Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults

 ,
,  ,
,  ,
,  ,
,  , , , ,
, , , , 
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of the Participants
3.2. MD Adherence, Lifestyle Habits and Nutritional Status
3.3. Subjective Well-Being
3.4. Variables Influence on the MD Adherence: Exploring the Relationship between MD and SWB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Radd-Vagenas, S.; Kouris-Blazos, A.; Singh, M.F.; Flood, V.M. Evolution of mediterranean diets and cuisine: Concepts and definitions. Asia Pac. J. Clin. Nutr. 2017, 26, 749–763. [Google Scholar] [CrossRef]
- Keys, A.; Menotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Bonanni, A.; Costanzo, S.; De Lucia, F.; Pounis, G.; Zito, F.; Donati, M.B.; de Gaetano, G.; Iacoviello, L. Adherence to a mediterranean diet is associated with a better health-related quality of life: A possible role of high dietary antioxidant content. BMJ Open 2013, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galilea-Zabalza, I.; Buil-Cosiales, P.; Salas-Salvado, J.; Toledo, E.; Ortega-Azorin, C.; Diez-Espino, J.; Vazquez-Ruiz, Z.; Zomeno, M.D.; Vioque, J.; Martinez, J.A.; et al. Mediterranean diet and quality of life: Baseline cross-sectional analysis of the predimed-plus trial. PLoS ONE 2018, 13, e0198974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, A.T.; Williams, P.; Tapsell, L. Reviewing the meanings of wellness and well-being and their implications for food choice. Perspect. Public Health 2010, 130, 282–286. [Google Scholar] [CrossRef] [PubMed]
- WHO. Constitution of Who: Principles. Available online: http://www.who.int/about/en/ (accessed on 23 November 2020).
- WHO. The European Health Report 2015. Targets and Beyond—Reaching New Frontiers in Evidence; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Cummins, R.; Mellor, D.; Stokes, M.; Lau, A.L.D. Measures of subjective well-being. In Rehabilitation and Health Assessment: Applying ICF Guidelines; Springer: Berlin/Heidelberg, Germany, 2010; pp. 409–426. [Google Scholar]
- OECD. OECD Guidelines on Measuring Subjective Well-Being; OECD: Paris, France, 2013. [Google Scholar]
- Godos, J.; Castellano, S.; Marranzano, M. Adherence to a mediterranean dietary pattern is associated with higher quality of life in a cohort of italian adults. Nutrients 2019, 11, 981. [Google Scholar] [CrossRef] [Green Version]
- Hendy, H.M. Which comes first in food–mood relationships, foods or moods? Appetite 2012, 58, 771–775. [Google Scholar] [CrossRef]
- Rahe, C.; Unrath, M.; Berger, K. Dietary patterns and the risk of depression in adults: A systematic review of observational studies. Eur. J. Nutr. 2014, 53, 997–1013. [Google Scholar] [CrossRef]
- Crichton, G.E.; Bryan, J.; Hodgson, J.M.; Murphy, K.J. Mediterranean diet adherence and self-reported psychological functioning in an australian sample. Appetite 2013, 70, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Jacka, F.N.; Cherbuin, N.; Anstey, K.J.; Butterworth, P. Dietary patterns and depressive symptoms over time: Examining the relationships with socioeconomic position, health behaviours and cardiovascular risk. PLoS ONE 2014, 9, e87657. [Google Scholar] [CrossRef] [PubMed]
- Gregório, M.J.; Rodrigues, A.M.; Eusébio, M.; Sousa, R.D.; Dias, S.; André, B.; Grønning, K.; Coelho, P.S.; Mendes, J.M.; Graça, P.; et al. Dietary patterns characterized by high meat consumption are associated with other unhealthy life styles and depression symptoms. Front Nutr. 2017, 4, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gougeon, L.; Payette, H.; Morais, J.; Gaudreau, P.; Shatenstein, B.; Gray-Donald, K. Dietary patterns and incidence of depression in a cohort of community-dwelling older canadians. J. Nutr. Health Aging 2015, 19, 431–436. [Google Scholar] [CrossRef]
- Orpana, H.; Vachon, J.; Pearson, C.; Elliott, K.; Smith, M.; Branchard, B. Correlates of well-being among canadians with mood and/or anxiety disorders. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2016, 36, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Durão, C.R.O.J.; de Almeida, M.D.V. Portugal e o padrão alimentar mediterrânico. Aliment. Hum. 2008, 14, 115–128. [Google Scholar]
- Pinto, I.; Franchini, B.; Rodrigues, S. Mediterranean Diet Food Guide Report; Ministério da Saúde. Direção-Geral da Saúde: Lisbon, Portugal, 2016; p. 30.
