Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
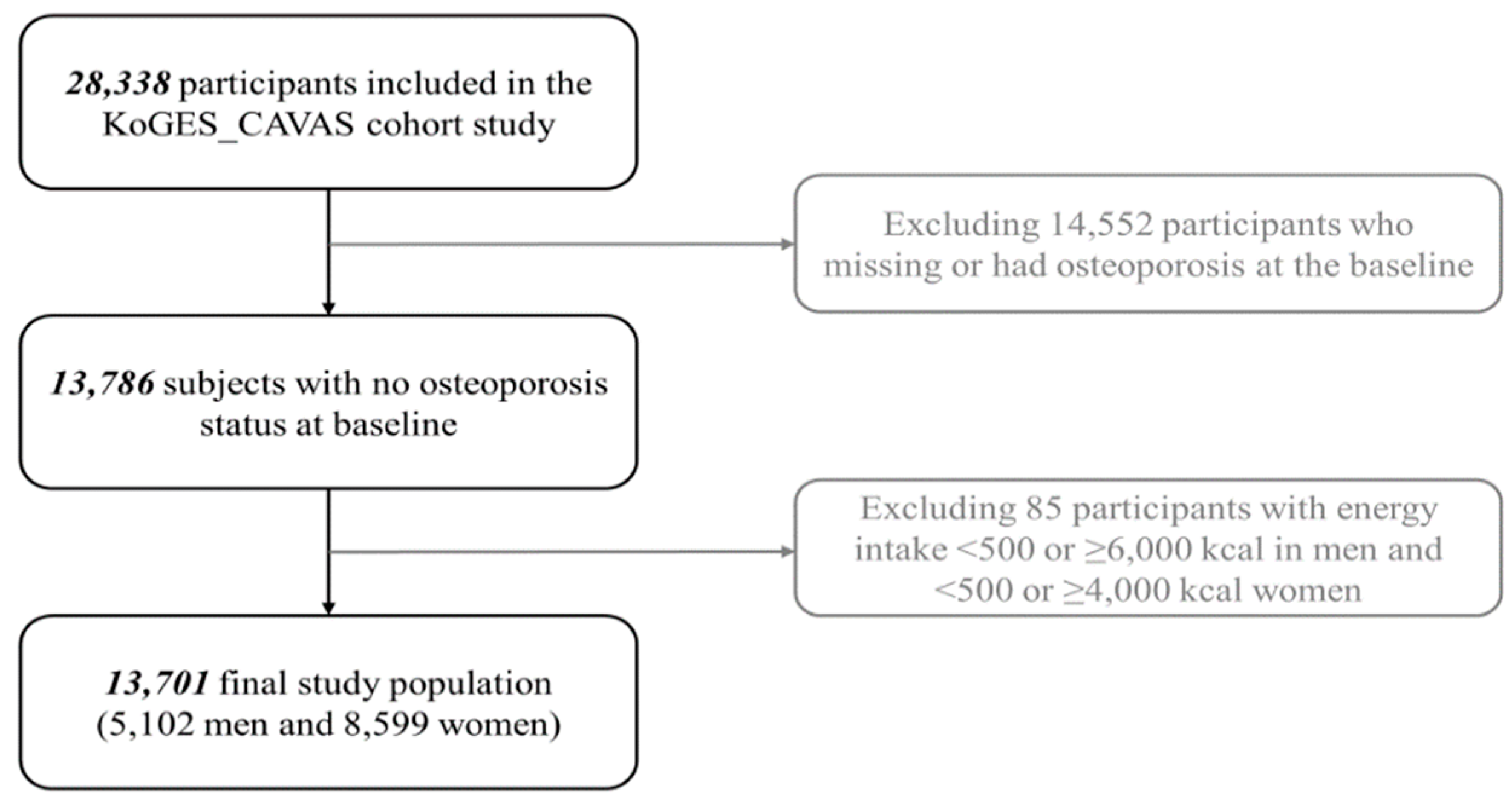
2.1. Study Population
2.2. Data Collection
2.3. Diagnostic Criteria
2.4. Dietary Assessment Using SQ-FFQ and Calculation of DII
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lin, K.C.; Lin, H.Y.; Chou, P. The interaction between uric acid level and other risk factors on the development of gout among asymptomatic hyperuricemic men in a prospective study. J. Rheumatol. 2000, 27, 1501–1505. [Google Scholar] [PubMed]
- Bellomo, G. Uric acid and chronic kidney disease: A time to act? World J. Nephrol. 2013, 2, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Vuorinen-Markkola, H.; Yki-Järvinen, H. Hyperuricemia and insulin resistance. J. Clin. Endocrinol. Metab. 1994, 78, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Gaffo, A.L.; Edwards, N.L.; Saag, K.G. Gout. Hyperuricemia and cardiovascular disease: How strong is the evidence for a causal link? Arthritis Res. Ther. 2009, 11, 240. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.K.; White, C.M. The Emerging Role of Inflammation in Cardiovascular Disease. Ann. Pharmacother. 2018, 52, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Page, R.C. The role of inflammatory mediators in the pathogenesis of periodontal disease. J. Periodontal Res. 1991, 26, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Pannen, B.H.; Robotham, J.L. The acute-phase response. New Horiz. 1995, 3, 183–197. [Google Scholar] [PubMed]
- Spiga, R.; Marini, M.A.; Mancuso, E.; Di Fatta, C.; Fuoco, A.; Perticone, F.; Andreozzi, F.; Mannino, G.C.; Sesti, G. Uric Acid Is Associated With Inflammatory Biomarkers and Induces Inflammation Via Activating the NF-κB Signaling Pathway in HepG2 Cells. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Xu, Y.; Shao, X.; Gao, F.; Li, Y.; Hu, J.; Zuo, Z.; Shao, X.; Zhou, L.; Zhao, Y.; et al. Uric Acid Produces an Inflammatory Response through Activation of NF-κB in the Hypothalamus: Implications for the Pathogenesis of Metabolic Disorders. Sci. Rep. 2015, 5, 12144. [Google Scholar] [CrossRef]
- Giugliano, D.; Ceriello, A.; Esposito, K. The effects of diet on inflammation: Emphasis on the metabolic syndrome. J. Am. Coll. Cardiol. 2006, 48, 677–685. [Google Scholar] [CrossRef]
- Galland, L. Diet and Inflammation. Nutr. Clin. Pract. 2010, 25, 634–640. [Google Scholar] [CrossRef]
- Esposito, K.; Giugliano, D. Diet and inflammation: A link to metabolic and cardiovascular diseases. Eur. Heart J. 2006, 27, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Bulló, M.; Casas-Agustench, P.; Amigó-Correig, P.; Aranceta, J.; Salas-Salvadó, J. Inflammation, obesity and comorbidities: The role of diet. Public Health Nutr. 2007, 10, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Wirth, M.D.; Hurley, T.G.; Hebert, J.R. Association between the Dietary Inflammatory Index (DII) and telomere length and C-reactive protein from the National Health and Nutrition Examination Survey-1999–2002. Mol. Nutr. Food Res. 2016, 61. [Google Scholar] [CrossRef] [PubMed]
