The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Diet and Physical Activity Questionnaires
2.3. Statistical Analyses
3. Results
3.1. Study Participants
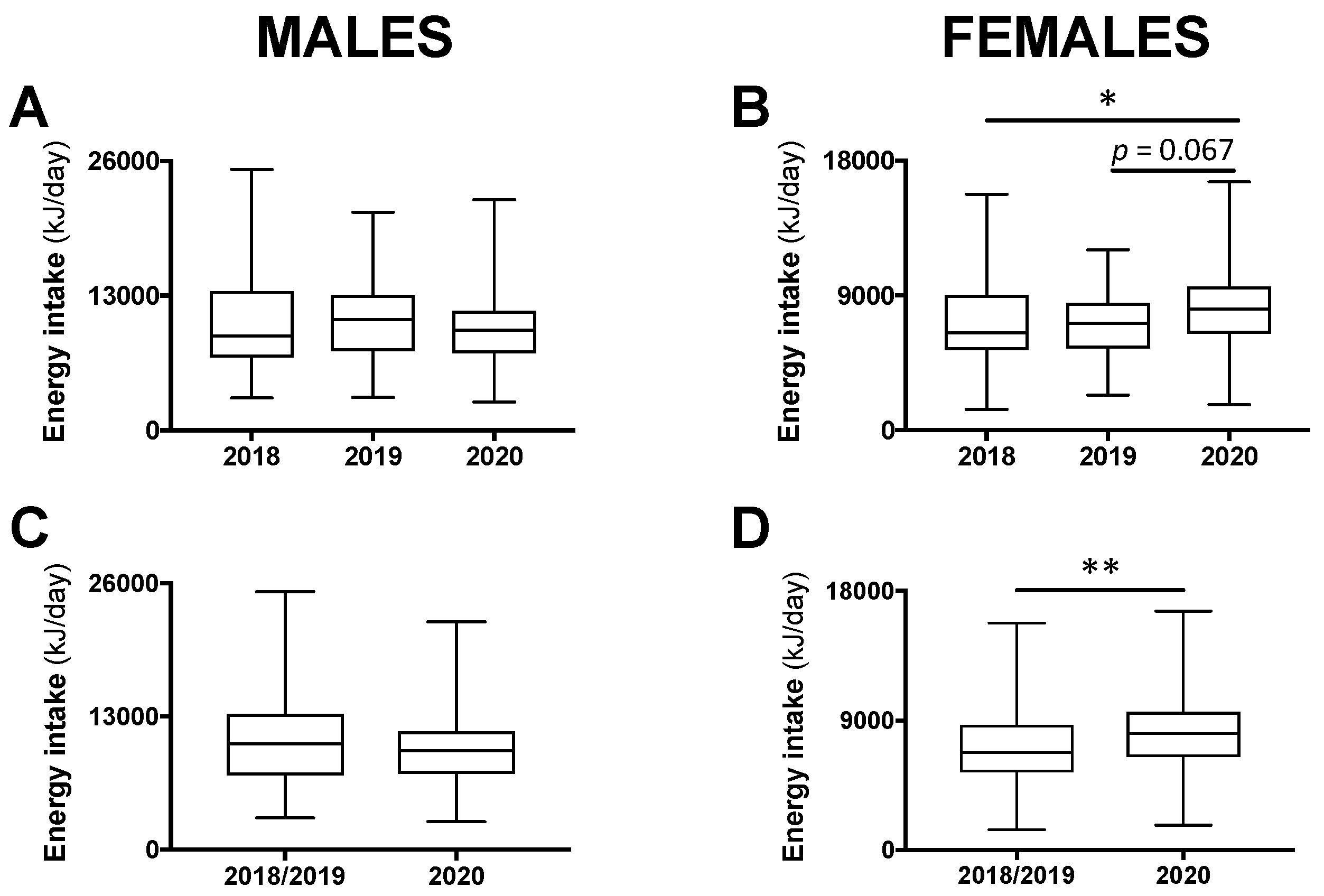
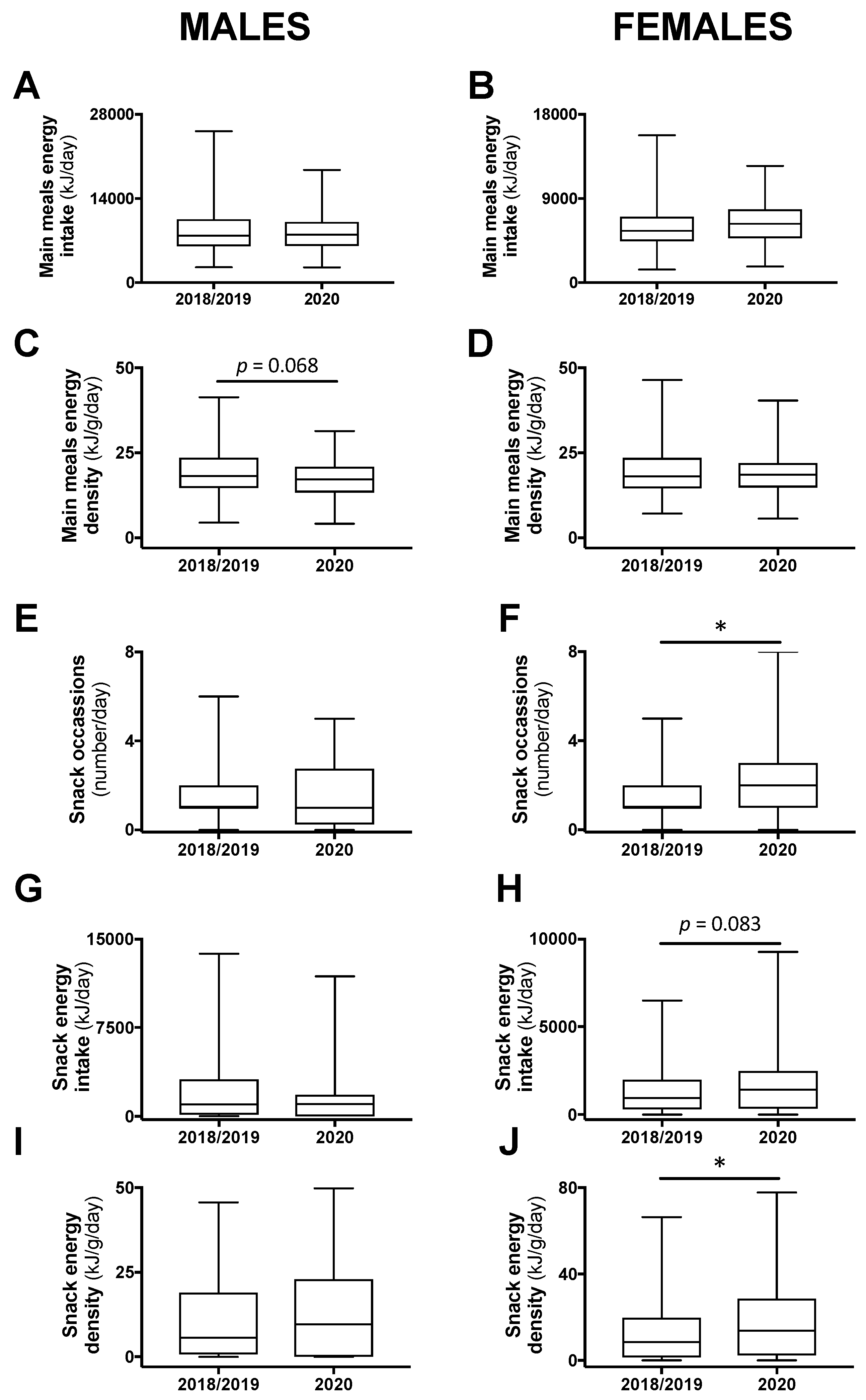
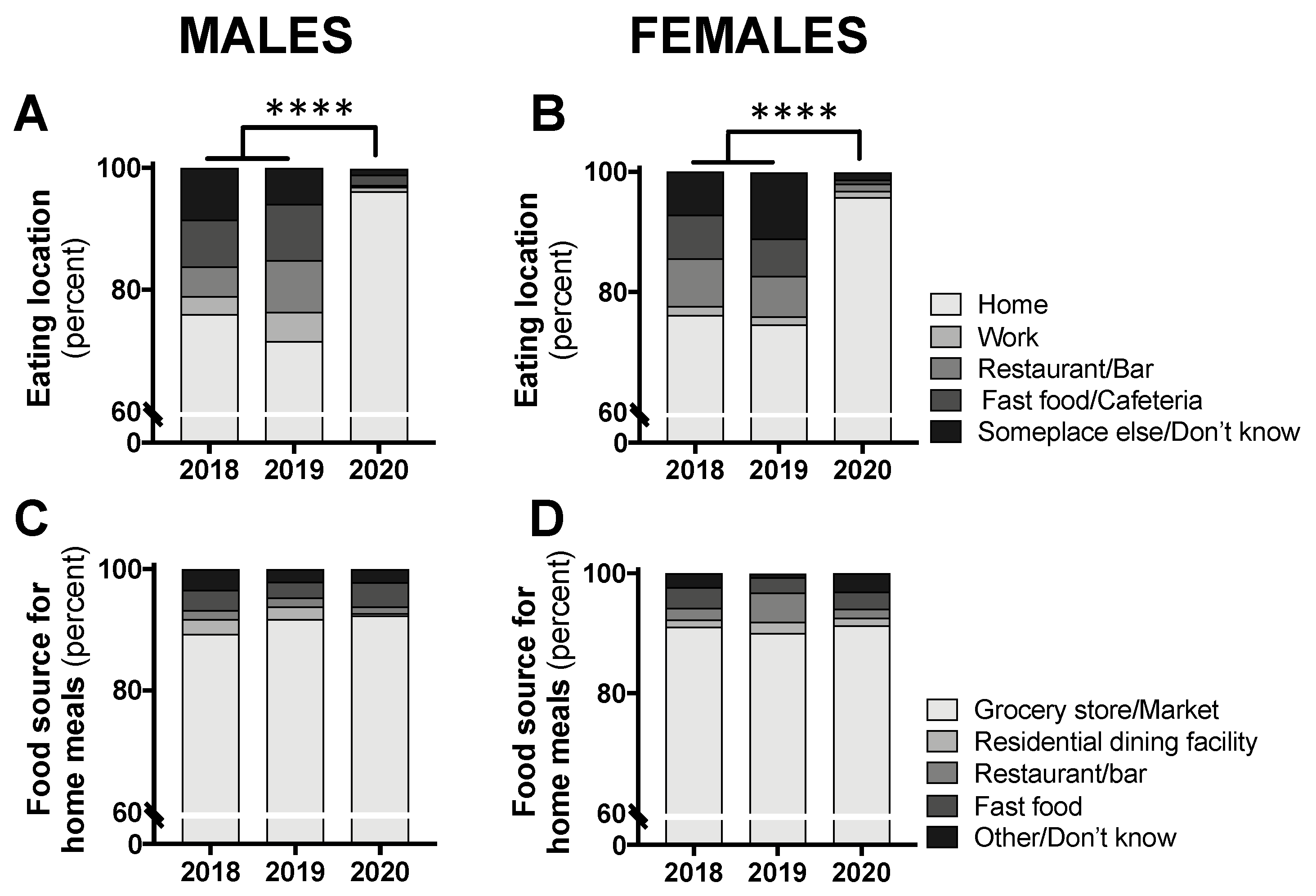
