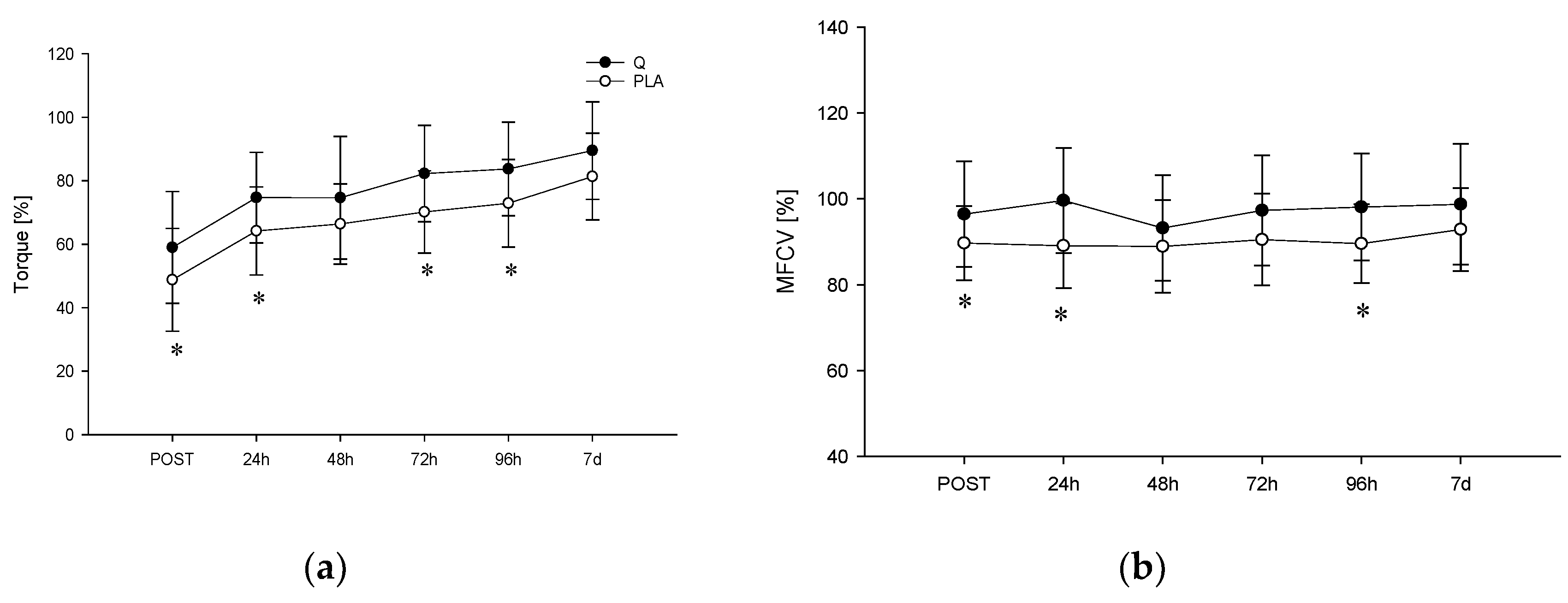
3.1. MVIC
3.2. FV Task
3.3. Other EEIMD Indices
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Proske, U.; Morgan, D.L. Muscle damage from eccentric exercise: Mechanism, mechanical signs, adaptations and clinical applications. J. Physiol. 2001, 537, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Hirose, L.; Nosaka, K.; Newton, M.; Laveder, A.; Kano, M.; Peake, J.; Suzuki, K. Changes in inflammatory mediators following eccentric exercise of the elbow flexors. Exerc. Immunol. Rev. 2004, 10, 75–90. [Google Scholar] [PubMed]
- Duranti, G.; Ceci, R.; Patrizio, F.; Sgrò, P.; Di Luigi, L.; Sabatini, S.; Felici, F.; Bazzucchi, I. Chronic consumption of quercetin reduces erythrocytes oxidative damage: Evaluation at resting and after eccentric exercise in humans. Nutr. Res. 2018, 50, 73–81. [Google Scholar] [PubMed]
- Bazzucchi, I.; Patrizio, F.; Ceci, R.; Duranti, G.; Sgrò, P.; Sabatini, S.; Di Luigi, L.; Sacchetti, M.; Felici, F. The effects of quercetin supplementation on eccentric exercise-induced muscle damage. Nutrients 2019, 11, 205. [Google Scholar] [CrossRef]
- Patrizio, F.; Ditroilo, M.; Felici, F.; Duranti, G.; De Vito, G.; Sabatini, S.; Sacchetti, M.; Bazzucchi, I. The acute effect of Quercetin on muscle performance following a single resistance training session. Eur. J. Appl. Physiol. 2018, 118, 1021–1031. [Google Scholar] [CrossRef]
- Hyldahl, R.D.; Hubal, M.J. Lengthening our perspective: Morphological, cellular, and molecular responses to eccentric exercise. Muscle Nerve 2014, 49, 155–170. [Google Scholar] [CrossRef]
- Sbriccoli, P.; Felici, F.; Rosponi, A.; Aliotta, A.; Castellano, V.; Mazzà, C.; Bernardi, M.; Marchetti, M. Exercise induced muscle damage and recovery assessed by means of linear and non-linear sEMG analysis and ultrasonography. J. Electromyogr. Kinesiol. 2001, 11, 73–83. [Google Scholar] [CrossRef]
- Konrad, M.; Nieman, D.C.; Henson, D.A.; Kennerly, K.M.; Jin, F.; Wallner-Liebmann, S.J. The acute effect of ingesting a quercetin-based supplement on exercise-induced inflammation and immune changes in runners. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 338–346. [Google Scholar] [CrossRef]
- O’Fallon, K.S.; Kaushik, D.; Michniak-Kohn, B.; Dunne, C.P.; Zambraski, E.J.; Clarkson, P.M. Effects of quercetin supplementation on markers of muscle damage and inflammation after eccentric exercise. Int. J. Sport Nutr. Exerc. Metab. 2012, 22, 430–437. [Google Scholar] [CrossRef]
