Food Insecurity and COVID-19: Disparities in Early Effects for US Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.2. Analysis
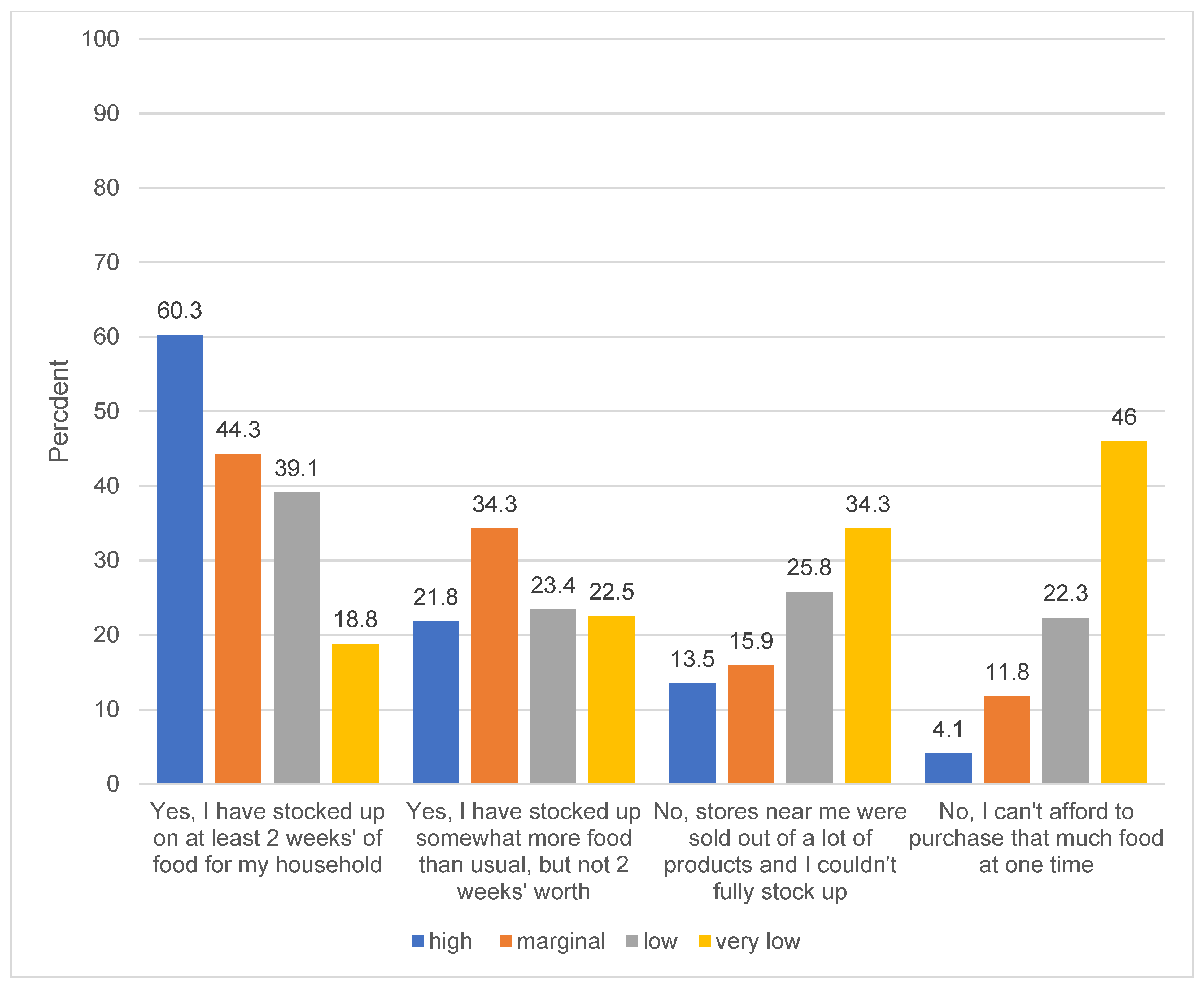
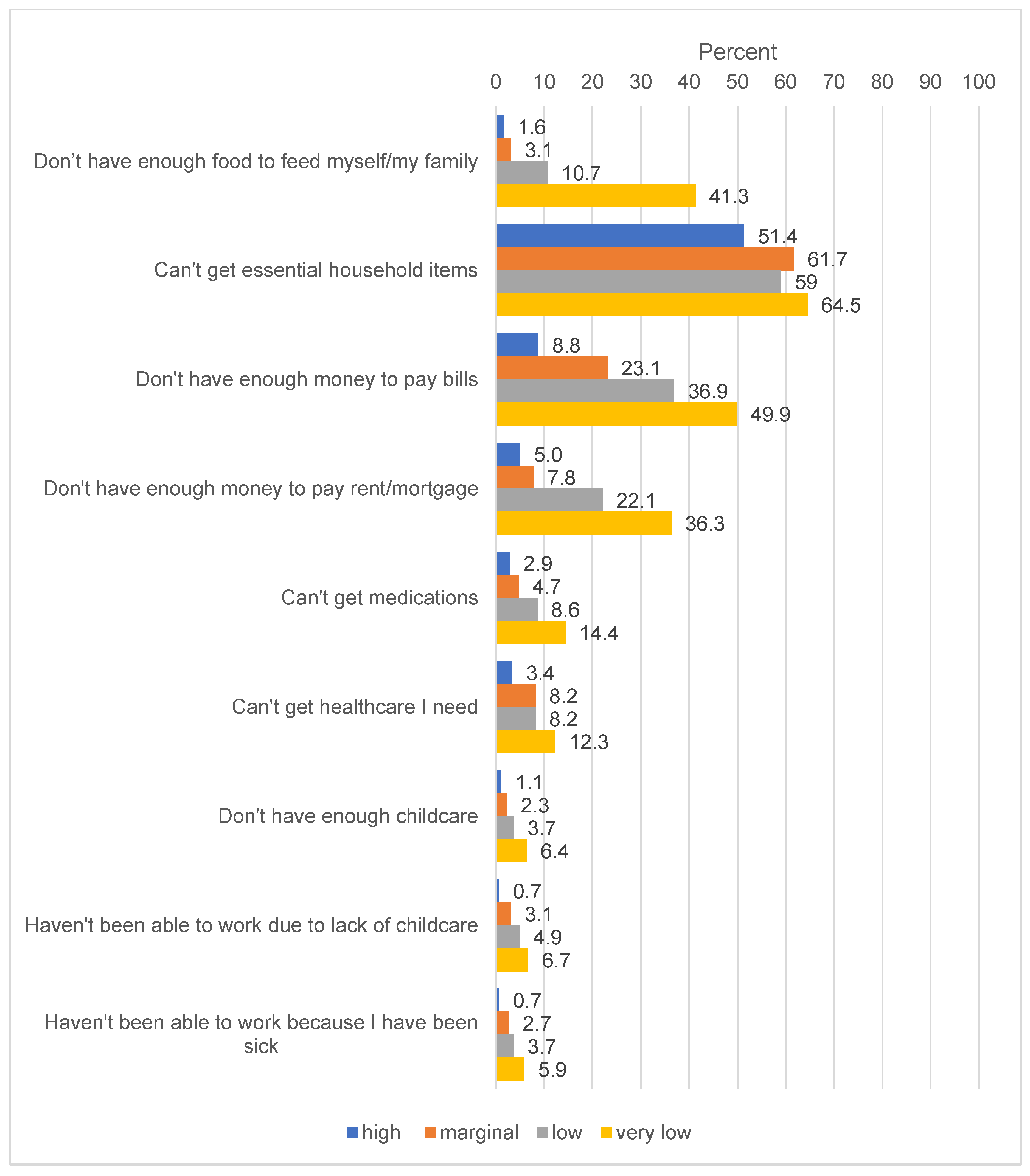
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| State | N | Percent |
|---|---|---|
| Alabama | 22 | 1.49 |
| Alaska | 3 | 0.2 |
| Arizona | 35 | 2.37 |
| Arkansas | 16 | 1.08 |
| California | 150 | 10.15 |
| Colorado | 19 | 1.29 |
| Connecticut | 10 | 0.68 |
| Delaware | 7 | 0.47 |
| District of Columbia | 2 | 0.14 |
| Florida | 102 | 6.9 |
| Georgia | 50 | 3.38 |
| Hawaii | 7 | 0.47 |
| Idaho | 8 | 0.54 |
| Illinois | 62 | 4.19 |
| Indiana | 28 | 1.89 |
| Iowa | 11 | 0.74 |
| Kansas | 19 | 1.29 |
| Kentucky | 27 | 1.83 |
| Louisiana | 17 | 1.15 |
| Maine | 10 | 0.68 |
| Maryland | 20 | 1.35 |
| Massachusetts | 26 | 1.76 |
| Michigan | 58 | 3.92 |
| Minnesota | 21 | 1.42 |
| Mississippi | 14 | 0.95 |
| Missouri | 30 | 2.03 |
| Montana | 4 | 0.27 |
| Nebraska | 5 | 0.34 |
| Nevada | 26 | 1.76 |
| New Hampshire | 6 | 0.41 |
| New Jersey | 37 | 2.5 |
| New Mexico | 13 | 0.88 |
| New York | 100 | 6.77 |
| North Carolina | 52 | 3.52 |
| North Dakota | 0 | 0 |
| Ohio | 68 | 4.6 |
| Oklahoma | 25 | 1.69 |