- Kotemori, A.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Shivappa, N.; Hebert, J.R. Association between dietary inflammatory index and high-sensitivity C-reactive protein levels in cancer screening in Japanese. Rev. Epidemiol. Sante Publique 2018, 66, S347. [Google Scholar] [CrossRef]
- Julia, C.; Assmann, K.E.; Shivappa, N.; Hebert, J.R.; Wirth, M.D.; Hercberg, S.; Touvier, M.; Kesse-Guyot, E. Long-term associations between inflammatory dietary scores in relation to long-term C-reactive protein status measured 12 years later: Findings from the Supplementation en Vitamines et Mineraux Antioxydants (SU.VI.MAX) cohort. Br. J. Nutr. 2017, 117, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Kizil, M.; Tengilimoglu-Metin, M.M.; Gumus, D.; Sevim, S.; Turkoglu, I.; Mandiroglu, F. Dietary inflammatory index is associated with serum C-reactive protein and protein energy wasting in hemodialysis patients: A cross-sectional study. Nutr. Res. Pract. 2016, 10, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Na, W.; Kim, M.; Sohn, C. Dietary inflammatory index and its relationship with high-sensitivity C-reactive protein in Korean: Data from the health examinee cohort. J. Clin. Biochem. Nutr. 2018, 62, 83–88. [Google Scholar] [CrossRef]
- Shivappa, N.; Wirth, M.D.; Murphy, E.A.; Hurley, T.G.; Hebert, J.R. Association between the Dietary Inflammatory Index (DII) and urinary enterolignans and C-reactive protein from the National Health and Nutrition Examination Survey-2003–2008. Eur. J. Nutr. 2019, 58, 797–805. [Google Scholar] [CrossRef]
- Ramallal, R.; Toledo, E.; Martínez-González, M.A.; Hernández-Hernández, A.; García-Arellano, A.; Shivappa, N.; Hébert, J.R.; Ruiz-Canela, M. Dietary Inflammatory Index and Incidence of Cardiovascular Disease in the SUN Cohort. PLoS ONE 2015, 10, e0135221. [Google Scholar] [CrossRef] [PubMed]
- Boden, S.; Wennberg, M.; Van Guelpen, B.; Johansson, I.; Lindahl, B.; Andersson, J.; Shivappa, N.; Hebert, J.R.; Nilsson, L.M. Dietary inflammatory index and risk of first myocardial infarction; a prospective population-based study. Nutr. J. 2017, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Sohn, C.; Kwon, M.; Na, W.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive Association between Dietary Inflammatory Index and the Risk of Osteoporosis: Results from the KoGES_Health Examinee (HEXA) Cohort Study. Nutrients 2018, 10, 1999. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Itsiopoulos, C.; Tierney, A.C.; Ruiz-Canela, M.; Hebert, J.R.; Shivappa, N.; Thomas, C.J. Improvement in dietary inflammatory index score after 6-month dietary intervention is associated with reduction in interleukin-6 in patients with coronary heart disease: The AUSMED heart trial. Nutr. Res. 2018, 55, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G.; KoGES group. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Hong, E.J.; Nam, J.M.; Han, H.; Chu, C.; Park, O. Opening of the national biobank of Korea as the infrastructure of future biomedical science in Korea. Osong Public Health Res. Perspect. 2012, 3, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.N.; Shi, Y.X.; Cheng, H.Y.; Huang, X.L.; Liu, S.S. An observational study on the relationship between serum uric acid and hypertension in a Northern Chinese population aged 45 to 59 years. Medicine 2017, 96, e6773. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Hisatome, I.; Nakagawa, T.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Bjornstad, P.; Jensen, T.; Sato, Y.; Milagres, T.; et al. Asymptomatic Hyperuricemia Without Comorbidities Predicts Cardiometabolic Diseases: Five-Year Japanese Cohort Study. Hypertension 2017, 69, 1036–1044. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Trevisan, C.; Bolzetta, F.; De Rui, M.; Maggi, S.; Sartori, L.; Musacchio, E.; Zambon, S.; Perissinotto, E.; et al. Results of an Observational Cohort Study of Hyperuricemia as a Predictor of Poor Physical Performance in the Elderly. Arthritis Care Res. 2017, 69, 1238–1244. [Google Scholar] [CrossRef]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef]
- Mina, K.; Fritschi, L.; Knuiman, M. A valid semiquantitative food frequency questionnaire to measure fish consumption. Eur. J. Clin. Nutr. 2007, 61, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- National Rural Resources Development Institute. Food Composition Table, 9th ed.; Rural Development Administration, National Rural Resources Development Institute: Suwon, Korea; Available online: http://koreanfood.rda.go.kr/eng/fctFoodSrchEng/engMain (accessed on 4 June 2019).
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literaturederived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Ogata, S.; Tanaka, H.; Omura, K.; Honda, C.; Osaka Twin Research Group; Hayakawa, K. The relationship between body mass index and uric acid: A study on Japanese adult twins. Environ. Health Prev. Med. 2015, 20, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Ishizaka, N.; Ishizaka, Y.; Toda, A.; Tani, M.; Koike, K.; Yamakado, M.; Nagai, R. Changes in Waist Circumference and Body Mass Index in Relation to Changes in Serum Uric Acid in Japanese Individuals. J. Rheumatol. 2010, 37, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Lou, S.; Xu, K.; Meng, Z.; Zhang, Q.; Song, K. Relationship between lifestyle choices and hyperuricemia in Chinese men and women. Clin. Rheumatol. 2013, 32, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Remedios, C.; Shah, M.; Bhasker, A.G.; Lakdawala, M. Hyperuricemia: A Reality in the Indian Obese. Obes. Surg. 2012, 22, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, S.; Yilmaz, R.; Akinci, D.; Arici, M.; Altun, B.; Erdem, Y.; Yasavul, U.; Turgan, C. U-Shaped Association of Body Mass Index With Inflammation and Atherosclerosis in Hemodialysis Patients. J. Ren. Nutr. 2005, 15, 377–386. [Google Scholar] [CrossRef]
- Mave, V.; Erlandson, K.M.; Gupte, N.; Balagopal, A.; Asmuth, D.M.; Campbell, T.B.; Smeaton, L.; Kumarasamy, N.; Hakim, J.; Santos, B.; et al. Inflammation and Change in Body Weight With Antiretroviral Therapy Initiation in a Multinational Cohort of HIV-Infected Adults. J. Infect. Dis. 2016, 214, 65–72. [Google Scholar] [CrossRef]
- Drum, D.E.; Goldman, P.A.; Jankowski, C.B. Elevation of serum uric acid as a clue to alcohol abuse. Arch. Intern. Med. 1981, 141, 477–479. [Google Scholar] [CrossRef]
- Sharpe, C.R. A case-control study of alcohol consumption and drinking behaviour in patients with acute gout. Can. Med. Assoc. J. 1984, 131, 563–567. [Google Scholar]
