Drinking Refined Deep-Sea Water Improves the Gut Ecosystem with Beneficial Effects on Intestinal Health in Humans: A Randomized Double-Blind Controlled Trial

Abstract
1. Introduction
2. Materials and Methods
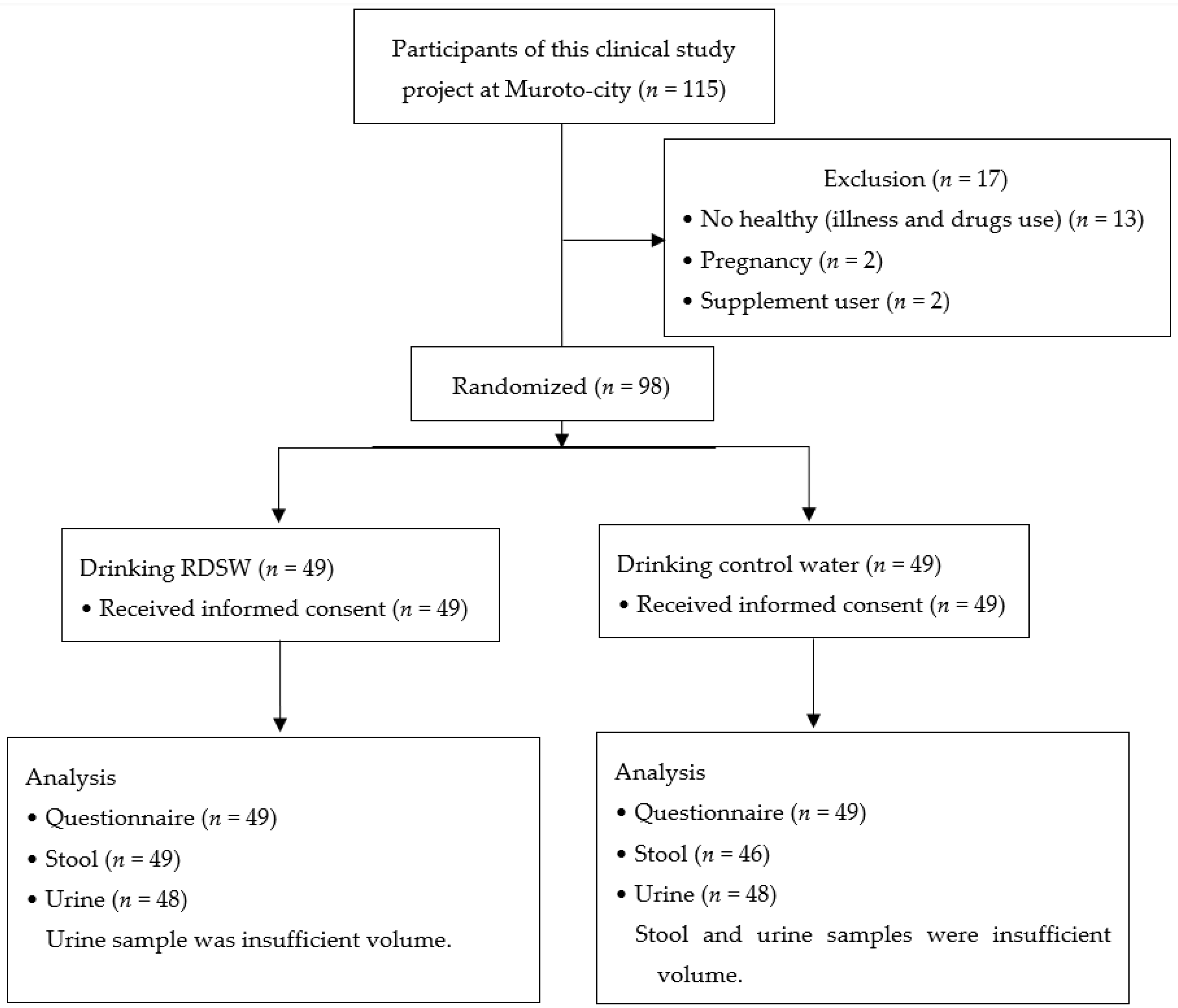
2.1. Clinical Study Design
2.2. Subjects
2.3. Ingestion Schedule
2.4. Evaluation
Self-Administered Questionnaire
2.5. Measurement of Samples
2.5.1. Measurement of Fecal sIgA
2.5.2. Measurement of Fecal Putrefactive Products
2.5.3. Measurement of Urinary Isoflavones
2.6. Statistical Analysis
3. Results
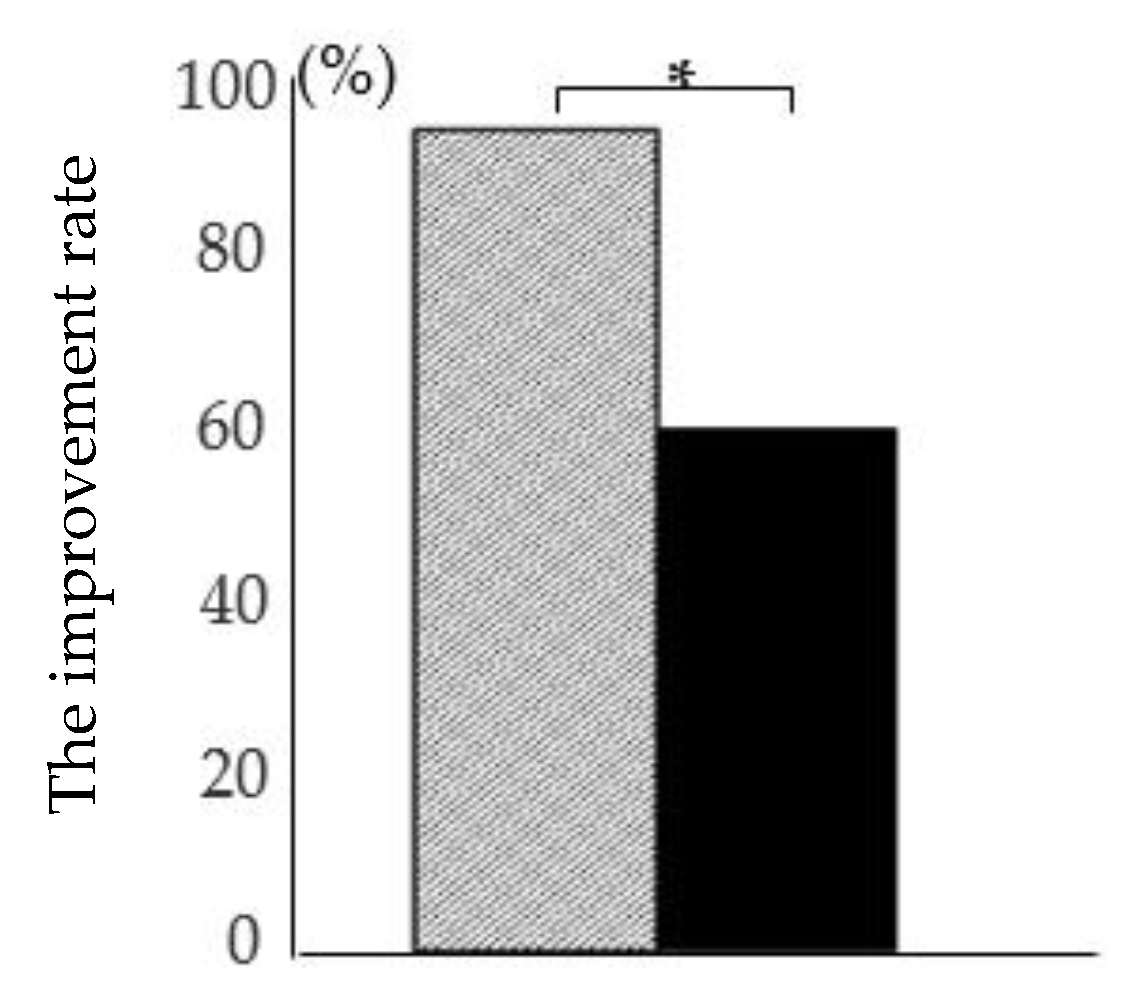
3.1. Self-Administered Questionnaire
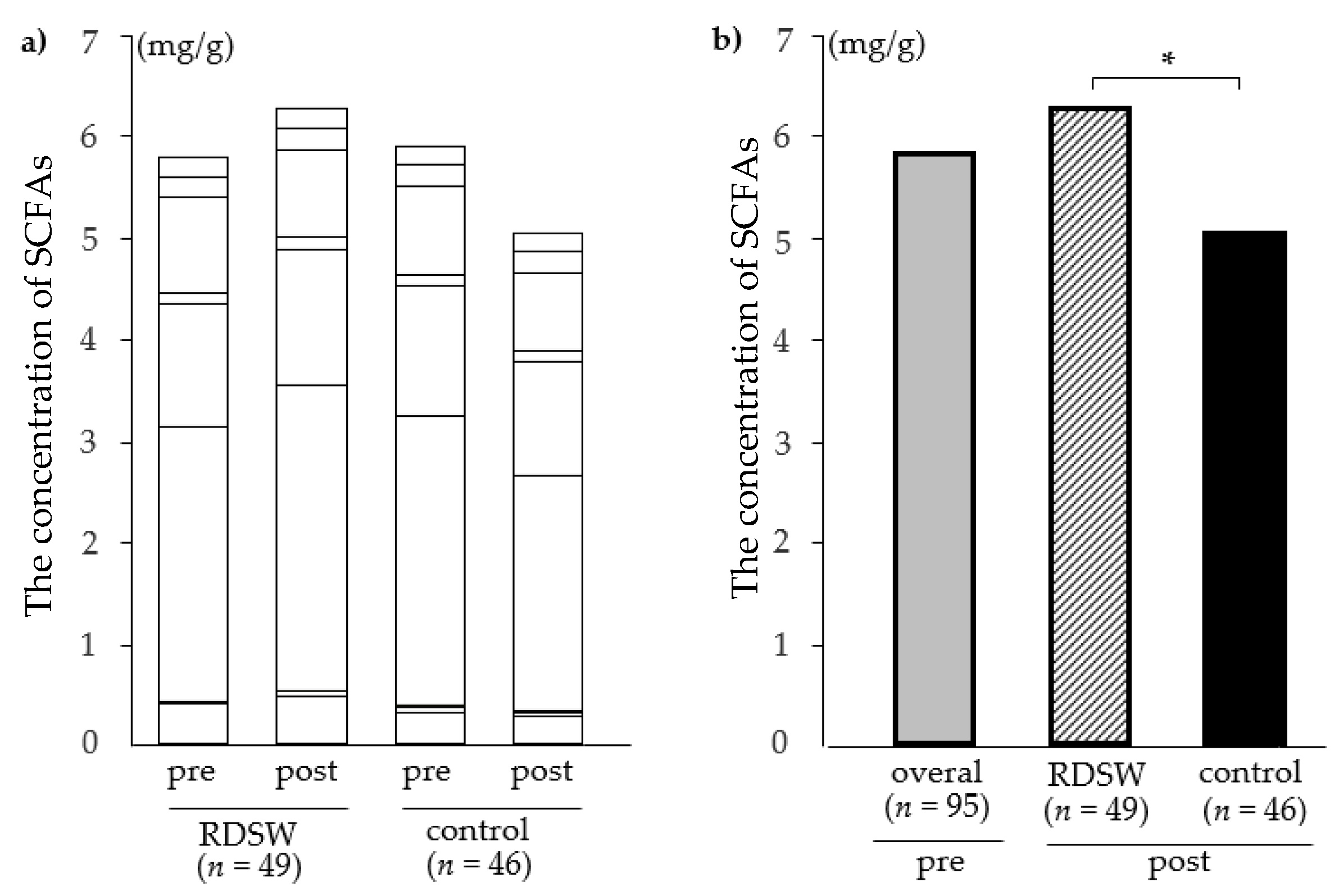
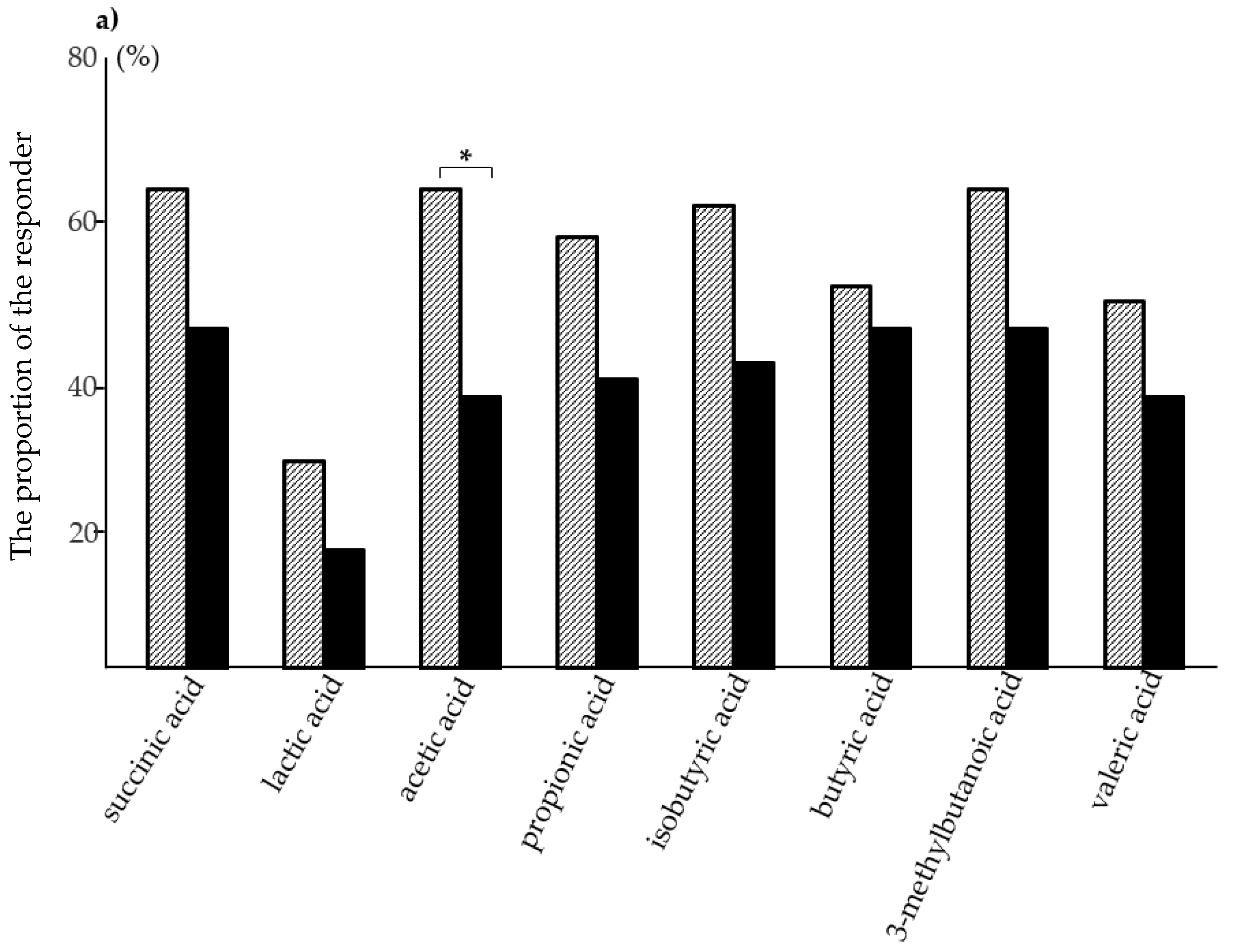
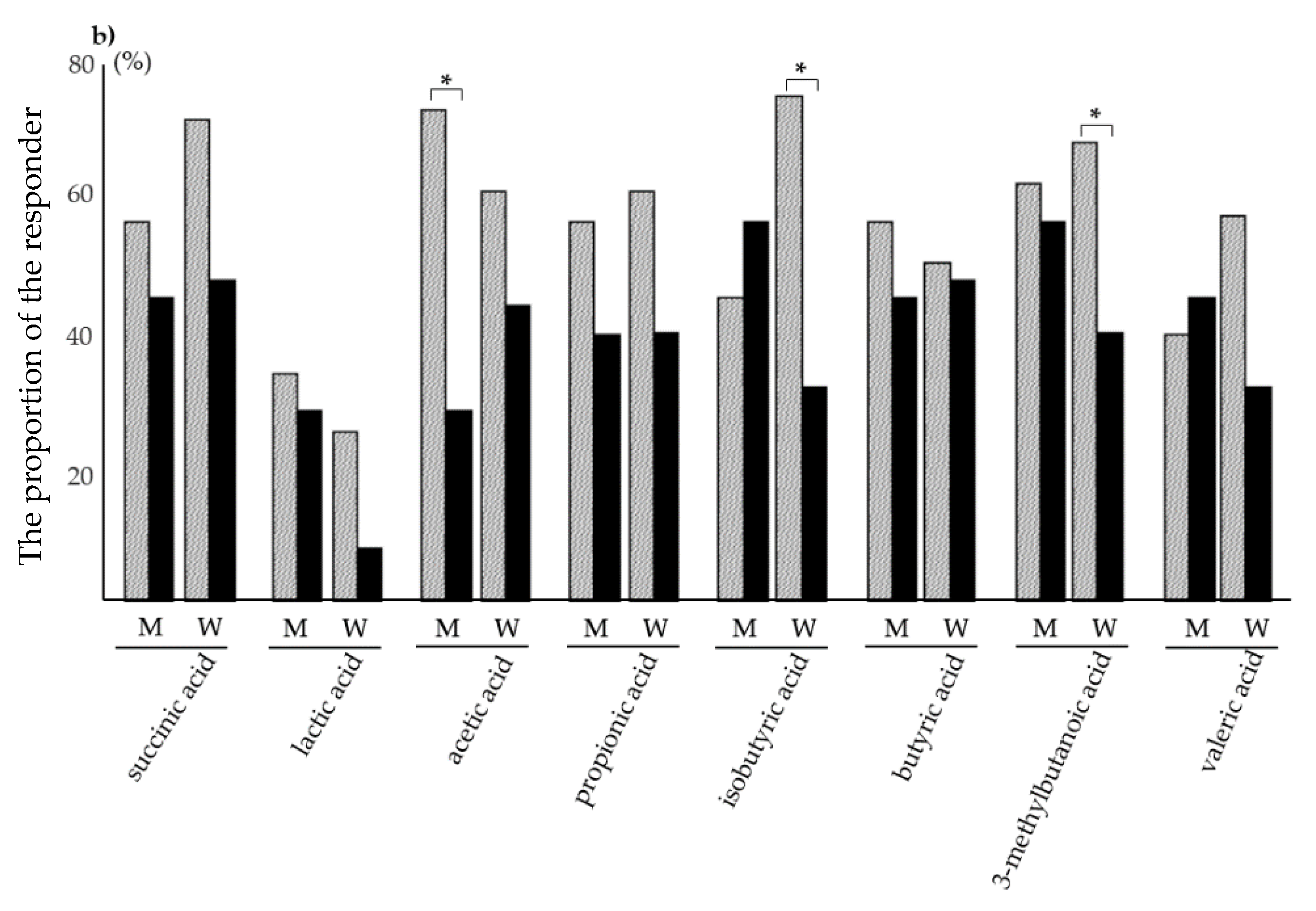
3.2. Analysis of Fecal sIgA, Putrefactive Products, and SCFAs
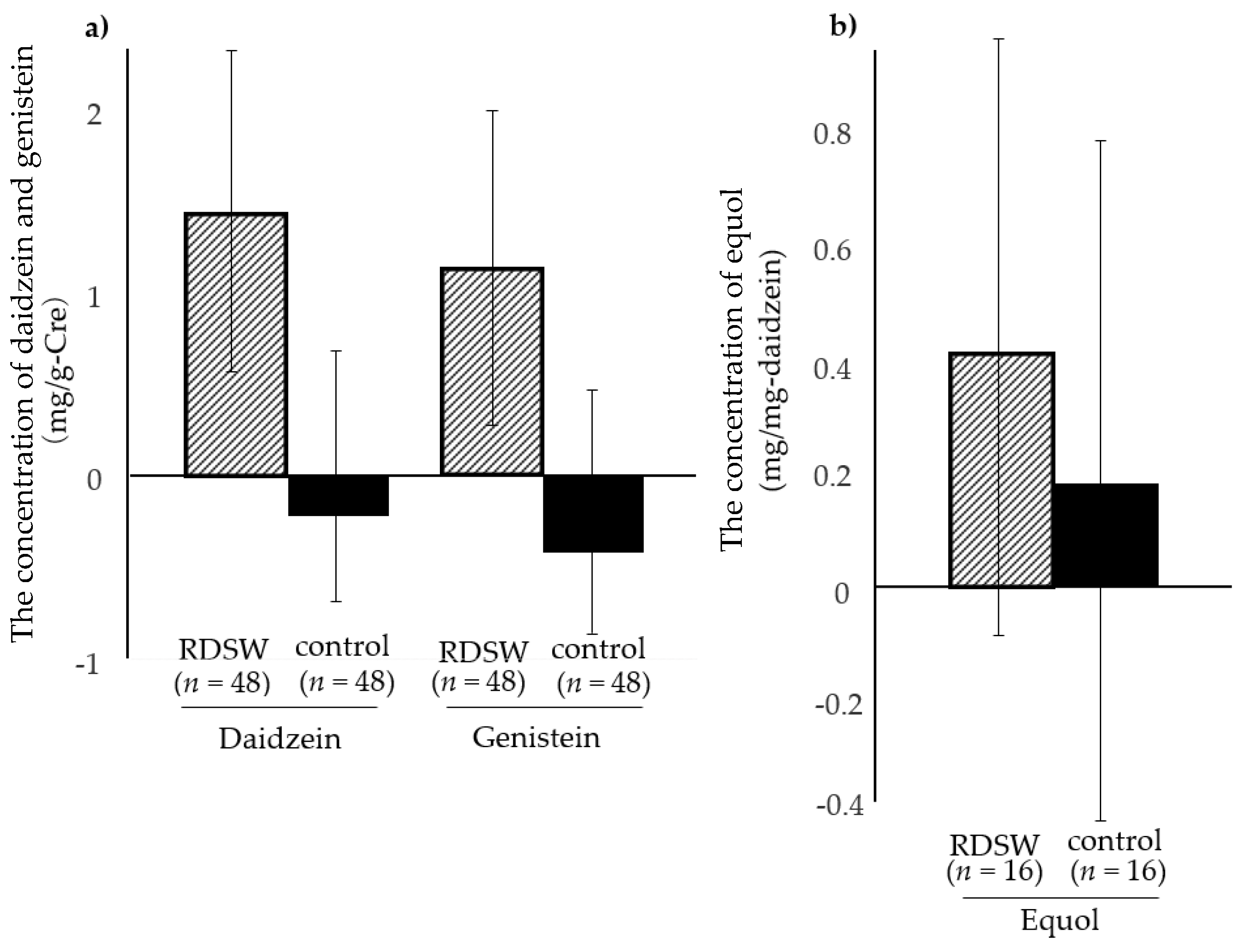
3.3. Analysis of Urinary Isoflavones
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nani, S.Z.M.; Majid, F.A.A.; Jaafar, A.B.; Mahdzir, A.; Musa, M.N. Potential Health Benefits of Deep Sea Water: A Review. Evid. Based Complement. Altern. Med. 2016. [Google Scholar] [CrossRef]
- Yoshioka, S.; Hamada, A.; Cui, T.; Yokota, J.; Yamamoto, S.; Kusunose, M.; Miyamura, M.; Kyotani, S.; Kaneda, R.; Tsutsumi, Y.; et al. Pharmacological Activity of Deep-Sea Water: Examination of Hyperlipemia Prevention and Medical Treatment Effect. Biol. Pharm. Bull. 2003, 26, 1552–1559. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Hao, J.; Peng, W.; Qiu, P.; Li, C.; Guan, H. Modulation of Lipid Metabolism by Deep-Sea Water in Cultured Human Liver (HepG2) Cells. Mar. Biotechnol. 2014, 16, 219–229. [Google Scholar] [CrossRef]
- Ha, B.G.; Park, J.E.; Shin, E.J.; Shon, Y.H. Effects of Balanced Deep-Sea Water on Adipocyte Hypertrophy and Liver Steatosis in High-Fat, Diet-Induced Obese Mice. Obesity 2014, 22, 1669–1678. [Google Scholar] [CrossRef]
- Katsuda, S.; Yasukawa, T.; Nakagawa, K.; Miyake, M.; Yamasaki, M.; Katahira, K.; Mohri, M.; Shimizu, T.; Hazama, A. Deep-Sea Water Improves Cardiovascular Hemodynamics in Kurosawa and Kusanagi-Hypercholesterolemic (KHC) Rabbits. Biol. Pharm. Bull. 2008, 31, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.S.; Kim, H.A.; Lee, S.H.; Yun, J.W. Anti-obesity and Antidiabetic Effects of Deep Sea Water on ob/ob Mice. Mar. Biotechnol. 2009, 11, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Ha, B.G.; Shin, E.J.; Park, J.E.; Shon, Y.H. Anti-Diabetic Effect of Balanced Deep-Sea Water and Its Mode of Action in High-Fat Diet Induced Diabetic Mice. Mar. Drugs 2013, 11, 4193–4212. [Google Scholar] [CrossRef]
