Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research

 , , , ,
, , , , 
Abstract
1. Introduction
Study Purpose
2. Materials and Methods
2.1. Scoping Review Step 1: Identify Restaurant Menu Labeling Policies
2.2. Scoping Review—Step 2: Identify Evidence for Restaurant Menu Labeling Effects
2.2.1. Identifying the Research Question
2.2.2. Identifying Relevant Studies
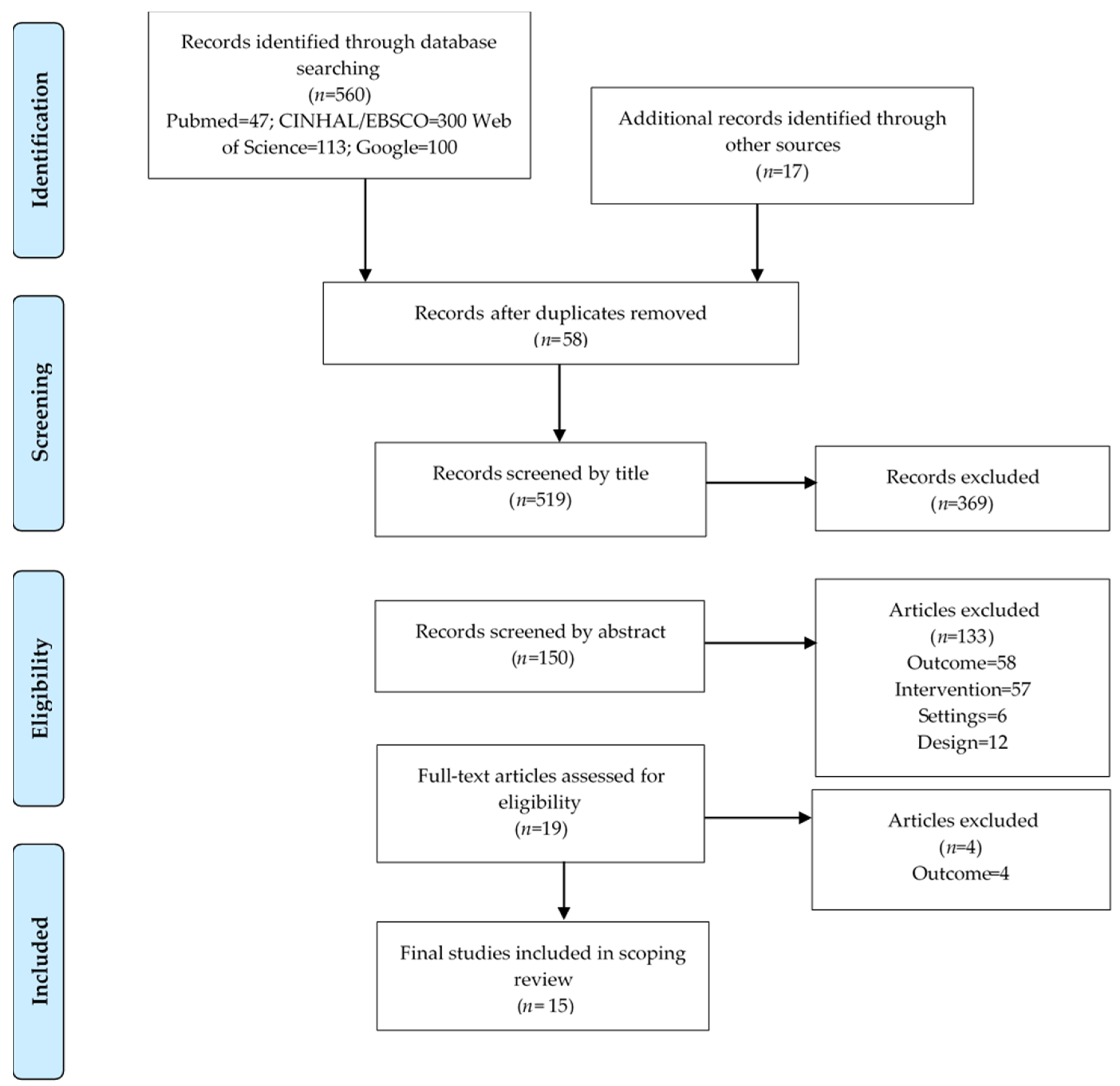
2.2.3. Study Selection
2.2.4. Charting the Data
2.2.5. Collating, Summarizing and Reporting Results
3. Results
3.1. Scoping Review Results for Step 1: Identify Restaurant Menu Labeling Policies
3.2. Scoping Review Results for Step 2: Identify Evidence for Restaurant Menu Labeling Effects
3.2.1. Changes to Menu Items by Food and Beverage Category
3.2.2. Changes in the Nutritional Composition by Nutrients of Concern
3.2.3. Newly Introduced Menu Items Versus Common or Regular Menu Items
4. Discussion
4.1. Implications for Policy, Practice, and Research
4.2. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M. Relationship between shifts in food system dynamics and acceleration of the global nutrition transition. Nutr. Rev. 2017, 75, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.P.; Ng, S.W.; Popkin, B.M. Resistant to the recession: Low-income adults’ maintenance of cooking and away-from-home eating behaviors during times of economic turbulence. Am. J. Public Health 2014, 104, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Vandevijvere, S.; Jaacks, L.M.; Monteiro, C.A.; Moubarac, J.C.; Girling-Butcher, M.; Lee, A.C.; Pan, A.; Bentham, J.; Swinburn, B. Global trends in ultraprocessed food and drink product sales and their association with adult body mass index trajectories. Obes. Rev. 2019, 20 (Suppl. 2), 10–19. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K.; Graubard, B.I. A prospective study of frequency of eating restaurant prepared meals and subsequent 9-year risk of all-cause and cardiometabolic mortality in US adults. PLoS ONE 2018, 13, e0191584. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.A.; Aggarwal, A.; Vermeylen, F.; Drewnowski, A. Consumption Frequency of Foods Away from Home Linked with Higher Body Mass Index and Lower Fruit and Vegetable Intake among Adults: A Cross-Sectional Study. J. Environ. Public Health 2016, 2016, 3074241. [Google Scholar] [CrossRef]
- Alturki, H.A.; Brookes, D.S.; Davies, P.S. Comparative evidence of the consumption from fast-food restaurants between normal-weight and obese Saudi schoolchildren. Public Health Nutr. 2018, 21, 2280–2290. [Google Scholar] [CrossRef]
- Tambalis, K.D.; Panagiotakos, D.B.; Psarra, G.; Sidossis, L.S. Association between fast-food consumption and lifestyle characteristics in Greek children and adolescents; results from the EYZHN (National Action for Children’s Health) programme. Public Health Nutr. 2018, 21, 3386–3394. [Google Scholar] [CrossRef] [PubMed]
- Llanaj, E.; Ádány, R.; Lachat, C.; D’Haese, M. Examining food intake and eating out of home patterns among university students. PLoS ONE 2018, 13, e0197874. [Google Scholar] [CrossRef]
- Goffe, L.; Rushton, S.; White, M.; Adamson, A.; Adams, J. Relationship between mean daily energy intake and frequency of consumption of out-of-home meals in the UK National Diet and Nutrition Survey. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 131. [Google Scholar] [CrossRef]
- Nielsen. Nielsen Global Out-of-Home Dining Survey; The Nielsen Company: New York, NY, USA, 2015. [Google Scholar]
- Kuo, T.; Jarosz, C.J.; Simon, P.; Fielding, J.E. Menu labeling as a potential strategy for combating the obesity epidemic: A health impact assessment. Am. J. Public Health 2009, 99, 1680–1686. [Google Scholar] [CrossRef]
- Cawley, J.; Wen, K. Policies to Prevent Obesity and Promote Healthier Diets: A Critical Selective Review. Clin. Chem. 2018, 64, 163–172. [Google Scholar] [CrossRef] [PubMed]
- World health Organization. Follow-up to the Political Declaration of the High-Level Meeting of the General Assembly WHA66.10. Annex: Global Action Plan for Prevention and Control of Non-Communicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Tackling NCDs: ‘Best Buys’ and other Recommended Interventions for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Bleich, S.N.; Economos, C.D.; Spiker, M.L.; Vercammen, K.A.; VanEpps, E.M.; Block, J.P.; Elbel, B.; Story, M.; Roberto, C.A. A Systematic Review of Calorie Labeling and Modified Calorie Labeling Interventions: Impact on Consumer and Restaurant Behavior. Obesity 2017, 25, 2018–2044. [Google Scholar] [CrossRef] [PubMed]
- Bruemmer, B.; Krieger, J.; Saelens, B.E.; Chan, N. Energy, saturated fat, and sodium were lower in entrees at chain restaurants at 18 months compared with 6 months following the implementation of mandatory menu labeling regulation in King County, Washington. J. Acad. Nutr. Diet. 2012, 112, 1169–1176. [Google Scholar] [CrossRef] [PubMed]