- Choi, H.K.; Curhan, G. Beer, liquor, and wine consumption and serum uric acid level: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2004, 51, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Gibson, T.; Rodgers, A.V.; Simmonds, H.A.; Toseland, P. Beer drinking and its effect on uric acid. Br. J. Rheumatol. 1984, 23, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.M.; Liu, Y.J.; Huang, Y.; Yu, H.J.; Yuan, S.; Tang, B.W.; Wang, P.G.; He, Q.Q. Dietary total flavonoids intake and risk of mortality from all causes and cardiovascular disease in the general population: A systematic review and meta-analysis of cohort studies. Mol. Nutr. Food Res. 2017, 61. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.S.; Kim, H.; Vijayakumar, A.; Kwon, O.; Kim, Y.; Chang, N. Association of Dietary Flavonoid Intake with Prevalence of Type 2 Diabetes Mellitus and Cardiovascular Disease Risk Factors in Korean Women Aged ≥30 Years. J. Nutr. Sci. Vitaminol. 2017, 63, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Wang, T.; Song, D.; Wang, A. Dietary intake of flavonoid subclasses and risk of type 2 diabetes in prospective cohort studies: A dose-response meta-analysis. Clin. Nutr. 2018, 37, 2294–2298. [Google Scholar] [CrossRef] [PubMed]
- Lajous, M.; Rossignol, E.; Fagherazzi, G.; Perquier, F.; Scalbert, A.; Clavel-Chapelon, F.; Boutron-Ruault, M.C. Flavonoid intake and incident hypertension in women. Am. J. Clin. Nutr. 2016, 103, 1091–1098. [Google Scholar] [CrossRef]
- Wang, Z.M.; Zhao, D.; Nie, Z.L.; Zhao, H.; Zhou, B.; Gao, W.; Wang, L.S.; Yang, Z.J. Flavonol intake and stroke risk: A meta-analysis of cohort studies. Nutrition 2014, 30, 518–523. [Google Scholar] [CrossRef]
- Geleijnse, J.M.; Launer, L.J.; Van der Kuip, D.A.; Hofman, A.; Witteman, J.C. Inverse association of tea and flavonoid intakes with incident myocardial infarction: The Rotterdam Study. Am. J. Clin. Nutr. 2002, 75, 880–886. [Google Scholar] [CrossRef]
- Wang, Z.M.; Nie, Z.L.; Zhou, B.; Lian, X.Q.; Zhao, H.; Gao, W.; Wang, Y.S.; Jia, E.Z.; Wang, L.S.; Yang, Z.J. Flavonols intake and the risk of coronary heart disease: A meta-analysis of cohort studies. Atherosclerosis 2012, 222, 270–273. [Google Scholar] [CrossRef]
- Mazidi, M.; Katsiki, N.; Banach, M. A higher flavonoid intake is associated with less likelihood of nonalcoholic fatty liver disease: Results from a multiethnic study. J. Nutr. Biochem. 2019, 65, 66–71. [Google Scholar] [CrossRef]
- Orhan, I.E.; Daglia, M.; Nabavi, S.F.; Loizzo, M.R.; Sobarzo-Sánchez, E.; Nabavi, S.M. Flavonoids and dementia: An update. Curr. Med. Chem. 2015, 22, 1004–1015. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Barupal, D.K.; Rothwell, J.A.; Jenab, M.; Fedirko, V.; Romieu, I.; Aleksandrova, K.; Overvad, K.; Kyrø, C.; Tjønneland, A.; et al. Dietary flavonoid intake and colorectal cancer risk in the European prospective investigation into cancer and nutrition (EPIC) cohort. Int. J. Cancer. 2017, 140, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Terao, J. Dietary Flavonoids as Antioxidants. In Food Factors for Health Promotion; Karger Publishers: Basel, Switzerland, 2009; Volume 61, pp. 87–94. [Google Scholar]
