Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Location
2.2. Study Design, Population, and Sample Size
2.3. Sampling Procedure
2.4. Data Collection
2.5. Questionnaire
2.5.1. Socio-Demographic Characteristics
2.5.2. Knowledge on Malnutrition
2.5.3. Attitude on Malnutrition
2.5.4. Practice on Malnutrition
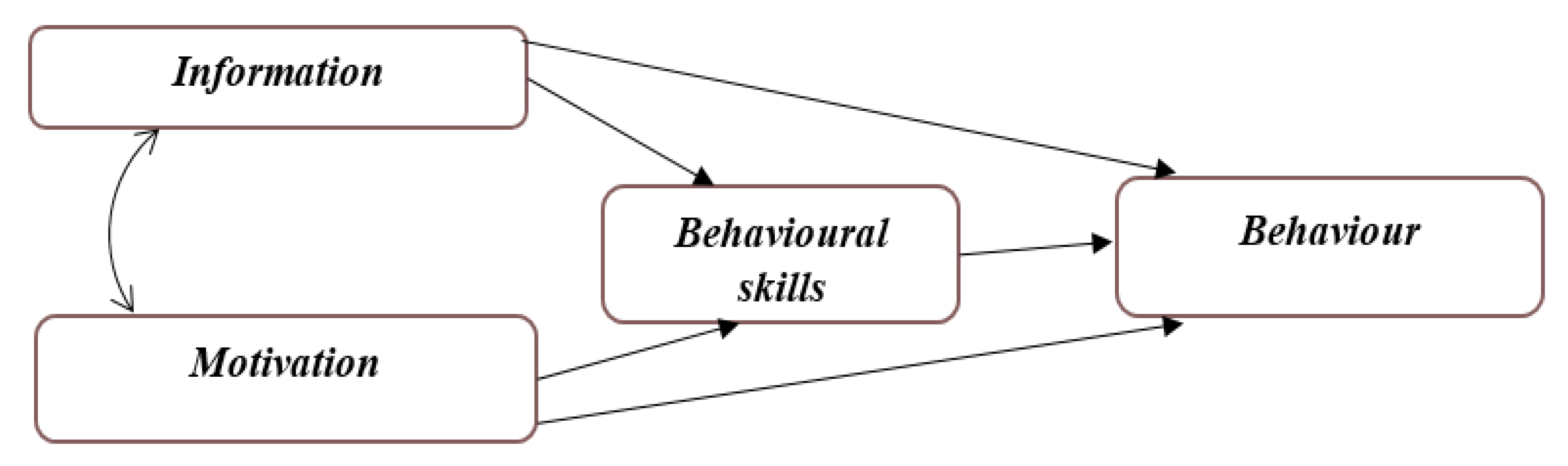
2.5.5. Information–Motivation–Behavioral Skills Construct (IMB)
2.6. Data Analysis
2.7. Ethical Approval and Consent
3. Results
3.1. Descriptive Analysis
3.1.1. Socio-Demographic Characteristics of Respondents
3.1.2. Knowledge towards Reducing Malnutrition
3.1.3. Attitude towards Reducing Malnutrition
3.1.4. Practice towards Reducing Malnutrition
3.1.5. Information, Motivation, and Behavioral Skills of Respondents towards Reducing Malnutrition
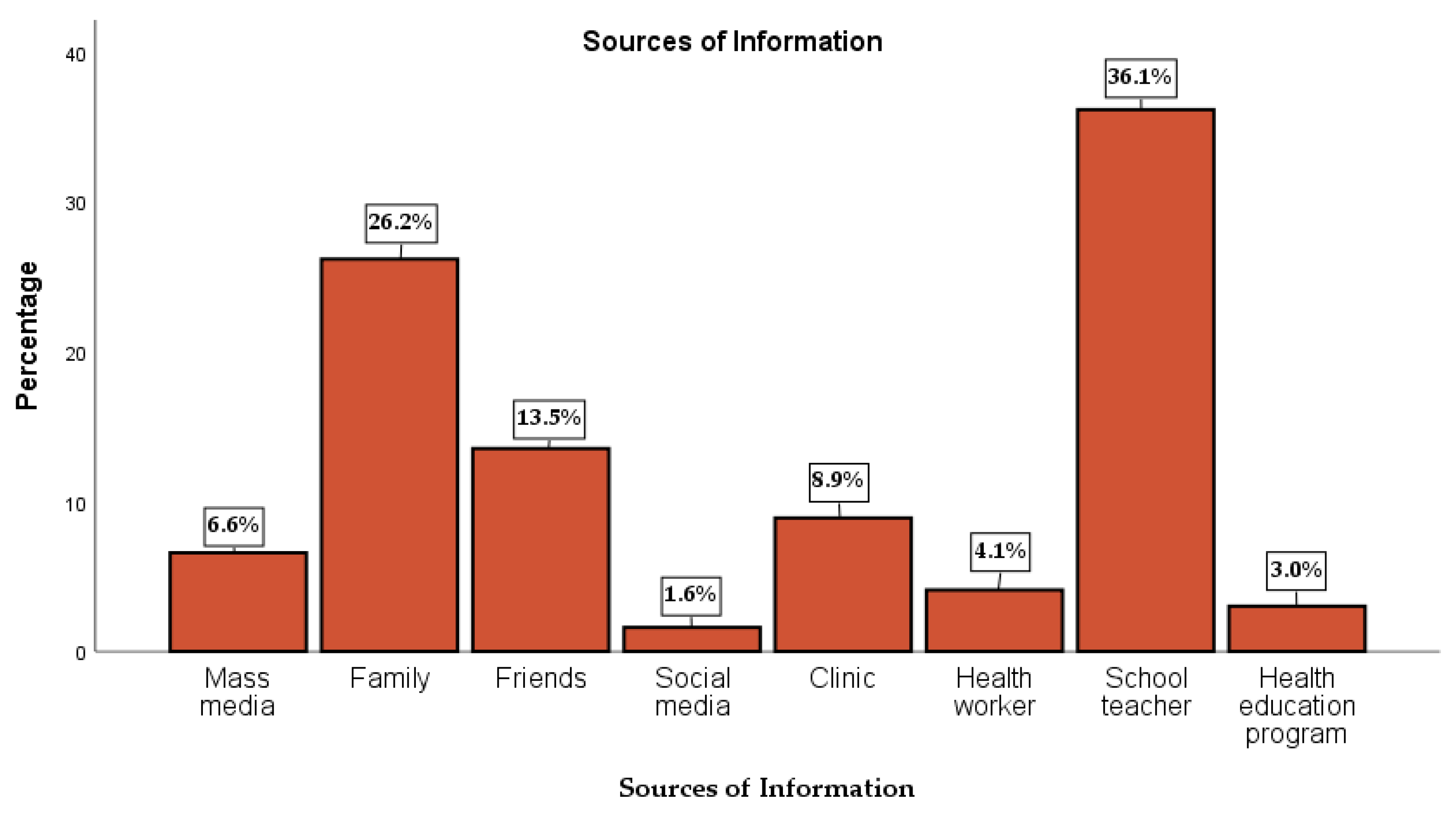
3.1.6. Sources of Information