- Muth, M.K.; Karns, S.A.; Mancino, L.; Todd, J.E. How Much Can Product Reformulation Improve Diet Quality in Households with Children and Adolescents? Nutrients 2019, 11, 618. [Google Scholar] [CrossRef]
- Federici, C.; Detzel, P.; Petracca, F.; Dainelli, L.; Fattore, G. The impact of food reformulation on nutrient intakes and health, a systematic review of modelling studies. BMC Nutr. 2019, 5, 2. [Google Scholar] [CrossRef]
- Bleich, S.N.; Moran, A.J.; Jarlenski, M.P.; Wolfson, J.A. Higher-Calorie Menu Items Eliminated in Large Chain Restaurants. Am. J. Prev. Med. 2018, 54, 214–220. [Google Scholar] [CrossRef]
- Kraak, V.; Englund, T.; Misyak, S.; Serrano, E. Progress Evaluation for the Restaurant Industry Assessed by a Voluntary Marketing-Mix and Choice-Architecture Framework that Offers Strategies to Nudge American Customers toward Healthy Food Environments, 2006–2017. Int. J. Environ. Res. Public Health 2017, 760. [Google Scholar] [CrossRef]
- Kraak, V.; Rincon-Gallardo Patino, S.; Renukuntla, D.; Kim, E. Progress Evaluation for Transnational Restaurant Chains to Reformulate Products and Standardize Portions to Meet Healthy Dietary Guidelines and Reduce Obesity and Non-Communicable Disease Risks, 2000-2018: A Scoping and Systematic Review to Inform Policy. Int. J. Environ. Res. Public Health 2019, 2732. [Google Scholar] [CrossRef]
- Fernandes, A.C.; Oliveira, R.C.; Proenca, R.P.; Curioni, C.C.; Rodrigues, V.M.; Fiates, G.M. Influence of menu labeling on food choices in real-life settings: A systematic review. Nutr. Rev. 2016, 74, 534–548. [Google Scholar] [CrossRef]
- Harnack, L.J.; French, S.A. Effect of point-of-purchase calorie labeling on restaurant and cafeteria food choices: A review of the literature. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 51. [Google Scholar] [CrossRef]
- Kiszko, K.M.; Martinez, O.D.; Abrams, C.; Elbel, B. The influence of calorie labeling on food orders and consumption: A review of the literature. J. Community Health 2014, 39, 1248–1269. [Google Scholar] [CrossRef] [PubMed]
- Littlewood, J.A.; Lourenco, S.; Iversen, C.L.; Hansen, G.L. Menu labelling is effective in reducing energy ordered and consumed: A systematic review and meta-analysis of recent studies. Public Health Nutr. 2016, 19, 2106–2121. [Google Scholar] [CrossRef] [PubMed]
- Long, M.W.; Tobias, D.K.; Cradock, A.L.; Batchelder, H.; Gortmaker, S.L. Systematic review and meta-analysis of the impact of restaurant menu calorie labeling. Am. J. Public Health 2015, 105, e11–e24. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, S.E.; Cooper, M.; Mansfield, E.D. The influence of menu labeling on calories selected or consumed: A systematic review and meta-analysis. J. Acad. Nutr. Diet. 2014, 114, 1375–1388.e15. [Google Scholar] [CrossRef] [PubMed]
- Swartz, J.J.; Braxton, D.; Viera, A.J. Calorie menu labeling on quick-service restaurant menus: An updated systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 135. [Google Scholar] [CrossRef] [PubMed]
- VanEpps, E.M.; Roberto, C.A.; Park, S.; Economos, C.D.; Bleich, S.N. Restaurant Menu Labeling Policy: Review of Evidence and Controversies. Curr. Obes. Rep. 2016, 5, 72–80. [Google Scholar] [CrossRef]
- Sarink, D.; Peeters, A.; Freak-Poli, R.; Beauchamp, A.; Woods, J.; Ball, K.; Backholer, K. The impact of menu energy labelling across socioeconomic groups: A systematic review. Appetite 2016, 99, 59–75. [Google Scholar] [CrossRef] [PubMed]
- Cantu-Jungles, T.M.; McCormack, L.A.; Slaven, J.E.; Slebodnik, M.; Eicher-Miller, H.A. A Meta-Analysis to Determine the Impact of Restaurant Menu Labeling on Calories and Nutrients (Ordered or Consumed) in U.S. Adults. Nutrients 2017, 1088. [Google Scholar] [CrossRef]
- Crockett, R.A.; King, S.E.; Marteau, T.M.; Prevost, A.T.; Bignardi, G.; Roberts, N.W.; Stubbs, B.; Hollands, G.J.; Jebb, S.A. Nutritional labelling for healthier food or non-alcoholic drink purchasing and consumption. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Sucharew, H.; Macaluso, M. Progress Notes: Methods for Research Evidence Synthesis: The Scoping Review Approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef]
- World Health Organization. Global Database on the Implementation of Nutrition Action (GINA); World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Hawkes, C.; Jewell, J.; Allen, K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: The NOURISHING framework. Obes. Rev. 2013, 14, 159–168. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund International. NOURISHING Framework; World Cancer Research Fund International: London, UK, 2017. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Daudt, H.M.L.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [PubMed]
