Faster Gastric Emptying Is Unrelated to Feeding Success in Preterm Infants: Randomized Controlled Trial

 ,
,  ,
, 
 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Assessment of Gastric Emptying by Real-Time Ultrasonography
2.3. Statistical Analysis
3. Results
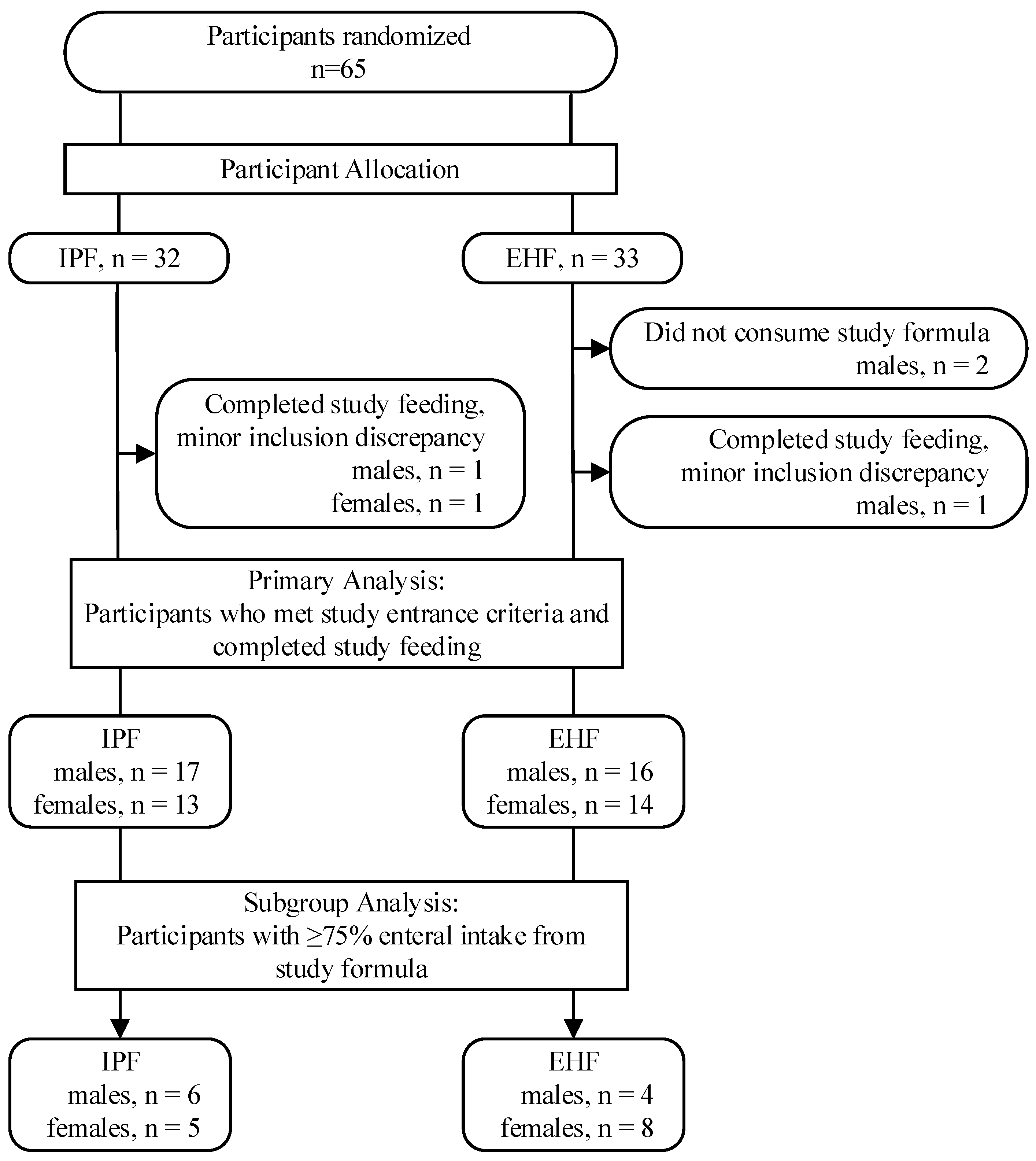
3.1. Study Population
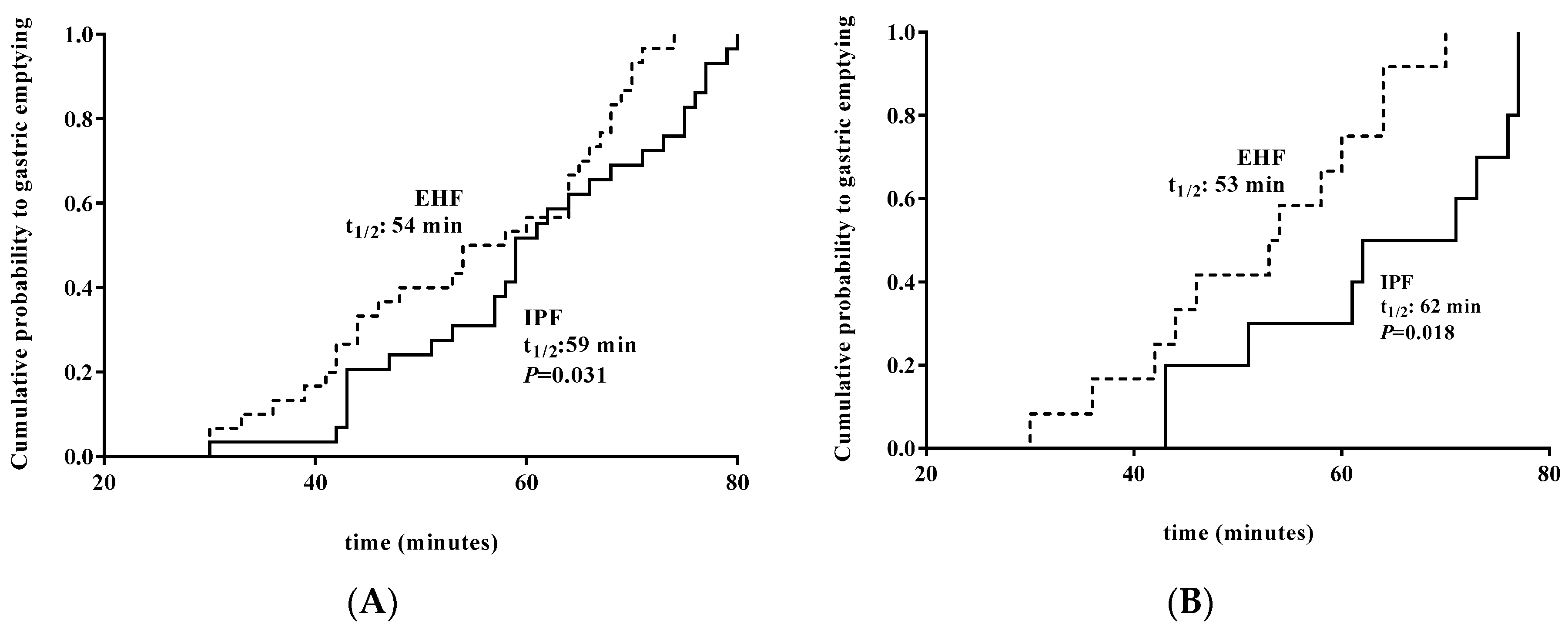
3.2. Gastric Emptying (GE) Time
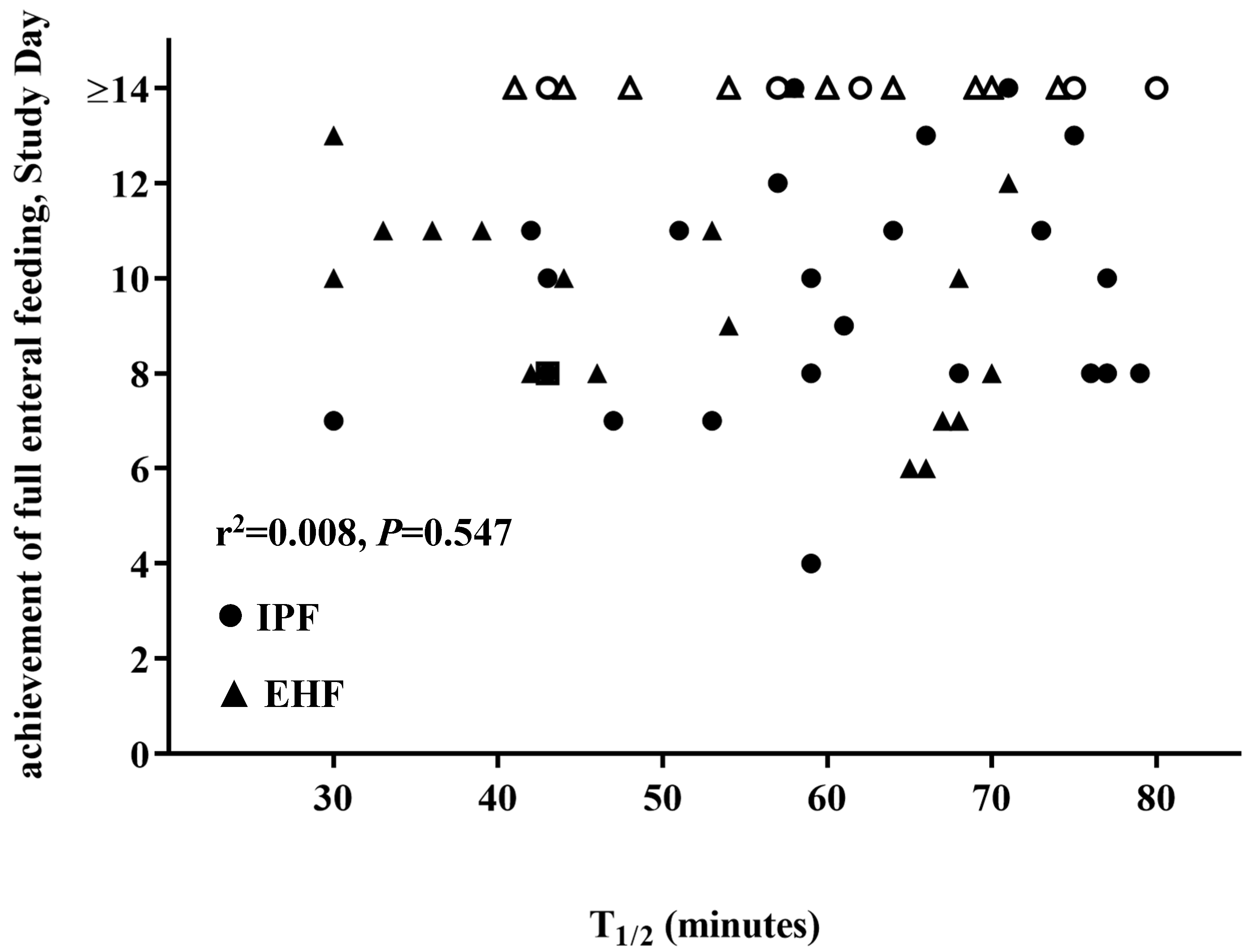
3.3. Effect of GE Time on Achievement of Full Enteral Feeding
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviation
References
- Indrio, F.; Riezzo, G.; Cavallo, L.; Di Mauro, A.; Francavilla, R. Physiological basis of food intolerance in VLBW. J. Matern. Fetal Neonatal Med. 2011, 24 (Suppl. 1), 64–66. [Google Scholar] [CrossRef] [PubMed]
- Fanaro, S. Feeding intolerance in the preterm infant. Early Hum. Dev. 2013, 89 (Suppl. 2), S13–S20. [Google Scholar] [CrossRef] [PubMed]
- Lapillonne, A.; Matar, M.; Adleff, A.; Chbihi, M.; Kermorvant-Duchemin, E.; Campeotto, F. Use of extensively hydrolysed formula for refeeding neonates postnecrotising enterocolitis: A nationwide survey-based, cross-sectional study. BMJ Open 2016, 6, e008613. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ng, D.H.C.; Klassen, J.; Embleton, N.D.; McGuire, W. Protein hydrolysate versus standard formula for preterm infants. Cochrane Database Syst. Rev. 2017, 10, CD012412. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.H.C.; Embleton, N.D.; McGuire, W. Hydrolyzed Formula Compared With Standard Formula for Preterm Infants. JAMA 2018, 319, 1717–1718. [Google Scholar] [CrossRef] [PubMed]
- Siegel, M.; Lebenthal, E.; Topper, W.; Krantz, B.; Li, P.K. Gastric emptying in prematures of isocaloric feedings with differing osmolalities. Pediatr. Res. 1982, 16, 141–147. [Google Scholar] [CrossRef]