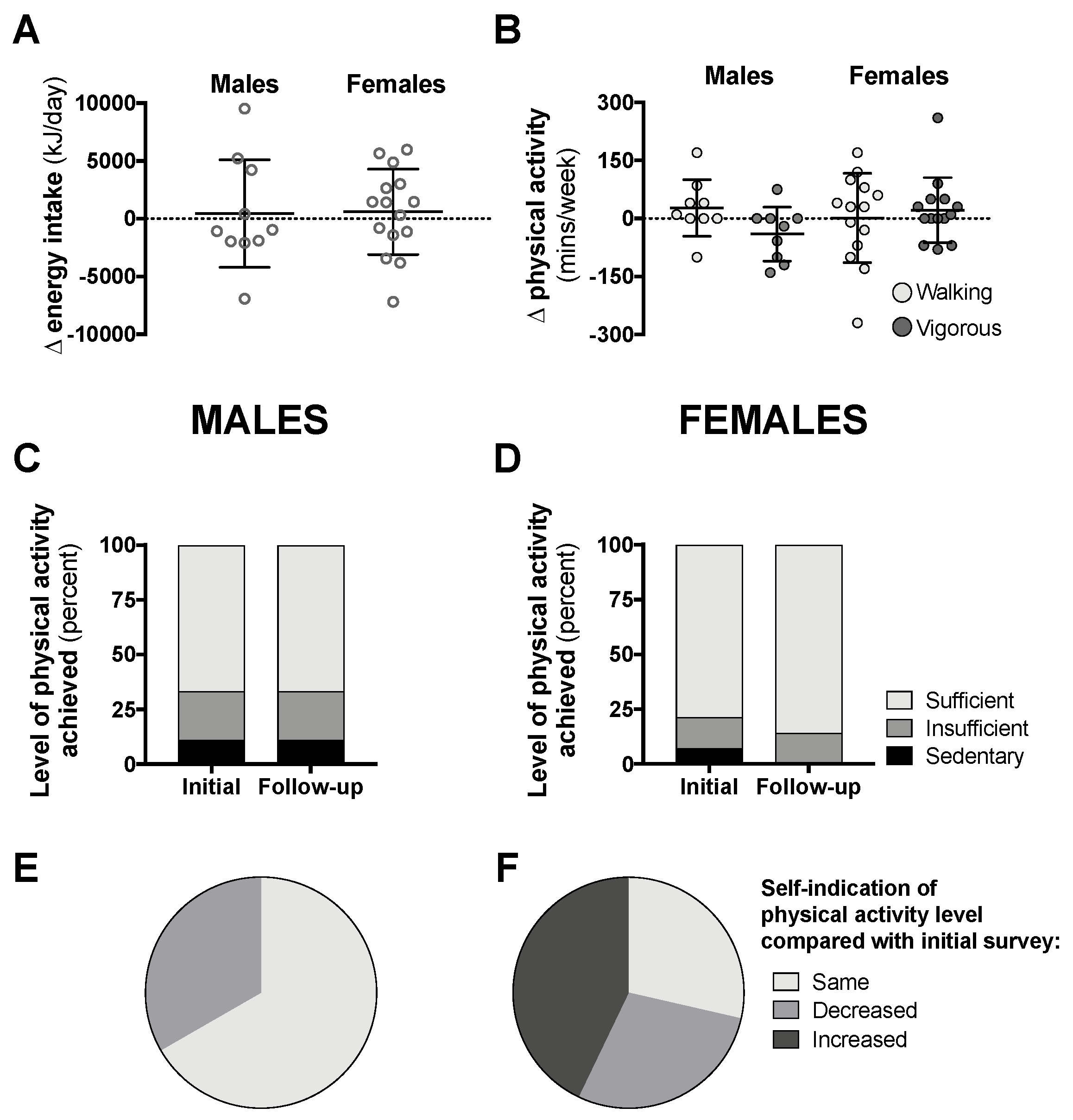
3.2. Dietary Intake from ASA 24-Hour Recall
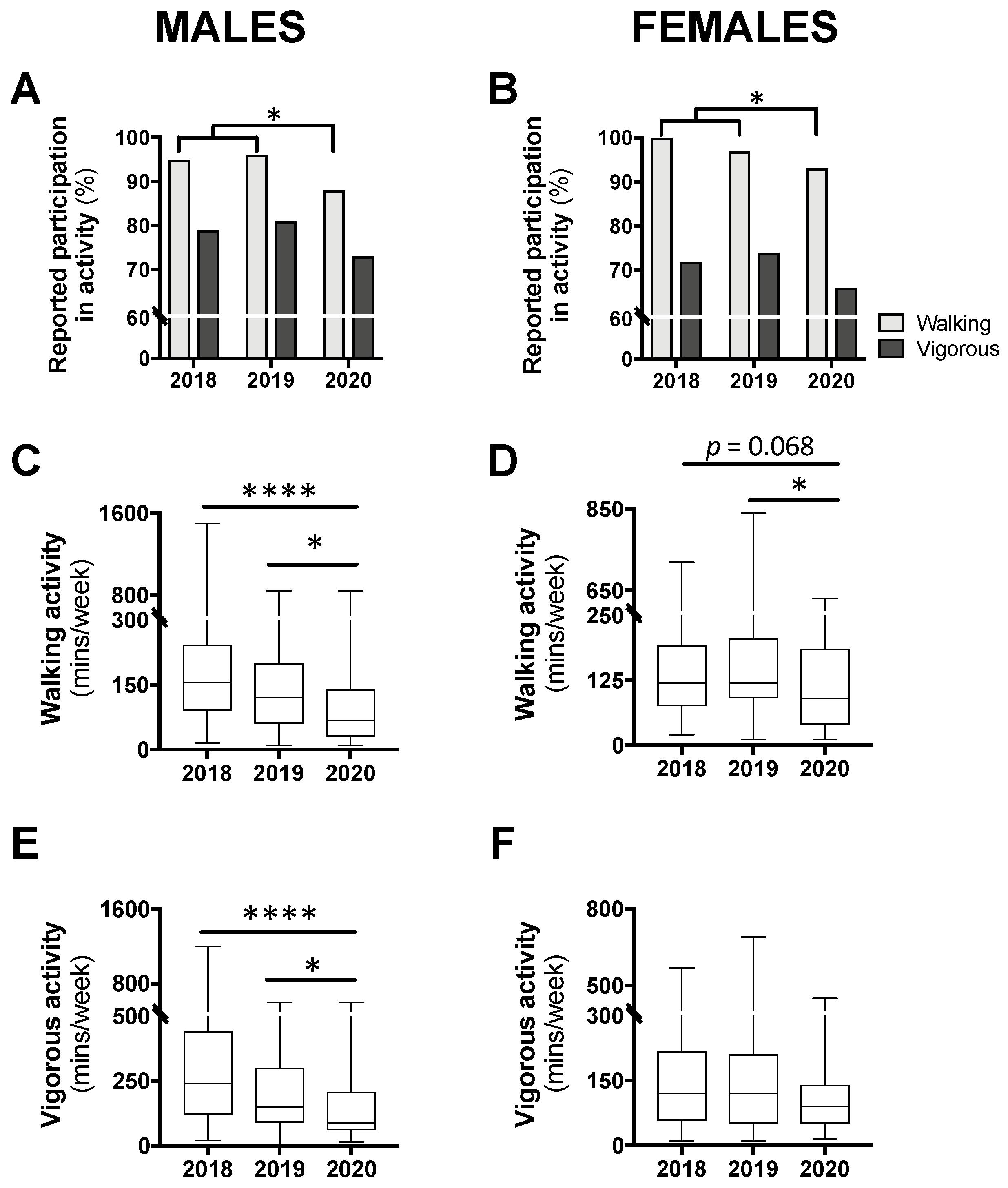