- Menotti, F.; Bazzucchi, I.; Felici, F.; Damiani, A.; Gori, M.C.; Macaluso, A. Neuromuscular function after muscle fatigue in Charcot-Marie-Tooth type 1A patients. Muscle Nerve 2012, 46, 434–439. [Google Scholar]
- Felici, F.; Bazzucchi, I.; Sgrò, P.; Quinzi, F.; Conti, A.; Aversa, A.; Gizzi, L.; Mezzullo, M.; Romanelli, F.; Pasquali, R.; et al. Acute severe male hypo-testosteronemia affects central motor command in humans. J. Electromyogr. Kinesiol. 2016, 28, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Bazzucchi, I.; Felici, F.; Montini, M.; Figura, F.; Sacchetti, M. Caffeine improves neuromuscular function during maximal dynamic exercise. Muscle Nerve 2011, 43, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Bazzucchi, I.; Felici, F.; Sacchetti, M. Effect of Short-Term Creatine Supplementation on Neuromuscular Function. Med. Sci. Sport. Exerc. 2009, 41, 1934–1941. [Google Scholar] [CrossRef]
- Hübscher, M.; Tu, S.; Stanton, T.; Moseley, G.L.; Wand, B.M.; Booth, J.; McAuley, J.H. Movement restriction does not modulate sensory and perceptual effects of exercise-induced arm pain. Eur. J. Appl. Physiol. 2015, 115, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Nosaka, K.; Clarkson, P.M. Muscle damage following repeated bouts of high force eccentric exercise. Med. Sci. Sports Exerc. 1995, 27, 1263–1269. [Google Scholar] [CrossRef]
- Warren, G.L.; Lowe, D.A.; Armstrong, R.B. Measurement tools used in the study of eccentric contraction-induced injury. Sport. Med. 1999, 27, 43–59. [Google Scholar] [CrossRef]
- Owens, D.J.; Twist, C.; Cobley, J.N.; Howatson, G.; Close, G.L. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? Eur. J. Sport Sci. 2019, 19, 71–85. [Google Scholar] [CrossRef]
- Armstrong, R.B. Mechanisms of exercise-induced delayed onset muscular soreness: A brief review. Med. Sci. Sports Exerc. 1984, 16, 529–538. [Google Scholar] [CrossRef]
- Gissel, H. The role of Ca2+ in muscle cell damage. Ann. N. Y. Acad. Sci. 2006, 1066, 166–180. [Google Scholar] [CrossRef] [PubMed]
- Georganas, C.; Liu, H.; Perlman, H.; Hoffmann, A.; Thimmapaya, B.; Pope, R.M. Regulation of IL-6 and IL-8 Expression in Rheumatoid Arthritis Synovial Fibroblasts: The Dominant Role for NF-κB But Not C/EBPβ or c-Jun. J. Immunol. 2000, 165, 7199–7206. [Google Scholar] [CrossRef]