- Siegel, M.; Krantz, B.; Lebenthal, E. Effect of fat and carbohydrate composition on the gastric emptying of isocaloric feedings in premature infants. Gastroenterology 1985, 89, 785–790. [Google Scholar] [CrossRef]
- Ramirez, A.; Wong, W.W.; Shulman, R.J. Factors regulating gastric emptying in preterm infants. J. Pediatr. 2006, 149, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Indrio, F.; Riezzo, G.; Raimondi, F.; Di Mauro, A.; Francavilla, R. Microbiota involvement in gut-brain axis. J. Pediatr. Gastroenterol. Nutr. 2013, 57, S11–S15. [Google Scholar] [CrossRef]
- Meyer, R.; Foong, R.X.; Thapar, N.; Kritas, S.; Shah, N. Systematic review of the impact of feed protein type and degree of hydrolysis on gastric emptying in children. BMC Gastroenterol. 2015, 15, 137. [Google Scholar] [CrossRef]
- Perrella, S.L.; Hepworth, A.R.; Gridneva, Z.; Simmer, K.N.; Hartmann, P.E.; Geddes, D.T. Gastric emptying and curding of pasteurized donor human milk and mother’s own milk in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2015, 61, 125–129. [Google Scholar]
- Mihatsch, W.A.; Franz, A.R.; Hogel, J.; Pohlandt, F. Hydrolyzed protein accelerates feeding advancement in very low birth weight infants. Pediatrics 2002, 110, 1199–1203. [Google Scholar] [CrossRef]
- Florendo, K.N.; Bellflower, B.; van Zwol, A.; Cooke, R.J. Growth in preterm infants fed either a partially hydrolyzed whey or an intact casein/whey preterm infant formula. J. Perinatol. 2009, 29, 106–111. [Google Scholar] [CrossRef]