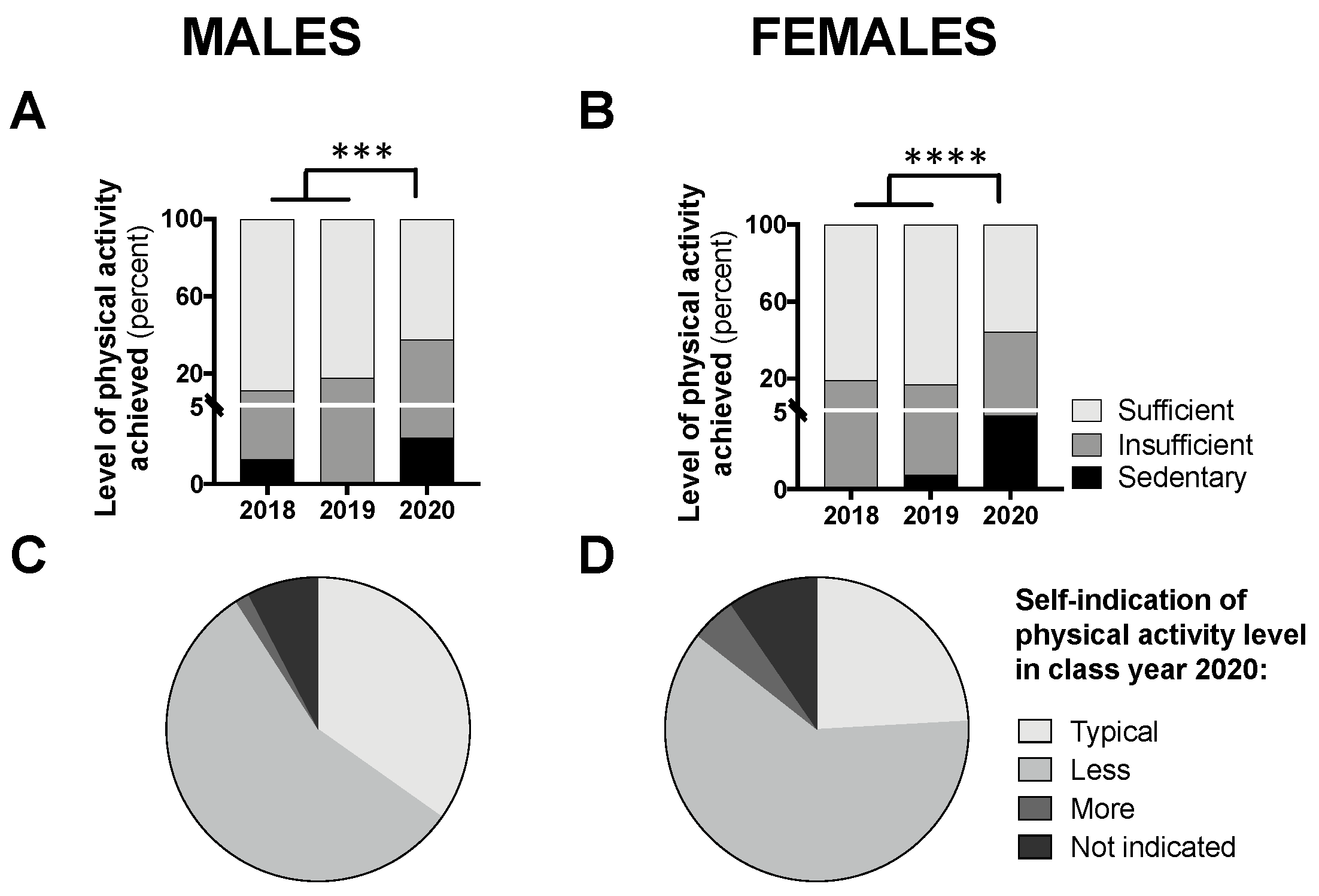
3.3. Physical Activity Levels from the Active Australia Survey
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Disease (COVID-2019) Situation Report—152; World Health Organization: Geneva, Switzerland, 2020.