- Doody, O.; Bailey, M.E. Setting a research question, aim and objective. Nurse Res. 2016, 23, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Moola, S.; Munn, Z.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Tufanaru, C.; Qureshi, R.; Mattis, P.; Mu, P. Conducting systematic reviews of association (etiology): The Joanna Briggs Institute’s approach. Int. J. Evid. -Based Healthc. 2015, 13, 163–169. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar]
- Veritas Health. Covidence Systematic Review Software; Melbourne, Australia. 2019. Available online: https://www.medianet.com.au/releases/162025 (accessed on 15 February 2020).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- The Johana Briggs Institute. Checklist for Analytical Obesravtional Studies; The University of Adelaide: Adelaide, Australia, 2017. [Google Scholar]
- Ryan, R. Cochrane Consumer and Communication Review Group: Data Synthesis and Analysis. 2013. Available online: https://cccrg.cochrane.org/sites/cccrg.cochrane.org/files/public/uploads/Analysis.pdf (accessed on 15 January 2020).
- Castleberry, A.; Nolen, A. Thematic analysis of qualitative research data: Is it as easy as it sounds? Curr. Pharm. Teach. Learn. 2018, 10, 807–815. [Google Scholar] [CrossRef]
- Scourboutakos, M.J.; Orr, S.; Hobin, E.; Murphy, S.A.; Manson, H.; L’Abbé, M.R. Assessing the Early Impact of Menu-Labeling on Calories in Chain Restaurants in Ontario, Canada. Am. J. Prev. Med. 2019, 56, e195–e203. [Google Scholar] [CrossRef]
- Bleich, S.N.; Wolfson, J.A.; Jarlenski, M.P.; Block, J.P. Restaurants With Calories Displayed On Menus Had Lower Calorie Counts Compared To Restaurants Without Such Labels. Health Aff. 2015, 34, 1877–1884. [Google Scholar] [CrossRef]
- Bleich, S.N.; Wolfson, J.A.; Jarlenski, M.P. Calorie Changes in Large Chain Restaurants: Declines in New Menu Items but Room for Improvement. Am. J. Prev. Med. 2016, 50, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Wolfson, J.A.; Jarlenski, M.P. Calorie changes in large chain restaurants from 2008 to 2015. Prev. Med. 2017, 100, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Soto, M.J.; Dunn, C.G.; Moran, A.J.; Block, J.P. Calorie and nutrient trends in large U.S. chain restaurants, 2012–2018. PLoS ONE 2020, 15, e0228891. [Google Scholar] [CrossRef] [PubMed]
- Namba, A.; Auchincloss, A.; Leonberg, B.L.; Wootan, M.G. Exploratory analysis of fast-food chain restaurant menus before and after implementation of local calorie-labeling policies, 2005–2011. Prev. Chronic Dis. 2013, 10, E101. [Google Scholar] [CrossRef] [PubMed]
- Petimar, J.; Zhang, F.; Cleveland, L.P.; Simon, D.; Gortmaker, S.L.; Polacsek, M.; Bleich, S.N.; Rimm, E.B.; Roberto, C.A.; Block, J.P. Estimating the effect of calorie menu labeling on calories purchased in a large restaurant franchise in the southern United States: Quasi-experimental study. BMJ 2019, 367, l5837. [Google Scholar] [CrossRef] [PubMed]
- Saelens, B.E.; Chan, N.L.; Krieger, J.; Nelson, Y.; Boles, M.; Colburn, T.A.; Glanz, K.; Ta, M.L.; Bruemmer, B. Nutrition-labeling regulation impacts on restaurant environments. Am. J. Prev. Med. 2012, 43, 505–511. [Google Scholar] [CrossRef][Green Version]
- Tran, A.; Moran, A.; Bleich, S.N. Calorie changes among food items sold in U.S. convenience stores and pizza restaurant chains from 2013 to 2017. Prev. Med. Rep. 2019, 15, 100932. [Google Scholar] [CrossRef]
- Wu, H.W.; Sturm, R. Changes in the energy and sodium content of main entrees in US chain restaurants from 2010 to 2011. J. Acad. Nutr. Diet. 2014, 114, 209–219. [Google Scholar] [CrossRef]
- Theis, D.R.Z.; Adams, J. Differences in energy and nutritional content of menu items served by popular UK chain restaurants with versus without voluntary menu labelling: A cross-sectional study. PLoS ONE 2019, 14, e0222773. [Google Scholar] [CrossRef]
- Wellard-Cole, L.; Goldsbury, D.; Havill, M.; Hughes, C.; Watson, W.L.; Dunford, E.K.; Chapman, K. Monitoring the changes to the nutrient composition of fast foods following the introduction of menu labelling in New South Wales, Australia: An observational study. Public Health Nutr. 2018, 21, 1194–1199. [Google Scholar] [CrossRef]
- Wellard-Cole, L.; Hooper, A.; Watson, W.L.; Hughes, C. Nutrient composition of Australian fast-food and fast-casual children’s meals available in 2016 and changes in fast-food meals between 2010 and 2016. Public Health Nutr. 2019, 22, 2981–2988. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Statistics and Information Systems. Definition of Regional Grouping; Global Health Estimates: Geneva, Switzerland, 2020. [Google Scholar]
- Food and Drug Administration. Food Labeling: Revision of the Nutrition and Supplement Facts Labels. In Final Rule. Fed. Regist; 2016; 81, pp. 33741–33999. Available online: https://pubmed.ncbi.nlm.nih.gov/27236870/ (accessed on 15 January 2020).