- Yang, C.C.; Yao, C.A.; Lin, Y.R.; Yang, J.C.; Chien, C.T. Deep-Sea Water Containing Selenium Provides Intestinal Protection against Duodenal Ulcers through the Upregulation of Bcl-2 and Thioredoxin Reductase 1. PLoS ONE 2014, 9, e96006. [Google Scholar] [CrossRef]
- Nagai, N.; Ito, Y.; Inomata, M.; Shumiya, S.; Tai, H.; Hataguchi, Y.; Nakagawa, K. Delay of Cataract Development in the Shumiya Cataract Rat by the Administration of Drinking Water Containing High Concentration of Magnesium Ion. Biol. Pharm. Bull. 2006, 29, 1234–1238. [Google Scholar] [CrossRef][Green Version]
- Nagai, N.; Ito, Y. Delay of cataract development in the Shumiya cataract rat by water containing enhanced concentrations of magnesium and calcium. Curr. Eye Res. 2007, 32, 439–445. [Google Scholar] [CrossRef]
- Tai, H.; Watanabe, Y.; Nakagawa, K.; Nozaki, Y.; Kikuchi, Y. Effect of Deep Sea Water on Blood Rheological Properties. Hemorheol. Relat. Res. 1999, 2, 43–47. [Google Scholar]
- Tai, H.; Nakagawa, K.; Watanabe, Y.; Yokoyama, Y.; Nakajima, H.; Ikegami, Y.; Nozaki, Y.; Kikuchi, Y. Effect of long-term drinking of high mineral water prepared from deep sea water on hemorheology and blood pressure. Hemorheol. Relat. Res. 2001, 4, 21–25. [Google Scholar]
- Kimata, H.; Tai, H.; Nakajima, H. Reduction of allergic skin responses and serum allergen-specific IgE and IgE-inducing cytokines by drinking deep-sea water in patients with allergic Rhinitis. Otorhinolaryngol. Nova 2001, 11, 302–303. [Google Scholar] [CrossRef]
- Kimata, H.; Tai, H.; Nakagawa, K.; Yokoyama, Y.; Nakajima, H.; Ikegami, Y. Improvement of skin symptoms and mineral imbalance by drinking deep sea water in patients with atopic eczema/dermatitis syndrome (AEDS). Acta Med. 2002, 45, 83–84. [Google Scholar] [CrossRef]
- Hataguchi, Y.; Tai, H.; Nakajima, H.; Kimata, H. Drinking deep-sea water restores mineral imbalance in atopic eczema/dermatitis syndrome. Eur. J. Clin. Nutr. 2005, 59, 1093–1096. [Google Scholar] [CrossRef]
- Kawada, M.; Takeuchi, H.; Con, S.A.; Yamamoto, E.; Yasukawa, T.; Nakagawa, K.; Ikegami, Y.; Sugiura, T. Antibacterial activity of refined deep seawater on Helicobacter pylori. J. Med. Microbiol. Diagn. 2012, S1. [Google Scholar] [CrossRef]
- Takeuchi, H.; Trang, V.T.; Morimoto, N.; Nishida, Y.; Matsumura, Y.; Sugiura, T. Natural products and food components with anti-Helicobacter pylori activities. World J. Gastroenterol. 2014, 20, 8971–8978. [Google Scholar] [CrossRef]
- Izuoka, T.; Toyama, M.; Higuchi, T.; Kobayashi, K.; Mitsui, H.; Yamagata, K.; Nishitani, M.; Fukuda, M. Postmarketing functional food survey–efficacy and safety of magnesium containing mineral water for patients with constipation. J. Jpn. Physicians Assoc. 2009, 24, 102–107. [Google Scholar]