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Hopmeyer, A.; Medovoy, T. Emerging adults’ self-identified peer crowd affiliations, risk behavior, and social–emotional adjustment in college. Emerg. Adulthood 2017, 5, 143–148. [Google Scholar] [CrossRef]
- Umberson, D.; Crosnoe, R.; Reczek, C. Social relationships and health behavior across life course. Annu. Rev. Sociol. 2010, 36, 139–157. [Google Scholar] [CrossRef] [PubMed]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The automated self-administered 24-h dietary recall (ASA24): A resource for researchers, clinicians, and educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- The Active Austrralia Survey: A Guide and Manual for Implementation, Analysis and Reporting; Autralian Institute of Health and Welfare (AIHW): Canberra, Australia, 2003.
- Nguyen, B.T.; Powell, L.M. The impact of restaurant consumption among US adults: Effects on energy and nutrient intakes. Public Health Nutr. 2014, 17, 2445–2452. [Google Scholar] [CrossRef]
- Seguin, R.A.; Aggarwal, A.; Vermeylen, F.; Drewnowski, A. Consumption frequency of foods away from home linked with higher body mass index and lower fruit and vegetable intake among adults: A cross-sectional study. J. Environ. Public Health 2016, 2016, 3074241. [Google Scholar] [CrossRef]
- Wansink, B. Environmental factors that increase the food intake and consumption volume of unknowing consumers. Annu. Rev. Nutr. 2004, 24, 455–479. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus and COVID-19 pandemic: A review. Int. J. Surg. 2020. [Google Scholar] [CrossRef]
- Higgs, S.; Thomas, J. Social influences on eating. Curr. Opin. Behav. Sci. 2016, 9, 1–6. [Google Scholar] [CrossRef]
- Brindal, E.; Wilson, C.; Mohr, P.; Wittert, G. Eating in groups: Do multiple social influences affect intake in a fast-food restaurant? J. Health Psychol. 2015, 20, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Ton, W. Kids Helpline Strains under Youth Demand; Australian Associated Press: Rhodes, Australia, 2020; Available online: https://www.aap.com.au/kids-helpline-strains-under-youth-demand/ (accessed on 7 May 2020).
- Stress and Gender. In: Stress in America; American Psychological Association: Washington, DC, USA, 2010; Available online: https://www.apa.org/news/press/releases/stress/2010/gender-stress.pdf (accessed on 7 May 2020).
- Yau, Y.H.C.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar] [PubMed]
- Asarian, L.; Geary, N. Sex differences in the physiology of eating. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 305, R1215–R1267. [Google Scholar] [CrossRef] [PubMed]
- Gearhardt, A.N.; Grilo, C.M.; DiLeone, R.J.; Brownell, K.D.; Potenza, M.N. Can food be addictive? Public health and policy implications. Addiction 2011, 106, 1208–1212. [Google Scholar] [CrossRef] [PubMed]
- Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011–2012. Report 4364.0.55.007 Table 1.1; Australian Bureau of Statistics: Canberra, Australia. Available online: http://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4364.0.55.0072011-12?OpenDocument (accessed on 1 May 2020).