3.2. Association between Sociodemographic Characteristics, Information, Motivation, and Behavioral Skills with Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition
3.2.1. Predictors of Knowledge, Attitude, and Practices towards Reducing Malnutrition
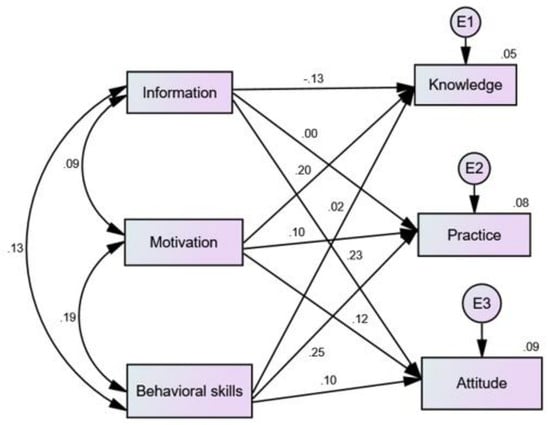
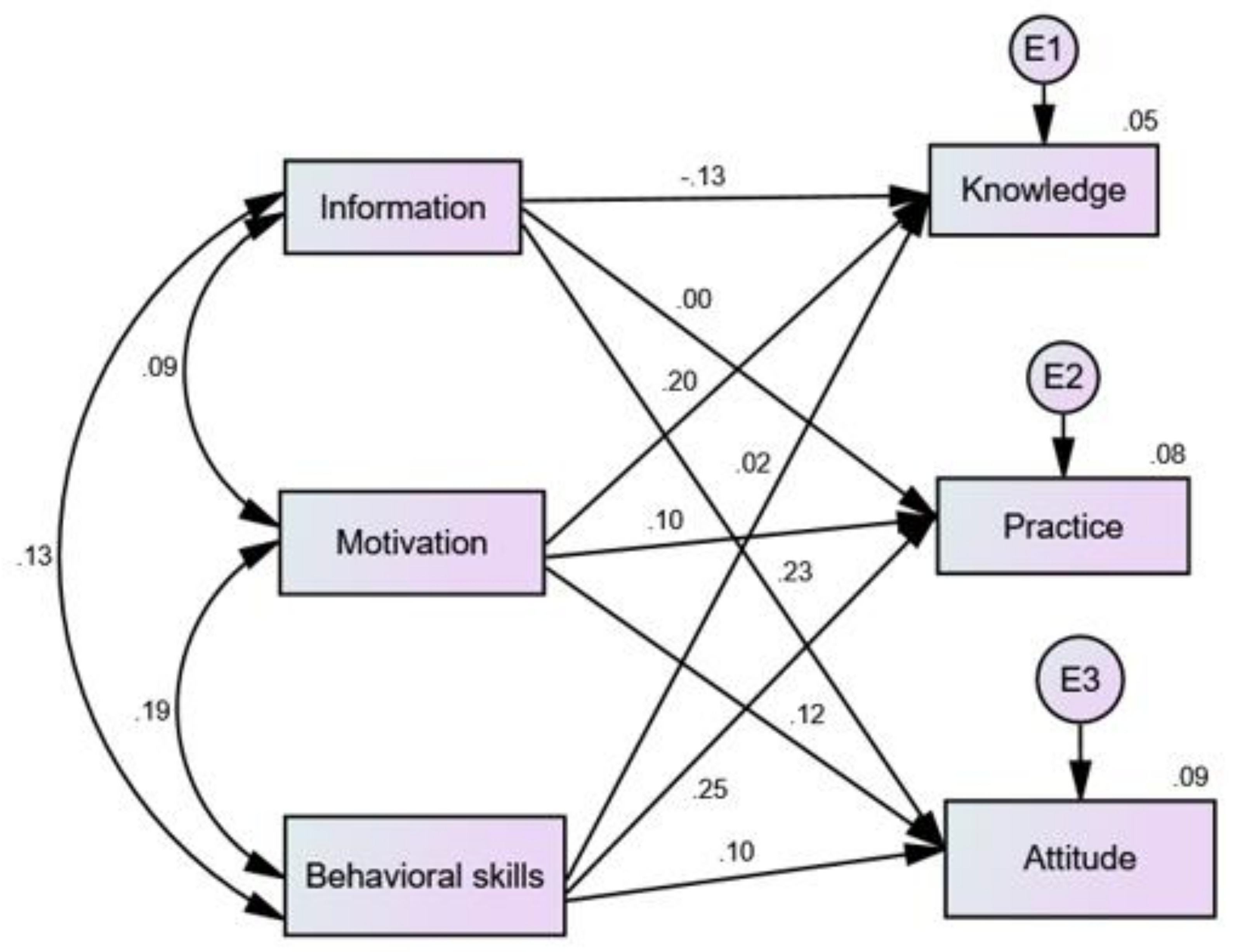
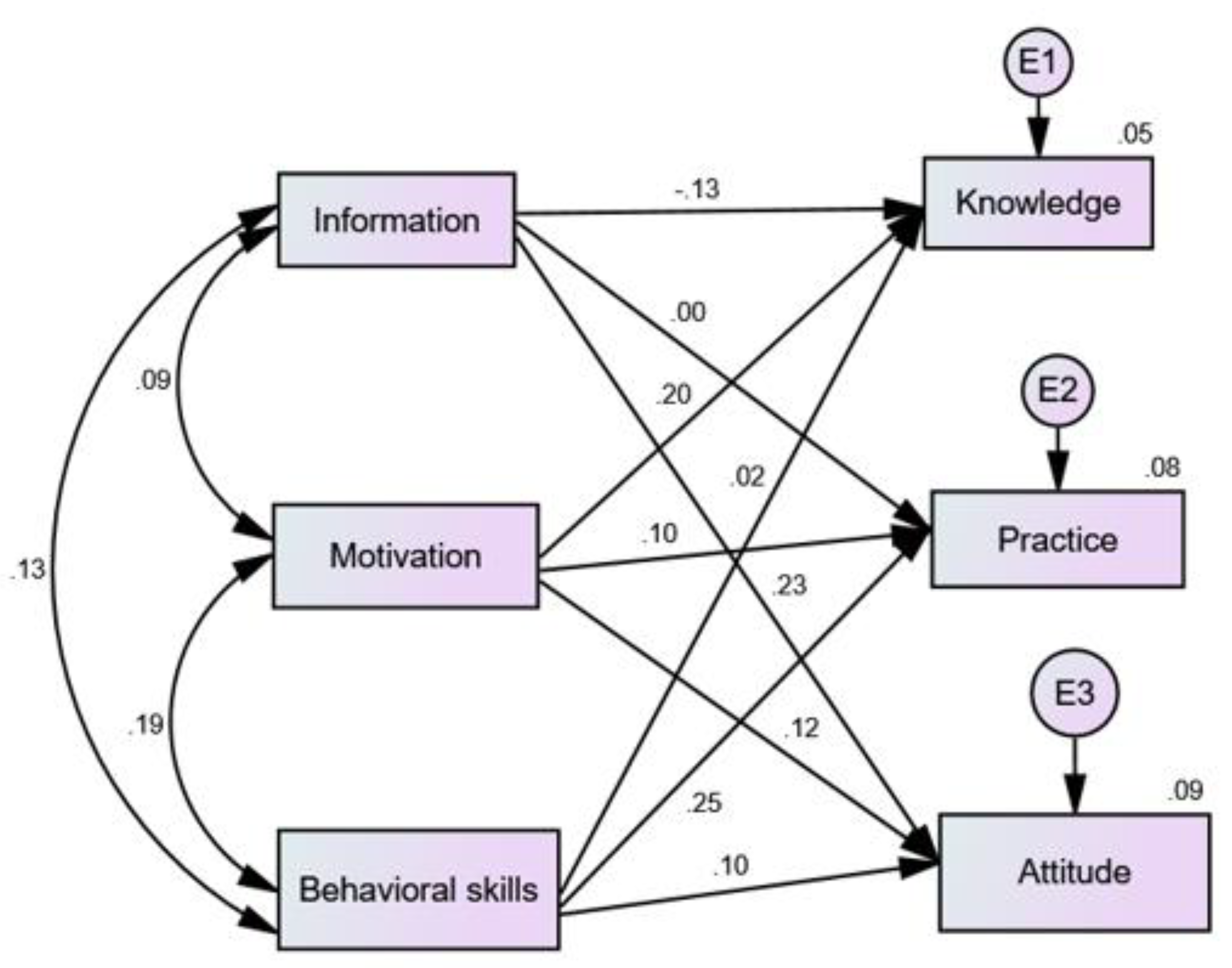
3.2.2. Information, Motivation, Behavioral skills (IMB) Model and Knowledge, Attitude, Practice
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- UNICEF. The State of the World’s Children 2011: Adolescence an Age of Opportunity; United Nation Children’s Fund: New York, NY, USA, 2011; pp. 1–137. [Google Scholar]
- Christian, P.; Smith, E.R. Adolescent Undernutrition: Global Burden, Physiology, and Nutritional Risks. Ann. Nutr. Metab. 2018, 72, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Aa, A.; Ahmed, P. Adolescent malnutrition: Prevalence and pattern in Abuja Municipal Area Council, Nigeria. Niger. J. Paediatr. 2014, 41, 99–103. [Google Scholar]
- World Health Organization. Adolescent Pregnancy; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- World Health Organization. Adolescent Pregnancy: Issues in Adolescent Health and Development; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- World Health Organization (WHO). The Health of the People: What Works: The African Regional Health Report 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Save the Children. Changing the story (of the nigerian child). Save Child. Niger. 2016, 1–8. Available online: https://nigeria.savethechildren.net/sites/nigeria.savethechildren.net/files/library/Changing%20the%20story%20of%20the%20Nigerian%20Girl%20Child.pdf (accessed on 10 March 2020).