- Bertino, E.; Spada, E.; Occhi, L.; Coscia, A.; Giuliani, F.; Gagliardi, L.; Gilli, G.; Bona, G.; Fabris, C.; De Curtis, M.; et al. Neonatal anthropometric charts: The Italian neonatal study compared with other European studies. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 353–361. [Google Scholar] [CrossRef]
- Darwiche, G.; Östman, E.M.; Liljeberg, H.G.; Kallinen, N.; Björgell, O.; Björck, I.M.; Almér, L.-O. Measurements of the gastric emptying rate by use of ultrasonography: Studies in humans using bread with added sodium propionate. Am. J. Clin. Nutr. 2001, 74, 254–258. [Google Scholar] [CrossRef]
- Elashoff, J.D.; Reedy, T.J.; Meyer, J.H. Analysis of gastric emptying data. Gastroenterology 1982, 83, 1306–1312. [Google Scholar]
- Billeaud, C.; Guillet, J.; Sandler, B. Gastric emptying in infants with or without gastro-oesophageal reflux according to the type of milk. Eur. J. Clin. Nutr. 1990, 44, 577–583. [Google Scholar]
- Garzi, A.; Messina, M.; Frati, F.; Carfagna, L.; Zagordo, L.; Belcastro, M.; Parmiani, S.; Sensi, L.; Marcucci, F. An extensively hydrolysed cow’s milk formula improves clinical symptoms of gastroesophageal reflux and reduces the gastric emptying time in infants. Allergol. Immunopathol. 2002, 30, 36–41. [Google Scholar]
- Staelens, S.; Van den Driessche, M.; Barclay, D.; Carrie-Faessler, A.L.; Haschke, F.; Verbeke, K.; Vandebroek, H.; Allegaert, K.; Van Overmeire, B.; Van Damme, M.; et al. Gastric emptying in healthy newborns fed an intact protein formula, a partially and an extensively hydrolysed formula. Clin. Nutr. 2008, 27, 264–268. [Google Scholar] [CrossRef]
- Perrella, S.L.; Hepworth, A.R.; Simmer, K.N.; Hartmann, P.E.; Geddes, D.T. Repeatability of gastric volume measurements and intragastric content using ultrasound in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 254–263. [Google Scholar] [CrossRef]