- Pietta, P.G. Flavonoids as antioxidants. J. Nat. Prod. 2000, 63, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative stress, inflammation, and cancer: How are they linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.; Olsen, R.W. Alcohol use disorders and current pharmacological therapies: The role of GABA(A) receptors. Acta Pharmacol. Sin. 2014, 35, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Hak, A.E.; Choi, H.K. Menopause, postmenopausal hormone use and serum uric acid levels in US women—The Third National Health and Nutrition Examination Survey. Arthritis Res. Ther. 2008, 10, R116. [Google Scholar] [CrossRef] [PubMed]
- Sumino, H.; Ichikawa, S.; Kanda, T.; Nakamura, T.; Sakamaki, T. Reduction of serum uric acid by hormone replacement therapy in postmenopausal women with hyperuricaemia. Lancet 1999, 354, 650. [Google Scholar] [CrossRef]
- Nicholls, A.; Snaith, M.L.; Scott, J.T. Effect of oestrogen therapy on plasma and urinary levels of uric acid. Br. Med. J. 1973, 1, 449–451. [Google Scholar] [CrossRef]
- Vegeto, E.; Benedusi, V.; Maggi, A. Estrogen anti-inflammatory activity in brain: A therapeutic opportunity for menopause and neurodegenerative diseases. Front. Neuroendocrinol. 2008, 29, 507–519. [Google Scholar] [CrossRef]
- Eskes, T.; Haanen, C. Why do women live longer than men? Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 133, 126–133. [Google Scholar] [CrossRef]
- Park, Y.J.; Kim, H.S.; Kang, H.C. The Age at Menopause and Related Factors in Korean Women. J. Korean Acad. Nurs. 2002, 32, 1024–1031. [Google Scholar] [CrossRef]
- Pandey, A.S.; Shreevastva, N.K.; Neupane, D.P. Nicotine exposure, blood pressure, and inflammation in tobacco smokers and chewers in a rural community in Nepal. Subst. Use Misuse. 2014, 49, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Barquera, S.; Hernández-Barrera, L.; Campos-Nonato, I.; Espinosa, J.; Flores, M.; Barriguete, A.J.; Rivera, J.A. Energy and nutrient consumption in adults: Analysis of the Mexican National Health and Nutrition Survey 2006. Salud Pública México 2009, 51, S562–S573. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Clavel-Chapelon, F.; E3N Study Group. Cohort Profile: The French E3N Cohort Study. Int. J. Epidemiol. 2015, 44, 801–809. [Google Scholar] [CrossRef]
- Sari, I.; Akar, S.; Pakoz, B.; Sisman, A.R.; Gurler, O.; Birlik, M.; Onen, F.; Akkoc, N. Hyperuricemia and its related factors in an urban population, Izmir, Turkey. Rheumatol. Int. 2009, 29, 869–874. [Google Scholar] [CrossRef]


{kind=link}
| Male | Female | |||||
|---|---|---|---|---|---|---|
| Characteristics | With Hyperuricemia (n = 875) | Without Hyperuricemia (n = 4227) | p Value a | With Hyperuricemia (n = 640) | Without Hyperuricemia (n = 7959) | p Value |
| Serum uric acid (mg/dL) | 8.06 ± 0.99 b | 5.32 ± 1.00 | <0.0001 | 6.90 ± 0.85 | 4.24 ± 0.87 | <0.0001 |
| DII | −0.01 ± 2.08 | −0.08 ± 2.18 | 0.3610 | 0.46 ± 2.23 | 0.13 ± 2.16 | 0.0002 |
| Age (years) | 61.2 ± 10.1 | 62.2 ± 9.56 | 0.0035 | 64.2 ± 9.02 | 60.5 ± 9.94 | <0.0001 |
| BMI (kg/m2) | 25.0 ± 3.10 | 23.8 ± 2.94 | <0.0001 | 25.8 ± 3.64 | 24.4 ± 3.19 | <0.0001 |