- García-Conesa, M.-T.; Philippou, E.; Pafilas, C.; Massaro, M.; Quarta, S.; Andrade, V.; Jorge, R.; Chervenkov, M.; Ivanova, T.; Dimitrova, D.; et al. Exploring the validity of the 14-item mediterranean diet adherence screener (medas): A cross-national study in seven european countries around the mediterranean region. Nutrients 2020, 12, 2960. [Google Scholar] [CrossRef]
- Schroder, H.; Fito, M.; Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Lamuela-Raventos, R.; Ros, E.; Salaverria, I.; Fiol, M.; et al. A short screener is valid for assessing mediterranean diet adherence among older spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- EU. Regulation (eu) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the Protection of Natural Persons with Regard to the Processing of Personal Data and on the Free Movement of such Data, and Repealing Directive 95/46/ec (General Data Protection Regulation); European Union: Brussels, Belgium, 2016. [Google Scholar]
- Marôco, J. Análise Estatística com SPSS Statistics; Report Number, Lda: Pêro Pinheiro, Portugal, 2018; p. 1005. [Google Scholar]
- Curtin, F.; Schulz, P. Multiple correlations and bonferroni’s correction. Biol. Psychiatry 1998, 44, 775–777. [Google Scholar] [CrossRef]
- Norušis, M.J. Ibm Spss Statistics 19 Statistical Procedures Companion; Prentice Hall: Upper Saddle River, NJ, USA, 2012. [Google Scholar]
- Martinez-Gonzalez, M.A.; Garcia-Arellano, A.; Toledo, E.; Salas-Salvado, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schroder, H.; Aros, F.; Gomez-Gracia, E.; et al. A 14-item mediterranean diet assessment tool and obesity indexes among high-risk subjects: The predimed trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic: Report of a Who Consultation; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Gregório, M.J.; Rodrigues, A.M.; Salvador, C.; Dias, S.S.; de Sousa, R.D.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Lopes, C.; Martínez-González, M.A.; et al. Validation of the telephone-administered version of the mediterranean diet adherence screener (medas) questionnaire. Nutrients 2020, 12, 1511. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Pêgo, C.; Rodrigues, J.; Costa, A.; Sousa, B. Adherence to the mediterranean diet in portuguese university students: Adesão à dieta mediterrânea em estudantes universitários portugueses. J. Biomed. Biopharm. Res. 2019, 16, 41–49. [Google Scholar] [CrossRef]
- Gregorio, M.J.; Rodrigues, A.M.; Graca, P.; de Sousa, R.D.; Dias, S.S.; Branco, J.C.; Canhao, H. Food insecurity is associated with low adherence to the mediterranean diet and adverse health conditions in portuguese adults. Front. Public Health 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Cuenca, A.I.; Garrido-Miguel, M.; Soriano-Cano, A.; Ferri-Morales, A.; Martínez-Vizcaíno, V.; Martín-Espinosa, N.M. Adherence to the mediterranean diet and its association with body composition and physical fitness in spanish university students. Nutrients 2019, 11, 2830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodoridis, X.; Grammatikopoulou, M.G.; Gkiouras, K.; Papadopoulou, S.E.; Agorastou, T.; Gkika, I.; Maraki, M.I.; Dardavessis, T.; Chourdakis, M. Food insecurity and mediterranean diet adherence among greek university students. Nutr. Metab. Cardiovasc. Dis. NMCD 2018, 28, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Papadaki, A.; Johnson, L.; Toumpakari, Z.; England, C.; Rai, M.; Toms, S.; Penfold, C.; Zazpe, I.; Martinez-Gonzalez, M.A.; Feder, G. Validation of the english version of the 14-item mediterranean diet adherence screener of the predimed study, in people at high cardiovascular risk in the uk. Nutrients 2018, 10, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, Y.J.; Lee, H.; Yoon, Y.; Kim, H.M.; Chu, S.H.; Lee, J.W. Development and validation of a questionnaire to measure adherence to the mediterranean diet in korean adults. Nutrients 2020, 12, 1102. [Google Scholar] [CrossRef] [Green Version]