| Oregon | 17 | 1.15 |
| Pennsylvania | 72 | 4.87 |
| Puerto Rico | 0 | 0 |
| Rhode Island | 3 | 0.2 |
| South Carolina | 30 | 2.03 |
| South Dakota | 3 | 0.2 |
| Tennessee | 31 | 2.1 |
| Texas | 90 | 6.09 |
| Utah | 21 | 1.42 |
| Vermont | 3 | 0.2 |
| Virginia | 29 | 1.96 |
| Washington | 28 | 1.89 |
| West Virginia | 13 | 0.88 |
| Wisconsin | 28 | 1.89 |
| Wyoming | 0 | 0 |
| Total | 1478 | 100 |
References
- Coleman-Jensen, A.; Rabbitt, M.; Gregory, C.; Singh, A. Household Food Security in the United States in 2018; ERR-270; USDA, Economic Research Service: Washington, DC, USA, 2019.
- Marmot, M. Social determinants of health inequalities. Lancet 2005, 365, 1099–1104. [Google Scholar] [CrossRef]
- Gundersen, C.; Ziliak, J.P. Food Insecurity And Health Outcomes. Health Aff. (Millwood) 2015, 34, 1830–1839. [Google Scholar] [CrossRef]
- Martinez, S.M.; Frongillo, E.A.; Leung, C.; Ritchie, L. No food for thought: Food insecurity is related to poor mental health and lower academic performance among students in California’s public university system. J. Health Psychol. 2018. [Google Scholar] [CrossRef]
- Pooler, J.A.; Hartline-Grafton, H.; DeBor, M.; Sudore, R.L.; Seligman, H.K. Food Insecurity: A Key Social Determinant of Health for Older Adults. J. Am. Geriatr. Soc. 2019, 67, 421–424. [Google Scholar] [CrossRef]