| Waist circumference (cm) | 88.4 ± 8.41 | 85.1 ± 8.37 | <0.0001 | 86.5 ± 9.38 | 82.9 ± 8.93 | <0.0001 |
| hs-CRP (mg/L) | 2.72 ± 6.48 | 2.19 ± 5.81 | <0.0001 | 2.62 ± 4.48 | 1.58 ± 3.96 | <0.0001 |
| WBC (Thousand/ μL) | 7.04 ± 1.94 | 6.76 ± 2.00 | 0.0001 | 6.99 ± 2.16 | 6.14 ± 1.79 | <0.0001 |
| Glucose (mg/dL) | 102 ± 21.8 | 104 ± 28.8 | 0.0175 | 104 ± 24.3 | 98.2 ± 21.4 | <0.0001 |
| HOMA_IR | 2.28 ± 2.05 | 1.86 ± 1.00 | 0.0265 | 2.53 ± 1.43 | 1.93 ± 0.96 | <0.0001 |
| SBP (mmHg) | 127 (126–128) | 125 (124–125) | 0.0010 | 128 (127–130) | 124 (123–124) | <0.0001 |
| DBP (mmHg) | 80.0 (79.3–80.8) | 78.9 (78.6–79.2) | 0.0027 | 78.5 (77.7–79.4) | 76.8 (76.5–77.0) | <0.0001 |
| Triglyceride (mg/dL) | 199 (191–208) | 154 (151–157) | <0.0001 | 193 (184–201) | 141 (139–143) | <0.0001 |
| HDL-cholesterol (mg/dL) | 41.8 (41.0–42.5) | 44.2 (43.8–44.5) | <0.0001 | 42.7 (42.0–43.5) | 46.3 (46.0–46.5) | <0.0001 |
| Daily caloric intake (kcal) | 1694 (1661–1727) | 1710 (1694–1726) | 0.3980 | 1443 (1408–1477) | 1494 (1484–1504) | 0.0051 |
| Carbohydrate intake (g/day) | 308 (303–314) | 315 (312–317) | 0.0364 | 276 (269–282) | 285 (284–287) | 0.0030 |
| Carbohydrate (E%) | 73.7 (73.2–74.1) | 74.4 (74.2–74.6) | 0.0018 | 77.0 (76.5–77.5) | 76.9 (76.8–77.0) | 0.7963 |
| Protein intake (g/day) | 52.6 (51.2–54.0) | 53.0 (52.1–53.5) | 0.7806 | 42.7 (41.3–44.2) | 44.4 (44.0–44.8) | 0.1894 |
| Protein (E%) | 12.2 (12.1–12.4) | 12.1 (12.1–12.2) | 0.3754 | 11.7 (11.5–11.9) | 11.8 (11.7–11.8) | 0.7901 |
| Fat intake (g/day) | 24.8 (23.7–25.9) | 23.8 (23.4–24.3) | 0.1041 | 16.4 (15.4–17.3) | 17.0 (16.7–17.3) | 0.0237 |
| Fat (E%) | 12.4 (12.1–12.8) | 11.9 (11.7–12.0) | 0.0023 | 9.73 (9.35–10.1) | 9.79 (9.68–9.89) | 0.3891 |
| Fruits (g/day) | 146 (136–155) | 152 (147–157) | 0.2524 | 170 (157–183) | 184 (180–188) | 0.0386 |
| Vegetables (g/day) | 213 (203–222) | 235 (230–240) | <0.0001 | 184 (172–195) | 207 (304–210) | 0.0001 |
| Marriage | ||||||
| Married | 811 (93.2) | 3987 (94.8) | 0.07 | 422 (66.0) | 5932 (74.8) | <0.0001 |
| Single | 59 (6.8) | 220 (5.2) | 217 (34.0) | 1999 (25.2) | ||
| Education | ||||||
| ~Elementary school | 397 (45.5) | 1998 (47.4) | 0.19 | 474 (74.3) | 5524 (69.6) | 0.03 |
| Middle~High school | 379 (43.5) | 1831 (43.5) | 142 (22.2) | 2149 (27.1) | ||
| College~ | 96 (11.0) | 383 (9.1) | 22 (3.5) | 270 (3.3) | ||
| Household Income Levels c | ||||||
| Less than 100 | 72 (38.1) | 366 (38.1) | 0.58 | 97 (57.7) | 885 (46.9) | 0.01 |
| 100~less than 200 | 38 (20.1) | 234 (24.4) | 32 (19.1) | 383 (20.3) | ||
| 200~less than 300 | 35 (18.5) | 160 (16.7) | 22 (13.1) | 263 (13.9) | ||
| More than 300 | 44 (23.3) | 200 (20.8) | 17 (10.1) | 356 (18.9) | ||
| Smoking Status | ||||||
| Never | 217 (24.8) | 1070 (25.3) | 0.07 | 575 (89.8) | 7578 (95.3) | <0.0001 |
| Past | 397 (45.4) | 1751 (41.4) | 25 (3.9) | 144 (1.8) | ||
| Current | 261 (29.8) | 1404 (33.3) | 40 (6.3) | 234 (2.9) | ||
| Drinking Status | ||||||
| Never | 135 (15.5) | 1011 (23.9) | <0.0001 | 416 (65.10) | 5404 (68.0) | 0.0008 |
| Past | 114 (13.0) | 606 (14.4) | 41 (6.42) | 278 (3.5) | ||
| Current | 626 (71.5) | 2607 (61.7) | 182 (28.48) | 2268 (28.5) | ||
| Physical Activity d | ||||||
| No | 594 (67.9) | 2842 (67.2) | 0.72 | 435 (68.0) | 5526 (69.5) | 0.43 |