- Marques-Vidal, P.; Waeber, G.; Vollenweider, P.; Bochud, M.; Stringhini, S.; Guessous, I. Sociodemographic and behavioural determinants of a healthy diet in switzerland. Ann. Nutr. Metab. 2015, 67, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Cavaliere, A.; De Marchi, E.; Banterle, A. Exploring the adherence to the mediterranean diet and its relationship with individual lifestyle: The role of healthy behaviors, pro-environmental behaviors, income, and education. Nutrients 2018, 10, 141. [Google Scholar] [CrossRef] [Green Version]
- Vitale, M.; Racca, E.; Izzo, A.; Giacco, A.; Parente, E.; Riccardi, G.; Giacco, R. Adherence to the traditional mediterranean diet in a population of south of italy: Factors involved and proposal of an educational field-based survey tool. Nutrients 2018, 7, 815. [Google Scholar] [CrossRef]
- Marventano, S.; Godos, J.; Platania, A.; Galvano, F.; Mistretta, A.; Grosso, G. Mediterranean diet adherence in the mediterranean healthy eating, aging and lifestyle (meal) study cohort. Int. J. Food Sci. Nutr. 2018, 69, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Kavouras, S.A.; Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Arnaoutis, G.; Skoumas, Y.; Stefanadis, C. Physical activity and adherence to mediterranean diet increase total antioxidant capacity: The attica study. Cardiol. Res. Pract. 2011, 2011, 248626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosaka, S.; Suda, K.; Gunawan, B.; Raksanagara, A.; Watanabe, C.; Umezaki, M. Urban-rural difference in the determinants of dietary and energy intake patterns: A case study in west java, indonesia. PLoS ONE 2018, 13, e0197626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conner, T.S.; Brookie, K.L. Let them eat fruit! The effect of fruit and vegetable consumption on psychological well-being in young adults: A randomized controlled trial. PLoS ONE 2017, 12, e0171206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujcic, R.; Oswald, A.J. Evolution of well-being and happiness after increases in consumption of fruit and vegetables. Am. J. Public Health 2016, 106, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- Pano, O.; Sayón-Orea, C.; Gea, A.; Bes-Rastrollo, M.; Martínez-González, M.Á.; Martínez, J.A. Nutritional determinants of quality of life in a mediterranean cohort: The sun study. Int. J. Environ. Res. Public Health 2020, 17, 3897. [Google Scholar] [CrossRef]
- Sánchez-Villegas, A.; Ruíz-Canela, M.; Gea, A.; Lahortiga, F.; Martínez-González, M.A. The association between the mediterranean lifestyle and depression. Clin. Psychol. Sci. 2016, 4, 1085–1093. [Google Scholar] [CrossRef]
- Maccagnan, A.; Wren-Lewis, S.; Brown, H.; Taylor, T. Wellbeing and society: Towards quantification of the co-benefits of wellbeing. Soc. Indic. Res. 2019, 141, 217–243. [Google Scholar] [CrossRef] [Green Version]
- Steptoe, A. Happiness and health. Annu. Rev. Public Health 2019, 40, 339–359. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, R.; Bassett, S.M.; Boughton, S.W.; Schuette, S.A.; Shiu, E.W.; Moskowitz, J.T. Psychological well-being and physical health: Associations, mechanisms, and future directions. Emot. Rev. 2018, 10, 18–29. [Google Scholar] [CrossRef]
- Zaragoza-Marti, A.; Ferrer-Cascales, R.; Hurtado-Sanchez, J.A.; Laguna-Perez, A.; Cabanero-Martinez, M.J. Relationship between adherence to the mediterranean diet and health-related quality of life and life satisfaction among older adults. J. Nutr. Health Aging 2018, 22, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Fancourt, D. Leading a meaningful life at older ages and its relationship with social engagement, prosperity, health, biology, and time use. Proc. Natl. Acad. Sci. USA 2019, 116, 1207–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.S.; Shiba, K.; Boehm, J.K.; Kubzansky, L.D. Sense of purpose in life and five health behaviors in older adults. Prev. Med. 2020, 139, 106172. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Subjective Well-Being—Statistics. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Subjective_well-being_-_statistics (accessed on 26 October 2020).