- Siegel, M.; Lebenthal, E.; Krantz, B. Effect of caloric density on gastric emptying in premature infants. J. Pediatr. 1984, 104, 118–122. [Google Scholar] [CrossRef]
- Kreissl, A.; Zwiauer, V.; Repa, A.; Binder, C.; Haninger, N.; Jilma, B.; Berger, A.; Haiden, N. Effect of fortifiers and additional protein on the osmolarity of human milk: Is it still safe for the premature infant? J. Pediatr. Gastroenterol. Nutr. 2013, 57, 432–437. [Google Scholar] [CrossRef]
- Pearson, F.; Johnson, M.J.; Leaf, A.A. Milk osmolality: Does it matter? Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F166–F169. [Google Scholar] [CrossRef]
- Thorkelsson, T.; Mimouni, F.; Namgung, R.; Fernandez-Ulloa, M.; Krug-Wispe, S.; Tsang, R.C. Similar gastric emptying rates for casein- and whey-predominant formulas in preterm infants. Pediatr. Res. 1994, 36, 329–333. [Google Scholar] [CrossRef][Green Version]
- Brun, A.C.; Størdal, K.; Johannesdottir, G.B.; Bentsen, B.S.; Medhus, A.W. The effect of protein composition in liquid meals on gastric emptying rate in children with cerebral palsy. Clin. Nutr. 2012, 31, 108–112. [Google Scholar] [CrossRef]
- Mihatsch, W.A.; Hogel, J.; Pohlandt, F. Hydrolysed protein accelerates the gastrointestinal transport of formula in preterm infants. Acta Paediatr. 2001, 90, 196–198. [Google Scholar] [CrossRef]
- Okamoto, E.; Muttart, C.R.; Zucker, C.L.; Heird, W.C. Use of medium-chain triglycerides in feeding the low-birth-weight infant. Am. J. Dis. Child. 1982, 136, 428–431. [Google Scholar] [CrossRef]
- Sidebottom, R.; Curran, J.S.; Williams, P.R.; Kanarek, K.S.; Bramson, R.T. Effects of long-chain vs. medium-chain triglycerides on gastric emptying time in premature infants. J. Pediatr. 1983, 102, 448–450. [Google Scholar] [CrossRef]