| Yes | 281 (32.1) | 1384 (32.8) | 205 (32.0) | 2429 (30.5) | ||
| History of Hypertension | ||||||
| No | 556 (63.5) | 3193 (75.6) | <0.0001 | 297 (46.4) | 5749 (72.2) | <0.0001 |
| Yes | 319 (36.5) | 1033 (24.4) | 343 (53.6) | 2209 (27.8) | ||
| History of Diabetes | ||||||
| No | 787 (89.9) | 3769 (89.2) | 0.51 | 551 (86.1) | 7270 (91.4) | <0.0001 |
| Yes | 88 (10.1) | 457 (10.8) | 89 (13.9) | 688 (8.6) | ||
| Quartile of DII | ||||||
|---|---|---|---|---|---|---|
| First (Lowest) | Second | Third | Fourth (Highest) | p for Trend a | Continuous DII | |
| TOTAL | ||||||
| Range | −7.3344~−1.2409 | −1.2408~−0.2501 | −0.2499~1.5499 | 1.5513~7.0740 | ||
| Cases/controls | 349/3047 | 367/3047 | 391/3047 | 408/3045 | ||
| Odds ratio (95% CI) | ||||||
| Crude | 1.00 | 1.05 (0.90−1.23) b | 1.12 (0.96–1.31) | 1.17 (1.01–1.36) | 0.03 | 1.03 (1.00–1.05) |
| Multivariate adjusted | 1.00 | 1.05 (0.89–1.25) | 1.01 (0.92–1.30) | 1.23 (1.03–1.46) | 0.02 | 1.04 (1.01–1.07) |
| MENc | ||||||
| Range | −7.3344~−1.3572 | −1.3565~−0.3522 | −0.3520~1.4001 | 1.4012~6.9009 | ||
| Cases/controls | 212/1057 | 217/1057 | 220/1057 | 226/1056 | ||
| Odds ratio (95% CI) | ||||||
| Crude | 1.00 | 1.02 (0.83–1.26) | 1.04 (0.84–1.28) | 1.07 (0.87–1.31) | 0.53 | 1.02 (0.98–1.05) |
| Multivariate adjusted | 1.00 | 1.03 (0.82–1.29) | 1.00 (0.80–1.26) | 1.10 (0.87–1.39) | 0.49 | 1.02 (0.98–1.06) |
| WOMEN | ||||||
| Range | −7.3009~−1.1924 | −1.1915~−0.1928 | −0.1922~1.6153 | 1.6154~7.0740 | ||
| Cases/controls | 126/1990 | 148/1989 | 170/1991 | 196/1989 | ||
| Odds ratio (95% CI) | ||||||
| Crude | 1.00 | 1.18 (0.92–1.50) | 1.35 (1.06–1.71) | 1.56 (1.23–1.96) | <0.0001 | 1.07 (1.03–1.11) |
| Multivariate adjusted | 1.00 | 1.11 (0.85–1.45) | 1.17 (0.90–1.52) | 1.35 (1.03–1.77) | 0.02 | 1.04 (0.99–1.01) |
| Quartile of DII | p for | ||||||
|---|---|---|---|---|---|---|---|
| Subgroup | First (Lowest) | Second | Third | Fourth (Highest) | Trend a | Interaction b | Continuous DII |
| TOTAL | |||||||
| Body-mass index | |||||||
| Cases/controls | 134/1747 | 182/1896 | 182/1906 | 216/1974 | |||
| <25 | 1.00 | 1.11 (0.86–1.42) c | 1.04 (0.81–1.34) | 1.25 (0.97–1.62) | 0.12 | 0.56 | 1.04 (0.99–1.09) |
| Cases/controls | 214/1299 | 185/1150 | 209/1141 | 192/1069 | |||
| >=25 | 1.00 | 1.02 (0.81–1.29) | 1.15 (0.91–1.44) | 1.20 (0.94–1.54) | 0.09 | 1.03 (0.99–1.07) | |
| Drinking status | |||||||
| Cases/controls | 105/1460 | 141/1626 | 155/1610 | 150/1719 | |||
| No | 1.00 | 1.13 (0.85–1.50) | 1.23 (0.93–1.63) | 1.13 (0.84–1.52) | 0.41 | 0.24 | 1.02 (0.97–1.07) |
| Cases/controls | 244/1586 | 226/1415 | 235/1436 | 258/1322 | |||
| Yes d | 1.00 | 1.03 (0.83–1.27) | 1.03 (0.83–1.27) | 1.32 (1.06–1.63) | 0.02 | 1.05 (1.01–1.09) | |
| MEN | |||||||
| Body–mass index | |||||||
| Cases/controls | 89/602 | 115/708 | 109/722 | 130/751 | |||
| <25 | 1.00 | 0.98 (0.72–1.35) | 0.86 (0.62–1.19) | 1.02 (0.73–1.42) | 0.96 | 0.70 | 1.01 (0.96–1.07) |
| Cases/controls | 122/455 | 102/348 | 111/335 | 96/305 | |||
| >=25 | 1.00 | 1.10 (0.79–1.52) | 1.17 (0.85–1.61) | 1.18 (0.85–1.67) | 0.27 | 1.03 (0.97–1.09) | |
| Drinking status | |||||||
| Cases/controls | 26/246 | 37/252 | 44/249 | 28/264 | |||