{kind=link}
| Total | Men | Women | p-Value (1) | |
|---|---|---|---|---|
| Gender (%/N) | 28.5/139 | 71.5/349 | ||
| Age (median (IQR)) | 34.0 (22.0) | 29.0 (27.0) | 36.0 (22.0) | 0.34 |
| (mean ± SD) | 36.5 ± 13.6 | 36.0 ± 15.3 | 36.6 ± 12.8 | |
| Age categories (%/N) | ||||
| <35 years | 50.8/249 | 57.6/80 | 48.1/168 | |
| 35–54 years | 35.5/174 | 21.6/30 | 41.3/144 | |
| ≥55 years | 13.7/67 | 20.9/29 | 10.6/37 | |
| Years in Portugal (%/N) | 0.417 | |||
| <10 years | 15.1/73 | 13.7/19 | 15.4/53 | |
| 10 to 20 years | 18.8/91 | 17.3/24 | 19.5/67 | |
| >20 years | 66.2/321 | 69.1/96 | 65.1/224 | |
| Marital status (%/N) | 0.115 | |||
| Single | 46.9/230 | 53.2/74 | 44.4/155 | |
| Married or analogous relationship | 45.1/221 | 38.8/54 | 47.6/166 | |
| Divorced or separated | 7.1/35 | 7.2/10 | 7.2/25 | |
| Widowed | 0.8/4 | 0.7/1 | 0.9/3 | |
| Education level (%/N) | 0.025 | |||
| Middle school | 3.5/17 | 5.0/7 | 2.9/10 | |
| High school | 26.5/130 | 37.4/52 | 22.3/78 | |
| University | 42.9/210 | 30.2/42 | 47.9/167 | |
| Master | 20.8/102 | 20.9/29 | 20.9/73 | |
| Ph.D. | 6.3/31 | 6.5/9 | 6.0/21 | |
| Employment status (%/N) | 0.003 | |||
| Student | 21.6/106 | 30.9/43 | 17.8/62 | |
| Employed | 70.0/343 | 62.6/87 | 73.2/255 | |
| Unemployed part of the year | 2.9/14 | 1.4/2 | 3.4/12 | |
| Unemployed or Housework | 2.5/11 | 1.4/2 | 2.6/9 | |
| Pensioner (retired, disability) | 2.7/13 | 3.6/5 | 2.3/8 | |
| Monthly net income (euros) (%/N) | 0.024 | |||
| <PSSI (2) | 1.5/6 | 0.0/0 | 2.1/6 | |
| ≥PSSI to 2× PSSI | 10.4/42 | 6.9/8 | 11.9/34 | |
| ≥2× PSSI to 4× PSSI | 37.6/152 | 35.3/41 | 38.8/111 | |
| ≥4× PSSI | 50.5/204 | 57.8/67 | 47.2/135 |
| Total | Men | Women | p-Value (1) | |
|---|---|---|---|---|
| Adherence to the Mediterranean Diet | ||||
| (MEDAS score) | <0.001 | |||
| (median (IQR) | 7.0 (3.0) | 7.0 (3.0) | 8.0 (3.0) | |
| (mean ± SD) | 7.4 ± 2.1 | 6.6 ± 2.2 | 7.7 ± 2.0 | |