- Clemente, J.C.; Ursell, L.K.; Parfrey, L.W.; Knight, R. The Impact of the Gut Microbiota on Human Health: An Integrative View. Cell 2012, 148, 1258–1270. [Google Scholar] [CrossRef]
- Donovan, S.M. Introduction to the special focus issue on the impact of diet on gut microbiota composition and function and future opportunities for nutritional modulation of the gut microbiome to improve human health. Gut Microbes 2017, 8, 75–81. [Google Scholar] [CrossRef]
- Clark, A.; Mach, N. Exercise-induced stress behavior, gut-microbiota-brain axis and diet: A systematic review for athletes. J. Int. Soc. Sports Nutr. 2016, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Galland, L. The Gut Microbiome and the Brain. J. Med. Food 2014, 17, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Rea, K.; O’Mahony, S.M.; Dinan, T.G.; Cryan, J.F. The Role of the Gastrointestinal Microbiota in Visceral Pain. Handb. Exp. Pharmacol. 2017, 239, 269–287. [Google Scholar]
- Eiseman, B.; Silen, W.; Bascom, G.S.; Kauvar, A.J. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery 1958, 44, 854–859. [Google Scholar]
- Van Nood, E.; Vrieze, A.; Nieuwdorp, M.; Fuentes, S.; Zoetendal, E.G.; de Vos, W.M.; Visser, C.E.; Kuijper, E.J.; Bartelsman, J.F.; Tijssen, J.G.; et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N. Engl. J. Med. 2013, 368, 407–415. [Google Scholar] [CrossRef]
- Rossen, N.G.; MacDonald, J.K.; de Vries, E.M.; D’Haens, G.R.; de Vos, W.M.; Zoetendal, E.G.; Ponsioen, C.Y. Fecal microbiota transplantation as novel therapy in gastroenterology: A systematic review. World J. Gastroenterol. 2015, 2, 5359–5371. [Google Scholar] [CrossRef]
- Liu, C.; Cheng, L.; Ji, L.; Li, F.; Zhan, Y.; Wu, B.; Ke, Y.; Chen, P.; Hua, F.; Yuan, L.; et al. Intestinal microbiota dysbiosis play a role in pathogenesis of patients with primary immune thrombocytopenia. Thromb. Res. 2020, 190, 11–19. [Google Scholar] [CrossRef]
- Chauhan, A.; Kumar, R.; Sharma, S.; Mahanta, M.; Vayuuru, S.K.; Nayak, B.; Kumar, S.; Shalimar. Fecal Microbiota Transplantation in Hepatitis B e Antigen-Positive Chronic Hepatitis B Patients: A Pilot Study. Dig. Dis. Sci. 2020. [Google Scholar] [CrossRef]
- Vrieze, A.; Van Nood, E.; Holleman, F.; Salojärvi, J.; Kootte, R.S.; Bartelsman, J.F.; Dallinga-Thie, G.M.; Ackermans, M.T.; Serlie, M.J.; Oozeer, R.; et al. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology 2012, 143, 913–916. [Google Scholar] [CrossRef]