- Obesity Policy Coalition. Policy Brief: Menu Kilojoule Labelling in Chain Food Outlets in Australia; 2018. Available online: https://www.opc.org.au/downloads/policy-briefs/menu-kj-labelling-in-chain-food-outlets-in-australia.pdf (accessed on 15 January 2020).
- Legislative Assembly of the Province of Ontario, Canada. Healthy Menu Choices Act, 2015 (Bill 45, Making Healthier Choices Act) O.Reg.50/16; Canada, G.o., Ed.; Ontario, Canada. 2017. Available online: https://labbelab.utoronto.ca/wp-content/uploads/2017/12/Evidence-Document-ON-reformat-Nov-8.pdf (accessed on 15 January 2020).
- Food Safety Awareness and Applied Nutrition Unit; Department, F.S. Calorie Labeling in Food Service Establishments. In Requirements and Guidelines; Dubai Municipality: Dubai, United Arab Emirates, 2019. Available online: http://www.foodsafe.ae/pic/requirements/Calorie_Labeling_in_Food_Service_Establishments_Requirements_and_Guidelines_1907.pdf (accessed on 15 January 2020).
- Ministry of Health Malaysia. National Plan of Action for Nutrition of Malaysia (2016–2025); Nutrition Division, M.o.H.M., Ed.; Putrajaya, Malaysia. 2016. Available online: http://nutrition.moh.gov.my/wp-content/uploads/2016/12/NPANM_III.pdf (accessed on 15 January 2020).
- A’Ali, M. Bahrain News: Proposal for Restaurants and Cafés to Display Calories in Meals. GDNonline, 22 September. 2018. Available online: http://www.gdnonline.com/Details/402212/Proposal-for-restaurants-and-caf%E9s-to-display-calories-in-meals (accessed on 15 February 2020).
- Department of Health. Consultation with Food Businesses on the Introduction of Mandatory Calorie Posting on Menus; Health, G.o.i.D.o., Ed.; 2020. Available online: https://www.gov.ie/en/consultation/d9bfcc-consultation-with-food-businesses-on-the-introduction-of-mandatory-c/ (accessed on 15 January 2020).
- British Nutrition Foundation. The Public Health Responsibility Deal; Scotland. 2018. Available online: https://www.nutrition.org.uk (accessed on 15 January 2020).
- Department of health and Social Care. Mandating Energy Labelling of Food and Drink in Out-of-Home Settings; IA No:13009; Department of health and Social Care: UK. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/751532/impact-assessment-for-consultation-on-calorie-labelling-outside-of-the-home.pdf (accessed on 15 January 2020).
- Secretary of State for Health and Social Care. Government Response to the House of Commons Health and Social Care Select Committee Report on Childhood Obesity: Time for Action, Eight Report of Session 2017-19; London, UK. 2019. Available online: https://www.parliament.uk/documents/commons-committees/Health/Correspondence/2017-19/Childhood-obesity-Government-Response-to-eighth-report-17-19.pdf (accessed on 15 January 2020).
- Dame Sally Davies. Time to Solve Childhood Obesity. An Independent Report by the Chief Medical Officer. Annex A—Recommendations for Action. 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/837907/cmo-special-report-childhood-obesity-october-2019.pdf (accessed on 15 January 2020).
- Center for Disease Control and Prevention. CDC Policy Process: Definition of Policy. In Office of the Associate Director for Policy; 2015. Available online: https://www.cdc.gov/policy/analysis/process/index.html (accessed on 15 January 2020).
- Scourboutakos, M.J.; Semnani-Azad, Z.; L’Abbe, M.R. Added sugars in kids’ meals from chain restaurants. Prev. Med. Rep. 2016, 3, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Scourboutakos, M.J.; L’Abbe, M.R. Restaurant menus: Calories, caloric density, and serving size. Am. J. Prev. Med. 2012, 43, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, L.P.; Simon, D.; Block, J.P. Federal calorie labelling compliance at US chain restaurants. Obes. Sci. Pract. 2019. [Google Scholar] [CrossRef]
- Wellard, L.; Havill, M.; Hughes, C.; Watson, W.L.; Chapman, K. The availability and accessibility of nutrition information in fast food outlets in five states post-menu labelling legislation in New South Wales. Aust. N. Z. J. Public Health 2015, 39, 546–549. [Google Scholar] [CrossRef]
- Sacks, G.; Robinson, E. Inside Our Quick Service Restaurants: Assessment of Company Policies and Commitments Related to Obesity Prevention and Nutrition; Deakin University: Melbourne, Australia, 2018. [Google Scholar]
- Popkin, B.; Reardon, T. Obesity and the food system transformation in Latin America. Obes. Rev. 2018, 19, 1028–1064. [Google Scholar] [CrossRef]
- Nielsen. Battle of the Bulge & Nutrition Labels. Healthy Eating Trends Around the World; The Nielsen Company: New York, NY, USA, 2012. [Google Scholar]
- Healthy Weight Commitment Foundation. Food and Beverage Manufacterers Pledging to Reduce Annual Calories By 1.5 Trillion By 2015; CISION PR Newswire: London, UK, 2010. [Google Scholar]
- Children’s Food & Beverage Advertising Initiative. Advertising Initiative Category-Specific Uniform Nutrition Criteria; Council of Better Business Bureaus, Inc.: Arlington, VA, USA, 2018. [Google Scholar]
- Mantilla Herrera, A.M.; Crino, M.; Erskine, H.E.; Sacks, G.; Ananthapavan, J.; Mhurchu, C.N.; Lee, Y.Y. Cost-Effectiveness of Product Reformulation in Response to the Health Star Rating Food Labelling System in Australia. Nutrients 2018, 10, 614. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Hooton, W.; Critchley, J.; Capewell, S.; Collins, M.; Mason, H.; Guzman-Castillo, M.; O’Flaherty, M. Cost-effectiveness analysis of eliminating industrial and all trans fats in England and Wales: Modelling study. J. Public Health 2017, 39, 574–582. [Google Scholar] [CrossRef]
- Shangguan, S.; Afshin, A.; Shulkin, M.; Ma, W.; Marsden, D.; Smith, J.; Saheb-Kashaf, M.; Shi, P.; Micha, R.; Imamura, F.; et al. A Meta-Analysis of Food Labeling Effects on Consumer Diet Behaviors and Industry Practices. Am. J. Prev. Med. 2019, 56, 300–314. [Google Scholar] [CrossRef]
- Wilcox, M.L.; Mason, H.; Fouad, F.M.; Rastam, S.; al Ali, R.; Page, T.F.; Capewell, S.; O’Flaherty, M.; Maziak, W. Cost-effectiveness analysis of salt reduction policies to reduce coronary heart disease in Syria, 2010–2020. Int. J. Public Health 2015, 60 (Suppl. 1), S23–S30. [Google Scholar] [CrossRef]