- Sireesha, G.; Rajani, N.; Bindu, V. Teenage girls’ knowledge attitude and practices on nutrition. Int. J. Home Sci. 2017, 3, 491–494. [Google Scholar]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Mason, J.B.; Saldanha, L.S.; Ramakrishnan, U.; Lowe, A.; Elizabeth, A.; Girard, A.W.; Mcfarland, D.A.; Martorell, R. Opportunities for improving maternal nutrition and birth outcomes: Synthesis of country experiences. Food Nutr. Bull. 2013, 33, 104–138. [Google Scholar] [CrossRef]
- Mason, J.B.; Shrimpton, R.; Saldanha, L.S.; Ramakrishnan, U.; Victora, C.G.; Girard, A.W.; McFarland, D.A.; Martorell, R. The first 500 days of life: Policies to support maternal nutrition. Glob. Health Action 2015, 8, 1–8. [Google Scholar] [CrossRef]
- ACC/SCN. Low Birthweight: Report of a Meeting in Dhaka, Bangladesh on 14–17 June 1999; ACC/SCN in Collaboration with ICDDR,B: Geneva, Switzerland, 2000; Volume 63, pp. 1–56. [Google Scholar]
- National Population Commission (Nigeria) and ICP International. Nigeria Demographic and Health Survey 2013; NPC and ICF International: Abuja, Nigeria; Rockville, MD, USA, 2014; pp. 1–565. [Google Scholar]
- Omobuwa, O.; Alebiosu, C.O.; Olajide, F.O.; Adebimpe, W.O. Assessment of nutritional status of in-school adolescents in Ibadan, Nigeria Assessment of nutritional status of in-school adolescents in Ibadan, Nigeria. S. Afr. Fam. Pract. 2014, 56, 246–250. [Google Scholar] [CrossRef]
- Kola-Raji, B.A.; Mobolanle, R.; Balogun, T.O.O. A comparative study of nutritional status of adolescents from selected private and public boarding secondary schools in Ibadan, South Western Nigeria. J. Med. Trop. 2017, 19, 43–48. [Google Scholar]
- Esimai, O.A.; Ojofeitimi, E. Nutrition and Health Status of Adolescents in a Private Secondary School in Port Harcourt. Health Sci. J. 2015, 9, 2–6. [Google Scholar]
- Essien, E.; Emebu, P.K.; Iseh, K.R.; Haruna, M.J. Assessment of Nutritional Status and Knowledge of Students From Selected Secondary Schools in Sokoto Metropolis, Sokoto State, Nigeria. Afr. J. Food Agric. Nutr. Dev. 2014, 14, 9454–9468. [Google Scholar]
- Bindra, V. Anemia in adolescence. Med. Clin. N. Am. 2017, 59, 1481–1488. [Google Scholar] [CrossRef]
- Lehtimaki, S.; Schwalbe, N. Adolescent Health. The Missing Population in Universal Health Coverage. 2019, pp. 1–32. Available online: https://www.who.int/pmnch/media/news/2018/Adolescent-Health-Missing-Population-in-UHC.pdf (accessed on 10 March 2020).
- Peyman, N.; Abdollahi, M. Using of information-motivation-behavioral skills model on nutritional behaviors in controlling anemia among girl students. J. Res. Health 2017, 7, 736–744. [Google Scholar]
- Kelly, S.; Melnyk, B.M.; Belyea, M. Predicting physical activity and fruit and vegetable intake in adolescents: A test of the information, motivation, behavioral skills model. Res. Nurs. Health 2012, 35, 146–163. [Google Scholar] [CrossRef]
- Canavan, C.R.; Fawzi, W.W. Addressing knowledge gaps in adolescent nutrition: Toward advancing public health and sustainable development. Curr. Dev. Nutr. 2019, 3, 4–6. [Google Scholar] [CrossRef]
- World Atlas. Where is Maiduguri, Nigeria. Borno Map WorldAtlas. 2018. Available online: https://www.worldatlas.com/webimage/countrys/africa/ng.htm (accessed on 10 March 2020).
- National Population Commission NPC (2006). Federal Republic of Nigeria Official Gazzette; The Federal Government Press: Lagos, Nigeria, 2006; p. 96.