- Nguyen, H.X.; Tidball, J.G. Interactions between neutrophils and macrophages promote macrophage killing of rat muscle cells in vitro. J. Physiol. 2003, 547, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Di Meo, S.; Napolitano, G.; Venditti, P. Mediators of physical activity protection against ros-linked skeletal muscle damage. Int. J. Mol. Sci. 2019, 20, 3024. [Google Scholar]
- Sharifi-Rad, M.; Anil Kumar, N.V.; Zucca, P.; Varoni, E.M.; Dini, L.; Panzarini, E.; Rajkovic, J.; Tsouh Fokou, P.V.; Azzini, E.; Peluso, I.; et al. Lifestyle, Oxidative Stress, and Antioxidants: Back and Forth in the Pathophysiology of Chronic Diseases. Front. Physiol. 2020, 11, 649. [Google Scholar]
- Boots, A.W.; Wilms, L.C.; Swennen, E.L.R.; Kleinjans, J.C.S.; Bast, A.; Haenen, G.R. In vitro and ex vivo anti-inflammatory activity of quercetin in healthy volunteers. Nutrition 2008, 24, 704–710. [Google Scholar]
- Scholten, S.D.; Sergeev, I.N. Long-term quercetin supplementation reduces lipid peroxidation but does not improve performance in endurance runners. Open Access J. Sport. Med. 2013, 4, 53–61. [Google Scholar] [CrossRef]
- Çelik, N.; Vurmaz, A.; Kahraman, A. Protective effect of quercetin on homocysteine-induced oxidative stress. Nutrition 2017, 33, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Chen, X.; Li, J.; Li, Y.; Tang, Y.; Liu, L.; Chen, S.; Yu, H.; Yao, P. Myocardial mitochondrial oxidative stress and dysfunction in intense exercise: Regulatory effects of quercetin. Eur. J. Appl. Physiol. 2014, 114, 695–705. [Google Scholar]
- Salucci, S.; Falcieri, E. Polyphenols and their potential role in preventing skeletal muscle atrophy. Nutr. Res. 2020, 74, 10–22. [Google Scholar] [CrossRef]
- Phillips, T.; Childs, A.C.; Dreon, D.M.; Phinney, S.; Leeuwenburgh, C. A Dietary Supplement Attenuates IL-6 and CRP after Eccentric Exercise in Untrained Males. Med. Sci. Sports Exerc. 2003, 35, 2032–2037. [Google Scholar] [CrossRef]
- Nardone, A.; Romanò, C.; Schieppati, M. Selective recruitment of high-threshold human motor units during voluntary isotonic lengthening of active muscles. J. Physiol. 1989, 409, 451–471. [Google Scholar] [CrossRef]