- Fond, G.B.; Lagier, J.C.; Honore, S.; Lancon, C.; Korchia, T.; Verville, P.S.; Llorca, P.M.; Auquier, P.; Guedj, E.; Boyer, L. Microbiota-Orientated Treatments for Major Depression and Schizophrenia. Nutrients 2020, 12, 1024. [Google Scholar] [CrossRef] [PubMed]
- Charlotte, A.; Frankenfeld, C.L.; Lampe, J.W. Gut bacterial metabolism of the soy isoflavone daidzein: Exploring the relevance to human health. Exp. Biol. Med. 2005, 230, 155–170. [Google Scholar] [CrossRef]
- Takahashi, S.; Tomita, J.; Nishioka, K.; Hisada, T.; Nishijima, M. Development of a Prokaryotic Universal Primer for Simultaneous Analysis of Bacteria and Archaea Using Next-Generation Sequencing. PLoS ONE 2014, 9, e105592. [Google Scholar] [CrossRef] [PubMed]
- Unno, T.; Hisada, T.; Takahashi, S. Hesperetin Modifies the Composition of Fecal Microbiota and Increases Cecal Levels of Short-Chain Fatty Acids in Rats. J. Agric. Food Chem. 2015, 63, 7952–7957. [Google Scholar] [CrossRef]
- Thompson, W.G.; Longstreth, G.F.; Drossman, D.A.; Heaton, K.W.; Irvine, E.J.; Müller-Lissner, S.A. Functional bowel disorders and functional abdominal pain. Gut 1999, 45 (Suppl. S2), II43–II47. [Google Scholar] [CrossRef]
- Ueno, T.; Abiru, Y.; Uchiyama, S.; Ishimi, Y. Distribution of 24-h urinary equol excretion as an indicator of the physiological range in healthy Japanese equol excretors. J. Funct. Foods 2014, 7, 129–135. [Google Scholar] [CrossRef]
- Kudo, H.; Takeuchi, H.; Shimamura, T.; Kadota, Y.; Sugiura, T.; Ukeda, H. In vitro anti-Helicobacter pylori activity of Chinese chive (Allium tuberosum). Food Sci. Technol. Res. 2011, 17, 505–513. [Google Scholar] [CrossRef]
- Takeuchi, H.; Shimamura, T.; Kudo, H.; Ukeda, H.; Sugiura, T. Antimicrobial activity of natural products and food components. In Current Research in Agriculture & Food Chemistry; Sunitha, M., Ed.; Research Media: Kerala, India, 2012; Volume 1, pp. 1–12. [Google Scholar]
- Den Besten, G.; van Eunen, K.; Groen, A.K.; Venema, K.; Reijngoud, D.J.; Bakker, B.M. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J. Lipid Res. 2013, 54, 2325–2340. [Google Scholar] [CrossRef]
- Hijova, E.; Chemelarova, A. Short chain fatty acids and colonic health. Bratisl. Lek. Listy 2007, 108, 354–358. [Google Scholar]
- Binder, H.J. Role of colonic short-chain fatty acid transport in diarrhea. Annu. Rev. Physiol. 2010, 72, 297–313. [Google Scholar] [CrossRef]