| MEDAS categories (2) (%/N) | <0.001 | |||
| Low (≤5) | 20.2/99 | 33.1/46 | 14.9/52 | |
| Moderate (6–9) | 62.7/307 | 56.1/78 | 65.3/228 | |
| High (≥10) | 17.1/84 | 10.8/15 | 19.8/69 | |
| Lifestyle variables | ||||
| Meals per day (%/N) | <0.001 | |||
| ≤2 | 3.9/19 | 5.0/7 | 3.4/12 | |
| 3 | 21.0/103 | 33.6/47 | 16.0/56 | |
| 4 | 34.3/168 | 36.4/51 | 33.5/117 | |
| 5 | 31.0/152 | 16.4/23 | 36.7/128 | |
| ≥6 | 9.8/48 | 8.6/12 | 10.3/36 | |
| Smoking (%/N) | 0.005 | |||
| Non-smoker | 81.2/398 | 73.4/102 | 84.2/294 | |
| Smoker | 18.8/92 | 26.6/37 | 15.8/55 | |
| Physical Activity (%/N) | 0.811 | |||
| Not regular | 59.6/292 | 59.0/82 | 59.9/209 | |
| Regular | 40.4/198 | 41.0/57 | 40.1/140 | |
| Time spent in Nature (%/N) | 0.468 | |||
| Never or occasionally | 34.0/166 | 31.7/44 | 35.0/122 | |
| Sometimes | 35.9/176 | 36.7/51 | 35.5/124 | |
| Frequently or almost all the time | 30.1/148 | 31.7/44 | 29.5/103 | |
| Sociability: time with family and friends (%/N) | 0.78 | |||
| Never or occasionally | 7.3/36 | 10.8/15 | 6.0/21 | |
| Sometimes | 33.7/165 | 38.8/54 | 31.5/110 | |
| Frequently or almost all the time | 59.0/289 | 50.4/70 | 62.5/218 | |
| Sleeping (%/N) | 0.394 | |||
| Less than six hours per night | 14.7/72 | 17.3/24 | 13.8/48 | |
| Six to seven hours per night | 45.1/221 | 38.1/53 | 47.9/167 | |
| Seven to eight hours per night | 34.7/170 | 36.0/50 | 34.1/119 | |
| Eight to ten hours per night | 5.1/25 | 7.9/11 | 4.0/14 | |
| More than ten hours per night | 0.4/2 | 0.7/1 | 0.3/1 | |
| Total | Men | Women | p-Value (1) | |
|---|---|---|---|---|
| Pathologies (%/N) | 0.27 | |||
| Non diagnosed | 74.7/349 | 78.2/104 | 73.3/244 | |
| Diagnosed | 25.3/118 | 21.8/29 | 26.7/89 | |
| BMI (kg/m2) (median (IQR) /N) | 23.4 (5.2)/472 | 24.3 (4.7)/135 | 22.6 (5.1)/335 | <0.001 |
| (mean ± SD) | 24.2 ± 4.6 | 25.0 ± 3.7 | 23.9 ± 4.8 | |
| BMI categories (%/N) (2) | 0.004 | |||