- Quindry, J.; Miller, L.; McGinnis, G.; Irwin, M.; Dumke, C.; Magal, M.; Triplett, N.T.; McBride, J.; Urbiztondo, Z. Muscle-fiber type and blood oxidative stress after eccentric exercise. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Anderson, E.J.; Neufer, P.D. Type II skeletal myofibers possess unique properties that potentiate mitochondrial H2O2 generation. Am. J. Physiol. Cell Physiol. 2006, 290, C844–C851. [Google Scholar] [CrossRef] [PubMed]
- Alexander, S.P.H. Flavonoids as antagonists at A1 adenosine receptors. Phyther. Res. 2006, 20, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Konrad, M.; Nieman, D.C. Evaluation of Quercetin as a Countermeasure to Exercise-Induced Physiological Stress. Antioxid. Sport Nutr. 2014, 10, 155. [Google Scholar]
- Ganio, M.S.; Armstrong, L.E.; Johnson, E.C.; Klau, J.F.; Ballard, K.D.; Michniak-Kohn, B.; Kaushik, D.; Maresh, C.M. Effect of quercetin supplementation on maximal oxygen uptake in men and women. J. Sports Sci. 2010, 28, 201–208. [Google Scholar] [CrossRef]
- Davis, J.M.; Murphy, E.A.; Carmichael, M.D. Effects of the dietary flavonoid quercetin upon performance and health. Curr. Sports Med. Rep. 2009, 8, 206–213. [Google Scholar] [CrossRef]
- Manach, C.; Williamson, G.; Morand, C.; Scalbert, A.; Rémésy, C. Bioavailability and bioefficacy of polyphenols in humans. I. Review of 97 bioavailability studies. Am. J. Clin. Nutr. 2005, 81, 230S–242S. [Google Scholar] [CrossRef]
- Shi, Y.; Williamson, G. Quercetin lowers plasma uric acid in pre-hyperuricaemic males: A randomised, double-blinded, placebo-controlled, cross-over trial. Br. J. Nutr. 2016, 115, 800–806. [Google Scholar] [CrossRef]
- Egert, S.; Wolffram, S.; Bosy-Westphal, A.; Boesch-Saadatmandi, C.; Wagner, A.E.; Frank, J.; Rimbach, G.; Mueller, M.J. Daily quercetin supplementation dose-dependently increases plasma quercetin concentrations in healthy humans. J. Nutr. 2008, 138, 1615–1621. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MFCV (%) | |||||
|---|---|---|---|---|---|
| 30°/s | 60°/s | 120°/s | 240°/s | ||
| PRE | Q | 100.4 ± 5.3 | 101.5 ± 4.9 | 101.7 ± 5.1 | 102.5 ± 6.2 |
| PLA | 100.9 ± 7.4 | 101.0 ± 4.8 | 101.1 ± 4.6 | 101.2 ± 5.9 | |
| POST | Q | 97.1 ± 7.2 | 97.2 ± 8.0 | 97.2 ± 7.4 | 98.3 ± 7.4 |
| PLA | 96.2 ± 9.2 | 96.6 ± 7.3 | 90.2 ± 9.1 * | 87.8 ± 7.7 * | |
| 24 h | Q | 95.9 ± 9.5 | 96.0 ± 9.0 | 96.7 ± 8.0 | 97.2 ± 8.1 |
| PLA | 96.2 ± 5.4 | 97.2 ± 5.7 | 89.8 ± 7.7 * | 86.6 ± 8.5 * | |
| 48 h | Q | 98.2 ± 9.9 | 98.9 ± 8.1 | 98.8 ± 7.5 | 99.1 ± 7.8 |
| PLA | 97.6 ± 6.1 | 97.6 ± 4.4 | 91.8 ± 5.0 * | 89.1 ± 7.9 * | |