- Hunt, J.N.; Knox, M.T. A relation between the chain length of fatty acids and the slowing of gastric emptying. J. Physiol. 1968, 194, 327–336. [Google Scholar] [CrossRef]
- Riezzo, G.; Indrio, F.; Montagna, O.; Tripaldi, C.; Laforgia, N.; Chiloiro, M.; Mautone, A. Gastric electrical activity and gastric emptying in preterm newborns fed standard and hydrolysate formulas. J. Pediatr. Gastroenterol. Nutr. 2001, 33, 290–295. [Google Scholar] [CrossRef]
- Mihatsch, W.A.; von Schoenaich, P.; Fahnenstich, H.; Dehne, N.; Ebbecke, H.; Plath, C.; von Stockhausen, H.B.; Muche, R.; Franz, A.; Pohlandt, F. The significance of gastric residuals in the early enteral feeding advancement of extremely low birth weight infants. Pediatrics 2002, 109, 457–459. [Google Scholar] [CrossRef]
- Shulman, R.J.; Ou, C.N.; Smith, E.O. Evaluation of potential factors predicting attainment of full gavage feedings in preterm infants. Neonatology 2011, 99, 38–44. [Google Scholar] [CrossRef]
- Li, Y.F.; Lin, H.C.; Torrazza, R.M.; Parker, L.; Talaga, E.; Neu, J. Gastric residual evaluation in preterm neonates: A useful monitoring technique or a hindrance? Pediatr. Neonatol. 2014, 55, 335–340. [Google Scholar] [CrossRef]
- Parker, L.; Torrazza, R.M.; Li, Y.; Talaga, E.; Shuster, J.; Neu, J. Aspiration and evaluation of gastric residuals in the neonatal intensive care unit: State of the science. J. Perinat. Neonatal Nurs. 2015, 29, 51–59. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Group | p | ||
|---|---|---|---|
| IPF | EHF | ||
| gender, n (%) | |||
| male | 17 (56.7) | 16 (53.3) | 0.795 |
| female | 13 (43.3) | 14 (46.7) | |
| birth type, n (%) | |||
| singleton | 15 (50) | 17 (56.7) | 0.605 |