- Fukuda, S.; Toh, H.; Hase, K.; Oshima, K.; Nakanishi, Y.; Yoshimura, K.; Tobe, T.; Clarke, J.M.; Topping, D.L.; Suzuki, T.; et al. Bifidobacteria can protect from enteropathogenic infection through production of acetate. Nature 2011, 469, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Chambers, E.S.; Viardot, A.; Psichas, A.; Morrison, D.J.; Murphy, K.G.; Zac-Varghese, S.E.; MacDougall, K.; Preston, T.; Tedford, C.; Finlayson, G.S.; et al. Effects of targeted delivery of propionate to the human colon on appetite regulation, body weight maintenance and adiposity in overweight adults. Gut 2015, 64, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- Maslowski, K.M.; Vieira, A.T.; Ng, A.; Kranich, J.; Sierro, F.; Yu, D.; Schilter, H.C.; Rolph, M.S.; Mackay, F.; Artis, D.; et al. Regulation of inflammatory responses by gut microbiota and chemoattractant receptor GPR43. Nature 2009, 461, 1282–6128. [Google Scholar] [CrossRef]
- Sampson, T.R.; Debelius, J.W.; Thron, T.; Janssen, S.; Shastri, G.G.; Ilhan, Z.E.; Challis, C.; Schretter, C.E.; Rocha, S.; Gradinaru, V.; et al. Gut microbiota regulate motor deficits and neuroinflammation in a model of Parkinson’s disease. Cell 2016, 167, 1469–1480. [Google Scholar] [CrossRef] [PubMed]
- Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Otani, T.; Inoue, M.; Tsugane, S. Soy product and isoflavone consumption in relation to prostate cancer in Japanese men. Cancer Epidemiol. Biomark. Prev. 2007, 16, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Bersaglieri, T.; Sabeti, P.C.; Patterson, N.; Vanderploeg, T.; Schaffner, S.F.; Drake, J.A.; Rhodes, M.; Reich, D.E.; Hirschhorn, J.N. Genetic Signatures of Strong Recent Positive Selection at the Lactase Gene. Am. J. Hum. Genet. 2004, 74, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Tse, G.; Eslick, G.D. Soy and isoflavone consumption and risk of gastrointestinal cancer: A systematic review and meta-analysis. Eur. J. Nutr. 2016, 55, 63–73. [Google Scholar] [CrossRef]
- Zhang, Q.; Feng, H.; Qluwakemi, B.; Wang, J.; Yao, S.; Cheng, G.; Xu, H.; Qiu, H.; Zhu, L.; Yuan, M. Phytoestrogens and risk of prostate cancer: An updated meta-analysis of epidemiologic studies. Int. J. Food Sci. Nutr. 2017, 68, 28–42. [Google Scholar] [CrossRef]
- Hua, X.; Yu, L.; You, R.; Yang, Y.; Liao, J.; Chen, D.; Yu, L. Association among Dietary Flavonoids, Flavonoid Subclasses and Ovarian Cancer Risk: A Meta-Analysis. PLoS ONE 2016, 11, e0151134. [Google Scholar] [CrossRef]
- Jiang, R.; Botma, A.; Rudolph, A.; Hüsing, A.; Chang-Claude, J. Phyto-oestrogens and colorectal cancer risk: A systematic review and dose–response meta-analysis of observational studies. Br. J. Nutr. 2016, 116, 2115–2128. [Google Scholar] [CrossRef]
- Wei, P.; Liu, M.; Chen, Y.; Chen, D.C. Systematic review of soy isoflavone supplements on osteoporosis in women. Asian Pac. J. Trop. Med. 2012, 5, 243–248. [Google Scholar] [CrossRef]