- Watkins, D.A.; Olson, Z.D.; Verguet, S.; Nugent, R.A.; Jamison, D.T. Cardiovascular disease and impoverishment averted due to a salt reduction policy in South Africa: An extended cost-effectiveness analysis. Health Policy Plan 2016, 31, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Mason, H.; Shoaibi, A.; Ghandour, R.; O’Flaherty, M.; Capewell, S.; Khatib, R.; Jabr, S.; Unal, B.; Sozmen, K.; Arfa, C.; et al. A cost effectiveness analysis of salt reduction policies to reduce coronary heart disease in four Eastern Mediterranean countries. PLoS ONE 2014, 9, e84445. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, M.; Soler, L.G. Food reformulation and nutritional quality of food consumption: An analysis based on households panel data in France. Eur. J. Clin. Nutr. 2018, 72, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.M.; Bloem, M.Z.; Zheng, M.; Catterall, E.; Thomas, B.; Veerman, L.; Wu, J.H. The Impact of Policies to Reduce trans Fat Consumption: A Systematic Review of the Evidence. Curr. Dev. Nutr. 2017, 1. [Google Scholar] [CrossRef] [PubMed]
- Hendry, V.L.; Almiron-Roig, E.; Monsivais, P.; Jebb, S.A.; Neelon, S.E.; Griffin, S.J.; Ogilvie, D.B. Impact of regulatory interventions to reduce intake of artificial trans-fatty acids: A systematic review. Am. J. Public Health 2015, 105, e32–e42. [Google Scholar] [CrossRef] [PubMed]
- Griffith, R.; O’Connell, M.; Smith, K. The Importance of Product Reformulation Versus Consumer Choice in Improving Diet Quality. Economica 2017, 84, 34–53. [Google Scholar] [CrossRef]
- Leroy, P.; Requillart, V.; Soler, L.G.; Enderli, G. An assessment of the potential health impacts of food reformulation. Eur. J. Clin. Nutr. 2016, 70, 694–699. [Google Scholar] [CrossRef]
- Kraak, V.I.; Englund, T.; Misyak, S.; Serrano, E.L. A novel marketing mix and choice architecture framework to nudge restaurant customers toward healthy food environments to reduce obesity in the United States. Obes. Rev. 2017, 18, 852–868. [Google Scholar] [CrossRef]
- Roberto, C.A.; Khandpur, N. Improving the design of nutrition labels to promote healthier food choices and reasonable portion sizes. Int. J. Obes. 2014, 38 (Suppl. 1), S25–S33. [Google Scholar] [CrossRef]
- Kerins, C.; McHugh, S.; McSharry, J.; Reardon, C.M.; Hayes, C.; Perry, I.J.; Geaney, F.; Seery, S.; Kelly, C. Barriers and facilitators to implementation of menu labelling interventions from a food service industry perspective: A mixed methods systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 48. [Google Scholar] [CrossRef]
- Burke-Garcia, A.; Scally, G. Trending now: Future directions in digital media for the public health sector. J. Public Health 2014, 36, 527–534. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Laws and Universal Health Coverage; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Information Note on COVID-19 and NCDs; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]


{kind=link}
| PEO Framework | MeSH Terms and Synonyms |
|---|---|
| Population | “Restaurants”[MeSH] OR “Food Services”[MeSH] OR “Food Supply”[MeSH] OR “Fast Foods”[MeSH] OR “Food Industry”[MeSH] OR “Food-Processing Industry”[MeSH] “Chain restaurant*” OR restaurant or “food retail” OR “food services*” OR “food supply” OR “food supplies” OR “fast food*” NOT Schools [MeSH] AND |
| Exposure | “Policy”[MeSH] OR “Nutrition Policy”[MeSH] OR “Public Policy”[MeSH] OR “Health Policy”[MeSH] OR “Government Regulation”[MeSH] OR “Legislation” [Publication Type] OR “Legislation, Food”[MeSH] OR “Voluntary Programs”[MeSH] OR “Mandatory Programs”[MeSH] OR “Patient Protection and Affordable Care Act”[MeSH] OR “Mandatory Policy” OR “Voluntary Policy” OR “Self-regulation” OR “Nutrition policies” OR Guideline OR “Food Policy” AND “Food Labeling”[MeSH] OR “Product Labeling”[MeSH] OR “Food product label*” OR “Menu label*” OR “Restaurant label*” OR “Restaurant label” OR “Restaurant menu label*” OR “Food calories” OR “Nutrient label*” OR “Food content” NOT “Food Packaging” |
| Outcome | “Food”[MeSH] OR “Beverages”[MeSH] OR “Food and Beverages”[MeSH] OR “Food Ingredients”[MeSH] OR “food product*” OR “Fast food” AND “Food Quality”[MeSH] OR “Food, Formulated”[MeSH] OR “Serving Size”[MeSH] OR “Portion Size”[MeSH] OR “Food reformulation” OR “Reduce* Portion*” OR “Reduce* size*” OR “Product reformulation” |
| * World Region | Scoping Review—Step 1 | Scoping Review—Step 2 |
|---|---|---|
| Identify Policies (Policies = 11) | Identify Evidence (Studies n = 15) | |
| Africa | None identified (n = 0) | None identified |
| Americas (n = 2) | Canada and US (n = 2) | Canada (n = 1): Scourboutakos et al. (2019) [47]. US (n = 11): Bleich et al. (2015) [48], Bleich et al. (2016) [49], Bleich et al. (2017) [50], Bleich et al. (2018) [19], Bleich et al. (2020) [51], Bruemmer et al. (2012) [16], Namba et al. (2013) [52], Petimar et al. (2019) [53], Saelens et al. (2012) [54], Tran et al. (2019) [55], Wu et al. (2014) [56] |
| South-East Asia | None identified (n = 0) | None identified |
| Europe | Ireland and the UK (n = 2) | UK (n = 1): Theis et al. (2019) [57] |
| Eastern Mediterranean | Bahrain, Saudi Arabia, United Arab Emirates (n = 3) | None identified |
| Western Pacific | Australia, Malaysia, South Korea, Taiwan (n = 4) | Australia (n = 2): Wellard-Cole et al. (2018) [58], Wellard-Cole et al. (2019) [59]. |
| Country, Year | Policy Type | Action |
|---|---|---|
| Australia, 2011–2018 | Mandatory, four states and one territory | Restaurant chains with ≥20 outlets in the state, or 50 or more across the country, are required to present the energy content (kilojoules) and include a daily intake statement on menus and menu boards. Similar food businesses are invited to voluntarily implement menu labeling. |
| States of New South Wales, 2011: Food regulation 2011 | ||
| Australia Capital Territory, 2012: Amendments to Food Regulation 2002 | ||
| Australia, South Australia, 2012: Amendments to Food Regulation 2002 | ||
| Australia, Queensland, 2017: Amendments to Food Act 2006 | ||