| 72 h | Q | 99.5 ± 7.8 | 100.0 ± 7.3 | 99.8 ± 6.3 | 100.9 ± 6.6 |
| PLA | 98.6 ± 3.6 | 97.2 ± 4.3 | 91.4 ± 5.3 | 87.4 ± 6.0 * | |
| 96 h | Q | 99.6 ± 7.1 | 100.2 ± 6.6 | 100.7 ± 5.4 | 100.6 ± 5.5 |
| PLA | 97.0 ± 4.8 | 97.6 ± 4.1 | 92.3 ± 4.8 * | 88.7 ± 6.4 * | |
| 7 d | Q | 100.7 ± 7.8 | 101.2 ± 6.4 | 101.1 ± 5.9 | 102.0 ± 6.2 |
| PLA | 99.3 ± 4.6 | 100.2 ± 3.4 | 93.6 ± 4.4 * | 90.8 ± 5.9 * | |
| Arm Circumference | VAS | Elbow Angle | ||
|---|---|---|---|---|
| cm | cm | degrees | ||
| BASELINE | Q | 31.1 ± 0.7 | 0 | 175.3 ± 5.0 |
| PLA | 30.6 ± 0.7 | 0 | 175.0 ± 6.3 | |
| PRE | Q | 31.1 ± 0.7 | 0 | 174.3 ± 5.1 |
| PLA | 30.7 ± 0.8 | 0 | 175.6 ± 7.3 | |
| POST | Q | 32.2 ± 0.7 | 0.4 ± 0.2 | 164.7 ± 6.9 |
| PLA | 32.2 ± 0.8 | 1.2 ± 0.4 | 158.8 ± 14.4 * | |
| 24 h | Q | 31.7 ± 0.6 | 1.7 ± 0.3 | 163.1 ± 8.5 |
| PLA | 31.7 ± 0.8 | 2.8 ± 0.5 | 158.8 ± 13.2 | |
| 48 h | Q | 31.7 ± 0.7 | 2.8 ± 0.5 | 158.1 ± 9.8 |
| PLA | 31.6 ± 0.8 | 3.0 ± 0.5 | 159.1 ± 12.8 | |
| 72 h | Q | 31.4 ± 0.7 | 2.5 ± 0.6 | 160.0 ± 12.1 |
| PLA | 32.0 ± 0.8 | 3.3 ± 0.6 | 155.9 ± 15.6 | |
| 96 h | Q | 31.7 ± 0.7 | 2.8 ± 0.5 | 164.4 ± 11.8 |
| PLA | 31.6 ± 0.8 | 3.0 ± 0.5 | 157.8 ± 12.9 | |
| 7 d | Q | 31.4 ± 0.7 | 2.5 ± 0.6 | 169.7 ± 9.7 |
| PLA | 32.0 ± 0.8 | 3.3 ± 0.6 | 168.1 ± 13.3 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazzucchi, I.; Patrizio, F.; Ceci, R.; Duranti, G.; Sabatini, S.; Sgrò, P.; Di Luigi, L.; Sacchetti, M. Quercetin Supplementation Improves Neuromuscular Function Recovery from Muscle Damage. Nutrients 2020, 12, 2850. https://doi.org/10.3390/nu12092850
Bazzucchi I, Patrizio F, Ceci R, Duranti G, Sabatini S, Sgrò P, Di Luigi L, Sacchetti M. Quercetin Supplementation Improves Neuromuscular Function Recovery from Muscle Damage. Nutrients. 2020; 12(9):2850. https://doi.org/10.3390/nu12092850
Chicago/Turabian StyleBazzucchi, Ilenia, Federica Patrizio, Roberta Ceci, Guglielmo Duranti, Stefania Sabatini, Paolo Sgrò, Luigi Di Luigi, and Massimo Sacchetti. 2020. "Quercetin Supplementation Improves Neuromuscular Function Recovery from Muscle Damage" Nutrients 12, no. 9: 2850. https://doi.org/10.3390/nu12092850
APA StyleBazzucchi, I., Patrizio, F., Ceci, R., Duranti, G., Sabatini, S., Sgrò, P., Di Luigi, L., & Sacchetti, M. (2020). Quercetin Supplementation Improves Neuromuscular Function Recovery from Muscle Damage. Nutrients, 12(9), 2850. https://doi.org/10.3390/nu12092850