- Li, L.; Xu, L.; Wu, J.; Dong, L.; Zhao, S.; Zheng, Q. Comparative efficacy of nonhormonal drugs on menopausal hot flashes. Eur. J. Clin. Pharmacol. 2016, 72, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.N.; Lin, C.C.; Liu, C.F. Efficacy of phytoestrogens for menopausal symptoms: A meta-analysis and systematic review. Climacteric 2015, 18, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Tokede, O.; Onabanjo, T.A.; Yansane, A.; Gaziano, J.M.; Djoussé, L. Soya products and serum lipids: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2015, 114, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Frankenfeld, C.L. Cardiometabolic risk and gut microbial phytoestrogen metabolite phenotypes. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef]
- Paul, B.; Royston, K.J.; Li, Y.; Stoll, M.L.; Skibola, C.F.; Wilson, L.S.; Barnes, S.; Morrow, C.D.; Tollefsbol, T.O. Impact of genistein on the gut microbiome of humanized mice and its role in breast tumor inhibition. PLoS ONE 2017, 12, e0189756. [Google Scholar] [CrossRef]
- Iino, C.; Shimoyama, T.; Iino, K.; Yokoyama, Y.; Chinda, D.; Sakuraba, H.; Fukuda, S.; Nakaji, S. Daidzein Intake Is Associated with Equol Producing Status through an Increase in the Intestinal Bacteria Responsible for Equol Production. Nutrients 2019, 11, 433. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Nakajima-Shimada, J.; Onizuka, Y.; Kishi, M.; Ueno, T.; Uchiyama, S. Optimal cut-off value for equol-producing status in women: The Japan Nurses’ Health Study urinary isoflavone concentration survey. PLoS ONE 2018, 13, e0201318. [Google Scholar] [CrossRef]
- Akaza, H.; Miyanaga, N.; Takashima, N.; Naito, S.; Hirao, Y.; Tsukamoto, T.; Fujioka, T.; Mori, M.; Kim, W.J.; Song, J.M.; et al. Comparisons of percent equol producers between prostate cancer patients and controls: Case-controlled studies of isoflavones in Japanese, Korean and American residents. Jpn. J. Clin. Oncol. 2004, 34, 86–89. [Google Scholar] [CrossRef]
- Védrine, N.; Mathey, J.; Morand, C.; Brandolini, M.; Davicco, M.J.; Guy, L.; Rémésy, C.; Coxam, V.; Manach, C. One-month exposure to soy isoflavones did not induce the ability to produce equol in postmenopausal women. Eur. J. Clin. Nutr. 2006, 60, 1039–1045. [Google Scholar] [CrossRef]
- Mathey, J.; Lamothe, V.; Coxam, V.; Potier, M.; Sauvant, P.; Bennetau-Pelissero, C. Concentrations of isoflavones in plasma and urine of post-menopausal women chronically ingesting high quantities of soy isoflavones. J. Pharm. Biomed. Anal. 2006, 41, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.F.; Tsai, H.S.; Lin, S.M.; Liu, C.D.; Learn, S.P.; Chiou, R.Y. GC-MS determined distribution of urinary equol producers as affected by age, gender, and repeated ingestions of soymilk. J. Food Sci. 2010, 75, H306–H310. [Google Scholar] [CrossRef] [PubMed]