| Australia, Victoria, 2018: Amendment to Food Act 1984 | ||
| Bahrain, 2010 | Voluntary, national | The Nutrition Section of the Ministry of Health recommends that fast-food chain restaurants display nutrients per serving, including calories, fat, protein, carbohydrates, salt/sodium, and sugar. |
| Canada, Ontario, 2017 | Mandatory, province | In 2015, Ontario’s Healthy Menu Choices Act, part of the Making Healthier Choices Act (Bill 45) in the Ontario Regulation 50/16, requires food service establishments with 20 or more businesses to depict calories for menu items on paper and electronic menus, menu boards, drive-through menus, menu applications, and advertisements or promotional flyers. |
| Ireland, 2015 | Mandatory, national | In 2015, the Health Service Executive approved the implementation of Calorie Posting Policy across health services in all food and beverage facilities (i.e., restaurants, coffee shops, catering services, and vending machines). |
| Malaysia, 2008 | Voluntary, national | In 2008, the Malaysian government released voluntary guidelines for the advertising and nutrition labeling of restaurant chains to display nutrient information on the menu items (i.e., calories, carbohydrates, protein, fat, and sodium for food and total sugar for beverages). |
| Saudi Arabia, 2018 | Mandatory, national | In 2018, the Saudi Food and Drug Authority launched mandatory measures that require calorie labeling on menu items for all food facilities, including cashier desks, menu boards, table menus, drive-through menus, phone, and web applications. |
| South Korea, 2010 | Mandatory, national | In 2010, the South Korean government enforced through the Special Act on Safety Control of Children’s Dietary Life that restaurants with more than 100 outlets are required to report energy, total sugars, protein, saturated fat and sodium on the menus |
| Taiwan, 2015 | Mandatory, national | From 2015, the Taiwanese Act Governing Food Safety and Sanitation that regulates business chains (i.e., convenience stores, drink vendors, and fast-food restaurants) requires the labeling of the sugar and caffeine content of prepared-when-ordered drinks. |
| United Arab Emirates, 2020 | Mandatory, state/emirate | The 2017–2020 National Nutrition Agenda for Dubai requires food retailers to display the calorie content of menu items and a daily intake statement, effective 1 January 2020. |
| United Kingdom, 2011 | Voluntary, national | From 2011–2015, the Out of Home Calorie Labelling pledge, part of the government’s Responsibility Deal (2010 to 2015), established for businesses with 45 or more food establishments the need to provide calorie information on menus in England, Scotland, and Wales. In 2012, the Food Standards Agency worked with Northern Ireland and the local food industry to encourage calorie labeling on menus |
| United States, 2010-2018 | Mandatory, national | In 2010, Section 4205 of the Affordable Care Act, Public Law 111-148 (HR 3590), mandated that restaurant chains and other food retail establishments (i.e., convenience stores, coffee shops, grocery stores, cafeterias) with 20 or more locations would be required to disclose calories and daily intake statements on menus and menu boards and make other nutrition information available to customers upon request. The law became effective on 1 May 2018. |
| Author Year | Country | Study Design | Purpose | Sample | Setting | Data Sources | Menu Items | Nutrition Composition | New vs. Common Menu Items | Effect * |
|---|---|---|---|---|---|---|---|---|---|---|
| Bleich et al. 2015 [48] | USA | Observational, longitudinal | Compare differences in calorie counts from menu labeling, 2012–2014 | 23,066 menu items from 66 | Restaurant chains | MenuStat | Food and beverages | Calories. Average per item calories restaurants with voluntary labeling was significantly lower than those without the labeling (−286 kcal: 232 vs. 519) | Lower calorie content for new menu items introduced in 2013 (−182 kcal: 263 vs. 445; and in 2014 (−110 kcal: 309 vs. 419) | Positive |
| Bleich et al. 2016 [49] | USA | Observational, longitudinal | Describe trends in calories available in US chain restaurants from 2012 to 2014 to better understand restaurant-driven changes | 23, 066 menu items over 3 years in 66 large chain restaurants | QSR, FCR and FSR chains | MenuStat | Appetizers and sides, main courses, desserts, toppings, beverages, and children’s menu items. New food, beverages, and children’s menu items all had fewer mean calories relative to old menu items (66, 47, 43, and 35 fewer calories, respectively) | Calories. Predicted mean per-item calories in new main course items in 2013 had 85 fewer calories relative to old main course items in 2012. Calories declined in pizza (−120 calories), sandwiches (−82 calories), and salads (−68 calories) | Menu items newly introduced in 2013 and 2014 had significantly fewer calories relative to items on the menu in 2012 (2012 vs. 2013: −71 calories; 2012 vs. 2014, −69 calories) | Positive |
| Bleich et al. 2017 [50] | USA | Observational, longitudinal | Understand trends in calories in chain restaurants before and after the passage of the menu labeling rule | 19,391 menu items from chain restaurants | QSR, FCR and FSR chains | MenuStat | Appetizers and sides, fried potatoes, main courses, toppings, beverages, and children’s menu items. Largest differences were found for toppings that reduced from 93 kcal in 2008 to 84 kcal in 2015 | Calories. Overall calories declined from 327 kcal in 2008 to 318 kcal in 2015 | - | Positive |
| Bleich et al. 2018 [19] | USA | Observational, longitudinal | Compare mean calories for items that remained on restaurant menus with items dropped from the menu | 27,238 menu items from restaurant chains | Restaurant chains | MenuStat | Appetizers and sides, main courses, desserts, and beverages | Calories. Items that were dropped had 71 more calories | Items that stayed on the menu in all years had fewer calories than those items that were dropped (448 calories vs. 733 calories) | Positive |