| Underweight (<18.5) | 3.0/14 | 0.7/1 | 3.9/13 | |
| Normal (18.5; 24.9) | 62.7/296 | 54.1/73 | 66.3/222 | |
| Overweight (25; 29.9) | 23.5/111 | 36.3/49 | 18.5/62 | |
| Obese (≥30) | 10.8/51 | 8.9/12 | 11.3/38 |
| SWB Items (Scale 0 to 10) (1) (Median (IQR)/Mean ± sd) (Mean ± SD) | Total | Men | Women | p-Value |
|---|---|---|---|---|
| “Overall, to what extent do you feel that the things you do in your life are worthwhile?” | 8 (2) 7.7 ± 1.6 | 8 (2) 7.6 ± 1.8 | 8 (2) 7.8 ± 1.5 | 0.256 |
| “Overall, how satisfied are you with your life as a whole these days?” | 7 (1) 7.3 ± 1.5 | 7 (1) 7.1 ± 1.6 | 7 (1) 7.3 ± 2.3 | 0.467 |
| “How happy did you feel during the last week?” | 7 (2) 6.9 ± 1.9 | 7 (2) 6.9 ± 2.1 | 7(2) 6.9 ± 1.9 | 0.948 |
| “How worried did you feel during the last week?” | 6 (4) 5.8 ± 2.5 | 6 (4) 5.7 ± 2.9 | 6 (4) 5.9 ± 2.5 | 0.545 |
| “Did you feel depressed during the last week?” | 3 (4) 3.3 ± 2.8 | 3 (6) 3.2 ± 2.9 | 3 (4) 3.3 ± 2.7 | 0.736 |
| 5-item SWB index (2) | 7 (2) 6.5 ± 1.5 | 7 (2) 6.5 ± 1.7 | 7 (2) 6.6 ± 1.5 | 0.892 |
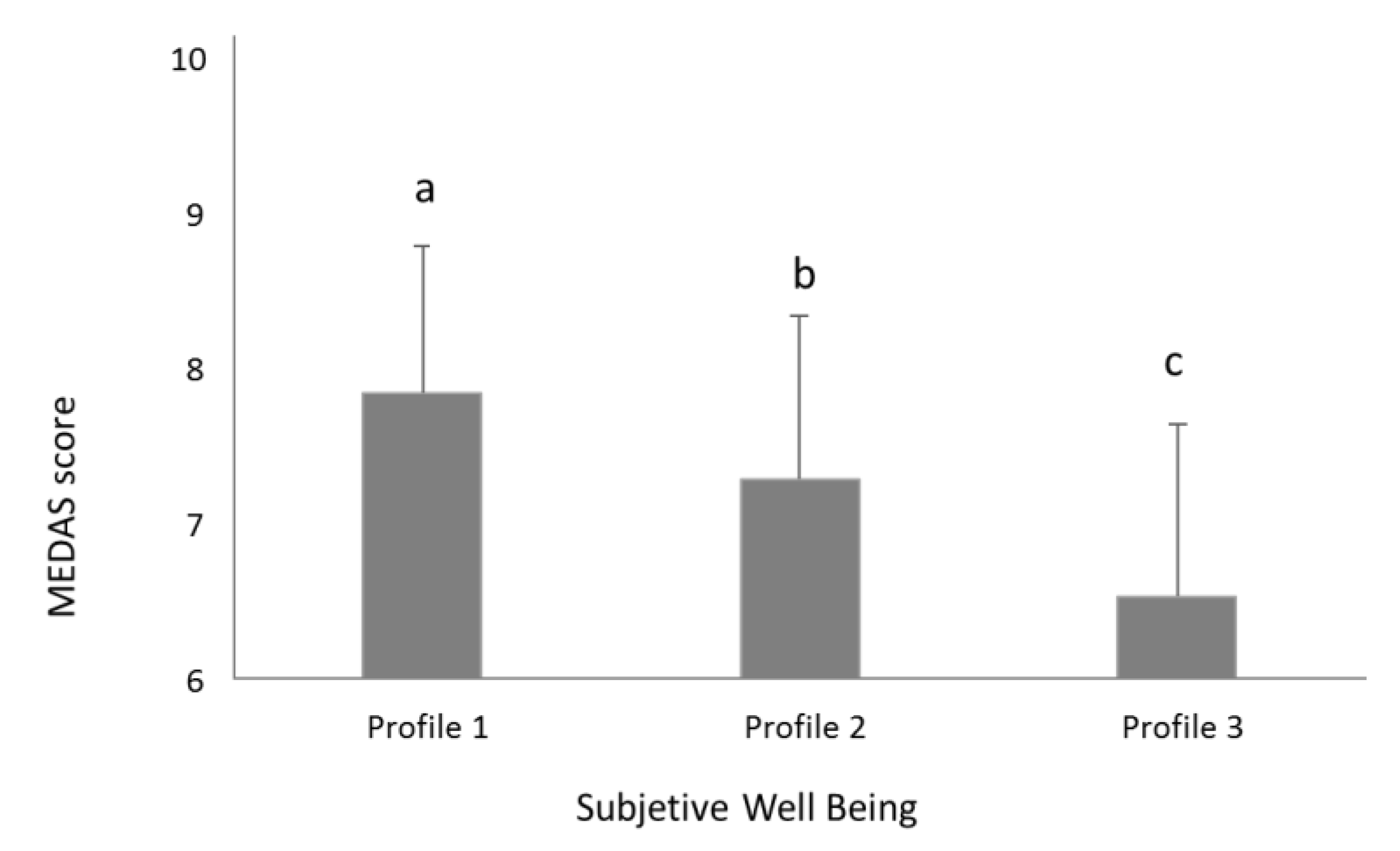
| SWB Profiles N (%) | Profile1 164 (31.4%) | Profile 2 275 (56.1%) | Profile 3 61 (12.4%) |
|---|---|---|---|
| Worthwhile life (Mean ± SD) | 8.9 ± 0.9 a | 7.7 ± 1.0 b | 5.1 ± 1.7 c |
| Overall life satisfaction (Mean ± SD) | 8.4 ± 1.0 a | 7.2 ± 1.0 b | 4.7 ± 1.6 c |
| Feeling of happiness (Mean ± SD) | 8.5 ± 0.9 a | 6.7 ± 1.4 b | 3.8 ± 1.5 c |
| Feeling of worry (1) (Mean ± SD) | 6.0 ± 2.4 a | 3.5 ± 2.1 b | 2.6 ± 2.0 c |
| Feeling of depression (1) (Mean ± SD) | 9.3 ± 1.0 a | 6.1 ± 2.4 b | 3.4 ± 2.1c |
| 5-item SWB index (2) | 8.2 ± 1.3 a | 6.2 ± 1.6 b | 3.9 ± 1.0 c |
| Parameters | MEDAS Score (Spearman ρ/p-Values) (1) |
|---|---|
| Sociodemographic | |
| Sex | 0.157/0.002 |
| Age | 0.169/0.185 |
| Time of residence in Portugal | 0.031/0.546 |
| Marital status | 0.112/0.031 |
| Household size | 0.018/0.730 |