| twin | 15 (50) | 13 (43.3) | |
| Cesarean Section, n (%) | 26 (86.7) | 26 (86.7) | 1.000 |
| Apgar score, n (%) | |||
| 6–7 | 3 (10.0) | 6 (20) | 0.760 |
| 8 | 6 (20.0) | 6 (20) | |
| 9 | 16 (53.3) | 12 (40) | |
| 10 | 5 (16.7) | 6 (20) | |
| gestational age (days) * | 30.1 (1.6) | 30.9 (1.9) | 0.803 |
| birth anthropometrics * | |||
| weight (g) | 1278.7 (259.7) | 1301 (293.2) | 0.756 |
| length (cm) | 38.1 (2.8) | 38.1 (3.3) | 0.973 |
| head circumference (cm) | 27.3 (1.7) | 27.7 (2.4) | 0.481 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldassarre, M.E.; Di Mauro, A.; Montagna, O.; Fanelli, M.; Capozza, M.; Wampler, J.L.; Cooper, T.; Laforgia, N. Faster Gastric Emptying Is Unrelated to Feeding Success in Preterm Infants: Randomized Controlled Trial. Nutrients 2019, 11, 1670. https://doi.org/10.3390/nu11071670
Baldassarre ME, Di Mauro A, Montagna O, Fanelli M, Capozza M, Wampler JL, Cooper T, Laforgia N. Faster Gastric Emptying Is Unrelated to Feeding Success in Preterm Infants: Randomized Controlled Trial. Nutrients. 2019; 11(7):1670. https://doi.org/10.3390/nu11071670
Chicago/Turabian StyleBaldassarre, Maria Elisabetta, Antonio Di Mauro, Osvaldo Montagna, Margherita Fanelli, Manuela Capozza, Jennifer L. Wampler, Timothy Cooper, and Nicola Laforgia. 2019. "Faster Gastric Emptying Is Unrelated to Feeding Success in Preterm Infants: Randomized Controlled Trial" Nutrients 11, no. 7: 1670. https://doi.org/10.3390/nu11071670
APA StyleBaldassarre, M. E., Di Mauro, A., Montagna, O., Fanelli, M., Capozza, M., Wampler, J. L., Cooper, T., & Laforgia, N. (2019). Faster Gastric Emptying Is Unrelated to Feeding Success in Preterm Infants: Randomized Controlled Trial. Nutrients, 11(7), 1670. https://doi.org/10.3390/nu11071670