- Cohen, A.K.; Rai, M.; Rehkopf, D.H.; Abrams, B. Educational attainment and obesity: A systematic review. Obes. Rev. 2013, 14, 989–1005. [Google Scholar] [CrossRef] [PubMed]
- Correa-Rodriguez, M.; Pocovi, G.; Schmidt-RioValle, J.; Gonzalez-Jimenez, E.; Rueda-Medina, B. Assessment of dietary intake in Spanish university students of health sciences. Endocrinol. Diabetes Nutr. 2018, 65, 265–273. [Google Scholar] [CrossRef]
- Czlapka-Matyasik, M.; Lonnie, M.; Wadolowska, L.; Frelich, A. “Cutting down on sugar” by Non-dieting young women: An impact on diet quality on weekdays and the weekend. Nutrients 2018, 10, 1463. [Google Scholar] [CrossRef]
- Racette, S.B.; Weiss, E.P.; Schechtman, K.B.; Steger-May, K.; Villareal, D.T.; Obert, K.A.; Holloszy, J.O. Influence of weekend lifestyle patterns on body weight. Obesity (Silver Spring) 2008, 16, 1826–1830. [Google Scholar] [CrossRef]
- An, R. Weekend-weekday differences in diet among U.S. adults, 2003–2012. Ann. Epidemiol. 2016, 26, 57–65. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020. [Google Scholar] [CrossRef]
- Ball, J.W.; Bice, M.R.; Parry, T. Adults’ motivation for physical activity: Differentiating motives for exercise, sport, and recreation. Recreat. Sports J. 2014, 38, 130–142. [Google Scholar] [CrossRef]
- Australian Health Survey: Physical Activity, 2011–2012. Australian Bureau of Statistics: Canberra, Australia. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/4364.0.55.0042011-12?OpenDocument (accessed on 7 May 2020).
- Molanorouzi, K.; Khoo, S.; Morris, T. Motives for adult participation in physical activity: Type of activity, age, and gender. BMC Public Health 2015, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working, G. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010.
- King, A.C.; Powell, K.E.; Kraus, W.E. The US physical activity guidelines advisory committee report-introduction. Med. Sci. Sports Exerc. 2019, 51, 1203–1205. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Warburton, D.E.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; Leblanc, A.G.; Zehr, L.; et al. New Canadian physical activity guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 36–46. [Google Scholar] [CrossRef] [PubMed]
- UK Chief Medical Officers’ Physical Activity Guidelines; Department of Health: London, UK, 2019.
- Australia’s Physical Activity & Sedentary Behaviour Guidelines for Adults (18–64 Years); Australian Government: Canberra, Australia, 2014.
- Grech, A.; Allman-Farinelli, M. Prevalence and period trends of overweight and obesity in Australian young adults. Eur. J. Clin. Nutr. 2016, 70, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N.; Kohl, H.W.; Gordon, N.F.; Paffenbarger, R.S., Jr. How much physical activity is good for health? Annu. Rev. Public Health 1992, 13, 99–126. [Google Scholar] [CrossRef]
- Charansonney, O.L.; Despres, J.P. Disease prevention—Should we target obesity or sedentary lifestyle? Nat. Rev. Cardiol. 2010, 7, 468–472. [Google Scholar] [CrossRef]
- McGuire, D.K.; Levine, B.D.; Williamson, J.W.; Snell, P.G.; Blomqvist, C.G.; Saltin, B.; Mitchell, J.H. A 30-year follow-up of the Dallas Bedrest and Training Study: I. Effect of age on the cardiovascular response to exercise. Circulation 2001, 104, 1350–1357. [Google Scholar] [CrossRef]
- Stathopoulou, G.; Powers, M.B.; Berry, A.C.; Smits, J.A.J.; Otto, M.W. Exercise Interventions for Mental Health: A Quantitative and Qualitative Review. Clin. Psychol. Sci. Pract. 2006, 13, 179–193. [Google Scholar] [CrossRef]