| No | 1.00 | 1.42 (0.79–2.53) | 1.73 (0.98–3.07) | 1.05 (0.56–1.98) | 0.83 | 0.08 | 1.01 (0.92–1.12) |
| Cases/controls | 186/810 | 180/803 | 176/808 | 198/792 | |||
| Yes | 1.00 | 0.97 (0.76–1.25) | 0.91 (0.71–1.17) | 1.12 (0.86–1.42) | 0.49 | 1.02 (0.98–1.07) | |
| WOMEN | |||||||
| Body-mass index | |||||||
| Cases/controls | 41/1146 | 61/1173 | 74/1192 | 95/1229 | |||
| <25 | 1.00 | 1.26 (0.81–1.95) | 1.33 (0.87–2.06) | 1.62 (1.05–2.52) | 0.03 | 0.67 | 1.09 (1.01–1.16) |
| Cases/controls | 85/843 | 87/816 | 96/799 | 101/758 | |||
| >=25 | 1.00 | 1.02 (0.73–1.43) | 1.09 (0.78–1.52) | 1.19 (0.84–1.68) | 0.34 | 1.01 (0.96–1.07) | |
| Drinking status | |||||||
| Cases/controls | 82/1265 | 101/1362 | 113/1359 | 120/1418 | |||
| No | 1.00 | 1.06 (0.76–1.48) | 1.11 (0.80–1.53) | 1.12 (0.80–1.57) | 0.48 | 0.21 | 1.01 (0.96–1.07) |
| Cases/controls | 44/725 | 47/623 | 56/631 | 76/567 | |||
| Yes | 1.00 | 1.22 (0.77–1.94) | 1.31 (0.84–2.06) | 1.92 (1.22–3.02) | 0.004 | 1.11 (1.03–1.19) | |
| Quartile of Components | |||||
|---|---|---|---|---|---|
| DII components (Flavonoids) | First (lowest) | Second | Third | Fourth (highest) | P for trend a |
| Flavan-3-ol (mg) | |||||
| Cases/controls | 190/1990 | 167/1990 | 147/1990 | 136/1989 | |
| Multivariate adjusted | 1.00 | 0.89 (0.71–1.12) b | 0.85 (0.68–1.08) | 0.78 (0.61–0.99) | 0.04 |
| Flavones (mg) | |||||
| Cases/controls | 183/1990 | 163/1989 | 167/1990 | 127/1990 | |
| Multivariate adjusted | 1.00 | 0.95 (0.76–1.20) | 0.97 (0.77–1.22) | 0.75 (0.59–0.96) | 0.04 |
| Flavonols (mg) | |||||
| Cases/controls | 181/1989 | 164/1990 | 166/1990 | 129/1990 | |
| Multivariate adjusted | 1.00 | 0.94 (0.75–1.18) | 0.98 (0.78–1.23) | 0.76 (0.59–0.97) | 0.06 |
| Flavonones (mg) | |||||
| Cases/controls | 196/1989 | 150/1991 | 161/1989 | 133/1990 | |
| Multivariate adjusted | 1.00 | 0.83 (0.66–1.05) | 0.89 (0.71–1.11) | 0.75 (0.59–0.95) | 0.04 |
| Flavonoids (mg) | |||||
| Cases/controls | 187/1990 | 165/1989 | 156/1991 | 132/1989 | |
| Multivariate adjusted | 1.00 | 0.92 (0.74–1.16) | 0.90 (0.71–1.13) | 0.75 (0.59–0.96) | 0.03 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Kwon, M.; Lee, H.Y.; Shivappa, N.; R. Hébert, J.; Sohn, C.; Na, W.; Kim, M.K. Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study. Nutrients 2019, 11, 1803. https://doi.org/10.3390/nu11081803
Kim HS, Kwon M, Lee HY, Shivappa N, R. Hébert J, Sohn C, Na W, Kim MK. Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study. Nutrients. 2019; 11(8):1803. https://doi.org/10.3390/nu11081803
Chicago/Turabian StyleKim, Hye Sun, Minji Kwon, Hyun Yi Lee, Nitin Shivappa, James R. Hébert, Cheongmin Sohn, Woori Na, and Mi Kyung Kim. 2019. "Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study" Nutrients 11, no. 8: 1803. https://doi.org/10.3390/nu11081803
APA StyleKim, H. S., Kwon, M., Lee, H. Y., Shivappa, N., R. Hébert, J., Sohn, C., Na, W., & Kim, M. K. (2019). Higher Pro-Inflammatory Dietary Score is Associated with Higher Hyperuricemia Risk: Results from the Case-Controlled Korean Genome and Epidemiology Study_Cardiovascular Disease Association Study. Nutrients, 11(8), 1803. https://doi.org/10.3390/nu11081803