- Cheung, H.C.; Shen, A.; Oo, S.; Tilahun, H.; Cohen, M.J.; Berkowitz, S.A. Food Insecurity and Body Mass Index: A Longitudinal Mixed Methods Study, Chelsea, Massachusetts, 2009–2013. Prev. Chronic Dis. 2015, 12, E125. [Google Scholar] [CrossRef][Green Version]
- Leung, C.W.; Epel, E.S.; Ritchie, L.D.; Crawford, P.B.; Laraia, B.A. Food insecurity is inversely associated with diet quality of lower-income adults. J. Acad. Nutr. Diet. 2014, 114, 1943–1953.e2. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Berkowitz, T.S.Z.; Meigs, J.B.; Wexler, D.J. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005–2012. PLoS ONE 2017, 12, e0179172. [Google Scholar] [CrossRef]
- Bruening, M.; Dinour, L.M.; Chavez, J.B.R. Food insecurity and emotional health in the USA: A systematic narrative review of longitudinal research. Public Health Nutr. 2017, 20, 3200–3208. [Google Scholar] [CrossRef]
- Kaiser Family Foundation. State Data and Policy Actions to Address Coronavirus. 2020. Available online: https://www.kff.org/health-costs/issue-brief/state-data-and-policy-actions-to-address-coronavirus/ (accessed on 12 April 2020).