| Education level | 0.110/0.104 |
| Employment status | 0.161/0.002 |
| Net income | 0.154/0.003 |
| BMI | −0.100/0.057 |
| Lifestyle | |
| Smoking | −0.051/0.323 |
| Sleeping hours per night | −0.013/0.810 |
| Physical activity | −0.079/0.129 |
| Time spent in Nature | 0.182/<0.001 |
| Sleeping | −0.062/0.235 |
| Time spent with family or friends | −0.030/0.568 |
| Meals per day | 0.243/<0.001 |
| SWB | |
| Worthwhile life | 0.127/0.012 |
| Overall life satisfaction | 0.098/0.053 |
| Feeling of happiness | 0.019/0.704 |
| Feeling of worry | −0.109/0.032 |
| Feeling of depression | −0.070/0.169 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrade, V.; Jorge, R.; García-Conesa, M.-T.; Philippou, E.; Massaro, M.; Chervenkov, M.; Ivanova, T.; Maksimova, V.; Smilkov, K.; Ackova, D.G.; et al. Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients 2020, 12, 3837. https://doi.org/10.3390/nu12123837
Andrade V, Jorge R, García-Conesa M-T, Philippou E, Massaro M, Chervenkov M, Ivanova T, Maksimova V, Smilkov K, Ackova DG, et al. Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients. 2020; 12(12):3837. https://doi.org/10.3390/nu12123837
Chicago/Turabian StyleAndrade, Vanda, Rui Jorge, María-Teresa García-Conesa, Elena Philippou, Marika Massaro, Mihail Chervenkov, Teodora Ivanova, Viktorija Maksimova, Katarina Smilkov, Darinka Gjorgieva Ackova, and et al. 2020. "Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults" Nutrients 12, no. 12: 3837. https://doi.org/10.3390/nu12123837
APA StyleAndrade, V., Jorge, R., García-Conesa, M.-T., Philippou, E., Massaro, M., Chervenkov, M., Ivanova, T., Maksimova, V., Smilkov, K., Ackova, D. G., Miloseva, L., Ruskovska, T., Deligiannidou, G. E., Kontogiorgis, C. A., & Pinto, P. (2020). Mediterranean Diet Adherence and Subjective Well-Being in a Sample of Portuguese Adults. Nutrients, 12(12), 3837. https://doi.org/10.3390/nu12123837