| Bleich et al. 2020 [51] | USA | Observational, longitudinal | Update calorie and nutrient trends 2012–2018 of menu items across restaurants | 28,238 menu items from chain restaurants | Fast-food, fast-casual, and full-service restaurant chains | MenuStat | Appetizers and sides, main courses, fried potatoes, desserts and baked goods | Calories, saturated fat, sodium, sugar and protein.Significant changes in food (sugar −0.67 g) and beverages (unsaturated fat −1.8 g, protein −2.7 g). Trend in years: calories −120 kcals (−25%), saturated fat −3.4 g (−41%), unsaturated fat −4.5 g (−37%), non-sugar carbohydrates −10.3 g (−40%), and protein −4.3 g (−25%) | Significant changes were found among all newly introduced items. It is possible that the declines in calories and nutrients in this study are related to local or national nutrition policies | Positive |
| Bruemmer et al. 2012 [16] | USA | Observational, longitudinal | Evaluated changes in energy, saturated fat, and sodium content of entrees 6 and 18 months that occurred following the implementation of menu labeling regulation | 37 chains | QSR and FSR chains | Personnel visited and recorded energy content from menu labels, and websites | Entrée items. Calorie content decline in overall average entrée calories (41 fewer calories post labeling; 73 fewer calories at full-service restaurants and 19 fewer at QSR) when comparing 6 and 18 months post labeling | Calories and sodium. Decrease in energy, saturated fat, and sodium content between the two study periods following implementation of menu regulation for menu items that were present at both time periods. Saturated fat and sodium levels decreased significantly across all chains and SD chains | - | Positive |
| Namba et al. 2013 [52] | USA | Observational, case-control | Evaluate the effect of menu labeling on menu offerings over 7 years, from 2005 through 2011 | 3887 menu items from chain restaurants | Top 50 QSR chains | Restaurant websites | Entrées, sides, and children’s entrées. Case restaurants increased the proportion of healthier entrées after labeling regulations: from 13% during years 2005 through 2008, up to 20% by 2011 with a mean difference of 5% pre–post 2008 in cases relative to controls. The prevalence of healthier side dishes was higher among case restaurants than controls (23% vs. 15%, respectively). Healthier children’s entrées at case restaurants were higher | Calories. Regression models found no statistically significant changes over time in nutrient averages and no statistically significant differences between the nutritional averages of case and control restaurants | 3 of 5 labeled restaurants improved their offerings. Control restaurants had a lower proportion of healthier items than cases. 2 of 5 showed no improvement and even launched new options, that increased average calories by over 20% and cholesterol by almost 140% | Mixed |
| Petimar et al. 2019 [53] | USA | Observational, longitudinal | Evaluate calorie labeling in mean calories purchased, pre-2015–2017 and post menu labeling implementation period 2017–2018 | 59 restaurants | Restaurants | Menustat | Entrées, sides, sugar-sweetened beverages | Calories. The top 50 menu offerings purchased in 2017–18 had a median of 350 calories (interquartile range 440–760) pre-implementation and a median of 340 calories (440–760) post-implementation. | - | Positive |
| Saelens et al. 2012 [54] | USA | Experimental, quasi-experimental | Examine changes in restaurants from before to after nutrition-labeling regulation in a regulated versus a nonregulated county of Washington state | Top 10 QSR chains | QSR and independent restaurant chains | Nutrition Environment Measures Survey Restaurant (NEMS-R) | Healthy vs. Unhealthy based on 10 items examined by the Nutrition Environment Measures Surveys—Restaurant version (NEMS-R) | The healthfulness of children’s menus improved modestly over time, but not differentially by county. Availability of reduced portions decreased in the regulated county | - | No effect |
| Scourboutakos et al. 2019 [47] | Canada | Observational, longitudinal | Investigate the early impact of Canada’s mandatory menu labeling legislation on calorie levels in foods offered on chain restaurant menus before, leading up to, and at the point-of-implementation, 2010 - 2017 | 2988 foods sold by 28 restaurant chains | QSR and FSR chains | Menu-FLIP database | Entrées, pizza, breakfast foods, side dishes, baked goods/desserts, kids’ foods | Calories. The average calories per serving on restaurant menus increased from 306 (SD = 6) kcal to 346 (SD = 6) kcal, between 2010 and 2017. An increase in serving size, from 155 (SD = 3) to 172 (SD = 3) grams, between 2010 and 2017. Calorie density (kcal per 100 g) did not significantly differ between 2010 and 2017. Significant increase in serving sizes among sit-down restaurants of 12 g per serving between 2010 and 2017 | Overall, new foods introduced in 2017 were significantly higher in calories per serving compared with those introduced in 2016. New foods introduced in 2017 had significantly higher serving sizes compared with new foods in 2013 and 2016 | No effect |
| Theis et al. 2019 [57] | UK | Observational, cross-sectional | Determine whether there are differences in the energy and nutritional content of menu items served by UK restaurants vs. without voluntary menu labeling | 100 UK chain restaurants | QSR and FSR chains ranked by sales | Restaurant websites | Appetizers and sides, baked goods, beverages, burgers, desserts, fried potatoes, mains, pizza, salads, sandwiches, soup, toppings, and ingredients. Main dishes (i.e., pizza and sandwich) had less sugar and salt. Toppings and ingredients had less fat and protein than items from restaurants without menu labeling. Baked goods items from restaurants with menu labeling had, more energy, fat, saturated fat, sugar but protein and more salt | Calories, saturated fat, sodium, sugar, carbohydrates, and protein. Restaurants with menu labeling had 45% less fat (beta coefficient 0.55; 95% CI 0.32 to 0.96) and 60% less salt (beta coefficient 0.40; 95% CI 0.18 to 0.92) | - | Mixed |