- Aday, L.A.; Cornelius, L.J. Designing and Conducting Health Surveys: A Comprehensive Guide, 3rd ed.; A Wiley Imprint: Hoboken, NJ, USA, 2006; pp. 1–546. [Google Scholar]
- Melaku, Y.; Dirar, A.; Feyissa, G.T.; Tamiru, D. Optimal dietary practices and nutritional knowledge of school adolescent girls in Jimma Town, South West Ethiopia. Int. J. Adolesc. Youth 2017, 3843, 1–9. [Google Scholar] [CrossRef]
- Susan Paul, N.S.; Mathew, P.; Johns, F.; Abraham, J. The feasibility of using remote data collection tools in field surveys. Int. J. Community Med. Public Health 2018, 5, 81. [Google Scholar] [CrossRef]
- Govender, D.; Naidoo, S.; Taylor, M. Knowledge, attitudes and peer influences related to pregnancy, sexual and reproductive health among adolescents using maternal health services in Ugu, KwaZulu-Natal, South Africa. BMC Public Health 2019, 19, 928. [Google Scholar] [CrossRef]
- Kassahun, C.W.; Mekonen, A.G. Knowledge, attitude, practices and their associated factors towards diabetes mellitus among non diabetes community members of Bale Zone administrative towns, South East. PLoS ONE 2017, 12, e0170040. [Google Scholar] [CrossRef] [PubMed]
- Westland, J.C. An Introduction to Structural Equation Models; Springer: Cham, Switerland, 2015; Volume 22, pp. 1–8. [Google Scholar]
- Molaifard, A.; Mohamadian, H.; Haghighi Zadeh, M.H. Predicting high school students’ health-promoting lifestyle: A test of the information, motivation, behavioral skills model. Int. J. Adolesc. Med. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Goodell, L.S.; Pierce, M.B.; Amico, K.R.; Ferris, A.M. Parental Information, Motivation, and Behavioral Skills Correlate with Child Sweetened Beverage Consumption. J. Nutr. Educ. Behav. 2012, 44, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Upadhaya, G. Structure Equation Modeling Basic Assumptions and Concepts: A novices guide. Int. J. Quant. Qual. Res. Methods 2017, 13, 1576–1580. [Google Scholar]
- Kumar, S. Structure Equation Modeling Basic Assumptions and Concepts: A Novices Guide. Asian J. Manag. Sci. 2015, 03, 25–28. [Google Scholar]
- Chen, M.Y. Validation of the wood’s job satisfaction questionnaire among taiwanese nonprofit sport organization workers. Soc. Indic. Res. 2009, 94, 437–447. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Saw, S.M.; Ng, T.P. The design and assessment of questionnaires in clinical research. Singap. Med. J. 2001, 42, 131–135. [Google Scholar]
- Birru, S.M.; Tariku, A.; Belew, A.K. Improved dietary diversity of school adolescent girls in the context of urban Northwest Ethiopia: 2017. Ital. J. Pediatr. 2018, 44, 1–6. [Google Scholar] [CrossRef]
- Pal, A.; Pari, A.K.; Sinha, A.; Dhara, P.C. Prevalence of undernutrition and associated factors: A cross-sectional study among rural adolescents in West Bengal. Indian Int. J. Pediatr. Adolesc. Med. 2017, 4, 9–18. [Google Scholar] [CrossRef]
- British Council. Girls’ Education in Nigeria. Report 2014: Issues, Influencers and Actions. 2014, pp. 1–47. Available online: https://www.britishcouncil.org/sites/default/files/british-council-girls-education-nigeria-report.pdf (accessed on 10 March 2020).
- Kigaru, D.M.D.; Loechl, C.; Moleah, T.; Macharia-Mutie, C.W.; Ndungu, Z.W. Nutrition knowledge, attitude, and practices among urban primary school children in Nairobi City, Kenya: A KAP study. BMC Nutr. 2015, 1, 44. [Google Scholar] [CrossRef]
- Badrasawi, M.M.; Shraim, N.Y.; Al-atrash, M.H. Knowledge of Physical Education Students about Nutrition: A Cross-Sectional Study from Palestine. Int. J. Nutr. Pharmacol. Neurol. Dis. 2018, 8, 101. [Google Scholar]
- Al-Yateem, N.; Rossiter, R. Nutritional knowledge and habits of adolescents aged 9 to 13 years in Sharjah, United Arab Emirates: A crosssectional study. East. Mediterr. Health J. 2017, 23, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Shi, Y.; Chang, C.; Stewart, D.; Ji, Y.; Wang, Y.; Harris, N. Knowledge, attitudes and behaviour regarding nutrition and dietary intake of seventh-grade students in rural areas of Mi Yun County, Beijing, China. Environ. Health Prev. Med. 2014, 19, 179–186. [Google Scholar] [CrossRef]
- Oldewage-Theron, W.; Egal, A.; Moroka, T. Nutrition Knowledge and Dietary Intake of Adolescents in Cofimvaba, Eastern Cape, South Africa. Ecol. Food Nutr. 2015, 54, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, S.; Mishra, C.P.; Shukla, K.P. Dietary Pattern and Nutrition Related Knowledge of Rural Adolescent Girls. Indian J. Prev. Soc. Med. 2010, 41, 4. [Google Scholar]
- Patimah, S.; Royani, I.; Mursaha, A.; Thaha, A.R. Knowledge, attitude, and practice of balanced diet and correlation with hypochromic microcytic anemia among adolescent school girls in maros district, South Sulawesi, Indonesia. Biomed. Res. 2016, 27, 165–171. [Google Scholar]
- Fisher, W.A.; Fisher, J.D.; Harman, J. The Information—Motivation—Behavioral Skills Model: A General Social Psychological Approach to Understanding and Promoting Health Behavior. Soc. Psychol. Found. Health Illn. 2003, 22, 82–106. [Google Scholar]