- Niles, M.T.; Bertmann, F.; Morgan, E.H.; Wentworth, T.; Biehl, E.; Neff, R. Food Access and Security during Coronavirus: A Vermont Study. In College of Agriculture and Life Sciences Faculty Publications; University of Vermont: Burlington, VT, USA, 2020. [Google Scholar]
- Fitzpatrick, K.; Harris, C.; Drawve, G. Assessing U.S. Food Insecurity in the United States during COVID-19 Pandemic. 2020. Available online: https://fulbright.uark.edu/departments/sociology/research-centers/community-family-institute/_resources/community-and-family-institute/revised-assessing-food-insecurity-brief.pdf (accessed on 28 April 2020).
- Bauer, L. The COVID-19 Crisis Has Already Left Too Many Children Hungry in America. 6 May 2020. Available online: https://www.brookings.edu/blog/up-front/2020/05/06/the-covid-19-crisis-has-already-left-too-many-children-hungry-in-america/ (accessed on 7 May 2020).
- Litman, L.; Robinson, J.; Abberbock, T. TurkPrime.com: A versatile crowdsourcing data acquisition platform for the behavioral sciences. Behav. Res. Methods 2017, 49, 433–442. [Google Scholar] [CrossRef]
- Zimmerman, M.; Kerr, S. How should the severity of depression be rated on self-report depression scales? Psychiatry Res. 2019, 280, 112512. [Google Scholar] [CrossRef]
- Yap, K.; Grisham, J.R. Unpacking the construct of emotional attachment to objects and its association with hoarding symptoms. J. Behav. Addict. 2019, 8, 249–258. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Lahne, J.; Raj, M.; Insolera, N.; Lavelle, F.; Dean, M. Food Agency in the United States: Associations with Cooking Behavior and Dietary Intake. Nutrients 2020, 12, 877. [Google Scholar] [CrossRef]
- Skrzynski, C.; Creswell, K.G.; Bachrach, R.L.; Chung, T. Social discomfort moderates the relationship between drinking in response to negative affect and solitary drinking in underage drinkers. Addict. Behav. 2018, 78, 124–130. [Google Scholar] [CrossRef]
- Minen, M.T.; Jalloh, A.; Begasse de Dhaem, O.; Seng, E.K. Behavioral Therapy Preferences in People with Migraine. Headache 2020, 32, 196–200. [Google Scholar] [CrossRef]
- Bickel, G.; Nord, M.; Price, C.; Hamilton, W.; Cook, J. Guide to Measuring Household Food Security; Revised 2000; U.S. Department of Agriculture: Washington, DC, USA, 2000. Available online: https://www.fns.usda.gov/guide-measuring-household-food-security-revised-2000 (accessed on 27 May 2020).
- United States Department of Agriculture Economic Research Service. Definition of Food Insecurity. 2019. Available online: https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/definitions-of-food-security/ (accessed on 13 April 2020).
- Aljazeera. Lockdowns, Closures: How Is Each US State Handling Coronavirus? 2020. Available online: https://www.aljazeera.com/news/2020/03/emergencies-closures-states-handling-coronavirus-200317213356419.html (accessed on 14 April 2020).