- Franke, A.A.; Lai, J.F.; Pagano, I.; Morimoto, Y.; Maskarinec, G. Equol production changes over time in pre-menopausal women. Br. J. Nutr. 2012, 107, 1201–1206. [Google Scholar] [CrossRef] [PubMed]
- Izumi, T.; Piskula, M.K.; Osawa, S.; Obata, A.; Tobe, K.; Saito, M.; Kataoka, S.; Kubota, Y.; Kikuchi, M. Soy Isoflavone Aglycones Are Absorbed Faster and in Higher Amounts than Their Glucosides in Humans. J. Nutr. 2000, 130, 1695–1699. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RDSW | Mineral Water (Control) | |||||
|---|---|---|---|---|---|---|
| Total (n = 49) | Men (n = 19) | Women (n = 30) | Total (n = 49) | Men (n = 21) | Women (n = 28) | |
| Age (year) | 48.1 | 45.9 | 49.4 | 44.2 | 44.2 | 44.2 |
| BMI (kg/m2) (Body Mass Index) | 24.8 | 26.8 | 23.6 | 24.1 | 25.6 | 23.1 |
| Total (n = 49) | Men (n = 19) | Women (n = 30) | Total (n = 46) | Men (n = 19) | Women (n = 27) | |
| sIgA (μg/g) (secretory immunoglobulin A) | 656 | 810 | 558 | 536 | 571 | 512 |
| Putrefaction (μg/g) | ||||||
| Phenol | 6.01 | 10.02 | 3.47 | 5.72 | 9.63 | 3.68 |
| p-Cresol | 51.59 | 43.78 | 56.53 | 62.78 | 27.26 | 87.78 |
| 4-Ethylphenol | 0.60 | 0.36 | 0.75 | 1.03 | 0.70 | 1.26 |
| Indol | 25.93 | 26.31 | 25.69 | 27.08 | 20.57 | 31.67 |
| Skatol | 2.69 | 2.31 | 2.94 | 3.69 | 2.72 | 4.37 |
| SCFA (short-chain-fatty-acids, mg/g) | ||||||
| Succinic acid | 0.39 | 0.65 | 0.22 | 0.30 | 0.33 | 0.29 |
| Lactic acid | 0.02 | 0.04 | 0.01 | 0.06 | 0.12 | 0.02 |
| Formic acid | 0.00 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 |
| Acetic acid | 2.73 | 3.09 | 2.50 | 2.88 | 3.43 | 2.49 |
| Propionic acid | 1.22 | 1.48 | 1.05 | 1.29 | 1.40 | 1.21 |
| Isobutyric acid | 0.10 | 0.10 | 0.10 | 0.11 | 0.08 | 0.13 |
| Butyric acid | 0.95 | 0.98 | 0.93 | 0.87 | 0.86 | 0.87 |
| 3-Methylbutanoic acid | 0.19 | 0.18 | 0.20 | 0.22 | 0.14 | 0.28 |
| Valeric acid | 0.20 | 0.21 | 0.19 | 0.18 | 0.16 | 0.20 |
| Total (n = 48 | Men (n = 18) | Women (n = 30) | Total (n = 48) | Men (n = 21) | Women (n = 27) | |
| Urine Isoflavones | ||||||
| Daidzein (mg/g-Cre) | 1.74 | 1.98 | 1.56 | 3.28 | 2.50 | 3.89 |
| Genistein (mg/g-Cre) | 2.16 | 2.34 | 2.04 | 3.99 | 3.27 | 4.55 |
| Total (n = 19) | Men (n = 6) | Women (n = 13) | Total (n = 17) | Men (n = 9) | Women (n = 8) | |
| Equol (mg/g-Cre) | 2.57 | 2.53 | 2.58 | 2.30 | 1.98 | 2.66 |
| RDSW (n = 49) | Mineral Water (Control) (n = 46) | |||
|---|---|---|---|---|
| Pre-Intervention | Post-Intervention | Pre-Intervention | Post-Intervention | |