- Fisher, J.D.; Fisher, W.A.; Bryan, A.D.; Misovich, S.J. Information-motivation-behavioral skills model-based HIV risk behavior change intervention for inner-city high school youth. Health Psychol. 2002, 21, 177–186. [Google Scholar] [CrossRef]
- Masuku, S.K.S.; Lan, S.J.J. Nutritional knowledge, attitude, and practices among pregnant and lactating women living with HIV in the manzini region of Swaziland. J. Health Popul. Nutr. 2014, 32, 261–269. [Google Scholar]
- Gali, N.; Tamiru, D.; Tamrat, M. Journal of Pediatric Nursing The Emerging Nutritional Problems of School Adolescents: Overweight/Obesity and Associated Factors in Jimma Town, Ethiopia. J. Pediatr. Nurs. 2017, 35, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.S.; Hogan, S.L.; Jordan, J.M.; De Vellis, R.F.; Carpenter, D.M. Examining whether the information-motivation-behavioral skills model predicts medication adherence for patients with a rare disease. Patient Prefer. Adherence 2017, 11, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.J.; Choi, S.; Kim, S.A.; Song, M. Intervention strategies based on information-motivation-behavioral skills model for health behavior change: A systematic review. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2014, 8, 172–181. [Google Scholar] [CrossRef]
- Bazargan, M.; Stein, J.A.; Bazargan-Hejazi, S.; Hindman, D.W. Using the Information-Motivation Behavioral Model to Predict Sexual Behavior Among Underserved Minority Youth. J. Sch. Health 2010, 3, 973–982. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Classification | Frequency (n = 562) | Percentage (%) |
|---|---|---|---|
| Schools a | Yerwa | 108 | 19.2 |
| GGSS | 63 | 11.2 | |
| GGC | 86 | 15.3 | |
| Shehu Garbai | 72 | 12.8 | |
| Bulabulin day | 149 | 26.5 | |
| Zajeri day | 84 | 14.9 | |
| Age of adolescent girls (years) | Early adolescents | 100 | 17.8 |
| Middle adolescents | 280 | 49.8 | |
| Late adolescents | 182 | 32.4 | |
| Class b | JSS1 | 132 | 23.5 |
| JSS2 | 110 | 19.6 | |
| SS1 | 147 | 26.2 | |
| SS2 | 173 | 30.8 | |
| Ethnicity | Bura | 48 | 8.5 |
| Kanuri | 173 | 30.5 | |
| Hausa | 58 | 10.3 | |
| Marghi | 52 | 9.3 | |
| Shuwa | 28 | 5.0 | |
| Fulani | 52 | 9.3 | |
| Chibok | 19 | 3.4 | |
| Gwoza | 87 | 15.5 | |
| Other ethnic group c | 45 | 8.0 | |
| Religion | Christianity | 115 | 20.5 |
| Islam | 447 | 79.5 | |
| Place of residence | Urban | 448 | 86.8 |
| Rural | 74 | 13.2 | |
| Household size | ≤5 members | 46 | 8.2 |
| 6–8 members | 207 | 36.8 | |
| ≥9 members | 309 | 55.0 | |
| Monthly income | >18,000 | 163 | 29.0 |
| 18,000–30,000 | 200 | 35.6 | |
| 31,000–50,000 | 139 | 24.7 | |
| ≥51,000 | 60 | 10.7 | |
| Head of household | Father | 510 | 90.7 |
| Mother | 31 | 5.5 | |
| Relations | 21 | 3.7 | |
| Age of father (years) | ≤34 | ||
| 35–44 | 52 | 9.6 | |
| ≥45 | 488 | 90.4 | |
| Education of father | No education | 57 | 10.3 |
| Informal education | 82 | 14.8 | |
| Primary education | 16 | 2.9 | |
| Secondary education | 193 | 34.8 | |
| Tertiary education | 206 | 37.2 | |
| Occupation of fathers | Civil service | 196 | 35.9 |
| Trading/business | 288 | 52.7 | |
| Farming | 41 | 7.5 | |
| Other occupation d | 21 | 3.8 | |
| Age of mother (years) | ≤34 | 100 | 18.1 |
| 35–44 | 280 | 50.6 | |
| ≥45 | 173 | 31.3 | |
| Education of mothers | No education | 101 | 18.1 |
| Informal education | 123 | 22.1 | |
| Primary education | 58 | 10.4 | |
| Secondary education | 187 | 33.6 | |
| Tertiary education | 88 | 15.8 | |
| Occupation of mothers | Civil service | 86 | 15.7 |
| Trading/business | 232 | 42.4 | |
| Farming | 27 | 4.9 | |
| House wives | 202 | 36.9 | |
| Family type | Monogamy | 281 | 50.0 |
| Polygamy | 239 | 42.5 | |
| single parenting | 42 | 7.5 |
| Knowledge Item on Malnutrition | Correct (%) | Incorrect (%) |
|---|---|---|
| Malnutrition refers to deficiencies in an individual nutritional intake | 199 (35.4) | 363 (64.6) |
| Undernutrition is a form of malnutrition | 50 (8.9) | 512 (91.1) |
| One of the causes of malnutrition is not eating enough food | 212 (37.7) | 350 (62.3) |
| Slow growth in adolescence is a sign of malnutrition | 53 (9.4) | 509 (90.6) |
| Muscle wasting is a sign of malnutrition | 108 (19.2) | 454 (80.8) |
| Stunted growth can be a result of malnutrition | 41 (7.3) | 521 (92.7) |
| One of the ways through malnutrition can be prevented by eating frequently. | 203 (36.1) | 359 (63.9) |
| Carbohydrates, protein, fats are an essential nutrient that the body needs in large amount for growth | 137 (24.4) | 425 (75.6) |
| Cereals are a good source of carbohydrate | 205 (36.5) | 357 (63.5) |
| Carbohydrates are energy giving food | 367 (65.3) | 195 (34.7) |
| Beans are sources of protein | 389 (69.2) | 173 (30.8) |
| Proteins are body building food | 376 (66.9) | 186 (33.1) |
| The body uses fat as a source of energy | 227 (40.4) | 335 (59.6) |