- Sachs-Ericsson, N.; Schatschneider, C.; Blazer, D.G. Perception of Unmet Basic Needs as a Predictor of Physical Functioning Among Community-Dwelling Older Adults. J. Aging Health 2006, 18, 852–868. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Seligman, H.K.; Choudhry, N.K. Treat or eat: Food insecurity, cost-related medication underuse, and unmet needs. Am. J. Med. 2014, 127, 303–310.e3. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Meigs, J.B.; DeWalt, D.; Seligman, H.K.; Barnard, L.S.; Bright, O.J.; Schow, M.; Atlas, S.J.; Wexler, D.J. Material need insecurities, control of diabetes mellitus, and use of health care resources: Results of the Measuring Economic Insecurity in Diabetes study. JAMA Intern. Med. 2015, 175, 257–265. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Basu, S.; Meigs, J.B.; Seligman, H.K. Food Insecurity and Health Care Expenditures in the United States, 2011–2013. Health Serv. Res. 2018, 53, 1600–1620. [Google Scholar] [CrossRef]
- Long, H.; Dam, A.V. America is in a depression, the challenge now is to make it short-lived. The Washington Post, 9 April 2020. [Google Scholar]
- Martin, M.S.; Maddocks, E.; Chen, Y.; Gilman, S.E.; Colman, I. Food insecurity and mental illness: Disproportionate impacts in the context of perceived stress and social isolation. Public Health 2016, 132, 86–91. [Google Scholar] [CrossRef]
- Leung, C.W.; Wolfson, J.A.; Lahne, J.; Barry, M.R.; Kasper, N.; Cohen, A.J. Associations between Food Security Status and Diet-Related Outcomes among Students at a Large, Public Midwestern University. J. Acad. Nutr. Diet. 2019, 119, 1623–1631. [Google Scholar] [CrossRef]
- Smith, T.M.; Colon-Ramos, U.; Pinard, C.A.; Yaroch, A.L. Household food insecurity as a determinant of overweight and obesity among low-income Hispanic subgroups: Data from the 2011–2012 California Health Interview Survey. Appetite 2016, 97, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Laraia, B.A.; Kushel, M.B. Food insecurity is associated with chronic disease among low-income NHANES participants. J. Nutr. 2009, 140, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Gundersen, C.; Cook, J.; Laraia, B.; Johnson, M.A. Food insecurity and health across the lifespan. Adv. Nutr. 2012, 3, 744–745. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Aid, Relief, and Economic Security (CARES) Act. Public Law 116-136. 2020.
- Families First Coronavirus Response Act. Public Law 116-127. 2020.
- Kulish, N. ‘Never Seen Anything Like It’: Cars Line up for Miles at Food Banks. 2020. Available online: https://www.nytimes.com/2020/04/08/business/economy/coronavirus-food-banks.html?referringSource=articleShare (accessed on 14 April 2020).
- United States Department of Agriculture Food and Nutrition Service. Find Meals for Kids When Schools are Closed. 2020. Available online: https://www.fns.usda.gov/meals4kids (accessed on 14 April 2020).
- Nord, M.; Prell, M. Food Security Improved Following the 2009 ARRA Increase in SNAP Benefits; ERR-116; Report No. 1477-2017-4088; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2011.
- Anderson, M.; Perrin, A.; Jiang, J.L.; Kumar, M. 10% of Americans Don’t Use the Internet. Who Are They? Pew Research Center. 2019. Available online: https://www.pewresearch.org/fact-tank/2019/04/22/some-americans-dont-use-the-internet-who-are-they/ (accessed on 27 May 2020).