| Tran et al. 2019 [55] | USA | Observational, longitudinal | Describe trends in calories among food items sold in US convenience stores and pizza restaurant chains from 2013 to 2017 | 1522 food items from convenience stores and 2085 items from pizza restaurant chains | Pizza restaurant chains | MenuStat | Appetizers and sides, main courses, and desserts. Lower calories among items that stayed on the menu compared to items dropped (overall: −60 kcal; appetizers and sides: −200 kcal p < 0.001; main courses: −50 kcal p = 0.03; desserts −60 kcal) | Calories. Reduced calories in menu items (−56 kcal: 390 kcal in 2013 vs. 334 kcal in 2017), appetizers (−230 kcal: 367 kcal in 2013 vs. 137 kcal in 2017) | Calories were lower among items that stayed on the menu compared to items dropped. Lower-calorie pizza options were introduced, but no significant changes | Positive |
| Wellard-Cole et al. 2018 [58] | Australia | Observational, longitudinal | Examine the energy content of Australian fast-food menu items before and after menu board labeling | 522 menu items from fast-food chains | 5 of the largest Australian QSR chains | Fast-food websites | Breakfast, burgers, desserts, chicken and seafood, salads, sides, sandwiches and wraps | Calories. No differences in energy per serving items, content per 100 g for burgers was higher after implementation (1040 vs. 999 kJ/100 g before implementation,) | No effect | |
| Wellard-Cole et al. 2019 [59] | Australia | Observational, longitudinal | Investigate the nutrient composition of children’s meals offers at fast-food chains, compare with children’s daily requirements and recommendations and determine if results have changed prior to the implementation of menu labeling | 289 children’s meals | Australian QSR and FCR chains | Fast-food websites, email and telephone requests, and personnel visits | Children’s meals per restaurant chain | Calories, saturated fat, sodium and sugar. Minimal changes were found. Meals from Chicken Treat reduced mean energy (−600 kJ/serving), saturated fat (−9·4 g/serving) and Na (−121 mg/serving), and from Red Rooster (−410 kJ/serving) and sugars (−11·8 g/serving), KFC reduced saturated fat (−10·5 g/serving). However, meals from Hungry Jack’s increased in energy (345 kJ/serving), sugars (8·6 g/serving), and Na (187 mg/serving) | - | Mixed |
| Wu et al. 2014 [56] | USA | Observational, longitudinal | Track changes in the energy and sodium content of US chain restaurant main entrées between spring 2010 (when the Affordable Care Act was passed) and spring 2011 | 25,256 regular menu entrées from 213 restaurant brands | Top US chain restaurants based on 2008 sales | Restaurant websites, and email request | Regular menu entrées and children’s menu entrées | Calories and sodium. 26 restaurants reduced sodium in newly added items by 707 mg on average. Significant decrease in mean energy (−40 kcal. Two upscale restaurants with children’s menu entrées had a significant increase in mean energy (46 kcal). Items removed from children’s menus were 36 kcal lower | Higher-sodium items decreased by 70 mg (p = 0.027) in added vs. removed items on regular menus. Calories decreased by 57 kcal (p = 0.047) for added vs. removed children’s entrées | Mixed |
| Food System Actors | Recommended Actions |
|---|---|
| Governments | Provide enough support for food service restaurant businesses to facilitate a low-cost, sustainable, and accountable policy. Policies could be improved to incentivize more holistic menu changes by requiring the display of energy and other nutrients of concern, including fats, sodium, and added sugars for each item offered by restaurants. |
| World Health Organization | Issue recommendations for governments and transnational restaurants and their franchise businesses, and food service providers to harmonize, standardize, and apply a universal set of healthy dietary standards across countries and regions. |
| Restaurant businesses | Make commitments and increase transparency to meet product profile targets based on WHO- or expert-recommended guidelines |
| Private foundations | Provide technical assistance and incentivize transnational restaurant chains to implement, monitor, and evaluate menu labeling policies across countries and regions. |
| Researchers | Expand external monitoring and evaluation efforts of transnational restaurant chains to assess their compliance with WHO- or expert-recommended guidelines across countries and regions. Examine how digital technology could be used to leverage the effects of restaurant menu labeling policies. |
| Civil society organizations | Use social media advocacy, public awareness campaigns, and shareholder resolutions to encourage governments to implement comprehensive restaurant menu labeling policies for healthy product reformulation and portion size reduction for products sold to customers across countries and regions. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rincón-Gallardo Patiño, S.; Zhou, M.; Da Silva Gomes, F.; Lemaire, R.; Hedrick, V.; Serrano, E.; Kraak, V.I. Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research. Nutrients 2020, 12, 1544. https://doi.org/10.3390/nu12061544
Rincón-Gallardo Patiño S, Zhou M, Da Silva Gomes F, Lemaire R, Hedrick V, Serrano E, Kraak VI. Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research. Nutrients. 2020; 12(6):1544. https://doi.org/10.3390/nu12061544
Chicago/Turabian StyleRincón-Gallardo Patiño, Sofía, Mi Zhou, Fabio Da Silva Gomes, Robin Lemaire, Valisa Hedrick, Elena Serrano, and Vivica I. Kraak. 2020. "Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research" Nutrients 12, no. 6: 1544. https://doi.org/10.3390/nu12061544
APA StyleRincón-Gallardo Patiño, S., Zhou, M., Da Silva Gomes, F., Lemaire, R., Hedrick, V., Serrano, E., & Kraak, V. I. (2020). Effects of Menu Labeling Policies on Transnational Restaurant Chains to Promote a Healthy Diet: A Scoping Review to Inform Policy and Research. Nutrients, 12(6), 1544. https://doi.org/10.3390/nu12061544