| Butter, oil, nuts, meat, fish, milk contain fats | 391 (69.6) | 171 (30.4) |
| Vitamins and minerals are essential nutrients that the body needs in small amounts to function properly | 132 (23.5) | 430 (76.5) |
| Fruits and vegetables are sources of minerals and vitamins | 373 (66.4) | 189 (33.6) |
| Anaemia can be caused by insufficient iron in the body. | 17 (3.0) | 545 (97.0) |
| Lack of iron in the diet can cause anaemia | 17 (3.0) | 545 (97.0) |
| Slow physical growth can be caused by insufficient iron in the body | 21 (3.7) | 541 (96.3) |
| Meat is a source of iron | 41 (7.3) | 521 (92.7) |
| Pumpkin, (kabewa), carrots, green vegetables are good sources of vitamin A | 141 (25.1) | 421 (74.9) |
| Night blindness is not a sign of insufficient vitamin A in the body * | 24 (4.3) | 538 (95.7) |
| Iodine deficiency can be caused by eating or preparing foods with salt that is not iodized | 29 (5.2) | 533 (94.5) |
| Goitre is a sign of a lack of iodine in the body | 31 (5.5 | 531 (94.5) |
| Calcium is a mineral that makes the bones strong and healthy | 51 (9.1) | 511 (90.9) |
| Milk or green vegetables or beans are good sources of calcium | 160 (28.5) | 402 (71.5) |
| Eating different kinds of food can make us healthy | 409 (72.8) | 153 (27.2) |
| Breakfast is the most important meal of the day | 505 (89.9) | 57 (10.1) |
| Poor knowledge towards malnutrition | 451 (80.2%) | |
| Good knowledge towards malnutrition | 111 (19.8%) | |
| Attitude Item on Malnutrition | Strongly Disagree n (%) | Disagree n (%) | Neutral n (%) | Agree n (%) | Strongly Agree n (%) |
|---|---|---|---|---|---|
| I think I may be malnourished | 154 (27.4) | 242 (43.1) | 105 (18.7) | 36 (6.4) | 25 (4.4) |
| I think poverty is one of the causes of malnutrition. | 41 (7.3) | 71 (12.6) | 78 (13.9) | 301 (53.6) | 71 (12.6) |
| Malnutrition is a serious problem in adolescents | 18 (3.2) | 75 (13.3) | 158 (28.1) | 240 (42.7) | 71 (12.6) |
| I think noodles have more nutrients than food cereals * | 48 (8.5) | 269 (47.9) | 109 (19.4) | 101 (18.0) | 35 (6.2) |
| I think adolescent girls do not need food containing fat at this stage * | 27 (4.8) | 202 (35.9) | 177 (31.5) | 125 (22.2) | 31 (5.5) |
| I think I can get energy from protein only * | 23 (4.1) | 128 (22.8) | 132 (23.5) | 233 (41.5) | 46 (8.2) |
| I think I may be iron deficient | 27 (4.8) | 157 (27.9) | 282 (50.2) | 61 (10.9) | 35 (6.2) |
| I think I may not have sufficient vitamin A in my body | 34 (6.0) | 183 (32.6) | 234 (41.6) | 79 (14.1) | 32 (5.7) |
| I think processed juices (e.g., chivita, five alive, faro) are more nutritious than fresh fruits (e.g., oranges, watermelon, pineapple, mango) * | 67 (11.9) | 294 (52.3) | 94 (16.7) | 71 (12.6) | 36 (6.4) |
| I think it is good to prepare meal with iodized salt | 17 (3.0) | 93 (16.5) | 174 (31.0) | 240 (42.7) | 38 (6.8) |
| I think it is only older people that suffer from calcium deficiency * | 52 (9.3) | 196 (34.9) | 198 (35.2) | 87(15.5) | 29 (5.2) |
| I think when I take breakfast, I perform better in school | 26 (4.6) | 77 (13.7) | 84 (14.9) | 233 (41.5) | 142 (25.3) |
| I think eating three times a day makes me perform better in school | 13 (2.3) | 18 (3.2) | 56 (10.0) | 282 (50.2) | 193 (34.3) |
| I think the taste of food is more important than its nutritional quality * | 28 (5.0) | 147 (26.2) | 121 (21.5) | 218 (38.8) | 48 (8.5) |
| I think expensive foods are the most healthy foods * | 21 (3.7) | 115 (20.5) | 86 (15.3) | 267 (47.5) | 73 (13.0) |
| I think I can be healthy even if I don’t eat varieties of food * | 32 (5.7) | 137 (24.4) | 122 (21.7) | 228 (40.6) | 43 (7.7) |
| I take less nutritious food to have a slim shape * | 42 (7.5) | 231 (41.1) | 164 (29.2) | 96 (17.1) | 29 (5.2) |
| Poor attitude towards malnutrition | 322 (57.3%) | ||||
| Good attitude towards malnutrition | 240 (42.7%) | ||||
| Variable | Medium (IQR)/n (%) |
|---|---|
| Food consumption score | 4(2) |
| Meal frequency score | 25.00(9) |
| Total (practice score) | 29.50 (9) |
| Poor practice (scores <29.5 below Median) | 278 (49.5%) |
| Good practice (scores ≥29.5 above Median) | 284 (50.5%) |
| Information Item | Strongly Disagree n (%) | Disagree n (%) | Neutral n (%) | Agree n (%) | Strongly Agree n (%) |
| The best way to prevent malnutrition is to eat different kinds of food | 18 (3.2) | 87 (15.5) | 154 (27.4) | 182 (32.4) | 121 (21.5) |
| What I eat makes me malnourished | 33 (5.9) | 241 (42.9) | 172 (30.6) | 86 (15.3) | 30 (5.3) |
| There is no food that can help prevent malnutrition * | 37 (6.6) | 226 (40.2) | 163 (29.0) | 108 (19.2) | 28 (5.0) |
| If you are malnourished, there is nothing you can do about it * | 56 (10.0) | 219 (39.0) | 168 (29.9) | 97 (17.3) | 22 (3.9) |
| Malnutrition makes people to be tired always | 18 (3.2) | 88 (15.7) | 234 (41.6) | 182 (32.4) | 40 (7.1) |
| I do not care about eating the right foods for malnutrition * | 31 (5.5) | 168 (29.9) | 209 (37.2) | 129 (23.0) | 25 (4.4) |