| Overall | Food Security Status | p-Value | ||||
|---|---|---|---|---|---|---|
| High | Marginal | Low | Very Low | |||
| n (%) a | n (%) b | n (%) b | n (%) b | n (%) b | ||
| Total | 1478 (100) | 532 (36) | 290 (20) | 256 (17) | 400 (27) | |
| Age | ||||||
| 18–39 | 635 (43) | 168 (26) | 116 (18) | 140 (22) | 211 (33) | <0.001 |
| 40–59 | 429 (29) | 152 (35) | 88 (21) | 62 (14) | 127 (30) | |
| ≥60 | 414 (28) | 212 (51) | 86 (21) | 54 (13) | 62 (15) | |
| Sex | ||||||
| Male | 733 (50) | 285 (39) | 135 (18) | 128 (17) | 185 (25) | 0.100 |
| Female | 745 (50) | 247 (33) | 155 (21) | 128 (17) | 215 (29) | |
| Race/ethnicity | ||||||
| NH White | 990 (67) | 384 (39) | 185 (19) | 160 (16) | 261 (26) | 0.026 |
| NH Black | 161 (11) | 47 (29) | 36 (22) | 36 (22) | 42 (26) | |
| Hispanic | 186 (13) | 55 (30) | 35 (19) | 39 (21) | 57 (31) | |
| Asian | 73 (5) | 24 (33) | 23 (32) | 11 (15) | 15 (21) | |
| Other | 68 (5) | 22 (32) | 11 (16) | 10 (15) | 25 (37) | |
| Household Size | ||||||
| 1–3 people | 1113 (75) | 416 (37) | 219 (20) | 177 (16) | 301 (27) | 0.054 |
| ≥4 people | 365 (25) | 116 (32) | 71 (19) | 79 (22) | 99 (27) | |
| Marital Status | ||||||
| Single, never married | 564 (38) | 199 (35) | 108 (19) | 118 (21) | 139 (35) | <0.001 |
| Married | 448 (30) | 180 (40) | 91 (20) | 68 (15) | 109 (24) | |
| Separated, divorced, widowed | 311 (21) | 124 (40) | 58 (19) | 43 (14) | 86 (28) | |
| Living with a partner | 150 (10) | 27 (18) | 32 (21) | 26 (17) | 65 (43) | |
| Children < 18 years in home | ||||||
| Yes | 445 (30) | 120 (27) | 85 (19) | 92 (21) | 148 (33) | <0.001 |
| No | 1033 (70) | 412 (40) | 205 (20) | 164 (16) | 252 (24) | |
| Income | ||||||
| <$35,000/year | 894 (60) | 297 (33) | 175 (20) | 165 (18) | 257 (29) | 0.015 |
| $35,000 ≤ $59,000/year | 418 (28) | 162 (39) | 75 (18) | 69 (17) | 112 (27) | |
| ≥$59,000/year | 166 (11) | 73 (44) | 40 (24) | 22 (13) | 31 (19) | |
| Education | ||||||
| High school/GED | 439 (30) | 122 (28) | 83 (19) | 91 (21) | 143 (33) | <0.001 |
| Some college | 524 (35) | 197 (38) | 104 (29) | 75 (14) | 148 (28) | |
| College/grad degree | 515 (35) | 213 (41) | 103 (20) | 90 (17) | 109 (21) | |
| Employment status | ||||||
| Full time job (hourly or salary) | 408 (29) | 139 (34) | 68 (17) | 81 (20) | 120 (29) | 0.002 |
| Part time job (hourly or salary) | 239 (17) | 83 (35) | 51 (21) | 41 (17) | 64 (27) | |
| Not working, looking for work | 197 (14) | 58 (29) | 38 (19) | 38 (19) | 63 (32) | |
| Not working, not looking for work | 415 (30) | 186 (45) | 86 (21) | 55 (13) | 88 (21) | |
| Home-maker | 141 (10) | 46 (33) | 27 (19) | 21 (15) | 47 (33) | |
| Student | ||||||
| Yes | 95 (6) | 29 (31) | 26 (27) | 20 (21) | 20 (21) | 0.106 |
| No | 1383 (94) | 503 (36) | 264 (19) | 236 (17) | 380 (27) | |
| Home ownership | ||||||
| Rent | 744 (50) | 201 (27) | 144 (19) | 154 (21) | 245 (33) | <0.001 |
| Own | 538 (43) | 287 (45) | 128 (20) | 89 (14) | 134 (21) | |
| Other | 96 (7) | 44 (46) | 18 (19) | 13 (14) | 21 (22) | |
| Health insurance | ||||||
| None | 231 (16) | 68 (29) | 40 (17) | 35 (15) | 88 (38) | <0.001 |
| Yes, through work | 260 (18) | 97 (37) | 45 (17) | 57 (22) | 61 (23) | |
| Yes, Medicare | 437 (30) | 189 (43) | 83 (19) | 73 (17) | 92 (21) | |
| Yes, Medicaid | 338 (23) | 91 (27) | 73 (22) | 55 (16) | 119 (35) | |
| Yes, other | 212 (14) | 87 (41) | 49 (23) | 35 (17) | 40 (19) | |