| sIgA (μg/g) | 656 | 567 ↓ ** | 536 | 544 |
| Putrefaction (μg/g) | ||||
| Phenol | 6.01 | 3.08 ↓ * | 5.72 | 5.77 |
| p-Cresol | 51.59 | 54.22 | 62.78 | 61.56 |
| 4-Ethylphenol | 0.60 | 1.21 | 1.03 | 0.46 |
| Indol | 25.93 | 25.99 | 27.08 | 30.50 |
| Skatol | 2.69 | 2.65 | 3.69 | 3.69 |
| SCFA (mg/g) | ||||
| Succinic acid | 0.39 | 0.47 ↑ * | 0.30 | 0.27 |
| Lactic acid | 0.02 | 0.05 ↑ * | 0.06 | 0.03 |
| Formic acid # | 0.00 | 0.00 | 0.00 | 0.02 |
| Acetic acid | 2.73 | 3.04 ↑ * | 2.88 | 2.34 ↓ ** |
| Propionic acid | 1.22 | 1.33 | 1.29 | 1.12 ↓ * |
| Isobutyric acid | 0.10 | 0.13 ↑ * | 0.11 | 0.12 |
| Butyric acid | 0.95 | 0.86 | 0.87 | 0.78 |
| 3-Methylbutanoic acid | 0.19 | 0.23 ↑ * | 0.22 | 0.21 |
| Valeric acid | 0.20 | 0.19 | 0.18 | 0.17 |
| RDSW (Rate, % Total) | Mineral Water (Rate, % Total) | Total (Rate, % Total) | |
|---|---|---|---|
| Daidzein | 46 */48 (96) | 48 **/48 (100) | 94/96 (98) |
| Genistein | 47 #/48 (98) | 47/48 (98) | 94/96 (98) |
| Daidzein and Genistein | 46/48 (96) | 47/48 (98) | 93/96 (97) |
| Equol | 19 †/48 (40) | 17 ††/48 (35) | 36/96 (38) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeuchi, H.; Higuchi, K.; Yoshikane, Y.; Takagi, R.; Tokuhiro, S.; Takenaka, K.; Oboshi, W.; Kimura, A.; Islam, J.M.; Kaneko, A.; et al. Drinking Refined Deep-Sea Water Improves the Gut Ecosystem with Beneficial Effects on Intestinal Health in Humans: A Randomized Double-Blind Controlled Trial. Nutrients 2020, 12, 2646. https://doi.org/10.3390/nu12092646
Takeuchi H, Higuchi K, Yoshikane Y, Takagi R, Tokuhiro S, Takenaka K, Oboshi W, Kimura A, Islam JM, Kaneko A, et al. Drinking Refined Deep-Sea Water Improves the Gut Ecosystem with Beneficial Effects on Intestinal Health in Humans: A Randomized Double-Blind Controlled Trial. Nutrients. 2020; 12(9):2646. https://doi.org/10.3390/nu12092646
Chicago/Turabian StyleTakeuchi, Hiroaki, Keiro Higuchi, Yu Yoshikane, Ryo Takagi, Shinji Tokuhiro, Koichi Takenaka, Wataru Oboshi, Asako Kimura, Jahirul Md. Islam, Ayami Kaneko, and et al. 2020. "Drinking Refined Deep-Sea Water Improves the Gut Ecosystem with Beneficial Effects on Intestinal Health in Humans: A Randomized Double-Blind Controlled Trial" Nutrients 12, no. 9: 2646. https://doi.org/10.3390/nu12092646
APA StyleTakeuchi, H., Higuchi, K., Yoshikane, Y., Takagi, R., Tokuhiro, S., Takenaka, K., Oboshi, W., Kimura, A., Islam, J. M., Kaneko, A., Sato, S., & Ishizuka, S. (2020). Drinking Refined Deep-Sea Water Improves the Gut Ecosystem with Beneficial Effects on Intestinal Health in Humans: A Randomized Double-Blind Controlled Trial. Nutrients, 12(9), 2646. https://doi.org/10.3390/nu12092646