| With everything else that is going on in my life, I don’t care about finding foods that can prevent me from being malnourished * | 32 (5.7) | 181 (32.2) | 202 (35.9) | 125 (22.2) | 22 (3.9) |
| Motivation | Strongly Disagre n (%) | Disagree n (%) | Neutral n (%) | Agree n (%) | Strongly Agree n (%) |
| I think I like eating different kinds of foods | 11 (2.0) | 45 (8.0) | 59 (10.5) | 324 (57.7) | 123 (21.9) |
| I think the people who are important to me (family and friends) like eating different kinds of food | 8 (1.4) | 52 (9.3) | 100 (17.8) | 324 (57.7) | 78 (13.9) |
| I think the people who are important to me (family and friends) always encourage me to eat different kinds of food | 10 (1.8) | 46 (8.2) | 101 (18.0) | 345 (61.4) | 60 (10.7) |
| I think the people who are important to me (friends and family) always encourage me to buy nutritious food | 9 (1.6) | 47 (8.4) | 108 (19.2) | 337 (60.0) | 61 (10.9) |
| Behavioral Skills | Very Hard n (%) | Hard n (%) | Neutral n (%) | Easy n (%) | Very Easy n (%) |
| How hard or easy is it for you to buy nutritious food? | 47 (8.4) | 303 (53.9) | 69 (12.3) | 129 (23) | 14 (2.5) |
| How hard or easy is it for you to buy nutritious food within your current budget for food? | 58(10.3) | 307 (54.6) | 73 (13.0) | 112 (19.9) | 12 (2.1) |
| How hard or easy is it for you to buy and store fish, rice, meat, or fruits at home? | 81 (14.4) | 298 (53.0) | 72 (12.8) | 98 (17.4) | 13 (2.3) |
| How hard or easy is it for you to cook nutritious food? | 48 (8.5) | 264 (47.0) | 101 (18.0) | 126 (22.4) | 23 (4.1) |
| How hard or easy is it for you to cook nutritious food for your family members | 51 (9.1) | 276 (49.1) | 93 (16.5) | 125 (22.2) | 17 (3.0) |
| Variable | Knowledge | Attitude | Practice | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | Adjusted Odd Ratio | 95% CI | p-Value | B | Adjusted Odd Ratio | 95% CI | p-Value | B | Adjusted Odd Ratio | 95% CI | p-Value | |
| Name of school | ||||||||||||
| Yerwa | Ref | Ref | ||||||||||
| GGSS | −1.193 | 0.303 | 0.109–0.842 | 0.022 * | - | - | - | - | 1.352 | 3.866 | 1.914–7.809 | <0.001 ** |
| GGC | 0.635 | 1.886 | 0.999–3.562 | 0.050 | - | - | - | - | 1.514 | 4.545 | 2.381–8.674 | <0.001 ** |
| Shehu Garbai | −1.895 | 0.150 | 0.043–0.521 | 0.003 * | - | - | - | - | 2.119 | 8.319 | 4.006–17.279 | <0.001 ** |
| Bulabulin Day | −0.488 | 0.614 | 0.323–1.166 | 0.136 | - | - | - | - | 0.622 | 1.862 | 1.063–3.263 | 0.030 * |
| Zajeri | 0.474 | 1.606 | 1.606–3.076 | 0.153 | - | - | - | - | 0.646 | 1.908 | 1.003–3.628 | 0.049 * |
| Religion | - | - | - | - | ||||||||
| Christianity | - | - | - | - | Ref | - | - | - | - | |||
| Islam | - | - | - | - | −0.461 | 0.631 | 0.400–0.994 | 0.047 * | - | - | - | - |
| Education of father | ||||||||||||
| No education | - | - | - | - | - | - | - | - | Ref | |||
| Informal education | - | - | - | - | - | - | - | - | −1.305 | 0.271 | 0.122–0.600 | 0.001 * |
| Primary education | - | - | - | - | - | - | - | - | −1.117 | 0.327 | 0.092–1.158 | 0.083 |
| Secondary education | - | - | - | - | - | - | - | - | −0.578 | 0.561 | 0.283–1.12 | 0.098 |
| Tertiary education | - | - | - | - | - | - | - | - | −0.467 | 0.652 | 0.332–1.282 | 0.215 |
| Information | ||||||||||||
| Poor level of information | - | - | - | - | Ref | Ref | ||||||
| Good level of information | - | - | - | - | 0.949 | 2.584 | 1.736–3.846 | <0.001 ** | 0.467 | 1.595 | 1.058–2.404 | 0.026 * |
| Motivation | ||||||||||||
| Poor level of motivation | - | - | - | - | Ref | - | - | - | - | |||
| Good level of motivation | - | - | - | - | 1.204 | 3.334 | 2.144–5.186 | <0.001 ** | - | - | - | - |
| Behavioral skills | ||||||||||||
| Poor behavioral skill level | - | - | - | - | - | - | - | - | Ref | |||
| Good behavioral skill level | - | - | - | - | - | - | - | - | 0.452 | 1.572 | 1.077–2.296 | 0.019 * |
| Intercept | −1.241 | 0.289 | −0.490 | 0.613 | −0.642 | 0.526 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Charles Shapu, R.; Ismail, S.; Ahmad, N.; Ying, L.P.; Abubakar Njodi, I. Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study. Nutrients 2020, 12, 1681. https://doi.org/10.3390/nu12061681
Charles Shapu R, Ismail S, Ahmad N, Ying LP, Abubakar Njodi I. Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study. Nutrients. 2020; 12(6):1681. https://doi.org/10.3390/nu12061681
Chicago/Turabian StyleCharles Shapu, Ruth, Suriani Ismail, Norliza Ahmad, Lim Poh Ying, and Ibrahim Abubakar Njodi. 2020. "Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study" Nutrients 12, no. 6: 1681. https://doi.org/10.3390/nu12061681
APA StyleCharles Shapu, R., Ismail, S., Ahmad, N., Ying, L. P., & Abubakar Njodi, I. (2020). Knowledge, Attitude, and Practice of Adolescent Girls towards Reducing Malnutrition in Maiduguri Metropolitan Council, Borno State, Nigeria: Cross-Sectional Study. Nutrients, 12(6), 1681. https://doi.org/10.3390/nu12061681