| Political party affiliation | ||||||
| Republican | 396 (27) | 174 (44) | 76 (19) | 50 (13) | 96 (24) | 0.004 |
| Democrat | 594 (40) | 190 (32) | 124 (21) | 115 (19) | 165 (28) | |
| Independent | 488 (33) | 168 (34) | 90 (18) | 91 (19) | 139 (28) | |
| SNAP benefits | ||||||
| No | 1065 (72) | 452 (42) | 207 (19) | 182 (17) | 224 (21) | <0.001 |
| Yes | 413 (28) | 80 (19) | 83 (20) | 74 (18) | 176 (43) | |
| Region of residence | ||||||
| Northeast | 273 (18) | 90 (33) | 57 (21) | 59 (22) | 67 (25) | 0.406 |
| Midwest | 332 (22) | 127 (38) | 69 (21) | 47 (14) | 89 (27) | |
| South | 542 (37) | 196 (36) | 95 (18) | 97 (18) | 154 (28) | |
| West | 331 (22) | 119 (36) | 69 (21) | 53 (16) | 90 (27) | |
| Overall (n = 655) | Food Security Status | p-Value | ||||
|---|---|---|---|---|---|---|
| High n = 225 (34%) | Marginal n = 120 (18%) | Low n = 124 (19%) | Very Low n = 186 (28%) | |||
| n (%) a | n (%) b | n (%) b | n (%) b | n (%)b | ||
| What is your workplace doing to adjust to COVID-19? c | ||||||
| Nothing, proceeding as normal | 152 (23) | 64 (42) | 27 (18) | 25 (16) | 36 (24) | 0.004 |
| Employees encouraged to work at home | 69 (11) | 15 (22) | 17 (25) | 17 (25) | 20 (29) | |
| Employees must work at home | 69 (11) | 17 (25) | 14 (20) | 16 (23) | 22 (32) | |
| Essential employees must come in, others work from home | 58 (9) | 29 (50) | 5 (9) | 14 (24) | 10 (32) | |
| Hours are reduced | 79 (12) | 20 (25) | 11 (14) | 17 (22) | 31 (39) | |
| Temporarily closed | 131 (20) | 44 (34) | 27 (21) | 21 (16) | 39 (30) | |
| Closed and I have been laid off | 25 (4) | 11 (44) | 6 (24) | 3 (12) | 5 (20) | |
| Busier, employees working extra hours | 47 (7) | 21 (45) | 9 (19) | 8 (17) | 9 (19) | |
| If you or someone in your family becomes ill with COVID-19, what do you expect will happen regarding your job? c (check all that apply) | ||||||
| I will be able to stay home without using sick or vacation days | 162 (26) | 71 (44) | 31 (19) | 31 (19) | 29 (18) | 0.003 |
| I will be able to use sick days to stay home without losing income | 123 (19) | 55 (45) | 22 (18) | 23 (19) | 23 (19) | 0.022 |
| I will be able to use vacation days to stay home without losing income | 74 (12) | 27 (36) | 11 (15) | 17 (23) | 19 (26) | 0.573 |
| I do not have sick days so if I am not able to work I will lose income | 260 (41) | 72 (28) | 49 (19) | 45 (17) | 94 (36) | 0.002 |
| I will have to go into work even if I am sick | 33 (5) | 6 (18) | 6 (18) | 8 (24) | 13 (39) | 0.180 |
| If I miss too many days of work I could lose my job | 61 (10) | 11 (18) | 9 (15) | 9 (15) | 32 (52) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolfson, J.A.; Leung, C.W. Food Insecurity and COVID-19: Disparities in Early Effects for US Adults. Nutrients 2020, 12, 1648. https://doi.org/10.3390/nu12061648
Wolfson JA, Leung CW. Food Insecurity and COVID-19: Disparities in Early Effects for US Adults. Nutrients. 2020; 12(6):1648. https://doi.org/10.3390/nu12061648
Chicago/Turabian StyleWolfson, Julia A., and Cindy W. Leung. 2020. "Food Insecurity and COVID-19: Disparities in Early Effects for US Adults" Nutrients 12, no. 6: 1648. https://doi.org/10.3390/nu12061648
APA StyleWolfson, J. A., & Leung, C. W. (2020). Food Insecurity and COVID-19: Disparities in Early Effects for US Adults. Nutrients, 12(6), 1648. https://doi.org/10.3390/nu12061648