- Eyler, A.E.; Wilcox, S.; Matson-Koffman, D.; Evenson, K.R.; Sanderson, B.; Thompson, J.; Wilbur, J.; Rohm-Young, D. Correlates of physical activity among women from diverse racial/ethnic groups. J. Womens Health Gend. Based Med. 2002, 11, 239–253. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraca, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Drew, M.K.; Finch, C.F. The Relationship Between Training Load and Injury, Illness and Soreness: A Systematic and Literature Review. Sports Med. 2016, 46, 861–883. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year 2018 | Year 2019 | Year 2020 | |
|---|---|---|---|
| Males | |||
| Entered study (n) | 75 | 80 | 70 |
| >27 years of age or unknown (n) | 1 | 2 | 4 |
| No diet and physical activity data (n) | 3 | 1 | 0 |
| Total included in study (n) | 71 | 77 | 66 |
| Included for diet [n (%)] | 65 (91.5) | 63 (81.8) | 64 (97.0) |
| Did not start/incomplete diet survey (n) | 4 | 12 | 2 |
| Excluded diet data (n) | 2 | 2 | 0 |
| Weekend: weekday diet recall [n (% weekend)] | 45:20 (69.2) | 27:36 (42.9) ** | 17:47 (26.6) **** |
| Included for physical activity [n (%)] | 61 (85.9) | 73 (94.8) | 66 (100) |
| Did not start/incomplete physical activity survey (n) | 2 | 2 | 0 |
| Excluded physical activity data (n) | 8 | 2 | 0 |
| Completed follow-up diet [n (% initial cohort)] | NA | NA | 10 (15.6) |
| Completed follow-up physical activity [n (% initial cohort)] | NA | NA | 9 (13.6) |
| Females | |||
| Entered study (n) | 105 | 112 | 89 |
| >27 years of age or unknown (n) | 2 | 2 | 5 |
| No diet and physical activity data (n) | 0 | 2 | 0 |
| Total included in study (n) | 103 | 108 | 84 |
| Included for diet [n (%)] | 101 (98.1) | 96 (88.9) | 82 (97.6) |
| Did not start/incomplete diet survey (n) | 2 | 10 | 2 |
| Excluded diet data (n) | 0 | 2 | 0 |
| Weekend: weekday diet recall [n (% weekend)] | 70:31 (69.3) | 28:68 (29.2) **** | 29:53 (35.4) **** |
| Included for physical activity [n (%)] | 97 (94.2) | 104 (96.3) | 83 (98.8) |
| Did not start/incomplete physical activity survey (n) | 1 | 2 | 1 |
| Excluded physical activity data (n) | 5 | 2 | 0 |
| Completed follow-up diet [n (% initial cohort)] | NA | NA | 15 (18.3) |
| Completed follow-up physical activity [n (% initial cohort)] | NA | NA | 14 (16.9) |
| Year 2018 | Year 2019 | Year 2020 | |
|---|---|---|---|
| Males | n = 71 | n = 77 | n = 66 |
| Age [median (range), years] | 19 (19–25) | 20 (19–25) | 20 (19–27) *^ |
| Ethnicity [n (%)] | |||
| Asian | 23 (32.4%) | 18 (23.4%) | 25 (37.9%) |
| Asian sub-continental | 4 (5.6%) | 7 (9.1%) | 6 (9.1%) |
| Caucasian | 39 (54.9%) | 42 (54.5%) | 29 (43.9%) |
| Multi | 2 (2.8%) | 1 (1.3%) | 4 (6.1%) |
| Other/not disclosed | 3/0 (4.2%) | 5/4 (11.7%) | 2/0 (3.0%) |
| Females | n = 103 | n = 108 | n = 84 |
| Age [median (range), years] | 20 (19–26) | 20 (19–23) | 21 (19–26) *^ |
| Ethnicity [n (%)] | |||
| Asian | 29 (28.2%) | 28 (25.9%) | 27 (32.1%) |
| Asian sub-continental | 3 (2.9%) | 10 (9.3%) | 8 (9.5%) |
| Caucasian | 65 (63.1%) | 60 (55.6%) | 44 (52.4%) |
| Multi | 3 (2.9%) | 6 (5.6%) | 2 (2.4%) |
| Other/not disclosed | 3/0 (2.9%) | 3/1 (3.7%) | 2/1 (3.6%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallo, L.A.; Gallo, T.F.; Young, S.L.; Moritz, K.M.; Akison, L.K. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients 2020, 12, 1865. https://doi.org/10.3390/nu12061865
Gallo LA, Gallo TF, Young SL, Moritz KM, Akison LK. The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients. 2020; 12(6):1865. https://doi.org/10.3390/nu12061865
Chicago/Turabian StyleGallo, Linda A., Tania F. Gallo, Sophia L. Young, Karen M. Moritz, and Lisa K. Akison. 2020. "The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students" Nutrients 12, no. 6: 1865. https://doi.org/10.3390/nu12061865
APA StyleGallo, L. A., Gallo, T. F., Young, S. L., Moritz, K. M., & Akison, L. K. (2020). The Impact of Isolation Measures Due to COVID-19 on Energy Intake and Physical Activity Levels in Australian University Students. Nutrients, 12(6), 1865. https://doi.org/10.3390/nu12061865